Introduction
Ischemic stroke is the most common type of stroke,
accounting for 60–80% of all types of strokes (1). In an ischemic stroke, impairment of
cerebral circulation causes hypoxia and ischemia, leading to
localized ischemic necrosis or softening of brain tissue, as
manifested by localized or diffuse loss of brain function.
Restoring blood supply to ischemic brain tissue is the primary
treatment for ischemic stroke and is performed via two main
methods: non-drug therapy (e.g., extracranial - intracranial
arterial anastomosis) and drug therapy (e.g., thrombolytic
therapy). However, in recent years clinicians have found that in
some patients with ischemic stroke, restoring blood supply to the
brain tissue aggravates the symptoms instead of relieving them.
Other studies have shown that the main pathological factors that
contribute to such reperfusion injuries include an increased number
of free radicals, calcium overload, excitatory amino acid toxicity
and excessive apoptosis of neural cells (2,3).
After the occurrence of acute brain ischemia, a
penumbra zone develops around the lesion area. The metabolism and
function of neurons in this zone are inhibited. If intervention can
reverse such inhibition and activate these neurons, normal function
can be restored. Animal studies have shown that 24 h after the
occurrence of brain ischemia, neuronal axon initiation is
triggered. The axons continue to grow and remodel over the next 14
days and reach maturity on day 28. Intervention that is provided
during neuronal axon initiation may be conducive to recovery of
neurological functions (4,5).
In China, electroacupuncture is used to treat various diseases,
including symptoms of stroke dysfunction. In western countries, the
role of electroacupuncture has also been gradually recognized and
promoted.
In the central nervous system of adult mammals,
there are two types of special neuron clusters: the subependymal
zone of the lateral ventricle and the subgranular zone of the
hippocampal dentate gyrus. Under certain conditions, neurons in
these zones are capable of proliferating (6). However, the amount of endogenous
neural cell proliferation is limited and is not sufficient to
counteract the brain damage induced by cerebral
ischemia-reperfusion (I/R). Therefore, identifying drugs or
measures that can stimulate endogenous neural stem cell
proliferation and differentiation is of great importance.
The extracellular signal-regulated kinase 1/2
(ERK1/2) signaling pathway belongs to the family of
mitogen-activated protein kinase signal transduction pathways. An
abnormality in the ERK1/2 signaling pathway is closely associated
with the occurrence and development of I/R injury. In neurons
affected by ischemic stroke, various mechanisms lead to excessive
activation of ERK, which then promotes cell proliferation, inhibits
apoptosis, promotes cell invasion and affects cell
differentiation.
In the present study, U0126, a highly selective
ERK1/2 pathway inhibitor, was injected in an ischemic-reperfusion
rat model and the mechanism underlying the neuroprotective function
of electroacupuncture at acupoints of Zusanli (ST36) and Quchi
(LI11), was explored. The results indicated that improvement in the
neurological function of ischemic-reperfusion rats, as a result of
electroacupuncture, is closely associated with the ERK1/2
pathway.
Materials and methods
Reagents
The reagents used in this study were: Cyclin D,
cyclin-dependent kinase 4 (CDK4), cyclin E, CDK2, proliferating
cell nuclear antigen (PCNA), p21, p27, β-actin primer (Shanghai
Sangon Biological Engineering Technology and Services Co., Ltd.,
Shanghai, China), TRIzol (Life Technologies Co., Paisley, UK), TTC
stain (Sigma, St. Louis, MO, USA), ERK1/2, p-ERK1/2, cyclin D,
CDK4, CDK2, PCNA, p21, p27, anti-β-actin all rabbit antibody, rat
anti-cyclin E antibody (Cell Signaling Technology, Inc., Danvers,
MA, USA), dimethyl sulfoxide (DMSO) (Xiamen Lulong Biological
Technology Development Co., Ltd., Beijing, China), and inhibitor
U0126 (1,4-diamino-2,3-dicyano-1,4-bis[2-aminophenylthio]butadiene)
(Promega Corp., Madison, WI, USA).
Instruments
Instruments used in this study included the Canon
sx20 digital camera, gel preparation device, protein
electrophoresis system, wet electroblotting system, gel imaging
system, chemiluminescence imager, PCR electrophoresis system
(Bio-Rad Corp., Hercules, CA, USA), automated microplate reader
(BioTek, Hialeah, FL, USA), inverted microscope (Leica Corp.,
Germany), single-arm digital stereotaxic apparatus 68000 (RWD Life
Technology Co., Ltd., China), ST-53311 syringe pump (Stoelting
Corp., Wood Dale, IL, USA), and 50 μl flat head micro-syringe
(Hamilton Corp., Bonaduz, Switzerland).
Animal grouping
A total of 60 healthy, SPF grade, male,
Sprague-Dawley (SD) rats, weighing 250±30 g and aged 2.21±0.15
months, were purchased from the Shanghai SLAC Laboratory Animal
Co., Ltd. [license number: SCXX (Shanghai) 2007-0005]. A random
number table was used to divide the 60 rats into five groups of 12
rats each: the sham control group (SC), middle cerebral artery
occlusion (MCAO) ischemic model control group (IC), MCAO +
electroacupuncture group (EA), MCAO + electroacupuncture + DMSO
group (ED) and MCAO + electroacupuncture + DMSO + U0126 group (EU).
There was no significant difference in the weight or age of rats
between the groups (P>0.05, Table
I).
 | Table IComparison in weight or age of rats
between groups. |
Table I
Comparison in weight or age of rats
between groups.
| Group | No. | Weight (g) | Age (month) |
|---|
| SC | 12 | 252.71±0.40 | 2.11±0.41 |
| IC | 12 | 258.67±0.39 | 2.17±0.26 |
| EA | 12 | 254.22±0.36 | 2.15±0.30 |
| ED | 12 | 255.19±0.36 | 2.13±0.21 |
| EU | 12 | 257.58±0.36 | 2.14±0.33 |
Inhibitor and solvent administration
The U0126 inhibitor was diluted to 10 μM and
injected into the left ventricle of the rat stereotaxically
(7). The dose used was based on
relevant literature (8).
