Introduction
Ovarian cancer is a common gynecological malignant
tumor that presents at a late clinical stage in >80% of the
total patient population (1). It
is associated with a 5-year survival rate of 35% in advanced
ovarian cancer patients. The incidence of ovarian cancer ranks
third while the mortality rate is the highest of all gynecological
malignant tumors. The National Comprehensive Cancer Network 2011
guidelines revealed that epithelial ovarian carcinoma (accounting
for 80% of all malignant ovarian tumors) is the leading cause of
mortality among gynecological cancers in the USA (2). In total, <40% of patients with
epithelial ovarian carcinoma are completely cured (3,4). The
occurrence of ovarian clear cell carcinoma (OCCA) is relatively
infrequent, accounting for 5% of all ovarian malignancies and
3.7–12.1% of all epithelial ovarian carcinomas (5–7). As
reported previously, OCCA has a distinct histological type with
poor prognosis and resistance to platinum-based chemotherapy
(7,14). The majority of patients with
advanced or recurrent OCCA have a low benefit-to-failure ratio from
palliative chemotherapy (7).
According to clinical data, splenic tumors
metastasized from ovarian cancer are uncommon, accounting for 2–4%
of all malignant tumors of the spleen with an incidence of 0.6% in
autopsy studies and ~1.1% in splenectomies (8). In the present study, a rare case of
splenic metastasis of OCCA was reported and an extensive review of
the literature on splenic metastases of ovarian carcinomas
published in the past decade was performed. The aim was to improve
the diagnosis and treatment of splenic metastasis of ovarian
cancer.
Case report
Patient history
A 53-year-old female was admitted to the First
Affiliated Hospital of Xi’an Jiaotong University, (Xi’an, China)
after presenting with a mass in the left upper quadrant which had
been there for three months. The patient did not present with any
other clinical manifestations. The study was conducted in
accordance with the Declaration of Helsinki and was performed with
approval from the Ethics Committee of Xi’an Jiaotong University.
Written informed consent was provided by the participant.
Examination
An abdominal B-ultrasound, performed prior to
hospitalization, revealed multiple mixed cystic-solid lesions in
the left upper quadrant and the lower abdominal region. A needle
biopsy of the mass revealed hyperplasia of fibrous granulation
tissue, infiltration of chronic inflammatory cells, focal shape
necrosis, active growth and tumor-like hyperplasia in sections of
the cells. The histological features prompted the consideration of
a mesenchymal tissue tumor. Following admission, the patient had a
cancer antigen (CA)-125 level of up to 4,712 U/ml (normal <35
U/ml). Subsequent abdominal and pelvic computed tomography (CT)
scans revealed multiple mixed cystic-solid lesions and abdominal
and pelvic cavity effusion, presumably due to an ovarian malignancy
and multiple metastatic intraperitoneal tumors (Fig. 1, prior to chemotherapy).
Pathological results of the needle biopsy on the pelvic mass
revealed a level II papillary adenocarcinoma accompanied by
necrosis.
