Introduction
Cardiac hypertrophy is one of the characteristics of
hypertension, myocardial infarction, valvular disease,
cardiomyopathy and congestive heart failure. It is a compensatory
response of cardiomyocytes to the changes in the molecular and
biochemical microenvironment, including pressure overload and
chronic increases in circulating hormones that place long term
stress on the heart (1,2). When the ventricle is initially
stressed, cardiac function can be maintained by adaptive myocyte
hypertrophy, since an adequate number of mast cells can meet the
requirements of the increasing ventricular wall tension and improve
cardiac output. Moreover, neurohumoral factors stimulated by the
adaptive hypertrophic growth of the myocardium and the activation
of intracellular signaling pathways in the heart and vasculature
can also meet the metabolic demands of the body. However, excessive
cellular hypertrophy and long-term hemodynamic overload will
finally lead to maladaptive myocardial remodeling and the
depression of myocardial contractility, which can progress to
congestive heart failure, a leading cause of morbidity and
mortality in our society (3,4).
Myocardial remodeling and the transition from
compensated hypertrophy to the failure of the myocardium involve a
complex series of events at the molecular and cellular level, which
may result in changes in myocardial structure and function
(5). To date, therapy for heart
failure is generally palliative. Thus, a better understanding of
the intracellular signal transduction networks that control myocyte
cell growth may provide new therapeutic directions. Signal
transduction networks are composed of second messengers, enzymes
and ion channels that form pathways relaying specific signals from
the cell surface to intracellular organelles (6). Multiple signaling pathways control
the induction of myocyte hypertrophy. These pathways include the
cAMP-dependent protein kinase A (PKA) pathways, the
mitogen-activated protein kinase (MAPK) pathways and the
calcineurin (CaN)-nuclear factor of activated T cells (NFATc)
transcription factor pathway (7,8).
These pathways serve as an important link between pathological
factors in the environment and the changes in the structure and
function of the cellular elements of the myocardium. An emerging
concept in the field of signal transduction is the existence of
nodes within a network where multiple signaling pathways converge
and share common molecules, thereby facilitating crosstalk between
pathways (6,9,10).
Molecules that participate in these centers of integration are of
special therapeutic interest due to their potential role in the
coordinated modulation of multiple signaling pathways.
A recent attractive family of scaffolding molecules
in the myocardium is the A-kinase anchoring protein (AKAP) family
(11,12). One member of this family that is
involved in cytokine and adrenergic-induced hypertrophy is the
alternatively spliced isoform of muscle AKAP (mAKAPβ) expressed
exclusively in striated myocytes (13). Known for its ability to bind to
PKA, mAKAPβ also binds to multiple proteins, including exchange
factor activated by cAMP (Epac), adenylate cyclase 5 (14), cAMP-specific phosphodiesterase 4D3
(PDE4D3), phosphatidylinositol-specific phospholipase Cε (PLCε)
(2), extracellular
signal-regulated kinase (ERK)5 (13), protein phosphatase 2A (PP2A)
(12), the cardiac-specific type
II ryanodine receptor (RyR2) (15), the
Ca2+/calmodulin-dependent protein phosphatase
calcineurin Aβ (CaN, PP2B) (16),
the sodium/calcium exchanger, NCX1 (17), hypoxia-inducible factor 1α (HIF1α)
and ubiquitin E3-ligases involved in HIF1α regulation (18) and myopodin (19). mAKAPβ localizes to the nuclear
envelope of myocytes, where it is targeted by nesprin-1α (20).
The renin-angiotensin system (RAS) functions as a
neuro-endocrine system playing a key role in cardiovascular and
renal physiology. The overactivation of the RAS system has been
implicated in the induction and progression of hypertension,
atherosclerosis, cardiac hypertrophy, heart failure, ischemic heart
disease and renovascular disorders (21–25). In the RAS system, angiotensinogen
is converted to angiotensin I (Ang I) under the catalytic activity
of renin and is subsequently converted to angiotensin II (AngII), a
short-chain octapeptide, in the presence of Ang I-converting enzyme
(ACEI). AngII, as the principal component of the RAS cascade,
mediates the physiological control of blood pressure and
electrolyte balance through a variety of effects that affect the
function of most of the organs, including the heart, kidneys,
adrenal glands, vasculature and the central nervous system. Studies
have demonstrated that AngII plays an important role in cardiac
cell proliferation, apoptosis and inotropy (26,27). However, chronic stimulation or
overactivation produces deleterious effects on cardiovascular and
renal function (22,23).
Although there have been several previous studies
detailing the role of AngII or mAKAPβ in the progression of
cardiocyte hypertrophy (13,16,26,27), whether mAKAPβ, as a key downstream
molecule in multiple signal transduction pathways, is involved in
the process of AngII-induced cardiocyte hypertrophy and its
potential role remain unclear. The aim of this study was to clarify
the role of mAKAPβ in AngII-induced cardiomyocyte hypertrophy and
investigate the possible mechanisms involved.
Materials and methods
Animals and reagents
All the experiments were performed in accordance
with the Guidelines of Animal Experiments from the Committee of
Medical Ethics at the National Health Department of China
(Shanghai, China) and were approved by the Central Laboratory of
the Shanghai Tenth People’s Hospital (Shanghai, China). The
suppliers of the materials and reagents were as follows: i)
animals: Kunming male rats (Shanghai SLAC Laboratory Animal Co.,
Ltd., Shanghai, China); ii) equipment: high-speed refrigerated
centrifuge (Heraeus, Hanau, Germany), real-time PCR apparatus
(Thermocycler; Biometra, Göttingen, Germany), gel image processing
system (Media Cybernetics, Inc., Rockville, MD, USA), liquid
scintillation counter (Beckman Coulter, Brea CA, USA); iii)
reagents: Dulbecco's modified Eagle’s medium (DMEM; Gibco, Grand
Island, NY, USA), fetal bovine serum (FBS; GE Healthcare Life
Sciences HyClone Laboratories, Logan, UT, USA), AngII
(Sigma-Aldrich Co., St. Louis, MO, USA), [3H]Leucine
(China Institute of Atomic Energy, Beijing, China), RNA PCR kit
(Takara Bio Inc., Otsu, Japan), reverse transcriptase (Promega
Corp., Madison, WI, USA), anti-GADPH antibody (Cat. no. G8795;
Sigma-Aldrich Co.), anti-mAKAPβ antibody (Cat. no. 07-087; Merck
Millipore, Billerica, MA, USA), phosphorylated (p-)ERK2 antibody
(Cat. no. #9108; Cell Signaling Technology, Beverly, MA, USA),
horseradish peroxidase-conjugated secondary antibody (Cat. no.
SP-9002; Zhongshan Golden Bridge Biotechnology Co., Ltd., Beijing,
China.), pLvx-shRNA2 vector (Invitrogen Corp., Madison, WI, USA),
DH-5α E. coli competent cells (Life Technologies, Grand
Island, NY, USA) and the 293T cell line [American Type Culture
Collection (ATCC), Manassas, VA, USA].
Cell culture and identification
Cardiomyocytes were isolated from 2- to 3-day old
male Kunming rats under sterile conditions. In brief, the hearts
were excised from the animals, cut into 1 mm3 fragments
and then rinsed in Hanks' balanced salt solution prior to digestion
with 3 rounds of collagenase type II (Life Technologies) in Hanks’
balanced salt solution without Ca2+ and Mg2+
with ice-cold phosphate-buffered saline (PBS) solution. The
extracts were then filtered and centrifuged at 1,000 × g for 5 min.
The clear supernatants containing ventricular cells were collected.
All the cells were cultured in DMEM (Gibco), which contained 5 mM
glucose, and were supplemented with 10% FBS and 1%
penicillin/streptomycin at 37°C with 5% CO2 in a
humidified atmosphere for 24 h. Non-myocytes were removed by the
preplating of the cells for 1 h at 37°C. The cardiomyocytes were
cultured in DMEM as described above containing 10 μmol/l
cytosine arabinoside. Cytosine arabinoside (10 μmol/l) was
applied for the first 3 days. Finally, the cultured cells were
identified with α-actin immunofluorescence staining, as previously
described (28).