Specifically, DMSO was used to dilute the U0126 inhibitor to 10 μM
and 5 μl of the diluted U0126 inhibitor was loaded into the
micro-syringe. Rats were anesthetized with 10% chloral hydrate (3
ml/kg i.p.) after which, the parietal skin was prepared and the
surgical area disinfected via a strict protocol. Rats were then
fixed in a stereotaxis and a skin incision was made along the
parietal midline, exposing the anterior fontanelle, which was then
marked. The lateral ventricle was precisely located (9) using the stereotaxis, at 2 mm lateral
to and 1 mm below, the anterior fontanelle on the left side. Using
the stereotaxis as a guide, a hole was drilled in the skull at this
localized point and a needle attached to a micro-syringe was
vertically inserted into the cerebral cortex to a depth of ~3.5 mm
beneath the surface. After confirmation that the needle tip was
inside the ventricle, the syringe pump was turned on and the drug
was slowly injected. Three min after completion of the injection,
the micro-syringe was slowly retracted (the duration of needle
retraction was ≥3 min) and the skin was sutured. Drug
administration was carried out 30 min prior to model establishment
(7).
MCAO model
The animals were preoperatively fasted for 12 h.
Rats were weighed and anesthetized with an i.p. injection of 3
ml/kg chloral hydrate. Longa’s suture-occluded method (10) was used to establish the MCAO and
reperfusion model: in rats, the left middle cerebral artery area
was selected as the infarction region and the detailed steps that
were used are the same as those described in previous studies
(11). Reperfusion was performed
2 h after occlusion and the suture was gently retracted to the
carotid artery bifurcation. Intraoperative and postoperative room
temperature was maintained at ~25°C. Incandescent light was used to
keep the animal warm in order to maintain rectal temperature at
37±1°C until recovery as evidenced by resumption of normal
activity. In the SC group, the artery was isolated, but not tied
with suture. After surgery and recovery, the animals were placed in
an environment at room temperature (25°C) and resumed a normal
diet.
Electroacupuncture intervention
Preparation for the electroacupuncture intervention
involved the following: a) SC group: the animals were returned to
the cage following the surgery and maintained, with no treatment
being provided. b) IC group: the animals were returned to the cage
after model establishment and maintained, with no treatment being
provided. c) EA group: on the diseased side, Zusanli and Quchi
acupoints were localized using the method described in
‘experimental acupuncture’ (12).
A electroacupuncture instrument (G6805; Shanghai Huayi Co.,
Shanghai, China; peak voltage = 6 V, dilatational wave, frequency
1–20 Hz) was used and adjusted in order that the limbs were gently
shaking. Each electroacupuncture session lasted 30 min and was
carried out once a day, beginning the day after surgery and ending
on the third day when the animals were euthanized.
Animal sample collection
Animals in different groups were anesthetized, the
abdominal aorta clamped and perfusion was performed through the
left ventricle with 0.9% saline, followed by 4% paraformaldehyde in
phosphate-buffered saline for fixation. The skull was opened and
the brain was quickly removed and placed on ice. The whole brain
tissue was placed in 4% paraformaldehyde in phosphate-buffered
saline, frozen and stored at 4°C. The tissues were embedded in
paraffin for immunohistochemical testing. For TTC staining, animals
in different groups were anesthetized, the abdominal aorta clamped
and perfusion was performed through the left ventricle with 0.9%
saline, followed by 4% paraformaldehyde in phosphate-buffered
saline for fixation. The skull was opened and the brain was quickly
removed and placed on ice. Whole brain tissue was placed in a −80°C
freezer. For western blotting and PCR, animals in different groups
were anesthetized, the skull opened and the brain quickly removed
and placed on ice. Cortical tissues from the left side were
collected, using a scalpel, placed in Eppendorf PCR (EP) tubes and
stored in liquid nitrogen for subsequent use.
Neurological severity score
The five-point scoring system developed by Longa
et al (10) and Bederson
et al (13) was used to
assess the neurological severity of the model animals. The
evaluation was performed 2 h after reperfusion and on days 1–3
immediately prior to electroacupuncture intervention. Neural damage
in model rats that manifested 2 h after the establishment of
infarction was scored on a scale of 0–4 points with a score of 1–3
points suggesting that the model was successful. Specifically the
scores were: 0 points, no neurological deficit; 1 point, the tail
was lifted and adduction (not able to fully extend) of the right
forelimb was observed; 2 points, spontaneous circling to the right
when walking; 3 points, the body was slanted to the right when
walking; 4 points, not able to walk spontaneously along with
possible loss of consciousness.
TTC staining
Fresh brain tissue was placed in −80°C freezer for
20 min, and sections were cut to a thickness of ~2 mm, along the
coronal plane, starting ~2 mm away from the end of the frontal
lobe. Each brain sample was cut into 5–6 slices, which were placed
in TTC, covered with aluminum foil and placed in an incubator at
37°C for 15–30 min. The brain slices were turned frequently to
achieve uniform staining. Following staining, the infarction region
was stained white, whereas the other regions were stained red. The
stained brain slices were placed on a scale, and images were
captured. The Image-ProPlus image analysis and processing system
were used to calculate the total volume of infarcted brain tissue
in each sample. This volume was then divided by the total brain
volume to obtain the percentage of brain infarction for subsequent
statistical analysis.
Immunohistochemistry
The tissue was subjected to routine
paraffin-embedded sectioning and antigen retrieval, then rinsed
with buffer. Anti-PCNA primary antibody was then added in drops, as
described in previous studies (11,14). Under a ×400 light microscope
(Leica DM2500M; Leica Microsystems, Wetzlar, Germany) five
non-overlapping fields were randomly selected and the number of
positively stained cells was counted using automation.