Treatment
The patient was diagnosed with ‘abdominal and pelvic
cavity metastasis of ovarian carcinoma’ and administered six cycles
of systemic chemotherapy (TP scheme). The patient received 100 mg
docetaxel (day l) and 40 mg cisplatin (days 1–2) for 21 days in
each cycle. During the course of therapy, the CA-125 level
decreased from 4,712 U/ml to 39.42 U/ml. Follow-up CT reexamination
demonstrated that the lesions had markedly diminished, thus, the
therapeutic evaluation was partial remission (PR) (Fig 1). Subsequently the patient underwent
ovarian cytoreductive surgery in addition to a splenectomy. The
final pathology results revealed OCCA (oxyphil cell type) with
massive necrosis and splenic metastasis of OCCA (oxyphil cell type)
with massive necrosis, which were in accordance with the
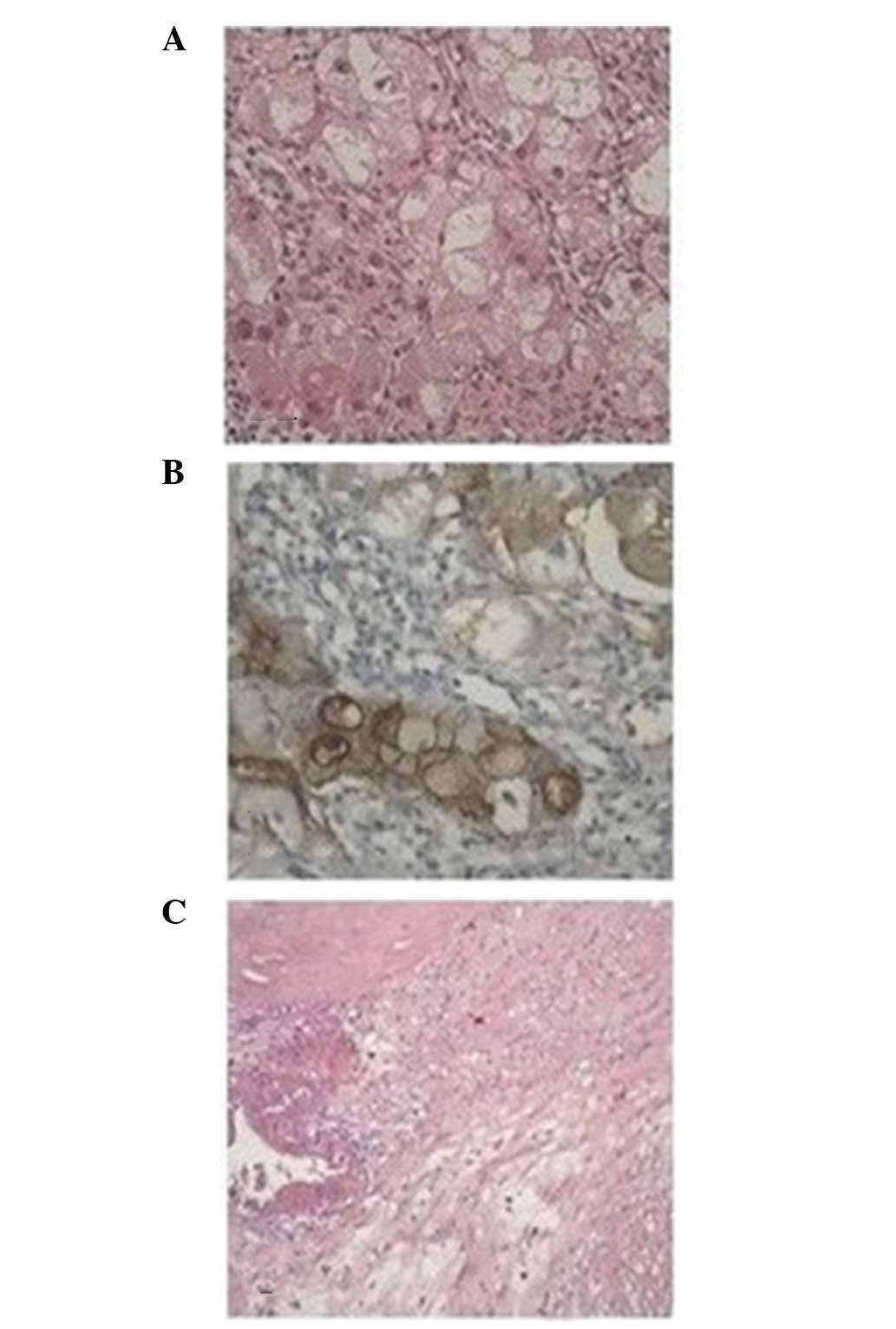
chemotherapeutic results. The immunohistochemical results were
positive for CA-125, cytokeratin (CK)7, CK19 and epithelial
membrane antigen, but negative for CK20 and CD68 (Fig. 2).