Establishment of cardiomyocyte
hypertrophy
The neonatal rat cardiomyocytes were divided into 4
groups as follows: i) control group; ii) 10−8 mol/l
AngII group; iii) 10−6 mol/l AngII group and
iv)10−4 μmol/l phenylephrine (Phe) group. The
cells were prepared for the analysis of the expression of
cardiomyocyte hypertrophic markers [atrial natriuretic peptide
(ANP) and actin, alpha 1 (Acta1)] 48 h and 72 h after treatment.
The optimal concentration and time required to induce cell
hypertrophy were identified and used as standard conditions in the
following experiments.
Reverse transcription-quantitative PCR
(RT-qPCR) for the detection of the mRNA expression of cardiomyocyte
hypertrophic markers
Total RNA was extracted using 1 ml TRIzol reagent
(Takara Bio Inc.) according to the manufacturer’s instructions.
Total RNA (1 μg) was reverse transcribed using the RT-qPCR
kit according to the manufacturer’s instructions. A Mastercycler
(Eppendorf AG, Hamburg, Germany) and a SYBR real-time PCR kit
(Takara Bio Inc.) were used for qPCR. The expression values were
normalized to those of the unaltered control, GAPDH. All the
RT-qPCR reactions were carried out in triplicate within each
experiment, and the experiments were replicated at least 3 times.
The primers used to amplify GADPH, ANP and Acta1 were as follows:
GAPDH upstream, 5′-TGCCCAGAACATCATCCCT-3′ and downstream,
5′-GGTCCTCAGTGTAGCCCAAG-3′; ANP upstream,
5′-TGGATACACTGGCATCTACT-3′ and downstream,
5′-TCTTCACCGTCCTCCTCAA-3′; and Acta1 upstream,
5′-AAGTACTCCGTGTGGATCGG-3′ and downstream,
5′-GGGCAGCAGCAACGCA-3′.
Immunocytochemistry and cell area
measurements
The cells were placed in 6-well plates at a density
of 1.0×105 cells/ml and 2 ml/well. Following treatment
with AngII, the cardio-myocytes were fixed in 4% paraformaldehyde,
permeabilized with 0.1% Nonidet P-40, and immunostained with mAKAPβ
antibody and α-actinin antibody (Cat. no. sc-17829; Santa Cruz
Biotechnology, Inc., Santa Cruz, CA, USA; in order to distinguish
the cardiomyocytes from the contaminating fibroblasts) in PBS [0.1%
Nonidet P-40 and 3% bovine serum albumin (BSA)] followed by Alexa
fluorescent dye-conjugated specific secondary antibody and Hoechst
33258 DNA staining, as previously described (29). Fluorescent images were taken using
a Leica DMRA fluorescence microscope (Leica Microsystems GmbH,
Wetzlar, Germany) and the cell surface areas were calculated using
the NIH ImageJ image processing program. Data were pooled from 2
independent experiments.
[3H]Leucine incorporation
The cardiocytes were placed in 24-well plates at a
density of 2×105 cells/ml and 500 μl/well.
[3H]Leucine (1 μCi/ml) was used to label the
newly translated proteins for 48 h in the absence or presence of
AngII. Cells were washed twice with ice-cold PBS and incubated in
5% trichloroacetic acid (TCA) for 30 min at 4°C to precipitate the
protein. The precipitates were washed twice and solubilized in 0.4
N NaOH for 2 h. The TCA precipitable radioactivity was measured by
scintillation counting. For analysis, the data were pooled from 2–3
independent experiments performed in triplicate.
mAKAPβ-shRNA lentiviral vector
construction and preparation
Primers for mAKAPβ were designed using Oligo 6.0
software (Molecular Biology Insights, Inc. Cascade, CO, USA), which
was conducted by Shanghai Sangon Biological Engineering Technology
& Services Co., Ltd. (Shanghai, China). The sequences of the
primers were as follows: mAKAPβ upstream,
5′-GATCCGACGAACCTTCCTTCCGAATTCAAGAGATTCGGAAGGAAGGTTCGTCTTTTTTG-3′
and downstream,
5′-AATTCAAAAAAGACGAACCTTCCTTCCGAATCTCTTGAATTCGGAAGGAAGGTTCGTCG-3′.
A target sequence (5′-GACGAACCTTCC TTCCGAA-3′) was selected to
construct the lentiviral shRNA according to a previous study
(10). The target sequence was
used to design 2 complementary oligonucleotides. Following the
dilution of the oligonucleotide fragments, double-stranded DNA
fragments were formed in the annealing reaction system. The
pLvx-shRNA2 vector was linearized by BamHI and EcoRI
restriction enzyme digestion. Pure linearized vector fragments,
double-stranded DNA fragments and vector fragments were collected
and combined together during a 12-h reaction. The recombinant
vector loop was then transformed into the freshly prepared E.
coli competent cells. Following E. coli cell culture for
16 h at 37°C, bacterial colonies were randomly selected as PCR
templates. Verification of the positive clones was conducted using
PCR technology. The positive purified lentiviral shRNA-expressing
plasmids were transfected with the packaging plasmids into 293T
cells. After 8 h, the culture medium was changed to complete
medium. The supernatant was concentrated and collected following
culture for 48 h. The viral titer of the 293T cells was generally
up to 108 TU/ml. The transfected cells were stored in a
−80°C refrig erator for later use. The exponentially growing
cardiomyocytes were seeded at 2×105 cells/well in 1 ml
of culture medium into a 12-well plate, and 10 μl of
concentrated vector stock with a multiplicity of infection (MOI)
value of 20 plus 5 μg/ml polybrene were also added. The
cells were then stored in a 37°C incubator. Following overnight
incubation, the culture medium was changed to fresh culture medium.
The transfection rate was determined by western blot analysis.
Protein extraction and western blot
analysis
Total proteins were obtained by rinsing the treated
cells with ice-cold PBS, and lysing in lysis buffer (10 mM Tris pH
7.4, 20 mM NaCl, 5 mM MgCl2, 0.5% Nonidet P-40 and 0.1
mM PMSF). The extracts were then centrifuged at 12,000 × g for 10
min at 4°C, and the clear super-natants containing total protein
were collected. The protein concentrations were measured using the
BCA protein assay kit (Beyotime Institute of Biotechnology,
Shanghai, China). Equal amounts of protein were loaded, separated
by SDS-PAGE and transferred onto nitrocellulose membranes. After
blocking with 5% non-fat milk in Tris-buffered saline with Tween-20
(TBST) at room temperature, the membranes were incubated overnight
at 4°C with the previously mentioned primary antibodies. After
being incubated with the respective secondary antibodies, immune
complexes were detected using the Odyssey system (LI-COR
Biosciences, Lincoln, NE, USA) based on the protocol. The band
density value was quantified using the NIH ImageJ image processing
program.
Statistical analysis
Data analysis was conducted using the SPSS 16.0
software package for Windows (SPSS Inc., Chicago, IL, USA).
Continuous variables are presented as the means ± standard
deviation (SD). The statistical significance of the differences was
determined by the analysis of variance (ANOVA) or an unpaired
two-tailed t-test; a value of P<0.05 was considered to indicate
a statistically significant difference.
Results
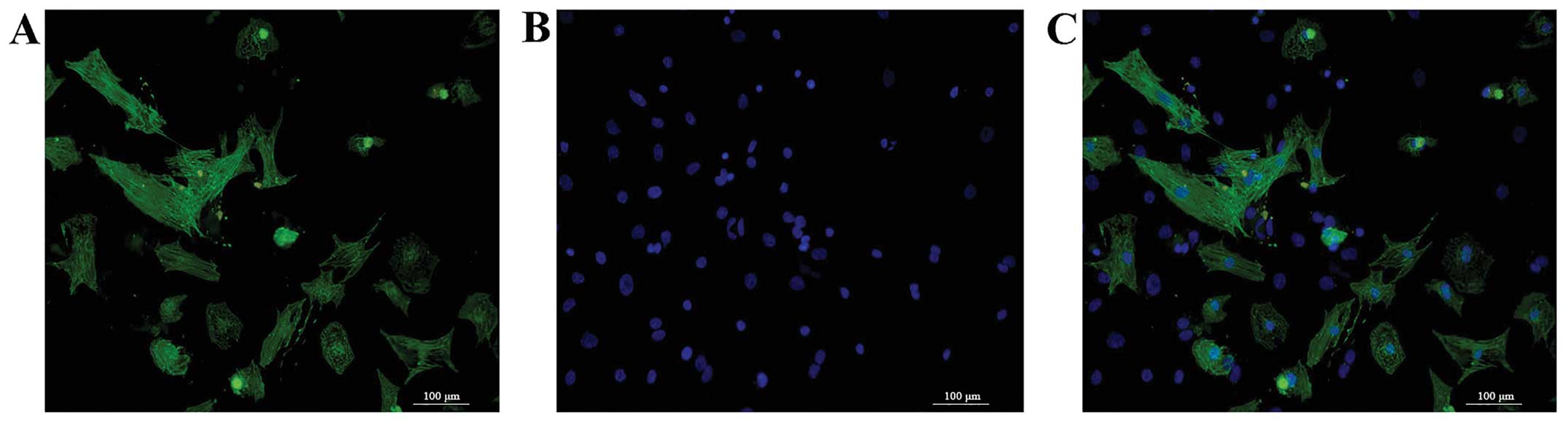
Morphology and identification of
cardiomyocytes
The morphological characteristics of the
cardiomyocyte were observed and images were acquired by digital
fluorescence microscopy (Fig. 1).
