Introduction
The management of patients with advanced prostate
cancer who have relapsed after initial hormonal therapy is
challenging. Some reports have demonstrated that substitution of
anti-androgen (SOA) remains effective in this setting prior to
introducing chemotherapies such as docetaxel, and it is mentioned
as a treatment option in the European Association of Urology (EAU)
2012 guidelines. However, SOA has a relatively low PSA response
rate (25–40%) and a short duration of efficacy (4–6 months)
(1–3). Therefore, we conducted this study to
determine whether it would be more effective to add a mild oral
chemotherapeutic agent to SOA.
Tegafur-uracil is an orally administered pro-drug of
5-fluorouracil (5-FU) with a cytostatic effect. Tegafur is
metabolized into 5-FU in the liver and uracil is added to prevent
5-FU degradation. This drug has been approved in over 30 countries,
including Japan. Adjuvant chemotherapy with tegafur-uracil has been
demonstrated to be effective for several types of cancers. Patient
survival after the complete resection of stage I lung
adenocarcinoma is improved with tegafur-uracil administration
(4). A significant survival
benefit after surgery is also observed in patients with locally
advanced gastric cancer when tegafur-uracil is used as an adjuvant
therapy (5). Furthermore, based on
the recent idea of ‘tumor dormancy’, tegafur-uracil has been given
with hormonal therapy as an initial treatment for advanced prostate
cancers with the expectation of cytostatic effect that results in a
longer progression-free survival (6).
It has been reported that the expression level of
enzymes involved in 5-FU metabolism may be correlated with 5-FU
efficacy and clinical outcome. If the expression level of
thymidylate synthase (TS), as a target enzyme of 5-FU, and
dihydropyrimidine dehydrogenase (DPD), as a degrading enzyme, was
low in gastrointestinal cancer tissues, there was a favorable
response to 5-FU, leading to better prognosis (7–9). As
5-FU metabolic pathways were further investigated, it has also been
indicated that thymidine phosphorylase (TP) (10) and orotate phosphoribosyltransferase
(OPRT) (11) may be related to the
5-FU sensitivity.
It is known that the expression level of these
5-FU-related enzymes are quite different among various types of
cancers (12). Invasive bladder
cancer has higher TS expression, and it has a positive correlation
with that of proliferation markers. Furthermore, patients with a
high level of TS immunostaining had a significantly poorer
prognosis in bladder cancer (13,14).
However, in prostate cancer, the expression level of these enzymes
has not fully been examined, and the correlation of their
expression level with stage, Gleason score or prognosis has not
been investigated.
Therefore, we have conducted a multi-center
prospective randomized phase II study to examine the effectiveness
and safety of the combination therapy by comparing the combination
therapy of SOA and tegafur-uracil with SOA alone for
castration-resistant prostate cancer. In addition, we sought to
examine whether the expression level of enzymes involved with 5-FU
metabolism were correlated with the efficacy of the combination
therapy and determine whether they would serve as predictive
factors for the combination therapy.
Materials and methods
Patients
This study enrolled patients who were histologically
confirmed to have prostate cancer and relapsed after initial
hormonal therapy. Relapse was defined as at least three consecutive
increases in PSA, the progression of measurable nodal or visceral
lesions, or new metastatic lesions. Additional eligibility criteria
included an Eastern Cooperative Oncology Group (ECOG) performance
status (PS) ≤2, a life expectancy of at least 3 months, adequate
bone marrow, liver and renal function, and a normal
electrocardiogram. Patients were ineligible if they had undergone a
radical prostatectomy or radiation therapy for primary prostate
cancer with curative intent, had an active infection, used
phenytoin, had serious co-morbidity such as ileus, interstitial
pneumonia and uncontrollable diabetes mellitus or had active
concomitant cancer. All patients provided written informed consent
to participate in this study. This study was approved by the
institutional review board at each hospital and conducted in
accordance with Good Clinical Practice guidelines and the
Declaration of Helsinki.
Study design
This study was a randomized multicenter phase II
study with 16 centers. Randomization was stratified based on prior
hormonal therapy [LH-RH analogue/castration or maximum androgen
blockage (MAB)], stage (non-metastatic or metastatic), and Gleason
score (≤6 or ≥7). If patients had disease progression after initial
hormonal therapy, the anti-androgen was discontinued, and the
patients were assessed for anti-androgen withdrawal syndrome (AWS).
Thereafter, the patients were centrally randomly assigned in a 1:1
ratio to receive another anti-androgen alone (SOA, group A) or
tegafur-uracil together with SOA (group B). The administered
anti-androgens included bicalutamide, flutamide and chlormadinone
acetate, which are available in Japan. Tegafur-uracil was orally
administered at 200 mg twice a day for patients with a body surface
area (BSA) ≥1.35 and 100 mg three times a day for those with a BSA
<1.35. Patients received continuous treatment until disease
progression, death, unacceptable toxicity or withdrawal of consent
for any reason. Subsequent anticancer therapy for patients with
progressive disease was at the discretion of the patients and their
physicians.