Literature review
Case reports and literature reviews on splenic
metastasis of ovarian carcinoma, which had been published in the
past decade, were collected. Based on the search results,
preliminary analysis of the clinical characteristics of splenic
metastasis of ovarian carcinoma was conducted in 34 cases (Table I).
 | Table IClinical characteristics of splenic
metastasis of ovarian carcinoma in 34 cases published in the past
decade. |
Table I
Clinical characteristics of splenic
metastasis of ovarian carcinoma in 34 cases published in the past
decade.
| Case | Age (years) | Pathology | Time of postoperative
splenic metastasis (years) | Characteristics of
splenic metastasis (ref.) |
|---|
| 1 | 52 | Serous | 20 | Solitary (10) |
| 2 | 85 | Serous | Simultaneity | Solitary (11) |
| 3 | 38 | Serous | 3 | Solitary (12) |
| 4 | 29 | Serous | 1 | Solitary (13) |
| 5 | 61 | Serous | 3 (following
subsequent surgery) | Isolated (14) |
| 6 | 51 | Serous | 1 | Bone metastatic
(15) |
| 7 | 53 | Serous | 4 | Solitary (15) |
| 8 | 59 | Serous | 9 | Solitary (16) |
| 9 | 45 | Serous | 6 (following
subsequent surgery) | Solitary (17) |
| 10 | 43 | Angiosarcoma | 2 | Solitary (18) |
| 11 | 59 | Serous | 6 | Solitary (19) |
| 12 | 72 | Carcinosarcoma | 4 | Solitary (20) |
| 13 | 57 | Serous | 12 | Solitary (21) |
| 14 | 55 | Serous | 2 | Solitary |
| 15 | 46 | Serous | 1 | Disseminated in the
omentum majus and pelvic cavity |
| 16 | 80 | Serous | 8 | Solitary |
| 17 | 57 | Serous | 2 | Solitary |
| 18 | 59 | Serous | 1 | Solitary |
| 19 | 49 | Serous | 11 | Solitary |
| 20 | 52 | Serous | 3 | Solitary |
| 21 | 66 | Endometrial
adenocarcinoma | 3 | Disseminated in the
omentum majus and the abdominal cavity |
| 22 | 70 | Serous | 1 | Solitary,
sporadic |
| 23 | 53 | Serous | 3 | a |
| 24 | 45 | Serous | 3 | a |
| 25 | 55 | Serous | Simultaneity | a |
| 26 | 43 | Serous | 4 | a |
| 27 | 64 | Serous | Simultaneity | a |
| 28 | 47 | Serous | Simultaneity | a |
| 29 | 53 | Serous | 2 | a |
| 30 | 55 | Serous | Simultaneity | a |
| 31 | 45 | Serous | 2 | a |
| 32 | 59 | Serous | 2 | a |
| 33 | 61 | Serous | 4 | a |
| 34 | 48 | Serous | 5 | a |
In total, 13 case reports were retrieved on splenic
metastasis of ovarian cancer published in Western countries.
Although each case had distinctive features, pathologically, the
majority were serous papillary adenocarcinoma (9–16,18,20)
with only one case of angiosarcoma (17) and one case of carcinosarcoma
(19). No case reports regarding
OCCA were found. Splenic metastasis occurred postoperatively with
the exception of one case in which splenic metastasis occurred
simultaneously with radical resectioning of ovarian cancer.
Preliminary analysis was also conducted on 21 cases in ten case
reports of splenic metastasis of ovarian cancer published in China
over the past decade. The analytical results were largely
consistent with the data from the case reports published in Western
countries. Pathologically, these cases were serous papillary
cystadenocarcinomas with two cases of mucinous papillary
adenocarcinoma. Splenic metastasis primarily occurred years after
surgery. Splenic metastasis was only detected in four cases when
ovarian cancer was first diagnosed.
OCCA is infrequently reported in literature owing to
its low incidence. Pathologically, the majority of cases in the
reports on splenic metastasis of ovarian cancer belong to serous
papillary cystadenocarcinoma and only individual cases are poorly
differentiated transitional cell carcinomas. Based on the present
analyses of the associated case reports and literature reviews, we
hypothesize that splenic metastasis of ovarian carcinoma largely
occurs postoperatively, following subsequent surgeries or years
after radiotherapy and chemotherapy. Splenic metastasis is
primarily accompanied by dissemination to the omentum majus and
pelvic cavity. Isolated metastatic splenic lesions only occur in a
few individual cases.
