Introduction
Breast cancer is the most common female cancer in
the United States (1). The
mortality of breast cancer has been decreasing over the last two
decades due to early detection and incremental improvements in
systemic therapy. Adjuvant chemotherapy reduces the risk of
recurrence and prolongs survival (2). Increasingly, these same chemotherapy
regimens are used in the neoadjuvant setting for the patients with
locally advanced breast cancer or high-risk biology (3–5).
Regarding the clinical response to chemotherapy, the presence of
pathological complete response (pCR) (defined as no cancer cells in
the breast and axilla lymph nodes at the time of surgical
resection) is associated with improved disease-free and overall
survival (4,6). Conversely, patients with residual
disease post-chemotherapy have a significantly higher risk of
disease recurrence (6).
The presence of immune cells in tumor tissues has
repeatedly been associated with response to chemotherapy (7). In particular, tumor-infiltrating T
lymphocytes (TILs) are often observed in solid tumors and are
associated with improved survival of cancer patients (8). However, the tumor immunity is
governed in a complex network between antitumoral and pro-tumoral
immune cells and molecules. For example, TILs consist of various
lymphocyte subtypes with different roles such as elimination of
cancer cells (e.g. CD8+ cytotoxic T cell (CTL) and
CD4+ helper T cells) or protection of cancer cells from
host immune attack [e.g. CD4+FoxP3+
regulatory T cell (Treg)]. In general, a higher level of
CD8+ T cell infiltration is thought to contribute to
better prognoses of patients with solid tumors (8). A meta-analysis focusing on breast
cancer showed that higher TIL numbers in pre-treatment biopsies was
associated with higher CR rates to neoadjuvant chemotherapy (NAC),
while more FoxP3+ Treg cells in post-treatment breast
tissue were associated with lower CR rates (9). However, most studies have simply
quantified the number of T lymphocytes in tumor tissues, but their
clonality and temporal changes in T cell repertoire during the
treatment have not been well investigated. In this regard, a recent
study revealed that clonal expansion of TILs was associated with
better response to a PD-1 (programmed death-1) blockade
(pembrolizumab) treatment in human melanoma patients (10). Therefore comprehensive
characterization of TILs during cancer treatment is imperative to
identify a predictive immune biomarker.
However, T lymphocytes are an extremely
heterogeneous immune cell population, due to the molecular
diversity in the T cell receptor (TCR) (11). Most T cells express TCR consisting
of a heterodimer of α (TCRA) and β (TCRB) chains. Both TCRA and
TCRB are generated through genetic rearrangement between V-J (for
TCRA) and V-D-J (for TCRB) segments. In addition, since nucleotides
are randomly deleted from V, (D), J exons and/or inserted between a
V-J junction (for TCRA), or V-D and D-J junctions (for TCRB) during
recombination (11–14), a huge variety in TCRs has hindered
detailed characterization of the T cell-mediated adaptive
immunity.
For the comprehensive analysis of immune functions
of TILs, we have established TCR repertoire analysis employing
next-generation sequencing technologies (15–20).
In this study, we investigated expression levels of immune-related
genes as well as the TCR repertoire of TILs in breast tumors in
order to characterize the T-cell mediated antitumor immunity that
is associated with clinical response to NAC.
Materials and methods
Clinical specimens
This study includes breast cancer patients who had
been treated with neoadjuvant chemotherapy. Fresh tumor biopsy
samples and surgically resected tumors were collected at Mayo
Clinic (MC-1 to MC-9) as previously described (21), Tokushima Breast Care Clinic (TK-1
to TK-6), and Hyogo College of Medicine (HG-1 to HG-4). In case of
patients who showed CR to chemotherapy, the tumor bed where tumor
had been detected was collected. All human clinical specimens were
obtained according to a study protocol and informed consent
procedures approved by Institutional Review Board of each
institution. Tumor samples were transferred to the University of
Chicago and subsequently TCR repertoire was analyzed under the
University of Chicago IRB protocol 13-0797. Detailed clinical
information is described in Table
I.
 | Table IClinical information of 19 female
breast cancer patients. |
Table I
Clinical information of 19 female
breast cancer patients.