Measurement of gene expression levels of
the enzymes that are involved with 5-FU metabolism
Laser capture microdissection
(LCM)
To exclusively obtain prostate cancer cells, a laser
capture microdissection system (Carl Zeiss Microscopy GmbH, Jena,
Germany) was utilized. Formalin-fixed paraffin-embedded (FFPE)
blocks from prostatic needle biopsy specimens at diagnosis were
serially sectioned and mounted onto non-coating slides and stained
with hematoxylin and eosin (H&E). Prostate cancer cells were
precisely discriminated from benign and stromal cells by a
pathologist. Tumor cell dissection was continued until at least a 1
mm2 area was obtained, and the dissected tumor cells
were collected in sterile 0.5 ml tube.
RNA extraction, complementary DNA
(cDNA) preparation and amplification
Total RNA extraction and reverse transcription were
performed using the Paradise Plus Whole Transcript Reverse
Transcription (WT-RT) Reagent System (MDS Analytical Technologies,
Sunnyvale, CA) according to the manufacturer’s instructions. The
amount and quality (i.e., RNA integrity number, RIN) of the
extracted RNA were assessed with an Agilent 2100 Bioanalyzer using
the Agilent RNA6000 Pico kit (Agilent Technologies, Santa Clara,
CA). If the RIN was between 0 and 2, the RNA was considered to be
degraded and not used for cDNA amplification. cDNA amplification
was performed using the TaqMan PreAmp Master Mix kit (Life
Technologies Inc., Carlsbad, CA) according to the manufacturer’s
instructions.
Quantitative reverse-transcription
polymerase chain reaction (qPCR)
A two-step TaqMan real-time qRT-PCR was performed
with an ABI Prism 7900 machine (Life Technologies). Reactions were
performed at 50°C for 2 min, 95°C for 10 min followed by 40 cycles
of 95°C for 15 sec and 60°C for 1 min. Relative quantification was
performed using the ΔΔCt method in which the gene
expression levels were normalized by using that of the β-actin gene
as an endogenous control. Primers and TaqMan MGB probes for TS,
DPD, OPRT, TP and β-actin were designed using the Primer
Express® Software Version 3.0 (Life Technologies) with
71 bp amplicons as follows: TS forward, 5′-GAATCACATCGAGCC
ACTGAAA-3′; reverse, 5′-GAAGAATCCTGAGCTTTGGG AAA-3′; probe,
5′-CAGCTTCAGCGAGAAC-3′; DPD forward,
5′-TCTGGCTACCAGGCTATACAGTTT-3′; reverse, 5′-CAGC
CTGTACAAGTGTCGGTTAT-3′; probe, 5′-AAACCCACCTG CCCAC-3′; OPRT
forward, 5′-GGGACTACACTAGAGCAG CGGTTA-3′; reverse,
5′-GCCAGAAATAAAACCAACAACA AATT-3′; probe, 5′-AGTGCTCCTC AGCCAT-3′;
TP forward, 5′-TCCTATATGCAGCCAGAGATGTG-3′; reverse, 5′-ACTG
AGAATGGAGGCTGTGATG-3′; probe, 5′-TGGACAGCCT GCCAC-3′; β-actin
forward, 5′-AAGGCCAACCGCGAG AAG-3′; reverse,
5′-ATAGCAACGTACATGGCTGGG-3′; probe, 5′-ACCCAGATCATGTTT-3′.
End-points and assessments
The primary end-point was the PSA response rate,
which is defined as the percentage of patients with a ≥50% PSA
decrease from baseline. The secondary end-points included time to
PSA progression (TTP), adverse events (AEs), and the correlation of
treatment efficacy with the mRNA expression of key enzymes involved
in 5-FU metabolism. TTP was defined as the time interval between
the start of therapy and the date of progression, which is defined
as a rise in the PSA level three consecutive times and a ≥50%
increase from the nadir for PSA responders or three consecutive
rising PSA levels and a ≥25% increase from the baseline for PSA
non-responders.
Patients were divided into two groups (low/high)
according to the median expression level of each gene and PSA
response rate and TTP were compared between two treatment
groups.
Clinical assessments for safety, including clinical
laboratory evaluations and any adverse events, were principally
evaluated at baseline and every 4 weeks during the study and graded
using the Common Terminology Criteria for Adverse Events of the
National Cancer Institute, version 3.0.
Statistical methods
Categorical data were compared using the Wilcoxon
test or the Fisher’s exact test for proportion. The PSA response
rate as a primary end-point was compared between two treatment arms
with the Fisher’s exact test. The PSA percent change from baseline
to 12 weeks and the maximum PSA decline that occurred at any point
after each treatment was compared using the Wilcoxon test. TTP
analysis was performed using the Kaplan-Meier method and compared
between two treatment arms using the log-rank test. Hazard ratios
(HRs) with 95% confidence interval (CI) were calculated using the
Cox proportional hazard model. The distribution of the mRNA
expression levels of the enzymes in the two treatment arms was
compared using a t-test. P-values were two-sided, and p-values
<0.05 were considered statistically significant. The statistical
analyses were performed with JMP 9® or SAS
9.1.3® (SAS Institute Inc., Cary, NC, USA).
Results
Patients
Fifty-two patients were enrolled between February
2006 and November 2009 from 16 centers; 26 patients were randomly
assigned to receive SOA alone (group A), and 26 patients were
assigned to receive the combination therapy of SOA and
tegafur-uracil (group B).