The normal cultured cardiomyocytes were positive for α-actinin
inmmunofluorescent staining, and were attached, with an irregular
or triangular shape. The spontaneous pulsation of the
cardiomyocytes was also detected. The negatively stained α-actinin
inmmunofluorescent cells were considered as the contaminating
fibroblasts.
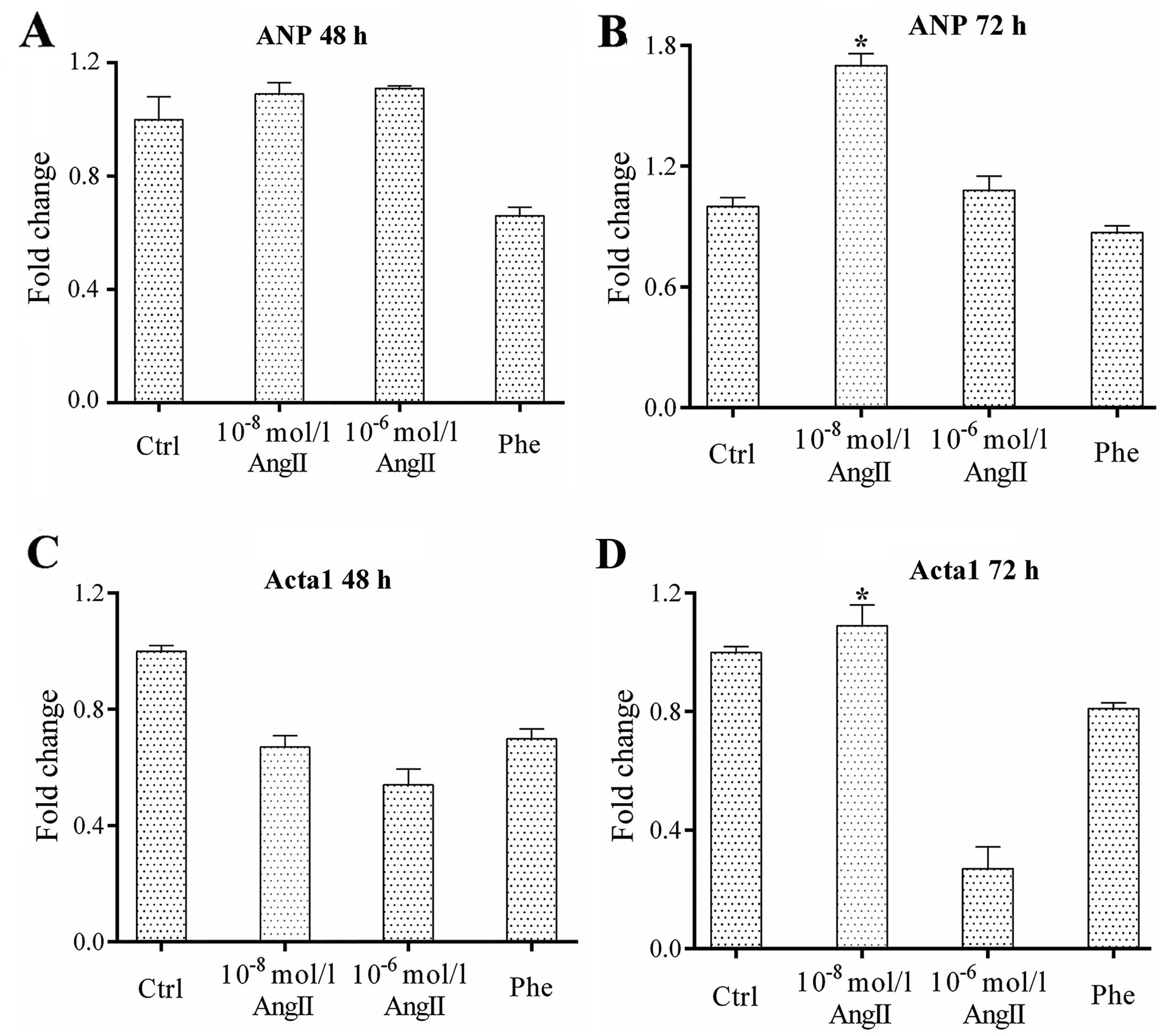
Increase in the expression of
cardiomyocyte hypertrophic makers at optimal concentrations of
AngII and at specific time points following treatment
The effects of AngII (10−8 and
10−6 mol/l AngII) on the expression of cardiomyocyte
hyper-trophic makers at 2 different time points (48 and 72 h) were
examined. Our results revealed that AngII at the appropriate
concentration increased the levels of the cardiomyocyte
hypertrophic makers, ANP and Acta1, at specific time points. The
results from RT-qPCR (shown in Fig.
2) revealed that the expression of the cardiomyocyte
hypertrophic makers was significantly higher following treatment
with 10−8 mol/l AngII at 72 h (all P<0.05 vs.
control). Thus, treatment of the cells with 10−8 mol/l
AngII for 72 h may be considered optimal for the induction of
cardiomyocyte hypertrophy.