| Patient | Response | Age | Subtype | Ki67 (%) | | Chemotherapy |
|---|
| MC-1 | SD/PD | 59 | TNBC | 43 | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| MC-2 | PR | 35 |
ER−/HER2+ | ND | | Paclitaxel +
Trastuzumab → Adriamycin/Cyclophosphamide |
| MC-3 | SD/PD | 60 | Luminal B | 5 | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| MC-4 | PR | 48 | TNBC | 6 | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| MC-5 | SD/PD | 35 |
ER+/HER2+ | 11 | | Paclitaxel +
Trastuzumab → Adriamycin/Cyclophosphamide |
| MC-6 | CR | 70 | TNBC | ND | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| MC-7 | PR | 38 | TNBC | 75 | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| MC-8 | CR | 54 | TNBC | ND | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| MC-9 | PR | 53 | TNBC | 6 | | Paclitaxel →
Adriamycin/Cyclophosphamide |
| Patient | Response | Age | ER (%) | PgR (%) | HER2 | Chemotherapy |
| TK-1 | SD/PD | 67 | 80 | 0 | 2+ |
Epirubicin/Cyclophosphamide →
Docetaxel |
| TK-2 | PR | 63 | 20 | 0 | 3+ |
Epirubicin/Cyclophosphamide → Docetaxel +
Trastuzumab |
| TK-3 | CR | 64 | 0 | 0 | 2+ |
Epirubicin/Cyclophosphamide → Paclitaxel +
Trastuzumab |
| TK-4 | PR | 56 | 1 | <1 | 2+ |
Epirubicin/Cyclophosphamide →
Docetaxel |
| TK-5 | PR | 46 | <1 | <1 | 3+ |
Epirubicin/Cyclophosphamide → Paclitaxel +
Trastuzumab |
| TK-6 | CR | 64 | 0 | 0 | 3+ |
Epirubicin/Cyclophosphamide → Paclitaxel +
Trastuzumab |
| HG-1 | PR | 48 | 2 | 1 | - |
Epirubicin/Cyclophosphamide + Capecitabine
→ Docetaxel + Capecitabine |
| HG-2 | PR | 57 | 0 | 0 | - |
Epirubicin/Cyclophosphamide + Capecitabine
→ Docetaxel + Capecitabine |
| HG-3 | PR | 71 | 90 | 10 | - |
5-Fluorouracil/Epirubicin/Cyclophosphamide
→ Docetaxel |
| HG-4 | CR | 40 | 0 | 0 | - |
Epirubicin/Cyclophosphamide + Capecitabine
→ Docetaxel + Capecitabine |
RNA isolation and cDNA library
preparation
The next generation sequencing technology-based TCR
repertoire analysis was done as previously described (16,17).
Briefly, total RNA was extracted from tumor sample using RNeasy
mini kit (Qiagen, Valencia, CA, USA), and cDNA was synthesized by
SMART (Switching Mechanism At 5′ end of RNA Transcript) cDNA
library construction kit (Clontech, Mountain View, CA, USA). PCR
reactions were performed to amplify compatible amplicon libraries
of TCRβ with the Ion Torrent sequencing platform (Life
Technologies, Carlsbad, CA, USA). A forward primer
(5′-CCTCTCTATGGGCAGTCGGTGATTATCAACGCAGAGTGGCCAT-3′) was designed
for the sequence of the SMART IV adaptor and the P1 adaptor. A
reverse primer (5′-CCATCTCATCCCTGCGTGTCTCCGACTCAGCAGAAGGAACGATTCTGATGGCTCAAACACAGC-3′)
was designed for the constant region of TCRβ, including the A1
adaptor sequence. Underline indicates the IonXpress barcode
sequences. PCR reaction was performed as follows: 3 min at 94°C; 40
cycles of 30 sec at 94°C, 30 sec at 65°C, and 35 sec at 68°C.
Amplified PCR products were purified using AMPure XP reagent
(Beckman Coulter, Brea, CA, USA) and products of 300–900 bp were
selected by Pippin Prep system (Sage Science, Beverly, MA, USA).