Western blotting
A 200-mg sample of cortical tissue was collected
from the left side of the brain. SDS-PAGE electrophoresis and
membrane transfer were performed, the polyvinylidene fluoride
membrane was removed, and then blocked with 5% skim milk for 2 h.
Anti-ERK1/2, p-ERK1/2, cyclin D, CDK4, cyclin E, CDK2, PCNA, p21 or
p27 antibody was then added and the polyvinylidene fluoride was
incubated at 4°C overnight. A corresponding secondary antibody
(1:5,000) was then added and a computer scan was performed and the
data stored for subsequent analysis.
Reverse transcription (RT)-PCR
RT-PCR was performed to determine mRNA expression
levels of cyclin D, CDK4, cyclin E, CDK2, PCNA, p21 and p27 in the
cortical tissues of left brain of rat. RNA extraction and PCR
products were obtained as described in previous studies (11,12). Then, 8 μl of the PCR product was
subjected to 1.5% agarose gel electrophoresis. Image analysis
software was used to analyze the electrophoretic bands, and the
integrated density value (IDV) of each band was obtained.
Statistical analysis
SPSS 16.0 was used for statistical analysis. Data
are expressed as mean ± standard deviation. For multiple
comparisons of quantitative data, one-way analysis of variance
(ANOVA) was used. If the data satisfied homogeneity of variance,
the Fisher’s least significant difference (LSD) method was applied,
otherwise Tamhane’s method was applied. P<0.05 was considered
statistically significant.
Results
Neurological assessment and brain tissue
morphology of MCAO rats following electroacupuncture treatment
Assessment of the neurological behavior of rats
showed no significant difference between the IC and EU groups at 2
h, 1–3 days after the reperfusion (P>0.05). In the EA and ED
groups, as disease progressed and the electroacupuncture
intervention proceeded, the neurological scores gradually
decreased. The score 2 days after reperfusion was lower compared
with 2 h (P>0.05) and 1 day (P<0.05). The score was lowest 3
days following reperfusion (P<0.05). No significant differences
were observed between any of the groups at 2 h and 1 day after
reperfusion (P>0.05). No significant differences were identified
between the IC and EU groups or between the EA and ED groups
(P>0.05) at 2 h and 2 days after reperfusion. The neurological
scores of the EA and ED groups were significantly lower compared to