Discussion
OCCA is a malignant tumor found primarily among
elderly females. It was formally defined as a special type of
ovarian cancer in 1973 by the World Health Organization (21–23).
OCCA originates from the Müllerian duct and is closely associated
with endometriosis (24). Compared
with other adenocarcinomas, OCCA has unique biological features,
resulting in poor prognosis and high rates of recurrence and
metastasis (25). The main
therapeutic strategies focus on surgery and chemotherapy, although
OCCA is relatively resistant to conventional platinum-based
chemotherapy (7,26). In the present study, a rare case of
splenic metastasis of OCCA was reported. No experience or rules
concerning the treatment and prognosis of OCCA were available to
follow. Thus, the aim was to provide new ideas for the treatment
and prognosis of this rare disease.
The case reported in this study is valuable due to
the unusual pathological type of OCCA. Dissemination to the spleen
and pelvic cavity were detected at the initial diagnosis. The case
was once misdiagnosed by needle biopsy, indicating that needle
biopsy alone may easily lead to misdiagnosis for special
pathological types of ovarian cancers, including OCCA, with splenic
metastasis.
Compared with easily affected organs, including the
liver and lung, the spleen is rarely affected (27) with an incidence of ~0.6% in autopsy
studies and 1.1% in splenectomies (8). Primary tumors with splenic
metastases, systematically reported in Western countries, are
mainly melanomas and lymphomas, followed by breast, lung and
ovarian cancers (28). It is
generally recognized that among the routes of metastasis,
hematogenous metastasis ranks first, followed by lymphatic and
implantation metastases. Reasons for the rare occurrence of splenic
metastases are as follows. Firstly, the sharp angle made by the
splenic artery makes it difficult for tumor emboli to enter the
spleen. Secondly, the rhythmic contractile nature of the spleen
squeezes out the tumor embolus and prevents the tumor lodging in
the spleen. Thirdly, the absence of afferent lymphatics that bring
metastatic tumors to the spleen. Finally, antitumor activity due to
the high concentration of lymphoid tissue in the spleen (29). It has been hypothesized that
metastatic tumors rarely grow in the spleen since the spleen is a
pharmacological and immunological sanctuary. Once a metastatic
splenic tumor grows, it may indicate that monoclonal slow-growth is
occurring (30).
There is no unified treatment and prognosis for
late-stage ovarian cancer with splenic metastasis due to the low
incidence. Therefore, more clinical studies are required. Bristow
et al (31) confirmed that
the thoroughness of cytoreductive surgery is key to prognosis.
Thus, a more thoroughly performed surgery is likely to lead to a
better prognosis. Destruction of 10% of the cancer cells enhances
the median survival rate by 5.5%. Patients in whom >75% of the
cancer cells have been eliminated have a median survival time of
33.9 months, while patients in whom <75% of the cancer cells
have been eliminated have a median survival time of 22.7 months
(P<0.05). However, in more than two-thirds of patients with
ovarian cancer, the lesions have already spread prior to undergoing
primary surgery. Thus, in order to excise all metastatic lesions,
cytoreductive surgery involves the pelvic and abdominal cavities,
including a splenectomy, diaphragmatic surgery and partial
hepatectomy. Splenectomies, based on the accurate evaluation of a
patient’s condition, may improve the patient’s median survival time
and quality of life. However, the decision to perform surgery
should be made cautiously. If satisfactory removal surgery cannot
be achieved, priority should be given to palliative surgery and
chemotherapy.
In the case of the present study, following six
cycles of TP chemotherapy, the CA-125 levels decreased gradually to
within a normal range. Imaging evaluation revealed that the
curative effect reached PR. In addition, the patient underwent
cytoreductive surgery and a splenectomy and the surgical results
were satisfactory. In the following 8 months of follow-up, the
patient was in a good condition without any sign of recurrence and
metastasis. The patient continues to be followed-up and further
observation is required for the long-term survival.
In conclusion, splenic metastasis of ovarian cancer
may be diagnosed by a combination of clinical history, imaging
information and histopathology. For space-occupying lesions of the
spleen, CT is capable of demonstrating intraparenchymal and
infiltrative splenic metastasis in patients with ovarian cancer,
even in the absence of increased CA-125 levels (32,33).