Finally, we measured the concentration of size-selected PCR
products by Agilent 2200 TapeStation System (Agilent, Santa Clara,
CA, USA).
TCR repertoire sequencing
The sequencing libraries for TCRβ were amplified
onto the proprietary Ion Sphere particles (ISP) by emulsion PCR
using the Ion PGM™ Template OT2 400 kit and the OneTouch2 system
(Life Technologies), as previously described (16,17).
After enrichment and purification of the template-bound ISPs, the
final ISP products were sequenced using the Ion 314v2 Chip, Ion
Sequencing 400 kit, and Ion PGM Sequencer (Life Technologies),
according to the manufacturer's instructions.
TCR repertoire analysis
Sequencing reads of TCRβ were produced in the FASTQ
format and mapped to the reference sequences derived from the
IMGT/GENE-DB (http://www.imgt.org), using the Bowtie2
aligner (Version 2.1.0) (22,23).
After decomposition of V, D, and J segments, the CDR3 region was
defined from a conserved cysteine encoded in the 3′ portion of the
V segment to a conserved phenylalanine encoded in the 5′ portion of
the J segment. The nucleotide sequences between the conserved TCR-V
cysteine and TCR-J phenylalanine were extracted to determine the
amino acid sequence of CDR3 region (24). Using the identified CDR3
clonotypes, we calculated the Simpson's diversity index to quantify
the clonality of the TCRβ repertoires, as we previously described
(15,18). For data visualization, we used the
Excel program (Microsoft, Redmond, WA, USA) to generate bar graphs
and pie charts of TCR repertoire.
Quantitative RT-PCR
To examine expression levels of immune signature
genes, we conducted quantitative RT-PCR from the tumor and tumor
bed cDNAs using TaqMan Gene Expression assays (Thermo Fisher
Scientific, Carlsbad, CA, USA) and ABI ViiA 7 system (Applied
Biosystems, Foster City, CA, USA), according to the manufacturer's
instructions. The TaqMan probes for CD4, CD8, FoxP3, IDO1,
PD-1 and PD-L1 genes were purchased from Life
Technologies. Samples were run in triplicate reactions using one
FAM and VIC-labeled probes per reaction. A probe for GAPDH