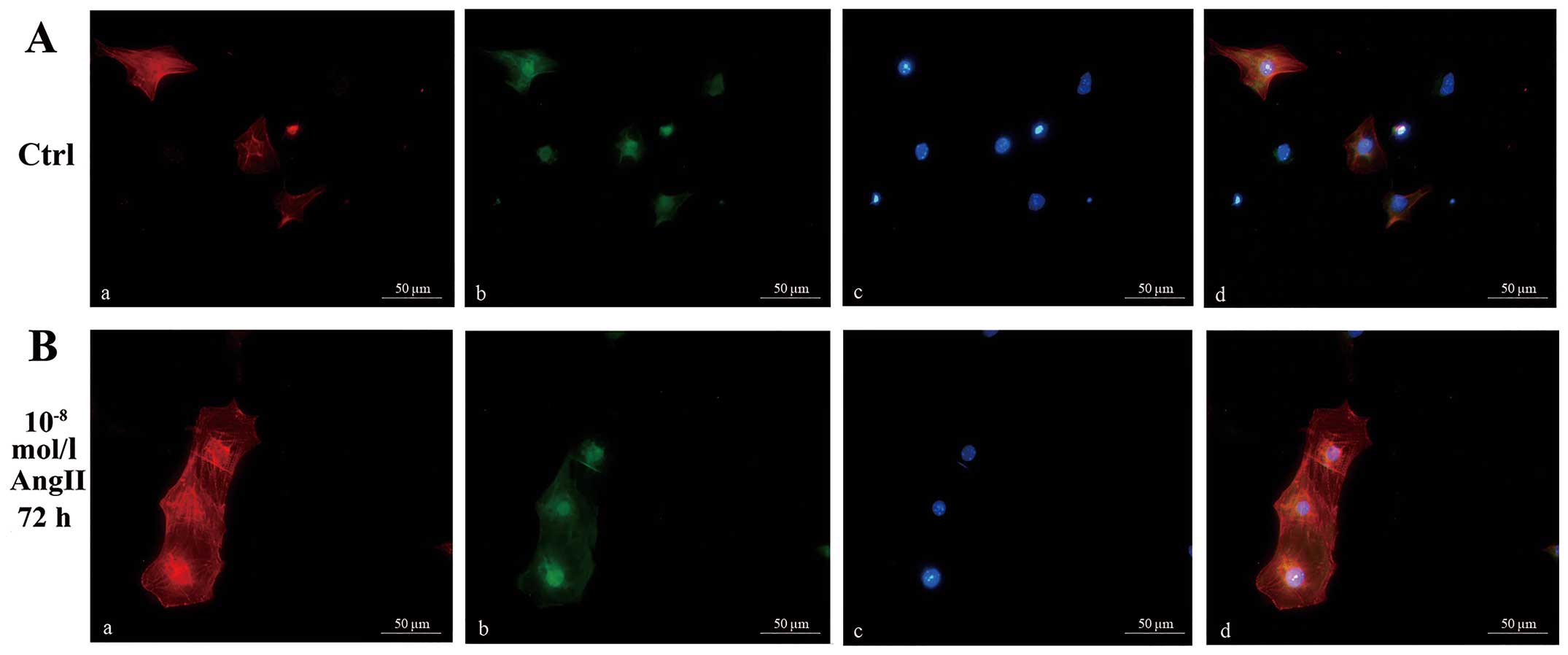
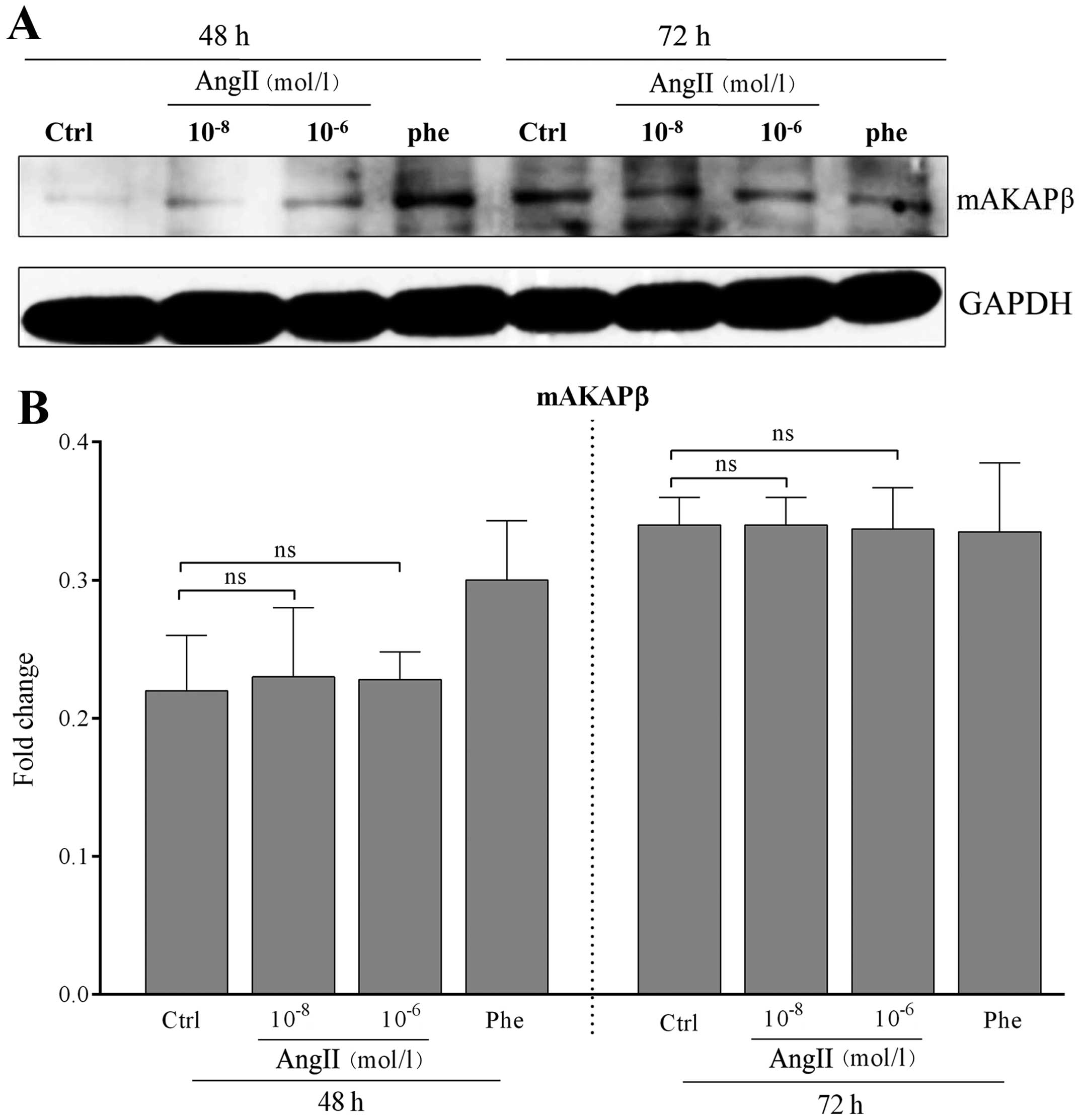
Role of mAKAPβ expression in the process
of AngII-induced cardiomyocyte hypertrophy
The size of the cardiomyocytes treated with or
without AngII is shown in Fig. 3.
The results revealed that AngII promoted the process of
cardiomyocyte hypertrophy. mAKAPβ was localized to the nuclear
envelope of the myocytes; however, the expression of mAKAPβ in the
AngII-treated groups was similar to that of the control group
according to the results of western blot analysis (all P>0.05
vs. control; Fig. 4). These
results demonstrated that mAKAPβ was involved in the process of
AngII-induced cardiomyocyte hypertrophy; however, its expression
remained unaltered.
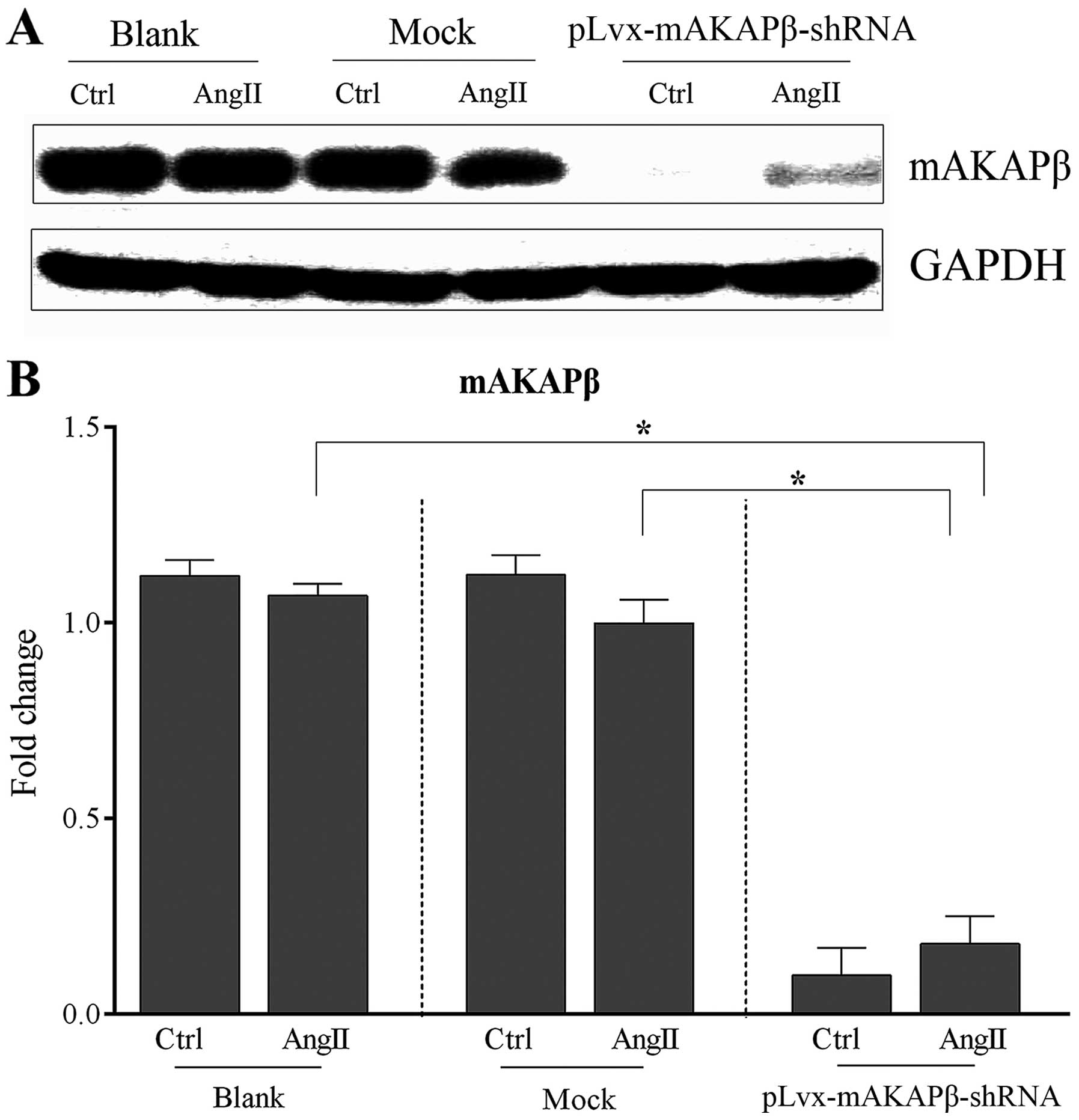
RNA interference significantly reduces
the expression of mAKAPβ in AngII-induced cardiomyocyte
hypertrophy
The requirement for mAKAPβ in AngII-induced
cardiomyocyte hypertrophy was examined by RNA interference using
mAKAPβ-shRNA which was constructed as aforementioned (see Materials
and methods). Six sets of cardiomyocytes were divided into 3
groups: i) the blank group, no virus; ii) the mock group, control
virus; and iii) the pLvx-mAKAPβ-shRNA lentivirus group. After 24 h,
the culture medium was changed to maintenance medium which does not
contain serum. One set from each group was treated with
10−8 mol/l AngII, and the other set was used as a
control. All myocardial cells were then cultured for 72 h. The
results from western blot analysis revealed that the expression of
mAKAPβ in the blank and mock groups showed no statistically
significant difference following treatment with AngII compared with
the control (P=0.08 and P=0.06, respectively; Fig. 5). However, the expression of
mAKAPβ was significantly reduced in the pLvx-mAKAPβ-shRNA
lentivirus group following RNA interference. Moreover, even
following treatment with AngII, the expression of mAKAPβ in the
pLvx-mAKAPβ-shRNA lentivirus group was significantly lower when
compared with that of the AngII-treated cells in the blank and mock
groups (both P<0.05; Fig.