While aspiration cytology is not recommended, complete
cytoreduction in primary or subsequent surgeries is an ideal
treatment for space-occupying lesions of the spleen; even for
recurrent carcinomas. Cytoreductive surgery is capable of
prolonging progression-free survival times and improving quality of
life (34–37). Due to the immunological function of
the spleen, the formation of a metastatic splenic carcinoma usually
indicates an advanced stage of the disease that has poor prognosis.
In such cases, a splenectomy followed by a comprehensive therapy is
the preferred course of treatment. Therapeutic treatments may be
more accurately determined based on the consideration of the
primary lesions, the general condition of the patient and whether
multiple metastases have occurred in other organs.
References
|
1
|
Fleming GF, Ronnett BM and Seidman J:
Epithelial ovarian cancer. Principles and Practice of Gynecologic
Oncology. Barakat RR, Markman M and Randall ME: 5th edition.
Lippincott Williams & Wilkins; Philadelphia, PA: pp. 763–836.
2009
|
|
2
|
Chan JK, Cheung MK, Husain A, et al:
Patterns and progress in ovarian cancer over 14 years. Obstet
Gynecol. 108:521–528. 2006.PubMed/NCBI
|
|
3
|
Jemal A, Siegel R, Ward E, et al: Cancer
statistics, 2009. CA Cancer J Clin. 59:225–249. 2009. View Article : Google Scholar
|
|
4
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar
|
|
5
|
Sugawa T, Umesaki N, Yajima A, et al: A
group study on prognosis of ovarian cancer in Japan. Nihon Sanka
Fukinka Gakki Zasshi. 44:827–832. 1992.(In Japanese).
|
|
6
|
O’Brien ME, Schofield JB, Tan S, et al:
Clear cell epithelial ovarian cancer (mesonephroid): bad prognosis
only in early stages. Gynecol Oncol. 49:250–254. 1993.PubMed/NCBI
|
|
7
|
Sugiyama T, Kamura T, Kigawa J, et al:
Clinical characteristics of clear cell carcinoma of the ovary: a
distinct histologic type with poor prognosis and resistance to
platinum-based chemotherapy. Cancer. 88:2584–2589. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lam KY and Tang V: Metastatic tumors to
the spleen: a 25-year clinicopathologic study. Arch Pathol Lab Med.
124:526–530. 2000.PubMed/NCBI
|
|
9
|
Izuishi K, Sano T, Usuki H, et al:
Isolated splenic metastasis of ovarian cancer 20 years after
operation: a case report and literature review. Tumor. 96:784–786.
2010.PubMed/NCBI
|
|
10
|
Ghani AA, Hashmi ZA, Chase DM, et al:
Intraparenchymal metastases to the spleen from ovarian cancer: a
case report. J Med Case Rep. 4:302010. View Article : Google Scholar
|
|
11
|
Yano H, Iwazawa T, Kinuta M, et al:
Solitary splenic metastasis from ovarian cancer successfully
treated by hand-assisted laparoscopic splenectomy: report of a
case. Surg Today. 32:750–752. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Koh YS, Kim JC and Cho CK: Splenectomy for
solitary splenic metastasis of ovarian cancer. BMC Cancer.
4:962004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yoshioka R, Okabayashi T, Nishimori I, et
al: A long-survived case with solitary splenic metastasis from
ovarian carcinoma. Surg Technol Int. 17:192–194. 2008.PubMed/NCBI
|
|
14
|
Alloni R, Garberini A, Caputo D and
Coppola R: Solitary splenic metastasis of ovarian carcinoma: report
of two cases. Surg Today. 38:1144–1147. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Furukawa N: Solitary splenic metastasis of
ovarian cancer. Arch Gynecol Obstet. 275:499–502. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ushijima K, Nishida T, Okura N, et al:
Solitary splenic recurrence of ovarian cancer: case report and
review of the literature. Arch Gynecol Obstet. 263:79–81. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Valbuena JR, Levenback C, Mansfield P and
Liu J: Angiosarcoma of the spleen clinically presenting as
metastatic ovarian cancer. A case report and review of the
literature. Ann Diagn Pathol. 9:289–292. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Otrock ZK, Seoud MA, Khalifeh MJ, et al:
Laparoscopic splenectomy for isolated parenchymal splenic
metastasis of ovarian cancer. Int J Gynecol Cancer. 16:1933–1935.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Olsen AB, Parqman S and Gillespie T:
Solitary splenic metastasis from ovarian carcinosarcoma: a case
report. J Med Case Rep. 5:562011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hasegawa H, Naitoh H, Tsuchihashi H, et
al: A case of solitary splenic metastasis from an ovarian cancer 12
years after primary resection. Gan To Kagaku Ryoho. 37:1799–1803.