The majority of patients in each group (group A,
76.9%; group B, 84.6%) had received a maximum androgen blockade
(MAB) with one prior anti-androgen at study enrollment. Only three
patients (11.5%) in group A and two patients (7.7%) in group B had
received two anti-androgens. There were no significant differences
between the two treatment groups with regards to the patient
characteristics including age at study entry, initial PSA level at
diagnosis, PSA level at study entry, stage at diagnosis, Gleason
score, prior therapy and number of anti-androgens (Table I). Bicalutamide was most frequently
used as a prior treatment, which was often switched to flutamide
after entry into the study (group A, 65.4%; group B, 80.8%).
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Treatment arms | Group Aa (n=26) | Group Bb (n=26) | P-value |
|---|
| Median age at study
entry, years | 77 (59–89) | 76.5 (47–92) | 0.993 |
| Median initial PSA,
ng/ml | 98.45
(5.8–15,168) | 311 (4.7–3,454) | 0.462 |
| Median PSA at study
entry, ng/ml | 5.1 (0.22–42.3) | 1.78
(0.17–111.0) | 0.151 |
| Stage at
diagnosis |
| B | 5 | 4 | 0.738 |
| C | 6 | 4 | |
| D1 | 1 | 3 | |
| D2 | 14 | 15 | |
| Gleason score |
| ≤6 | 4 | 3 | >0.999 |
| =7 | 3 | 4 | |
| ≥8 | 19 | 19 | |
| Prior therapy |
| LH-RH analogue
alone | 3 | 2 | >0.999 |
| MAB | 23 | 24 | |
| No. of prior
anti-androgen |
| 1 | 20 | 22 | >0.999 |
| 2 | 3 | 2 | |
| Sequence of
anti-androgens |
| BCL/FLT/CMA | 3 | 1 | 0.449 |
| CMA/BCL/FLT | 0 | 1 | |
| BCL/FLT | 17 | 20 | |
| BCL/CMA | 2 | 0 | |
| FLT/BCL | 0 | 1 | |
| CMA/BCL | 1 | 1 | |
| Add | BCL | 3 | 1 |
| Add | CMA | 0 | 1 |
PSA response rate
Nine of the 26 patients (34.6%) in group A and 16 of
the 26 patients (61.5%) in group B had a PSA response. Although
this difference was not statistically significant (p=0.095),
patients who received tegafur-uracil together with SOA tended to
have a higher PSA response rate (Table II).
| Table IIPSA response and clinicopathological
parameters. |
Table II
PSA response and clinicopathological