5).
mAKAPβ possibly contributes to
cardiomyocyte hypertrophy following treatment with AngII
To define the potential role of mAKAPβ in
AngII-induced cardiomyocyte hypertrophy, we examined the expression
of cardiomyocyte hypertrophic makers, the [3H]Leucine
incorporation rate and the cell surface area in each group. The
expression of the cardiomyocyte hypertrophic makers (ANP and Acta1)
in the blank and mock groups was significantly elevated following
treatment with 10−8 mol/l AngII for 72 h (both P<0.05
vs. control; Fig. 6A). However,
the expression of ANP and Acta1 in the pLvx-mAKAPβ-shRNA lentivirus
group showed no significant difference compared with the control
(P=0.06 and P=0.12, respectively; Fig. 6A) subsequent to the inhibition of
mAKAPβ.
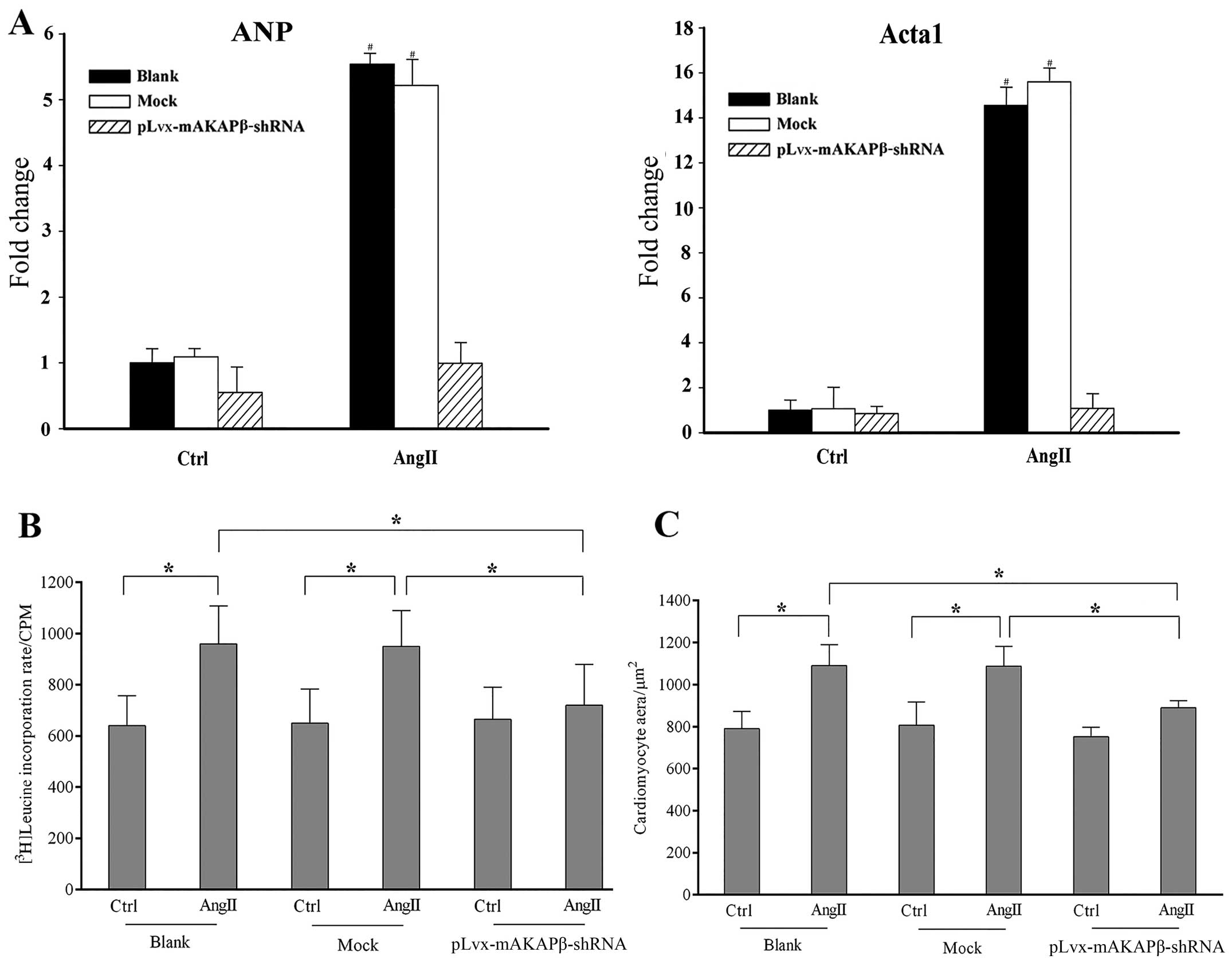 | Figure 6Results of the expression of
cardiomyocyte hypertrophic makers, [3H]Leucine
incorporation rate and cell area measurements of different
treatments. Six sets of cardiomyocytes were divided into 3 groups:
i) Blank group: no virus, ii) Mock group: control virus, and iii)
pLvx-mAKAPβ-shRNA lentivirus group. (A) Results of assays of
cardiomyocyte hypertrophic markers expression in different groups.
(B) [3H]Leucine incorporation rate of each group. (C)
Cell surface areas were calculated using the NIH ImageJ image
processing program. The expression of cardiomyocyte hypertrophic
makers (ANP and Acta1) in blank and mock groups was significantly
elevated following the treatment of 10−8 mol/l
Angiotensin II (AngII) for 72 h (both P<0.05 vs. control). No
significant difference was detected in the expression of ANP and
Acta1 in the pLvx-mAKAPβ-shRNA lentivirus group compared with the
control (P=0.06, P=0.12, respectively). The [3H]Leucine
incorporation rate and cell surface areas were significantly
increased in blank and mock groups, respectively (all P<0.05 vs.
control). No significant difference was observed in
[3H]Leucine incorporation rate and cell surface areas of
pLvx-mAKAPβ-shRNA lentivirus group when compared with control,
respectively (P=0.12 and P=0.08, respectively). Experiments were
repeated at least 3 times. Data are expressed as the mean ± SD in
the corresponding bar graph and statistical significance was
determined by the Student’s t-test. Ctrl, Control; AngII,
Angiotensin II; Columns, mean; error bars, ±SD;
*P<0.05. |
AngII induced a 50.1 and 46.2% increase in the
[3H]Leucine incorporation rate in the blank group
[967.8±147.9 counts per min (CPM) vs. control: 640.1±118.2 CPM] and
mock group (954.1±141.2 CPM vs. control: 652.4±133.0 CPM) groups,
respectively (Fig. 6B).