the IC group (P<0.05). However, the neurological score of the EU
group was higher compared to the EA and ED groups (P>0.05)
likely due to the effect of U0126 (Table II).
| Table IINeurological deficit scores. |
Table II
Neurological deficit scores.
| Groups (n=12) | 2 h after I/R | 1 day after I/R | 2 days after I/R | 3 days after I/R |
|---|
| SC | 0 | 0 | 0 | 0 |
| IC | 2.67±0.39 | 2.71±0.40 | 2.58±0.42 | 2.33±0.49 |
| EA | 2.58±0.36a | 2.50±0.30 | 1.92±0.60 | 1.42±0.29b,c |
| ED | 2.58±0.47a | 2.54±0.33 | 2.04±0.36 | 1.38±0.31b |
| EU | 2.63±0.38a | 2.67±0.44 | 2.42±0.36 | 2.29±0.40 |
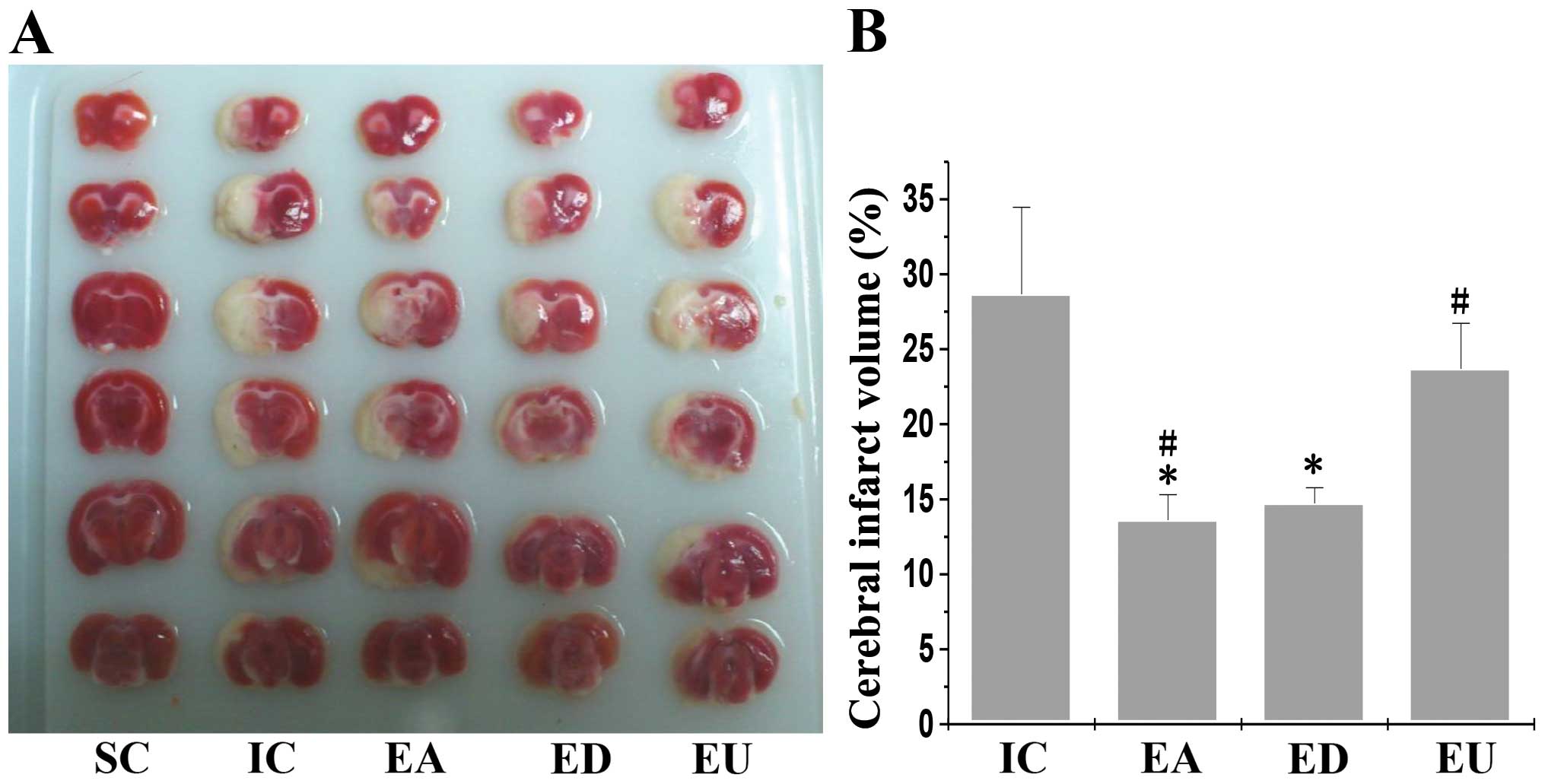
For the morphological and histological analyses,
brain slices of MCAO model rats were subjected to TTC staining and
examined. The IC group exhibited the largest volume of cerebral
infarction (28.67±5.79, n=3). The volume of cerebral infarction was
significantly smaller in the EA (13.60±1.71, n=3) and ED
(14.74±1.04, n=3) groups compared with the IC group (P=0.001). The
cerebral infarction volume was also smaller in the EU (23.69±3.04,
n=3) compared with the IC group, however the difference was not
significant (P=0.113). Similarly, there was no significant
difference in cerebral infarction volume when comparing the EA and
ED groups (P=0.695). Neurological score and the TTC staining
results suggest that electroacupuncture intervention treatment is
effective and that adding inhibitors can reduce treatment efficacy
(Fig. 1).
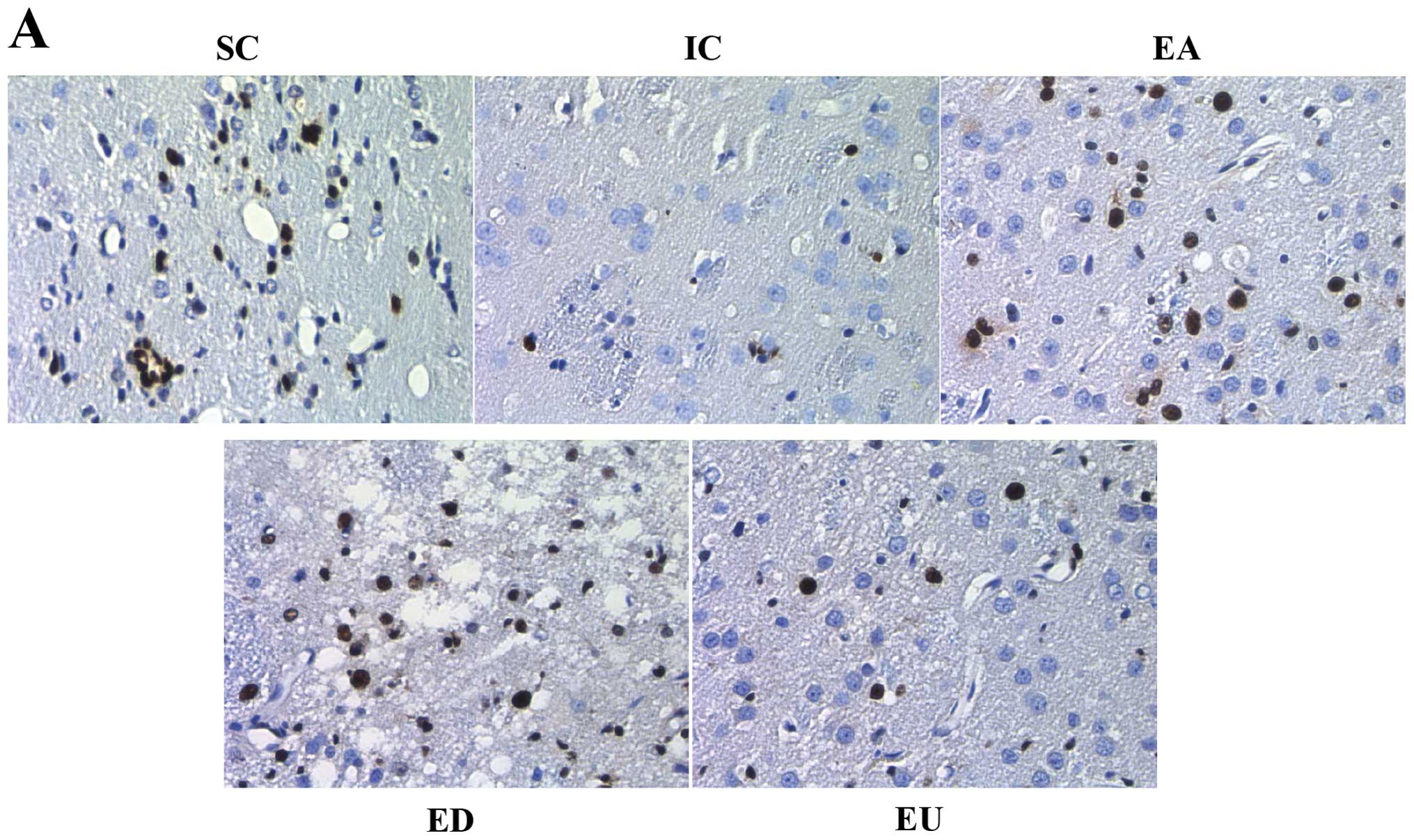
PCNA expression in cerebral ischemia and
reperfusion model rats
In immunohistochemical testing, PCNA-positive
substances that are located in the nuclei are brown in color and
serve as a good indicator of the state of cell proliferation. The
number of PCNA-positive cells was reduced in the IC, EA, ED and EU
groups (Fig. 2A). However, the
number of PCNA positive cells was significantly higher in both the
EA and ED groups compared with the IC group. No significant
difference was observed in the number of PCNA-positive cells in the
IC vs. EU group (Fig. 2B). To
validate these results, RT-PCR was performed to evaluate PCNA
expression. Results obtained by measuring PCNA mRNA expression
showed the same trend as that determined using immunohistochemistry
(Fig. 2C). This observation
suggests that cell proliferation occurs after electroacupuncture in
the infarction region of the rat cortex.