parameters.
| Clinical
parameters | Group Aa | Group Bb | P-value |
|---|
|
|
|---|
| No. | RR (%) | No. | RR (%) |
|---|
| All patients | 26 | 34.6 | 26 | 61.5 | 0.095 |
| Age, years |
| <77 | 12 | 33.3 | 13 | 53.8 | 0.428 |
| ≥77 | 14 | 35.7 | 13 | 69.2 | 0.128 |
| Stage |
| B, C | 11 | 45.5 | 8 | 75.0 | 0.352 |
| D1, D2 | 15 | 26.7 | 18 | 55.6 | 0.158 |
| Gleason |
| ≤6 | 4 | 75.0 | 3 | 66.7 | >0.999 |
| ≥7 | 22 | 27.3 | 23 | 60.9 | 0.036 |
The percent change in the PSA level from
baseline
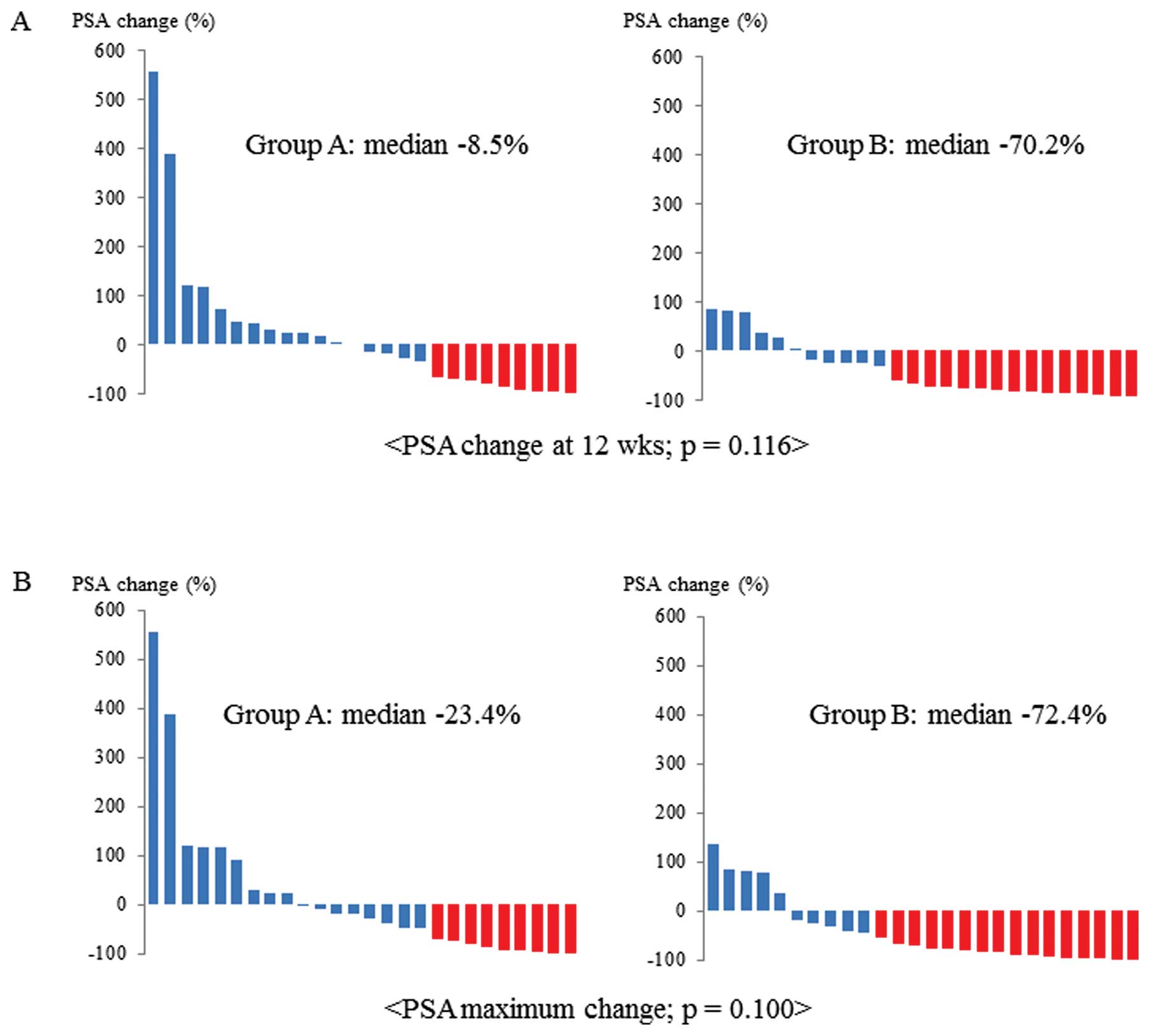
Half of the patients in group A had some PSA
decline, and the median percent change in the PSA level from
baseline to 12 weeks in group A was −8.5%. Seventy-seven percent of
the patients in group B had a PSA decline, and the median percent
change in the PSA level from baseline to 12 weeks in group B was
−70.2%. Although there was no significant difference between the
two treatment groups (p=0.116), patients treated with
tegafur-uracil together with SOA tended to have a greater PSA
decline (Fig. 1A).
The median maximum decline in PSA during treatment
was −23.4% in group A and −72.4% in group B. Though this difference
was also statistically non-significant (p=0.100), patients treated
with tegafur-uracil together with SOA tended to have a greater PSA
decline during the entire treatment period (Fig. 1B).
PSA response and clinicopathological
parameters
The PSA response rate was compared between the two
treatment groups in a subgroup divided according to each
clinicopathological parameter, such as age (<77 or ≥77), stage
(non-metastatic or metastatic), or Gleason score (≤6 or ≥7). The
combination therapy of tegafur-uracil and SOA demonstrated a better
PSA response rate than SOA alone in patients with higher Gleason
score (p=0.036) (Table II).
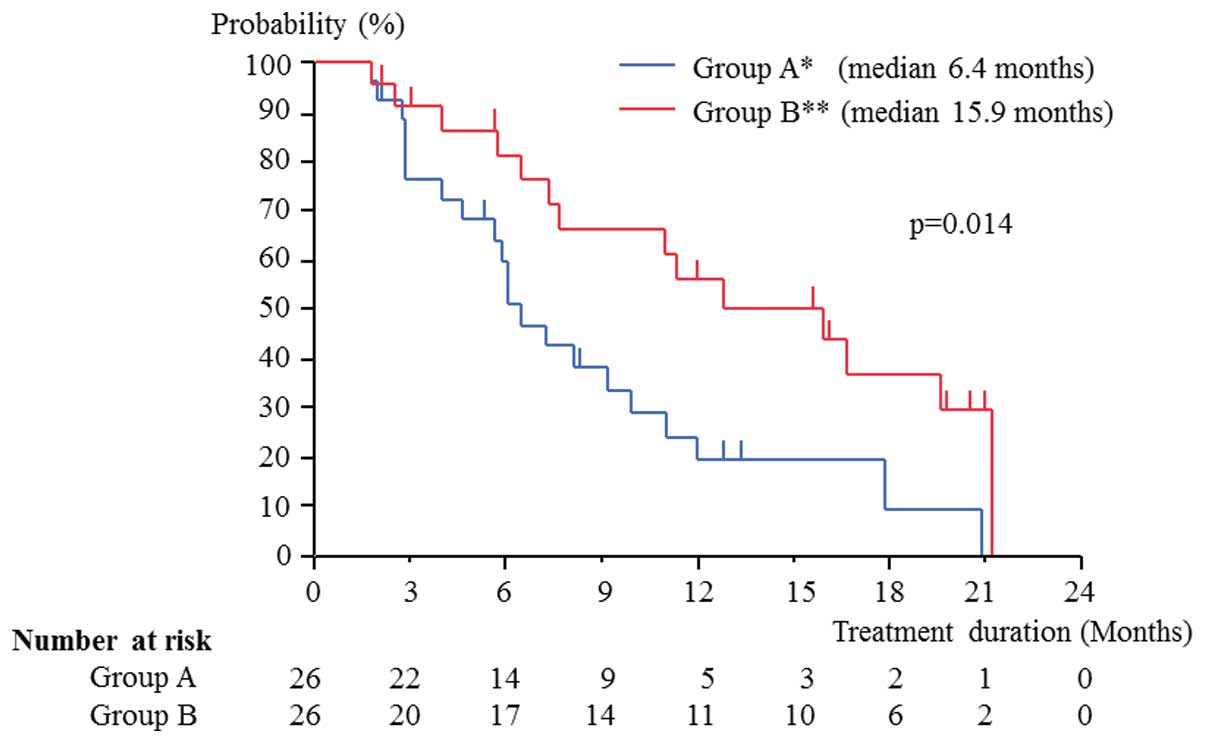
Time to PSA progression (TTP)
The TTP in group B was 15.9 months, which was
significantly longer than that (6.4 months) in group A (HR, 0.42;
95% CI: 0.20–0.85; p=0.014) (Fig.