Similarly, AngII promoted a 38.0% increase in the cell surface area
in the blank group compared with the control (790.2±82.9
μm2 vs. 1090.3±99.6 μm2), and a
34.8% increase was also detected in the mock group compared with
the control (807.4±109.8 μm2 vs. 1088.5±94.4
μm2) (Fig. 6C).
However, the [3H]Leucine incorporation rate in the
pLvx-mAKAPβ-shRNA lentivirus group showed only a 8.2% increase
following treatment with AngII (665.5±125.4 CPM vs. control:
720.5±160.1 CPM) (Fig. 6B).
Similarly, the cells were only 18.4% larger in the
pLvx-mAKAPβ-shRNA lentivirus group compared with the control
(752.6±45.6 μm2 vs. 891.1±33.2
μm2) (Fig. 6C).
These results indicated that the downregulation of mAKAPβ inhibited
AngII-induced cardiomyocyte hypertrophy.
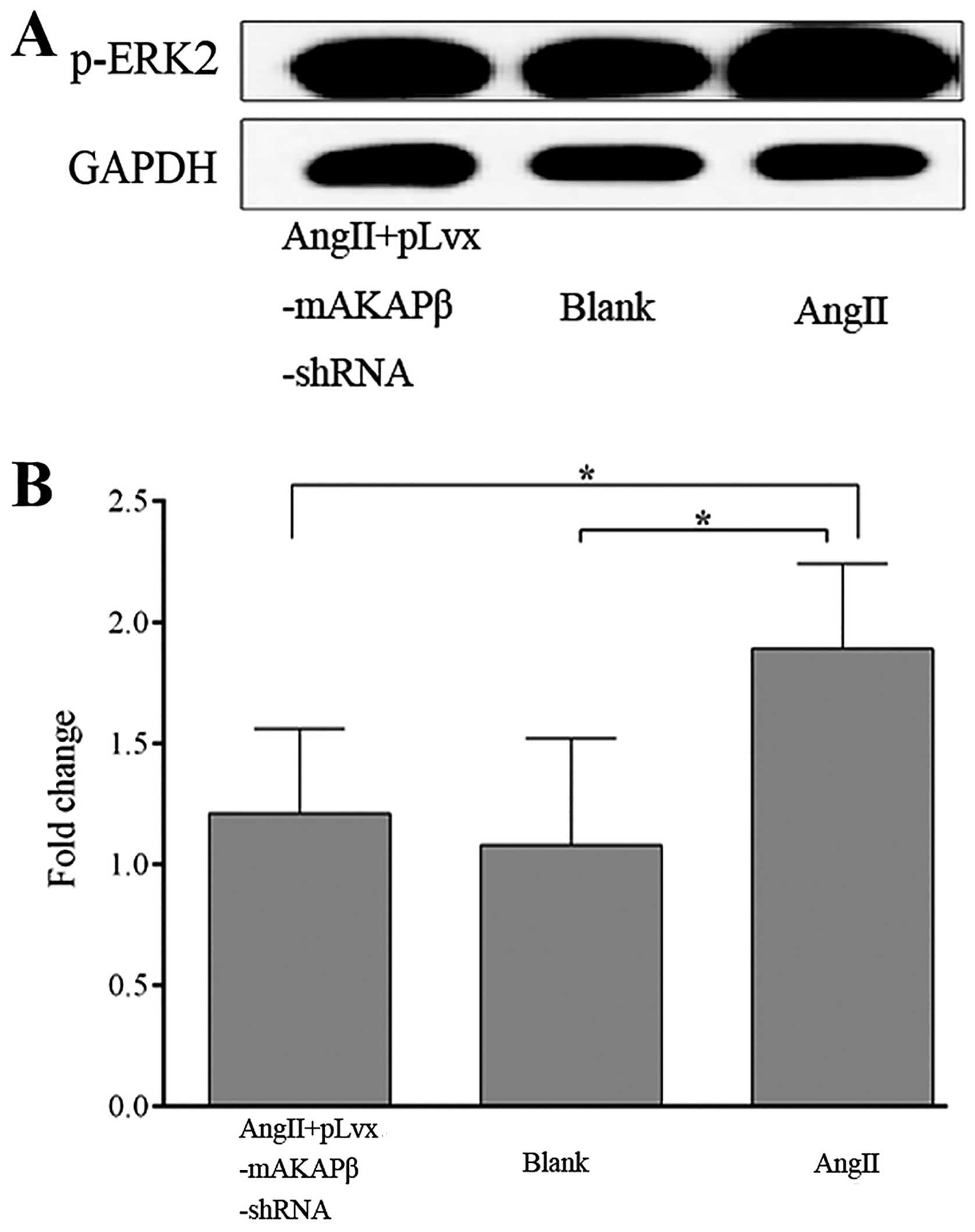
Inhibition of mAKAPβ suppresses the
expression of p-ERK2 in AngII-induced cardiomyocyte
hypertrophy
We also preliminarily investigated the possible
mechanisms underlying the effects of the downregulation of mAKAPβ
on the process of AngII-induced cardiomyocyte hypertrophy. Since
AngII activates ERK in the process of cardiomyocyte hypertrophy
(30), we also examined the
expression of p-ERK2 in the process of AngII-induced cardiomyocyte
hypertrophy. The cells were divided into 3 groups as follows: i)
the AngII + pLvx-mAKAPβ-shRNA group; ii) the blank group; and iii)
the AngII group. The results from western blot analysis revealed
that AngII significantly increased the expression of p-ERK2
(P=0.009 vs. blank group) (Fig.
7). However, the expression of p-ERK2 was significantly reduced
following the inhibition of mAKAPβ by RNA interference in the AngII
+ pLvx-mAKAPβ-shRNA group (P=0.013 vs. AngII group) (Fig. 7). These results indicated that
AngII induced an increase in p-ERK2 expression in the process of
cardio-myocyte hypertrophy, and this increase may be mediated by
mAKAPβ.
Discussion
The main aim of this study was to investigate the
effects of mAKAPβ on AngII-induced cardiomyocyte hypertrophy in
vitro. The potential mechanisms involved were also explored.
RNA interference technology was used and the expression of mAKAPβ
in AngII-induced cardiomyocyte hypertrophy was determined.
Simultaneously, the effects on the activation of the downstream
signaling molecule, ERK2, were also examined. The findings from our
study indicated that in the process of cardiomyocyte hypertrophy
induced by AngII, the expression of mAKAPβ showed no significant
change; however, a sharp increase in p-ERK2 expression was
detected, and this increase may be mediated by mAKAPβ.
Previous studies (31–33) have demonstrated that the
mechanisms responsible for cardiomyocyte hypertrophy involve the
concerted activation of a network of signal transduction pathways.
The hypertrophic signaling network is controlled by a wide array of
neuroendocrine, paracrine and autocrine hormones which include, for
example, catecholamines and peptide hormones that activate
G-protein coupled receptors, interleukin (IL)-6 type cytokines that
activate gp130 receptors, and growth factors that activate receptor
tyrosine kinases. The hypertrophic signaling network promotes
protein synthesis and sarcomeric assembly in the cytoplasm and
induces stereotypical changes in gene expression in the nucleus,
resulting overall in increased myocyte volume and power. The
signaling pathways that control these processes are diverse and
include a large set of second messengers, protein kinases,
phosphatases and downstream effector molecules. There have been a
number of elegant studies concerning hypertrophic intracellular
signaling (9,34,35). However, it is difficult to provide
a comprehensive understanding of this complex process. Thus, many
researchers have focused on a recently emerging concept in signal
transduction, the idea that scaffold proteins mediate the crosstalk
and integration of different signaling pathways through the
formation of multimolecular protein complexes that incorporate the
components of different pathways (10,19,36).