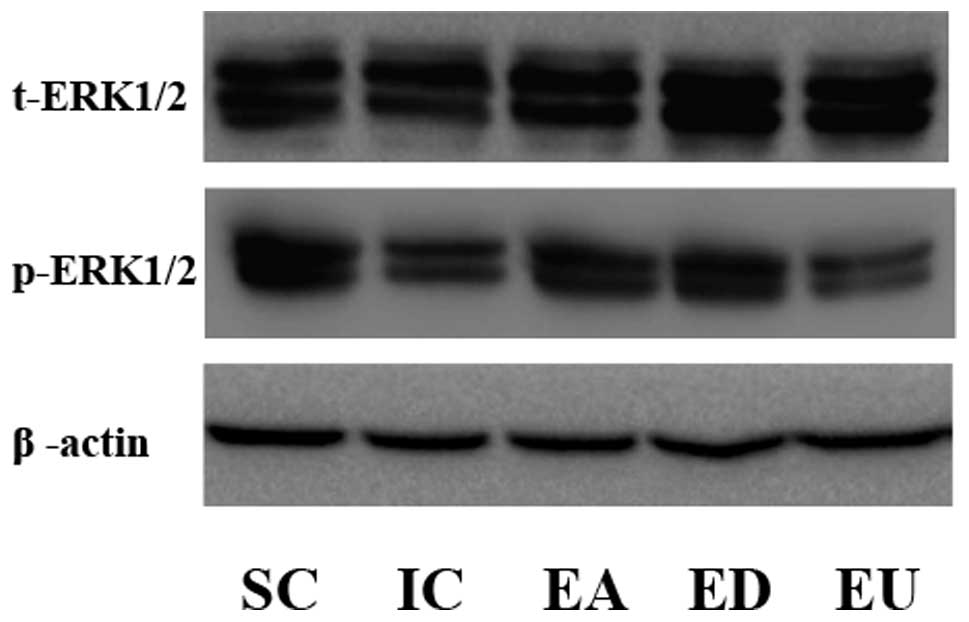
Electroacupuncture and p-ERK1/2
expression in cerebral ischemia and reperfusion model rats
As shown in Fig.
3, t-ERK1/2 was not notably different among different groups.
By contrast, p-ERK1/2 expression in the EA and ED groups was
notably increased compared to the SC group, whereas p-ERK1/2
expression in the IC group was decreased compared to the SC group.
p-ERK1/2 protein expression in the EU group was lower compared to
the SC group due to the effect of U0126. These results suggested
that in cerebral ischemia and reperfusion model rats, U0126 is able
to block activation of the ERK1/2 signaling pathway induced by
electroacupuncture, whereas DMSO does not have any notable effects
on brain damage.
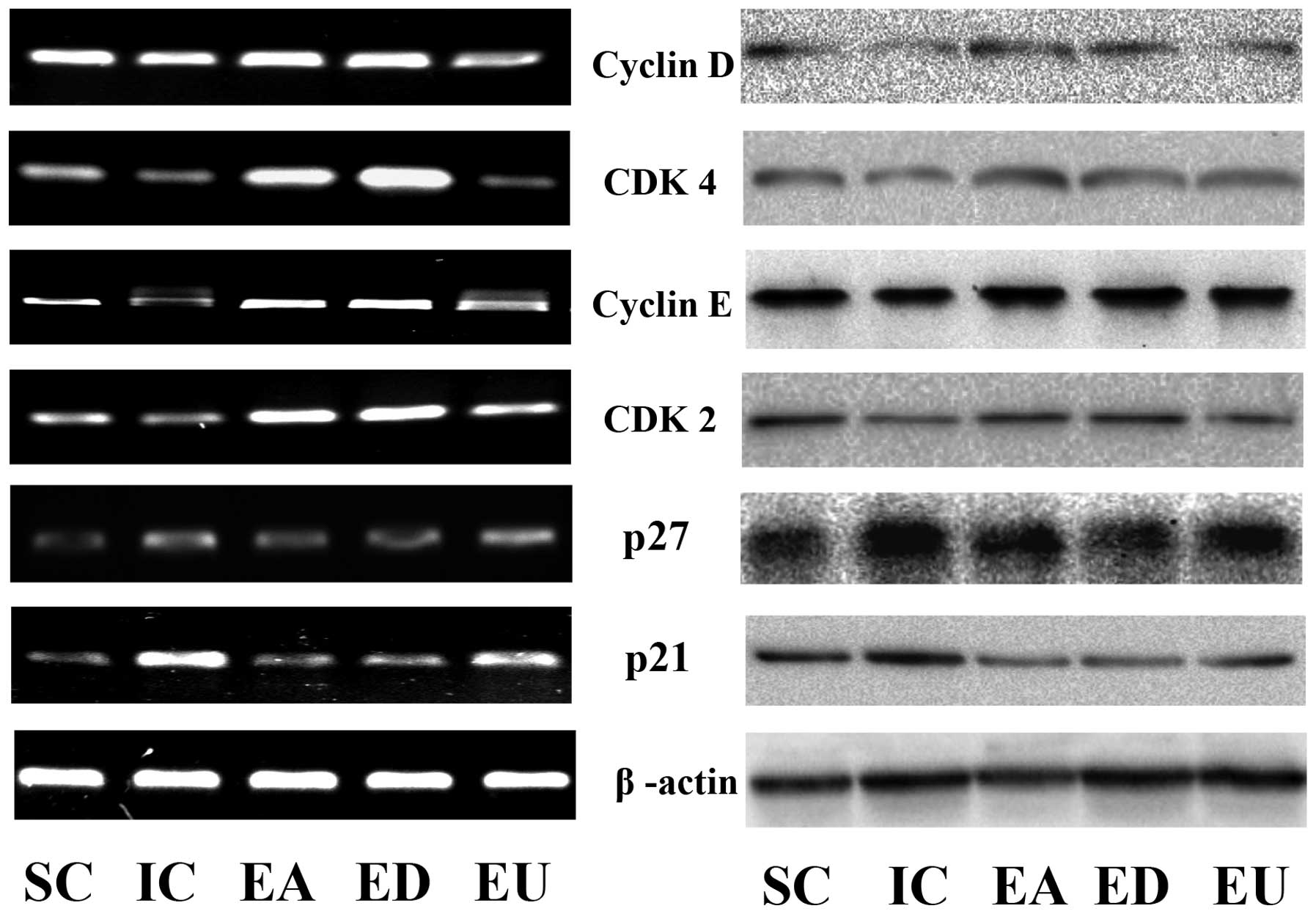
Analyses on growth factors promoting cell
proliferation
As shown in Fig.