2010.(In Japanese).
|
|
21
|
Teilum G: Gonocytoma homologous ovarian
and testicular tumours. Acta Pathol Microbiol Scand. 23:242–251.
1946.
|
|
22
|
Scully RE: Recent progress in ovarian
cancer. Hum Pathol. 1:73–98. 1970. View Article : Google Scholar
|
|
23
|
Serov SF, Scully RE and Sobin LH:
International histologic classification of tumours. (9)Histologic
typing of ovarian tumours. World Health Organization; Geneva:
1973
|
|
24
|
Tan DS and Kaye S: Ovarian clear cell
adenocarcinoma: a continuing enigma. J Clin Pathol. 60:355–360.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Miyamoto M, Takano M, Goto T, et al: Clear
cell histology as a poor prognostic factor for advanced epithelial
ovarian cancer: a single institutional case series through central
pathologic review. J Gynecol Oncol. 24:37–43. 2013. View Article : Google Scholar
|
|
26
|
Takano M, Kikuchi Y, Yaegashi N, et al:
Clear cell carcinoma of the ovary: a retrospective multicentre
experience of 254 patients with complete surgical staging. Br J
Cancer. 94:1369–1374. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Morgenstern L, Rosenberg J and Geller SA:
Tumors of the spleen. World J Surg. 9:468–476. 1985. View Article : Google Scholar
|
|
28
|
Siler J, Hunter TB, Weiss J and Haber K:
Increased echogenicity of the spleen in benign and malignant
disease. AJR Am J Roentgenol. 134:1011–1014. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Capizzi PJ, Allen KB, Amerson JR and
Skandalakis JE: Isolated splenic metastasis from rectal carcinoma.
South Med J. 85:1003–1005. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lauro S, Trasatti L, Capalbo C, et al:
Solitary splenic recurrence of epithelial ovarian cancer:a case
report and review. Anticancer Res. 22:3643–3645. 2002.PubMed/NCBI
|
|
31
|
Bristow RE, Tomacruz RS, Armstrong DK, et
al: Survival effect of maximal cytoreductive surgery for advanced
ovarian carcinoma during the platinum era: a meta-analysis. J Clin
Oncol. 20:1248–1259. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Spencer NJ, Spencer JA, Perren TJ and Lane
G: CT appearances and prognostic significance of splenic metastasis
in ovarian cancer. Clin Radiol. 53:417–421. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Senturk S, Karcaaltıncaba M and Akata D:
CT diagnosis of intrasplenic metastasis from ovarian carcinoma. Eur
J Radiol. 81:1094–1099. 2012. View Article : Google Scholar
|
|
34
|
Chen LM, Leuchter RS, Lagasse LD and
Karlan BY: Splenectomy and surgical cytoreduction for ovarian
cancer. Gynecol Oncol. 77:362–368. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Eisenkop SM, Spirtos NM, Friedman RL, et
al: Relative influences of tumor volume before surgery and the
cytoreductive outcome on survival for patients with ovarian cancer:
a prospective study. Gynecol Oncol. 90:390–396. 2003.
|
|
36
|
Eisenkop SM, Spirtos NM and Lin WCM:
Splenectomy in the context of primary cytoreductive operations for
advanced epithelial ovarian cancer. Gynecol Oncol. 100:344–348.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Magtibay PM, Adams PB, Silverman MB, et
al: Splenectomy as part of cytoreductive surgery in ovarian cancer.
Gynecol Oncol. 100:369–374. 2006. View Article : Google Scholar
|