One particular signaling complex that has been well
characterized and implicated in the control of cardiac hypertrophy
is the ‘mAKAPβ signalosome’, a concept that has become established
over the past decade, since the ‘mAKAPβ signalosome’ is a large
multimolecular complex that is involved in multiple signaling
transduction pathways, which integrate multiple upstream signals
and transduce specific downstream signals through the regulation of
multiple effectors (10). mAKAP
was initially identified in a screening for PKA binding proteins.
mAKAPα and mAKAPβ are the 2 known isoforms encoded by the single
mAKAP (AKAP6) gene and are expressed in neurons and striated
myocytes (36). As a consequence
of alternative mRNA splicing, mAKAPβ is identical to residues
245-2314 (the C terminus) of mAKAPα. In adult and neonatal cardiac
myocytes, mAKAPβ is primarily localized to the outer nuclear
membrane through its association with nesprin-1α (20). In addition to PKA, many other
mAKAPβ anchoring proteins, i.e., ‘mAKAPβ signalosome’ components,
have been identified (2,12–19). Due to the association of these
proteins with mAKAPβ in cardiaomyocytes, researchers have confirmed
that the ‘mAKAPβ signalosome’ plays an important role in the
regulation of pathologic cardiomyocyte hypertrophy in response to
upstream signals. To date, 3 of these proteins that can induce
cardiomyocyte hypertrophy have been identified: ERK5, calcineurin
Aβ and PLCε (2,13,16).
Much evidence has indicated that cardiac RAS is
linked to the formation of cardiac hypertrophy. Studies have
demonstrated that all components of RAS (e.g., renin,
angiotensinogen, ACE and AngII receptors) are identified in the
heart at both the mRNA and the protein levels (37) and that RAS is activated in
experimental left ventricular hypertrophy induced by hemodynamic
overload (37–40). It is already known that AngII
plays an important role in the regulation of the structure and
function in the heart (41,42). Apart from its physiological role,
AngII, acting through a family of receptors, exerts an array of
diverse pathological effects in the heart, blood vessels, kidneys,
adrenal glands, liver, smooth muscle, skeletal muscle, pancreatic
islets and other cell types (43–45). AngII directly induces
cardiomyocyte hypertrophy even without an increase in vascular
resistance or cardiac afterload (38). In fact, in vitro studies
have demonstrated that pressure overload also causes an increase in
AngII levels in cardiaomyocytes of neonatal rats, and AngII may act
to promote the growth of cardiomyocytes through an autocrine
mechanism (46,47). Moreover, AngII evokes a variety of
signals to induce cardiomyocyte hypertrophy and the proliferation
of cardiac fibroblasts (46,48), and the AngII-evoked signal
transduction pathways differ among cell types (49). It has been demonstrated that AngII
increases protein synthesis and induces the pathological
hypertrophic growth of cardiomyocytes in an ERK-dependent manner
(30). However, few studies have
explored the underlying mechanisms involved in this process. The
results of the present study demonstrated that the expression of
mAKAPβ remained unaltered in the process of cardiomyocyte
hypertrophy induced by AngII. However, the expression of p-ERK2 in
this process was significantly increased. Furthermore, the
expression of p-ERK2 decreased significantly and AngII-induced
cardiomyocyte hypertrophy was markedly attenuated following the
inhibition of mAKAPβ. Our results mainly provide preliminary
evidence that mAPAKβ potentially affects AngII-induced
cardiomyocyte hypertrophy through its regulation of p-ERK2, which
is useful in the understanding of the molecular mechanisms and the
pathogenesis of cardiac remodeling. Our findings may have
implications regarding novel therapeutic targets in cardiac
hypertrophy.
Although we analyzed the preliminary role of mAKAPβ
in the present study, the effects of mAKAPβ in cardiac hypertrophy
are believed to be more profound than previously reported. This
study was performed using in vitro experimental systems.
Additionally, the association between mAKAPβ and AngII-induced
cardiomyocyte hypertrophy should be confirmed in the isolated heart
through in vivo experiments. We only detected the role of
mAKAPβ through alterations in the ERK pathway. Since the mAKAPβ
complex is involved in multiple signaling transduction pathways,
further studies are required to elucidate the other signaling
pathways involved in this process.
In conclusion, the results of the present study
demonstrated that the expression of mAKAPβ remained unaltered in
the process of AngII-induced cardiomyocyte hypertrophy, and that
the effects of mAKAPβ on cardiomyocyte hypertrophy induced by AngII
may be associated with p-ERK2, whose expression was significantly
increased in this process.
Acknowledgments
This study was supported by a grant from the
National Natural Science Foundation of China (no. 30800466 and no.
81270193) to Y.W. We completed this study at the Central Laboratory
of the Shanghai Tenth People's Hospital of Tongji University,
Shanghai, P.R. China.
References
|
1
|
Gupta S, Das B and Sen S: Cardiac
hypertrophy: mechanisms and therapeutic opportunities. Antioxid
Redox Signal. 9:623–652. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zhang L, Malik S, Kelley GG, Kapiloff MS
and Smrcka AV: Phospholipase C epsilon scaffolds to muscle-specific
A kinase anchoring protein (mAKAPbeta) and integrates multiple
hypertrophic stimuli in cardiac myocytes. J Biol Chem.
286:23012–23021. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aoyagi T, Fujii AM, Flanagan MF, Arnold
LW, Brathwaite KW, Colan SD and Mirsky I: Transition from
compensated hypertrophy to intrinsic myocardial dysfunction during
development of left ventricular pressure-overload hypertrophy in
conscious sheep: Systolic dysfunction precedes diastolic
dysfunction. Circulation. 88:2415–2425. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Oka T and Komuro I: Molecular mechanisms
underlying the transition of cardiac hypertrophy to heart failure.
Circ J. 72(Suppl A): A13–A16. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Oka T, Akazawa H, Naito AT and Komuro I:
Angiogenesis and cardiac hypertrophy: maintenance of cardiac
function and causative roles in heart failure. Circ Res.
114:565–571. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Papin JA, Hunter T, Palsson BO and
Subramaniam S: Reconstruction of cellular signalling networks and
analysis of their properties. Nat Rev Mol Cell Biol. 6:99–111.
2005. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Molkentin JD and Dorn GW 2nd: Cytoplasmic
signaling pathways that regulate cardiac hypertrophy. Annu Rev
Physiol. 63:391–426. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Javadov S, Jang S and Agostini B:
Crosstalk between mitogen-activated protein kinases and
mitochondria in cardiac diseases: Therapeutic perspectives.
Pharmacol Ther. 144:202–225. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Heineke J and Molkentin JD: Regulation of
cardiac hypertrophy by intracellular signalling pathways. Nat Rev
Mol Cell Biol. 7:589–600. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pawson T and Nash P: Assembly of cell
regulatory systems through protein interaction domains. Science.
300:445–452. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Scott JD and Santana LF: A-kinase
anchoring proteins: getting to the heart of the matter.
Circulation. 121:1264–1271. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dodge-Kafka KL, Langeberg L and Scott JD:
Compartmentation of cyclic nucleotide signaling in the heart: the
role of A-kinase anchoring proteins. Circ Res. 98:993–1001. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dodge-Kafka KL, Soughayer J, Pare GC,
Carlisle Michel JJ, Langeberg LK, Kapiloff MS and Scott JD: The
protein kinase A anchoring protein mAKAP coordinates two integrated
cAMP effector pathways. Nature. 437:574–578. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kapiloff MS, Piggott LA, Sadana R, Li J,
Heredia LA, Henson E, Efendiev R and Dessauer CW: An adenylyl
cyclase-mAKAPbeta signaling complex regulates cAMP levels in
cardiac myocytes. J Biol Chem. 284:23540–23546. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Marx SO, Reiken S, Hisamatsu Y, Jayaraman
T, Burkhoff D, Rosemblit N and Marks AR: PKA phosphorylation
dissociates FKBP12.6 from the calcium release channel (ryanodine
receptor): defective regulation in failing hearts. Cell.