4, the mRNA, or transcription levels of cyclin D, CDK4, cyclin
E, and CDK2 were notably higher in the EA and ED groups, and lower
in the EU group, compared to the IC group. Protein expression
levels of cyclin D, CDK4, cyclin E and CDK2 were consistent with
the mRNA results. The mRNA and protein expression of the cyclin
kinase inhibitors p21 and p27 was notably inhibited in the EA and
ED groups, and notably increased in the EU group, compared to the
IC group. This result suggested that, after electroacupuncture
intervention, p21 and p27 expression is downregulated, although
this effect can be reversed by U0126.
Discussion
Ischemic stroke belongs to the ‘stroke’ category in
traditional Chinese medicine. According to the theory of
traditional Chinese medicine, the basic mechanism of ischemic
stroke is loss of ying and yang balance, as well as disruption of
Qi and blood flow. Ancient Chinese physicians believed that
paralysis should be treated ‘through Yangming meridians’. Zusanli
and Quchi are both in the Yangming meridians. Most Yangming
meridians are full of Qi and blood flow; if Qi and blood flow are
smooth in Yangming meridians, the whole meridian system is clear
and this allows the body to recover. The primary lesion area in a
stroke is the head. Quchi belongs to the hand Yangming meridian,
and Zusanli belongs to the foot Yangming meridian. The hand and
foot Yangming meridians pass through the head and the Qi in these
two meridians can act together to treat stroke. Previous studies
(11,14) on a large amount of ancient Chinese
medical literature conducted by our group have shown that Zusanli
and Quchi are the two acupoints that have been used relatively
frequently for stroke treatment. In rats with cerebral ischemia and
reperfusion, electroacupuncture at Zusanli and Quchi was found to
significantly increase β-EP and Glu expression levels in the
hypothalamus, reduce the total calcium level and free radicals in
the brain tissue and inhibit excitatory amino acid toxicity
(15). Functional magnetic
resonance imaging has also confirmed that acupuncture at Zusanli
activates most brain regions, mainly the frontal lobe, temporal
lobe, island lobe, parietal lobe, cingulate gyrus and cerebellum,
and that temporal lobe activation was found to be the most
substantial (16,17). The results of the present study
have demonstrated that the volume of the infarction region in the
EA group was significantly smaller than that in the IC group
(P<0.05). This finding suggests that electroacupuncture can
reduce the infarct volume in cerebral I/R rats, which is consistent
with results of a previous study conducted by our group (11).
Neurological severity scores may be used to predict
the histological effects in cerebral ischemia and reperfusion model
rats (18). The results of the
present study show that on the third day after reperfusion the
neurological severity score of the EA group was significantly lower
than that of the IC group (P<0.05). This suggests that 3 days of
daily treatment with electroacupuncture effectively improves
neurological function in rats that have had 2 h of ischemia
followed by reperfusion. A previous study (19) demonstrated that in male, bilateral
artery ischemia gerbils, p-ERK1/2 expression reached a peak value 5
min after reperfusion, following 3.5 min of ischemia and that on
day 3 after reperfusion the p-ERK1/2 expression was no longer
significantly different compared with the sham group (P>0.05).
This finding suggests that reperfusion activates the ERK1/2 pathway
(19). Since the ERK1/2 pathway
appears to be deactivated by day 3 post-ischemia and reperfusion,
we hypothesized that the neurological improvement observed on day 3
in the present study was due to activation of the ERK1/2 pathway by
electroacupuncture in the EA group.