2). Patients who received tegafur-uracil together with SOA had
a longer duration of PSA decline than patients treated with SOA
alone.
mRNA expression level of enzymes involved
in 5-FU metabolism and PSA response rate
mRNA expression level of enzymes involved in 5-FU
metabolism was measured in 49 patients because RNA of prostate
cancer cells in the remaining three patients was degraded. The
expression level distribution of genes encoding TS, DPD, OPRT and
TP was not different between the two treatment groups at the
diagnosis of prostate cancer (p=0.866, 0.776, 0.694 and 0.128,
respectively). The PSA response rate was compared between the two
treatment groups in a subgroup divided by the median expression
level of each gene. In patients with a lower TS expression and
those with a higher OPRT expression, the combination therapy
demonstrated significantly higher PSA response rate than the SOA
alone (p=0.019 and 0.041, respectively) (Table III).
| Table III5-FU metabolism-related mRNA
expression level and clinical response. |
Table III
5-FU metabolism-related mRNA
expression level and clinical response.
| | Group Aa | Group Bb | | TTP: Group
Bb vs. Group Aa |
|---|
| |
|
| |
|
|---|
| Gene | Expression
(x10−2) | No. | RR (%) | No. | RR (%) | P-value | HR (95% CI) | P-value |
|---|
| TS | <0.95 | 13 | 30.8 | 11 | 81.8 | 0.019 | 0.30
(0.10–0.83) | 0.018 |
| ≥0.95 | 12 | 33.3 | 13 | 46.2 | 0.688 | 0.48
(0.13–1.49) | 0.213 |
| DPD | <1.45 | 11 | 36.4 | 14 | 71.4 | 0.116 | 0.51
(0.18–1.40) | 0.172 |
| ≥1.45 | 14 | 28.6 | 10 | 50.0 | 0.403 | 0.35
(0.08–1.16) | 0.103 |
| TP | <4.83 | 14 | 42.9 | 10 | 80.0 | 0.104 | 0.38
(0.13–1.04) | 0.057 |
| ≥4.83 | 11 | 18.2 | 14 | 50.0 | 0.208 | 0.47
(0.14–1.37) | 0.166 |
| OPRT | <4.89 | 12 | 50.0 | 12 | 66.7 | 0.680 | 0.43
(0.14–1.23) | 0.113 |
| ≥4.89 | 13 | 15.4 | 12 | 58.3 | 0.041 | 0.36
(0.10–1.08) | 0.072 |
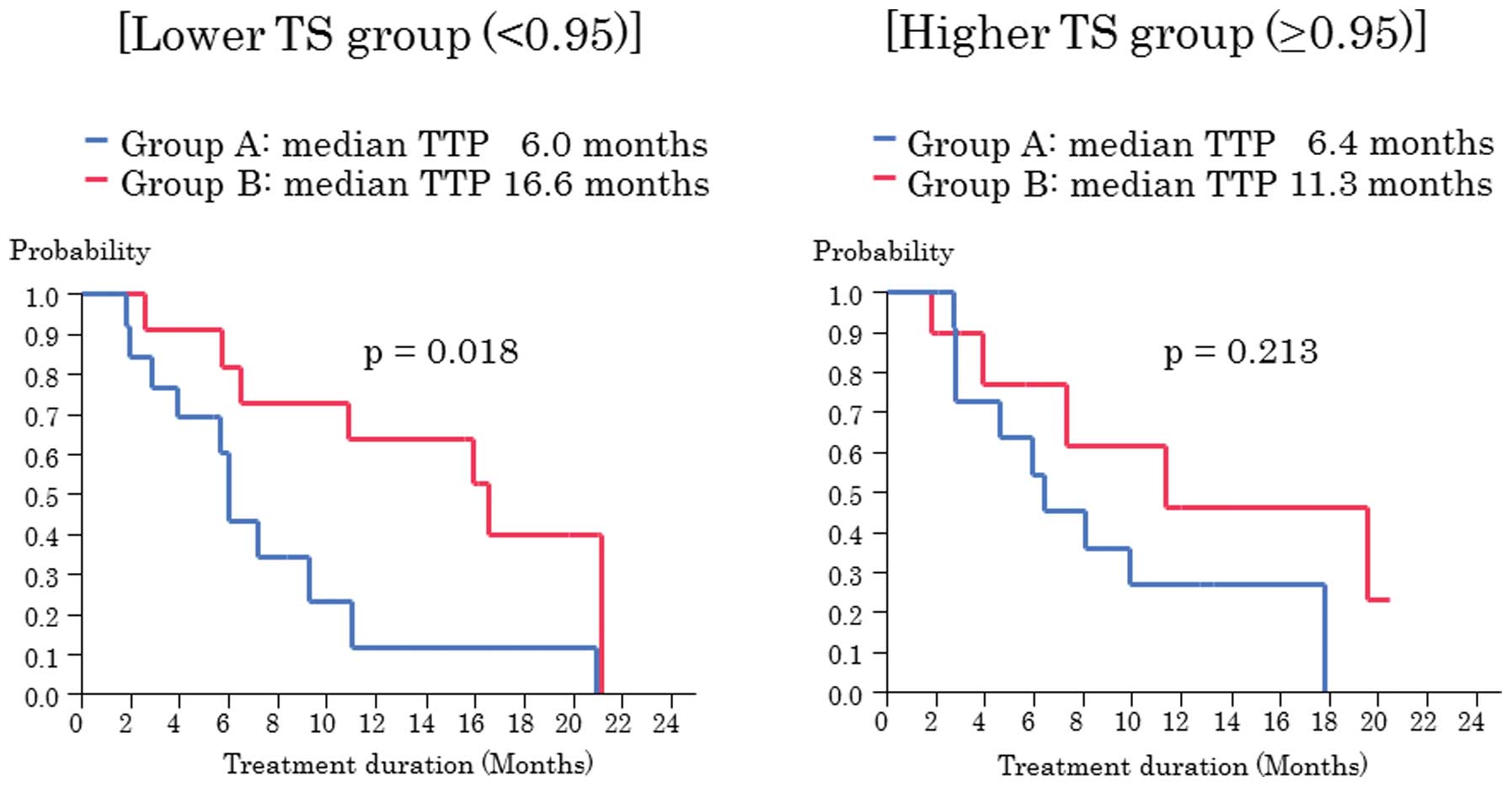
TS expression level and time to PSA
progression (TTP)
When we examined the correlation of TTP and gene
expression levels, patients with a lower TS level in group B had a
significantly longer TTP than those in group A (16.6 vs. 6.0
months, HR, 0.30; 95% CI: 0.10–0.83; p=0.018). However, the TTP was
not significantly different in patients with a higher TS level
(11.3 vs. 6.4 months; HR, 0.48; 95% CI: 0.13–1.49; p=0.213)
(Table III, Fig. 3). These data suggest that
tegafur-uracil combined with SOA may be more effective when
prostate cancer cells express a low TS level.
Safety
Most adverse events (AEs) were grade 1/2. Diarrhea
(grade 1, 7.7%) and ALT/AST elevation (grade 1/2, 7.7%) were
observed in group A. ALT/AST elevation (grade 1/2, 7.7%), fatigue
(grade 1/2, 11.5%), appetite loss (grade 2, 3.8%), nausea (grade 1,
3.8%) and elevation of total bilirubin (grade 3, 3.8%) were
reported in group B. Severe adverse events (AEs) were not observed