101:365–376. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pare GC, Bauman AL, McHenry M, Michel JJ,
Dodge-Kafka KL and Kapiloff MS: The mAKAP complex participates in
the induction of cardiac myocyte hypertrophy by adrenergic receptor
signaling. J Cell Sci. 118:5637–5646. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Schulze DH, Muqhal M, Lederer WJ and
Ruknudin AM: Sodium/calcium exchanger (NCX1) macromolecular
complex. J Biol Chem. 278:28849–28855. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wong W, Goehring AS, Kapiloff MS,
Langeberg LK and Scott JD: mAKAP compartmentalizes oxygen-dependent
control of HIF-1alpha. Sci Signal. 1:ra182008.PubMed/NCBI
|
|
19
|
Faul C, Dhume A, Schecter AD and Mundel P:
Protein kinase A, Ca2+/calmodulin-dependent kinase II,
and calcineurin regulate the intracellular trafficking of myopodin
between the Z-disc and the nucleus of cardiac myocytes. Mol Cell
Biol. 27:8215–8227. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pare GC, Easlick JL, Mislow JM, McNally EM
and Kapiloff MS: Nesprin-1alpha contributes to the targeting of
mAKAP to the cardiac myocyte nuclear envelope. Exp Cell Res.
303:388–399. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
de Gasparo M, Catt KJ, Inagami T, Wright
JW and Unger T: International union of pharmacology. XXIII. The
angiotensin II receptors. Pharmacol Rev. 52:415–472.
2000.PubMed/NCBI
|
|
22
|
Sever PS, Gradman AH and Azizi M: Managing
cardiovascular and renal risk: the potential of direct renin
inhibition. J Renin Angiotensin Aldosterone Syst. 10:65–76. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sata M and Fukuda D: Crucial role of
renin-angiotensin system in the pathogenesis of atherosclerosis. J
Med Invest. 57:12–25. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang CH, Li F and Takahashi N: The renin
angiotensin system and the metabolic syndrome. Open Hypertens J.
3:1–13. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Abadir PM: The frail renin-angiotensin
system. Clin Geriatr Med. 27:53–65. 2011. View Article : Google Scholar
|
|
26
|
Möllmann H, Schmidt-Schweda S, Nef H,
Möllmann S, Burstin JV, Klose S, Elsässer A and Holubarsch CJ:
Contractile effects of angiotensin and endothelin in failing and
non-failing human hearts. Int J Cardiol. 114:34–40. 2007.
View Article : Google Scholar
|
|
27
|
Fabris B, Candido R, Bortoletto M,
Zentilin L, Sandri M, Fior F, Toffoli B, Stebel M, Bardelli M,
Belgrado D, Giacca M and Carretta R: Dose and time-dependent
apoptotic effects by angiotensin II infusion on left ventricular
cardiomyocytes. J Hypertens. 25:1481–1490. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schroder E, Magyar J, Burgess D, Andres D
and Satin J: Chronic verapamil treatment remodels ICa,L
in mouse ventricle. Am J Physiol Heart Circ Physiol.
292:H1906–H1916. 2007. View Article : Google Scholar
|
|
29
|
Kapiloff MS, Jackson N and Airhart N:
mAKAP and the ryanodine receptor are part of a multi-component
signaling complex on the cardiomyocyte nuclear envelope. J Cell
Sci. 114:3167–3176. 2001.PubMed/NCBI
|
|
30
|
Ruf S, Piper M and Schlüter KD: Specific
role for the extracellular signal-regulated kinase pathway in
angiotensin II- but not phenylephrine-induced cardiac hypertrophy
in vitro. Pflugers Arch. 443:483–490. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Niizeki T, Takeishi Y, Arimoto T,
Takahashi H, Shishido T, Koyama Y, Goto K, Walsh RA and Kubota I:
Cardiac-specific overexpression of diacylglycerol kinase zeta
attenuates left ventricular remodeling and improves survival after
myocardial infarction. Am J Physiol Heart Circ Physiol.
292:H1105–H1112. 2007. View Article : Google Scholar
|
|
32
|
Tsutamoto T, Asai S, Tanaka T, Sakai H,
Nishiyama K, Fujii M, Yamamoto T, Ohnishi M, Wada A, Saito Y and
Horie M: Plasma level of cardiotrophin-1 as a prognostic predictor
in patients with chronic heart failure. Eur J Heart Fail.
9:1032–1037. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lu H, Fedak PW, Dai X, Du C, Zhou YQ,
Henkelman M, Mongroo PS, Lau A, Yamabi H, Hinek A, Husain M,
Hannigan G and Coles JG: Integrin-linked kinase expression is
elevated in human cardiac hypertrophy and induces hypertrophy in
transgenic mice. Circulation. 114:2271–2279. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Dorn GW 2nd and Force T: Protein kinase
cascades in the regulation of cardiac hypertrophy. J Clin Invest.
115:527–537. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Oka T, Xu J and Molkentin JD:
Re-employment of developmental transcription factors in adult heart
disease. Semin Cell Dev Biol. 18:117–131. 2007. View Article : Google Scholar
|
|
36
|
Michel JJ, Townley IK, Dodge-Kafka KL,
Zhang F, Kapiloff MS and Scott JD: Spatial restriction of PDK1
activation cascades by anchoring to mAKAPalpha. Mol Cell.
20:661–672. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Suzuki J, Matsubara H, Urakami M and Inada
M: Rat angiotensin II (type 1A) receptor mRNA regulation and
subtype expression in myocardial growth and hypertrophy. Circ Res.
73:439–447. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Baker KM, Booz GW and Dostal DE: Cardiac
actions of angiotensin II: Role of an intracardiac
renin-angiotensin system. Annu Rev Physiol. 54:227–241. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Schunkert H, Dzau VJ, Tang SS, Hirsch AT,
Apstein CS and Lorell BH: Increased rat cardiac angiotensin
converting enzyme activity and mRNA expression in pressure overload
left ventricular hypertrophy. Effect on coronary resistance,
contractility, and relaxation. J Clin Invest. 86:1913–1920. 1990.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Yamazaki T, Shiojima I, Komuro I, Nagai R
and Yazaki Y: Involvement of the renin-angiotensin system in the
development of left ventricular hypertrophy and dysfunction. J
Hypertens Suppl. 12:S153–S157. 1994.PubMed/NCBI
|
|
41
|
Pratt RE: Angiotensin II and the control
of cardiovascular structure. J Am Soc Nephrol. 10(Suppl 11):
S120–S128. 1999.PubMed/NCBI
|
|
42
|
Balakumar P and Jagadeesh G: A century old
renin-angiotensin system still grows with endless possibilities:
AT1 receptor signaling cascades in cardiovascular physiopathology.
Cell Signal. 26:2147–2160. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Mehta PK and Griendling KK: Angiotensin II
cell signaling: physiological and pathological effects in the
cardiovascular system. Am J Physiol Cell Physiol. 292:C82–C97.
2007. View Article : Google Scholar
|
|
44
|
Hunyady L and Catt KJ: Pleiotropic AT1
receptor signaling pathways mediating physiological and pathogenic
actions of angiotensin II. Mol Endocrinol. 20:953–970. 2006.
View Article : Google Scholar
|
|
45
|
Yoshida T, Tabony AM, Galvez S, Mitch WE,
Higashi Y, Sukhanov S and Delafontaine P: Molecular mechanisms and
signaling pathways of angiotensin II-induced muscle wasting:
potential therapeutic targets for cardiac cachexia. Int J Biochem
Cell Biol. 45:2322–2332. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yamazaki T, Komuro I, Kudoh S, Zou Y,
Shiojima I, Mizuno T, Takano H, Hiroi Y, Ueki K, Tobe K, Kadowaki
T, Nagai R and Yazaki Y: Angiotensin II partly mediates mechanical
stress-induced cardiac hypertrophy. Circ Res. 77:258–265. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Sadoshima J, Xu Y, Slayter HS and Izumo S:
Autocrine release of angiotensin II mediates stretch-induced
hypertrophy of cardiac myocytes in vitro. Cell. 75:977–984. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Schorb W, Booz GW, Dostal DE, Conrad KM,
Chang KC and Baker KM: Angiotensin II is mitogenic in neonatal rat
cardiac fibroblasts. Circ Res. 72:1245–1254. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Zou Y, Komuro I, Yamazaki T, Kudoh S,
Aikawa R, Zhu W, Shiojima I, Hiroi Y, Tobe K and Kadowaki T:
critical roles of Gbetagamma subunit, Src family, and Ras in
cardiac fibroblasts. Circ Res. 82:337–345. 1998. View Article : Google Scholar : PubMed/NCBI
|