The ERK1/2 pathway is closely associated with
ischemic stroke. However, whether it plays a protective or damaging
role after ischemic stroke is still under debate (20). A large amount of evidence has
shown that activation of the ERK1/2 pathway protects brain tissue
after ischemic stroke. For instance after cerebral ischemia
reperfusion injury, ERK1/2 can inhibit inflammatory reactions in
the brain tissue (21), promote
osteopontin (OPN) secretion, thereby reducing the release of
excitatory amino acids (22), and
enhance IL-20 expression, promoting cell proliferation, thus
protecting ischemic brain tissue (23). PD98059 and U0126 are both
effective ERK1/2 pathway inhibitors. PD98059 suppresses the
activation of mitogen-activated protein kinase kinase 1 (MAP2K1,
also known as MEK1) induced by upstream kinases, but is ineffective
on MEK1 which has already been activated and activated MEK1 can
still phosphorylate ERK1/2. In comparison, U0126 inhibits MEK1 and
MEK2 highly selectively, whether activated or not, thus effectively
suppressing ERK1/2 phosphorylation. Thus, the inhibitory effect on
the ERK1/2 pathway of U0126 is more stable than that of PD98059
(24). Therefore, in the present
study, U0126 was used as the ERK1/2 pathway inhibitor. The results
of the present study have demonstrated that p-ERK1/2 protein
expression in the EA group was significantly higher than that in
the SC and IC groups, suggesting that 3 days of electroacupuncture
intervention following reperfusion after 2 h of ischemia activates
the ERK1/2 pathway. Compared with the EA and ED groups, p-ERK
protein expression in the EU group was significantly decreased,
whereas p-ERK protein expression in the EA and ED groups did not
differ significantly. This finding suggests that U0126 effectively
inhibits ERK1/2 pathway activation and blocks the pathway
activation effect of electroacupuncture.
The present study has demonstrated that
electroacupuncture improved neurological function in I/R rats. In
addition, the ERK1/2 signaling pathway is one of the key pathways
that regulate cell proliferation. We therefore hypothesized that
the effect of electroacupuncture may be associated with the
regulation of cell proliferation. PCNA is a good indicator of cell
proliferation (25). It can
reflect the activity of neural cell proliferation, thus helping to
promote nerve repair after brain injury (26). In the present study,
immunohistochemistry and RT-PCR were performed to examine PCNA
levels and the results showed that the number of PCNA-positive
cells in the EA group was significantly higher than that in the IC
and EU groups (P<0.05). This finding suggests that
electroacupuncture increases PCNA expression and promotes cell
proliferation, consistent with a previous finding (11).
Cell proliferation is mainly achieved through
progression of cell cycles and is precisely regulated by three
types of factors: CDKs, cyclins and CKIs. In cell cycles specific
CDKs and specific cyclins bind, form complexes, and connect the
signaling pathway with the cell cycle at the G1/S-phase transition.
Studies have shown that when cells enter the S-phase from the
G1-phase, the phosphorylation and activation of ERK1/2 pathway is
crucial to inducing the binding of cyclin D1 and CDK4 and the
binding of cyclin E and CDK2. U0126 inhibits ERK1/2 activation,
thus effectively inhibiting the proliferative effect (27–29). When PD98059 inhibits ERK1/2
signaling pathway activation, p27Kip1 expression is upregulated,
cyclin D1 and E expression is downregulated and the cells are
arrested in the G1-phase (30).
Enhancement of p21Cip1 and p27Kip1 expression suppresses the
binding of cyclin E and CDK2 and hampers the progression of the
cell cycle from the G1/G0 to the S-phase (28). The results of the present study
show that electroacupuncture substantially upregulated the protein
and gene expression of cyclin D1, CDK4, cyclin E and CDK2.
Overexpression of these positive regulatory factors can shorten the
G1-phase, cause the G0/S and/or G1/S transition point to be missed
and lead to continued proliferation. Consistent with this,
electroacupuncture intervention significantly reduces the gene and
protein expression of negative regulators p21Cip1 and p27Kip1, thus
effectively preventing their inhibitory effect on positive
regulatory factors, helping to promote cell proliferation. The
present study also shows that DMSO did not have the above effect.
However, despite electroacupuncture intervention, cell
proliferation in the EU group was not found to increase. Instead, a
high expression of p21Cip1 and p27Kip1 inhibited the expression of
cyclin D1, CDK4, cyclin E and CDK2 expression, the cell cycle was
arrested in the G1-phase and the cells stopped growing, leading to
inhibition of cell proliferation.
In conclusion, the present study shows that
electroacupuncture at Zusanli and Quchi in cerebral I/R rats
activates the ERK1/2 pathway, upregulates positive regulatory
factors PCNA, cyclin D1, CDK4, cyclin E and CDK2 and downregulates
negative regulatory factors p21Cip1 and p27Kip1. This allows rat
cortical cells on the ischemic side to pass the G1-phase and enter
the S-phase 3 days after 2 h of ischemia followed by reperfusion.
This promotes neural cell proliferation and plays a protective role
in the brain, thereby improving neurological function in the rats.
Taken together, these data demonstrate that electroacupuncture
treatment is an effective measure for treating ischemic stroke.
However, the mechanism for long-term neuroprotective effects of
electroacupuncture at Zusanli and Quchi should be further
investigated.
Acknowledgements
We would like to thank Yijing Jiang, Yulong Zou,
Zhicheng Lin and Jiumao Lin for assistance. This study was
sponsored by the Natural Science Foundation of China (No. 81373778)
and Medical Innovation Program of the Fujian Ministry of Health of
China (No. 2012-CX-28).
References
|
1
|
The Chinese medical association of
neurology, cerebrovascular epidemiology group of acute ischemic
stroke treatment guidelines writing group. China’s acute ischaemic
stroke treatment guidelines. Chinese General Practice. 4013–4017.
2010.
|
|
2
|
Diener HC, Foerch C, Riess H, et al:
Treatment of acute ischaemic stroke with thrombolysis or
thrombectomy in patients receiving anti-thrombotic treatment.
Lancet Neurol. 12:677–688. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Flynn RW, MacWalter RS and Doney AS: The
cost of cerebral ischaemia. Neuropharmacology. 55:250–256. 2008.
View Article : Google Scholar
|
|
4
|
Hong J, Wu G, Zou Y, et al:
Electroacupuncture promotes neurological functional recovery via
the retinoic acid signaling pathway in rats following cerebral
ischemia-reperfusion injury. Int J Mol Med. 31:225–231.