in either treatment group. Although one patient in group B had a
grade 3 elevation of total bilirubin, it spontaneously decreased to
normal range after the discontinuation of tegafur-uracil. One
patient in group A and seven patients in group B discontinued
treatment. However, the treatment was discontinued due to patients
request regardless of the mild AEs in all but one patient who had a
grade 3 elevation in the total bilirubin.
Discussion
The majority of advanced prostate cancers relapse
from initial hormonal therapy. Recently, docetaxel has been
approved for castration-resistant prostate cancer as an effective
chemotherapeutic agent compared with mitoxantrone in two pivotal
studies (15,16). In the group given docetaxel every
three weeks with prednisone, the incidence of grades 3 and 4
neutropenia was relatively low (32%), and febrile neutropenia was
rare (3%) (16). In the group
given docetaxel and estramustine, the rate of grades 3–5
neutropenia was 16.1%, and grades 3 and 4 neutropenic fevers were
more common than those in the mitoxantrone group (15). In contrast, in a multicenter phase
II trial of docetaxel and prednisone in Japan, the rate of grades 3
and 4 neutropenia was 93%, and 16.3% of the patients had grades 3
or 4 febrile neutropenia, although a high response rate (44.2%) was
achieved (17).
Although docetaxel has also been the standard
treatment for castration-resistant prostate cancer in Japan, the
phenomenon of an aging population is remarkable compared with other
countries, and there are quite a few older patients with prostate
cancer, which may explain the higher rates of high grade
neutropenia and febrile neutropenia. Therefore, more attention
should be focused on Japanese patients with castration-resistant
prostate cancer when docetaxel administration is considered.
SOA has often been attempted for patients who
relapse from initial hormonal therapy in Japan. Although SOA is
effective and could delay the introduction of docetaxel, its
efficacy was relatively low with a PSA response rate of 25–40%, and
the efficacy duration was not long (4–6 months) (1–3).
Therefore, we conducted a multi-center randomized
phase II study to examine the efficacy and safety of tegafur-uracil
and SOA combination therapy compared with SOA alone. We have
demonstrated a higher PSA response rate in the group given
tegafur-uracil and SOA than the group given SOA alone. In addition,
the PSA percent change from baseline to 12 weeks and the maximum
PSA decline were greater for the combination therapy group.
Although the data were not significantly different, they may be the
result of a small sample size. Nevertheless, the TTP was
significantly longer in the combination therapy group than in the
SOA group, indicating a greater efficacy for the combination
therapy.