2013.PubMed/NCBI
|
|
5
|
Le W, Liu Y, Wang Q, et al: Effect of
scalp-acupuncture on cerebral ischemia/reperfusion rats of
proliferation and differentiation intervention neural stem cell. J
Hubei Univ Trad Chin Med. 2:12–15. 2013.
|
|
6
|
Tao J, Xue XH, Chen LD, et al:
Electroacupuncture improves neurological deficits and enhances
proliferation and differentiation of endogenous nerve stem cells in
rats with focal cerebral ischemia. Neurol Res. 32:198–204. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kawano T, Fukunaga K, Takeuchi Y, et al:
Neuroprotective effect of sodium orthovanadate on delayed neuronal
death after transient forebrain ischemia in gerbil hippocampus. J
Cereb Blood Flow Metab. 21:1268–1280. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pignataro G, Meller R, Inoue K, et al: In
vivo and in vitro characterization of a novel neuroprotective
strategy for stroke: ischemic postconditioning. J Cereb Blood Flow
Metab. 28:232–241. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bao XM and Shu SY: The stereotaxic atlas
of the rat brain. People’s Medical Publishing House; pp. 7–35.
1991
|
|
10
|
Longa EZ, Weinstein PR, Carlson S, et al:
Reversible middle cerebral artery occlusion craniectomy in rats.
Stroke. 20:84–91. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Xie G, Yang S, Chen A, et al:
Electroacupuncture at Quchi and Zusanli treats cerebral
ischemia-reperfusion injury through activation of ERK signaling.
Exp Ther Med. 5:1593–1597. 2013.PubMed/NCBI
|
|
12
|
Li ZR: The subject of experimental
acupuncture and moxibustion. Chinese Press of Traditional Chinese
Medicine; Beijing: 2003
|
|
13
|
Bederson JB, Pitts LH, Tsuji M, et al: Rat
middle cerebral artery occlusion: evaluation of the model and
development of a neurologic examination. Stroke. 17:472–476. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xue X, You Y, Tao J, Ye X, et al:
Electro-acupuncture at points of Zusanli and Quchi exerts
anti-apoptotic effect through the modulation of PI3K/Akt signaling
pathway. Neurosci Lett. 558:14–19. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cai Y-Y, Liu Z-S, Wang S, et al: The
influence of electroacupuncture acupoints on the protein expression
of β-EP and glu hypathalamus in rats with cerebral ischemia
reperfusion injury. Chin J Bas Med Trad Chin Med. 16:1030–1033.
2010.
|
|
16
|
Xiao YY, Du L, Hong BK, et al: Study the
acupuncture at acupoint of Zusanli effects in the brain magnetic
resonance imaging. Sichuan Zhongyi. 25:98–101. 2007.
|
|
17
|
Wang W, Qi JP, Xia YL, et al: The response
of human motor cortex to acupuncture of S36 and G34 as revealed by
functional MRI. Chin J Phys Med Rehabil. 26:472–475. 2004.
|
|
18
|
Garcia JH, Wagner S, Liu KF and Hu XJ:
Neurological deficit and extent of neuronal necrosis attributable
to middle cerebral artery occlusion in rats. Statistical
validation. Stroke. 26:627–634. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Namura S, Iihara K, Takami S, et al:
Intravenous administration of MEK inhibitor U0126 affords brain
protection against forebrain ischemia and focal cerebral ischemia.
Proc Natl Acad Sci USA. 98:11569–11574. 2001. View Article : Google Scholar
|
|
20
|
Sawe N, Steinberg G and Zhao H: Dual roles
of the MAPK/ERK1/2 cell signaling pathway after stroke. J Neurosci
Res. 86:1659–1669. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sironi L, Banfi C, Brioschi M, et al:
Activation of NF-κB and ERK1/2 after permanent focal ischemia is
abolished by simvastatin treatment. Neurobiol Dis. 22:445–451.
2006.
|
|
22
|
Meller R, Stevens SL, Minami M, et al:
Neuroprotection by osteopontin in stroke. J Cereb Blood Flow Metab.
25:217–225. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen WY and Chang MS: IL-20 is regulated
by hypoxia-inducible factor and up-regulated after experimental
ischemic stroke. J Immunol. 182:5003–5012. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dang ZC and Lowik CW: Differential effects
of PD98059 and U0126 on osteogenesis and adipogenesis. J Cell
Biochem. 92:525–533. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kim TJ and Yun YP: Potent inhibition of
serum-stimulated responses in vascular smooth muscle cell
proliferation by
2-chloro-3-(4-hexylphenyl)-amino-1,4-naphthoquinone, a newly
synthesized 1,4-naphthoquinone derivative. Biol Pharm Bull.
30:121–127. 2007. View Article : Google Scholar
|
|
26
|
Wharton SB, Williams GH, Stoeber K, et al:
Expression of Ki67, PCNA and the chromosome replication licensing
protein Mcm2 in glial cells of the aeing human hippocampus
increases with the burden of Alzheimer-type pathology. Neurosci
Lett. 383:33–38. 2005. View Article : Google Scholar
|
|
27
|
Wang B, Gao Y, Xiao Z, et al: ERK1/2
prootes proliferation and inhibits neuronal differentiation of
neural stem cells. Neurosci Lett. 461:252–257. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Feng Q, Huang S, Zhang A, et al: Y-box
protein 1 stimulates mesangial cell proliferation via activation of
ERK1/2. Nephron Exp Nephrol. 113:e16–e25. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Osaki LH, Figueiredo PM, Alvares EP and
Gama P: EGFR is involved in control of gastric cell proliferation
through activation of MAPK and Src signaling pathways
inearly-weaned rats. Cell Prolif. 44:174–182. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sah JF, Balasubramanian S, Eckert RL and
Rorke EA: Epigallo-catechin-3-gallate inhibits epidermal growth
factor receptor signaling pathway. Evidence for direct inhibition
of ERK1/2 and AKT kinases. J Biol Chem. 279:12755–12762. 2004.
View Article : Google Scholar : PubMed/NCBI
|