When we examined the correlation of PSA response
rate with clinicopathological parameters, the combination therapy
demonstrated significantly higher PSA response rate than SOA alone
in patients with higher Gleason score. This finding may suggest the
combination therapy is more effective for more aggressive prostate
cancer. However, as only a few patients had prostate cancer with
Gleason score ≤6 in this study, it should be confirmed by examining
more patients.
We found that the combination therapy demonstrated a
higher PSA response rate in patients with a lower TS expression or
those with a higher OPRT expression among four 5-FU-related enzymes
including TS, DPD, TP, and OPRT. In addition, in patients with a
lower TS expression, the combination therapy demonstrated a
significantly longer TTP than SOA alone. Inversely, Longley et
al have demonstrated that TS overexpression confers increased
resistance to TS inhibitors such as 5-FU by abrogating S-phase
arrest in a breast cancer-derived cell line (18). In other words, DNA synthesis should
be efficiently blocked by 5-FU in the environments where the TS
level is low. In addition, as a higher OPRT enzyme activity was
observed in 5-FU-sensitive tissues than non-sensitive ones in in
vitro chemosensitivity test in studies using human colorectal
cancer tissues (19,20), our results appear to be consistent
with those of the aforementioned studies. Especially, the TS mRNA
expression level in prostate cancer cells at diagnosis may predict
the efficacy of the tegafur-uracil and SOA combination therapy.
The majority of patients were switched from
bicalutamide to flutamide after they relapsed from the initial
hormonal therapy in this study. We recently established a
bicalutamide-resistant prostate cancer subline, CDX25R, and
demonstrated that the combined treatment of 5-FU and
hydroxyflutamide (OH-flutamide), the active metabolite of
flutamide, had a synergistic effect on CDX25R cells (21). In addition, we found that
OH-flutamide decreased the expression of the E2F1 transcription
factor followed by a decreased TS expression in CDX25R cells as the
underlying mechanism. Because the TS expression in AR negative
DU-145 cells was not affected by anti-androgens, it may be
suggested that OH-flutamide enhanced the growth-inhibitory activity
of 5-FU in CDX25R cells by reducing the TS expression through the
AR pathway.
There are several limitations to this study. Because
this study began before the recommendations from the Prostate
Cancer Clinical Trials Working Group (PCWG2) (22) were published, a measurable lesion
by RECIST was not an eligibility criteria requirement, and the PSA
change was particularly focused on as the treatment efficacy in
this study. In addition, 23 of the 52 evaluable patients (44%) had
a PSA level lower than 2 ng/ml at the start of the study. Because
an early PSA increase does not always indicate disease progression
in castration-resistant prostate cancer, some patients in this
study may not have reflected true disease progression and shown
actual treatment efficacy. However, because tegafur-uracil is a
mild chemotherapeutic agent with a cytostatic effect, it is
unlikely to show a significant shrinkage in the target lesions.
Some patients may request a change in treatment prior to their PSA
levels reaching 2 ng/ml in a clinical setting. Nonetheless, the
results in this study warrant further examination with more
patients because this study was conducted in a prospective
randomized fashion.
The tegafur-uracil and SOA combination therapy did
not cause severe adverse events and proved to be safe although more
patients discontinued the combination therapy due to mild adverse
events.
We conclude that this combination therapy may be a
treatment option before the introduction of chemotherapies such as
docetaxel, particularly when more severe adverse events are
expected in older patients. However, further investigation is
required with more patients to elucidate whether the combination
therapy could actually be an effective treatment option.
Acknowledgements
We thank the investigators at the following
participating institutions: The University of Tokushima Graduate
School, Sanuki Municipal Hospital, Tokushima Municipal Hospital,
Tsurugi Municipal Hospital, Tokushima Prefectural Central Hospital,
Tokushima Prefecture Naruto Hospital, Kamei Hospital, Oe Kyodou
Hospital, Anan Central Hospital of the Medical Association,
Tokushima Prefectural Miyoshi Hospital, Kaisei Hospital, National
Hospital Organization Zentsuji National Hospital, Japanese Red
Cross Takamatsu Hospital, Yashima General Hospital, Japanese Red
Cross Kochi Hospital and Kochi Takasu Hospital. This study was
conducted under financial support of TAIHO Pharmaceutical Co. Ltd.
(trial registration ID: UMIN000009181).
References
|
1
|
Kojima S, Suzuki H, Akakura K, Shimbo M,
Ichikawa T and Ito H: Alternative antiandrogens to treat prostate
cancer relapse after initial hormone therapy. J Urol. 171:679–683.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Okihara K, Ukimura O, Kanemitsu N,
Mizutani Y, Kawauchi A and Miki T: Clinical efficacy of alternative
antiandrogen therapy in Japanese men with relapsed prostate cancer
after first-line hormonal therapy. Int J Urol. 14:128–132. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Suzuki H, Okihara K, Miyake H, et al:
Alternative nonsteroidal antiandrogen therapy for advanced prostate
cancer that relapsed after initial maximum androgen blockade. J
Urol. 180:921–927. 2008. View Article : Google Scholar
|
|
4
|
Kato H, Ichinose Y, Ohta M, et al: A
randomized trial of adjuvant chemotherapy with uracil-tegafur for
adenocarcinoma of the lung. N Engl J Med. 350:1713–1721. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nakajima T, Kinoshita T, Nashimoto A, et
al: Randomized controlled trial of adjuvant uracil-tegafur versus
surgery alone for serosa-negative, locally advanced gastric cancer.
Br J Surg. 94:1468–1476. 2007. View
Article : Google Scholar
|
|
6
|
Kuriyama M, Takahashi Y, Sahashi M, et al:
Prospective and randomized comparison of combined androgen blockade
versus combination with oral UFT as an initial treatment for
prostate cancer. Jpn J Clin Oncol. 31:18–24. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ichikawa W, Uetake H, Shirota Y, et al:
Combination of dihydropyrimidine dehydrogenase and thymidylate
synthase gene expressions in primary tumors as predictive
parameters for the efficacy of fluoropyrimidine-based chemotherapy
for metastatic colorectal cancer. Clin Cancer Res. 9:786–791.
2003.
|
|
8
|
Salonga D, Danenberg KD, Johnson M, et al:
Colorectal tumors responding to 5-fluorouracil have low gene
expression levels of dihydropyrimidine dehydrogenase, thymidylate
synthase, and thymidine phosphorylase. Clin Cancer Res.
6:1322–1327. 2000.
|
|
9
|
Suda Y, Kuwashima Y, Tanaka Y, Uchida K
and Akazawa S: Immunohistochemical detection of thymidylate
synthase in advanced gastric cancer: a prognostic indicator in
patients undergoing gastrectomy followed by adjuvant chemotherapy
with 5-fluoropyrimidines. Anticancer Res. 19:805–810. 1999.
|
|
10
|
Metzger R, Danenberg K, Leichman CG, et
al: High basal level gene expression of thymidine phosphorylase
(platelet-derived endothelial cell growth factor) in colorectal
tumors is associated with nonresponse to 5-fluorouracil. Clin
Cancer Res. 4:2371–2376. 1998.
|
|
11
|
Ichikawa W, Uetake H, Shirota Y, et al:
Both gene expression for orotate phosphoribosyltransferase and its
ratio to dihydropyrimidine dehydrogenase influence outcome
following fluoropyrimidine-based chemotherapy for metastatic
colorectal cancer. Br J Cancer. 89:1486–1492. 2003. View Article : Google Scholar
|
|
12
|
Fukushima M, Morita M, Ikeda K and
Nagayama S: Population study of expression of thymidylate synthase
and dihydropyrimidine dehydrogenase in patients with solid tumors.
Int J Mol Med. 12:839–844. 2003.PubMed/NCBI
|
|
13
|
Hugosson J, Bergdahl S, Carlsson G,
Frosing R, Norlen L and Gustavsson B: Effects of intravesical
instillation of 5-fluorouracil and interferon in patients with
recurrent superficial urinary bladder carcinoma. A clinical and
pharmacodynamic study. Scand J Urol Nephrol. 31:343–347. 1997.
View Article : Google Scholar
|
|
14
|
Nomura T, Nakagawa M, Fujita Y, Hanada T,
Mimata H and Nomura Y: Clinical significance of thymidylate
synthase expression in bladder cancer. Int J Urol. 9:368–376. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Petrylak DP, Tangen CM, Hussain MH, et al:
Docetaxel and estramustine compared with mitoxantrone and
prednisone for advanced refractory prostate cancer. N Engl J Med.
351:1513–1520. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tannock IF, de Wit R, Berry WR, et al:
Docetaxel plus prednisone or mitoxantrone plus prednisone for
advanced prostate cancer. N Engl J Med. 351:1502–1512. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Naito S, Tsukamoto T, Koga H, et al:
Docetaxel plus prednisolone for the treatment of metastatic
hormone-refractory prostate cancer: a multicenter Phase II trial in
Japan. Jpn J Clin Oncol. 38:365–372. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Longley DB, Ferguson PR, Boyer J, et al:
Characterization of a thymidylate synthase (TS)-inducible cell
line: a model system for studying sensitivity to TS- and
non-TS-targeted chemotherapies. Clin Cancer Res. 7:3533–3539.
2001.PubMed/NCBI
|
|
19
|
Isshi K, Sakuyama T, Gen T, et al:
Predicting 5-FU sensitivity using human colorectal cancer
specimens: comparison of tumor dihydropyrimidine dehydrogenase and
orotate phosphoribosyl transferase activities with in vitro
chemosensitivity to 5-FU. Int J Clin Oncol. 7:335–342. 2002.
View Article : Google Scholar
|
|
20
|
Fujii R, Seshimo A and Kameoka S:
Relationships between the expression of thymidylate synthase,
dihydropyrimidine dehydrogenase, and orotate
phosphoribosyltransferase and cell proliferative activity and
5-fluorouracil sensitivity in colorectal carcinoma. Int J Clin
Oncol. 8:72–78. 2003. View Article : Google Scholar
|
|
21
|
Kawabata R, Oie S, Oka T, Takahashi M,
Kanayama H and Itoh K: Hydroxyflutamide enhances cellular
sensitivity to 5-fluorouracil by suppressing thymidylate synthase
expression in bicalutamide-resistant human prostate cancer cells.
Int J Oncol. 38:665–676. 2011. View Article : Google Scholar
|
|
22
|
Scher HI, Halabi S, Tannock I, et al:
Design and end-points of clinical trials for patients with
progressive prostate cancer and castrate levels of testosterone:
recommendations of the Prostate Cancer Clinical Trials Working
Group. J Clin Oncol. 26:1148–1159. 2008. View Article : Google Scholar
|