was used for data normalization.
Statistical analysis
To compare patient groups of CR, PR, and SD/PD, we
conducted the Mann Whitney test to examine any difference in the
expression levels of immune-related genes. A p-value of <0.05
was considered statistically signifi-cant. Analysis was carried out
using the Prism 6 software (GraphPad, San Diego, CA, USA).
Results
Antitumoral immune microenvironment in
the tumors of CR patients
In this study, we obtained pre- and post-treatment
cancer tissues from 19 breast cancer patients treated with NAC.
Five cases showed complete response (CR), ten cases showed partial
response (PR), and four had stable disease/progressive disease
(SD/PD) to NAC (Table I). In the
case of patients who showed CR, we collected tissue samples derived
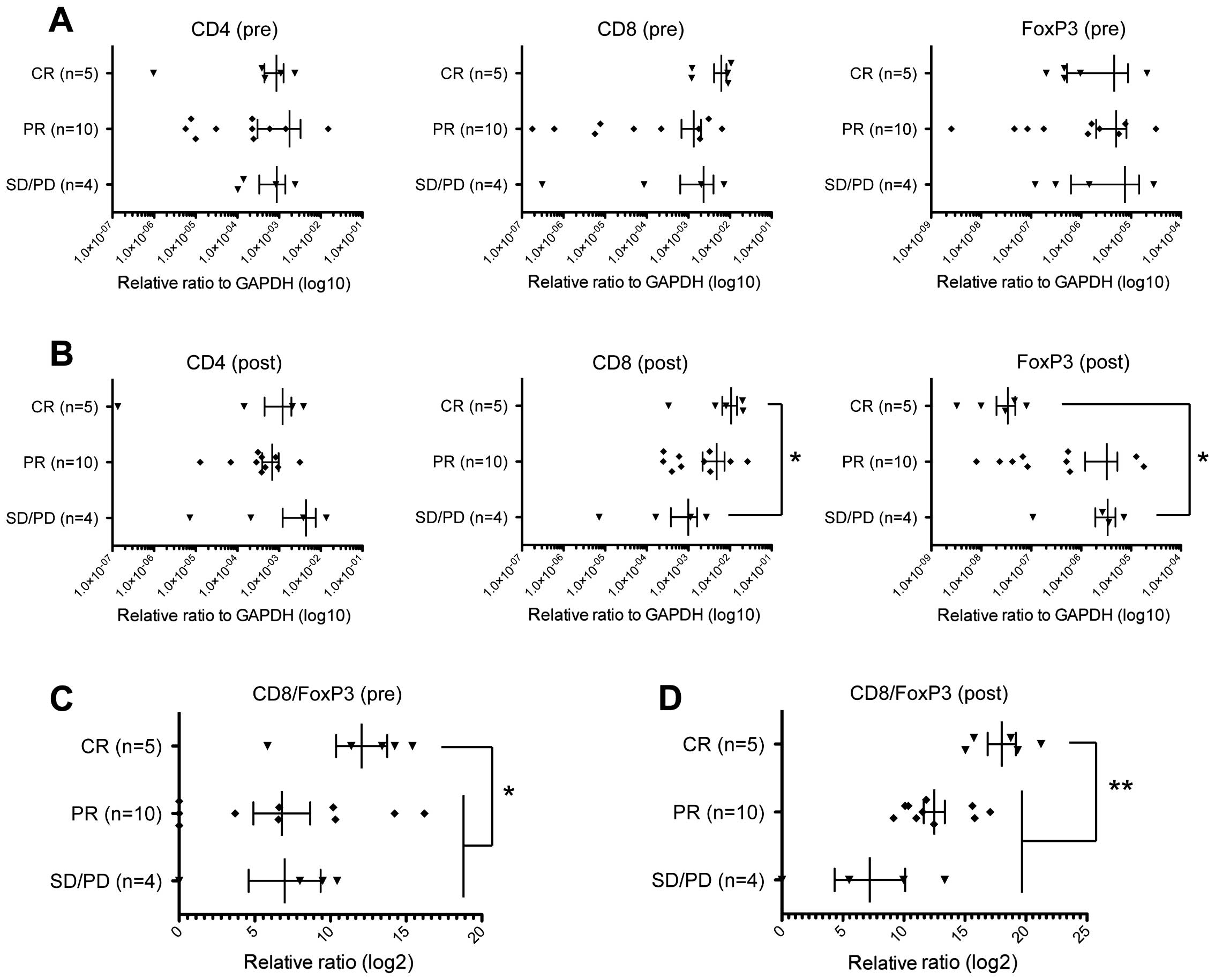
from the tumor bed. At first, we examined chemotherapy-induced
changes of the immune microenvironment based on expression levels
of CD4, CD8, and Foxp3. In pre-NAC tumors, we found
no significant differences comparing CD4, CD8, and
FoxP3 expression levels among the three patient groups
(Fig. 1A). CD8 expression
levels in the post-NAC tumor tissues of CR cases were significantly
higher than those in SD/PD cases (p=0.0317, Mann Whitney test)
(Fig. 1B), indicating that
stronger infiltration of CD8+ CTLs during NAC
contributed to effective elimination of cancer cells. On the
contrary, expression levels of Foxp3 in post-NAC tissues
were significantly lower in CR cases than in SD/PD cases (p=0.0159,
Mann Whitney test) (Fig. 1B).
Concordantly, the CD8/FoxP3 expression ratios in the tumors
of CR cases were higher than those of PR or SD/PD cases before NAC
(p=0.0349, Mann Whitney test) (Fig.
1C) as well as after NAC (p=0.0032, Mann Whitney test)
(Fig. 1D). These results indicated
that reduction of FoxP3+ Tregs by a certain mechanism
might also contribute to achieving complete elimination of tumors
and supporting the idea that immune responses in tumor tissues are
likely to play critical roles even in chemotherapy response
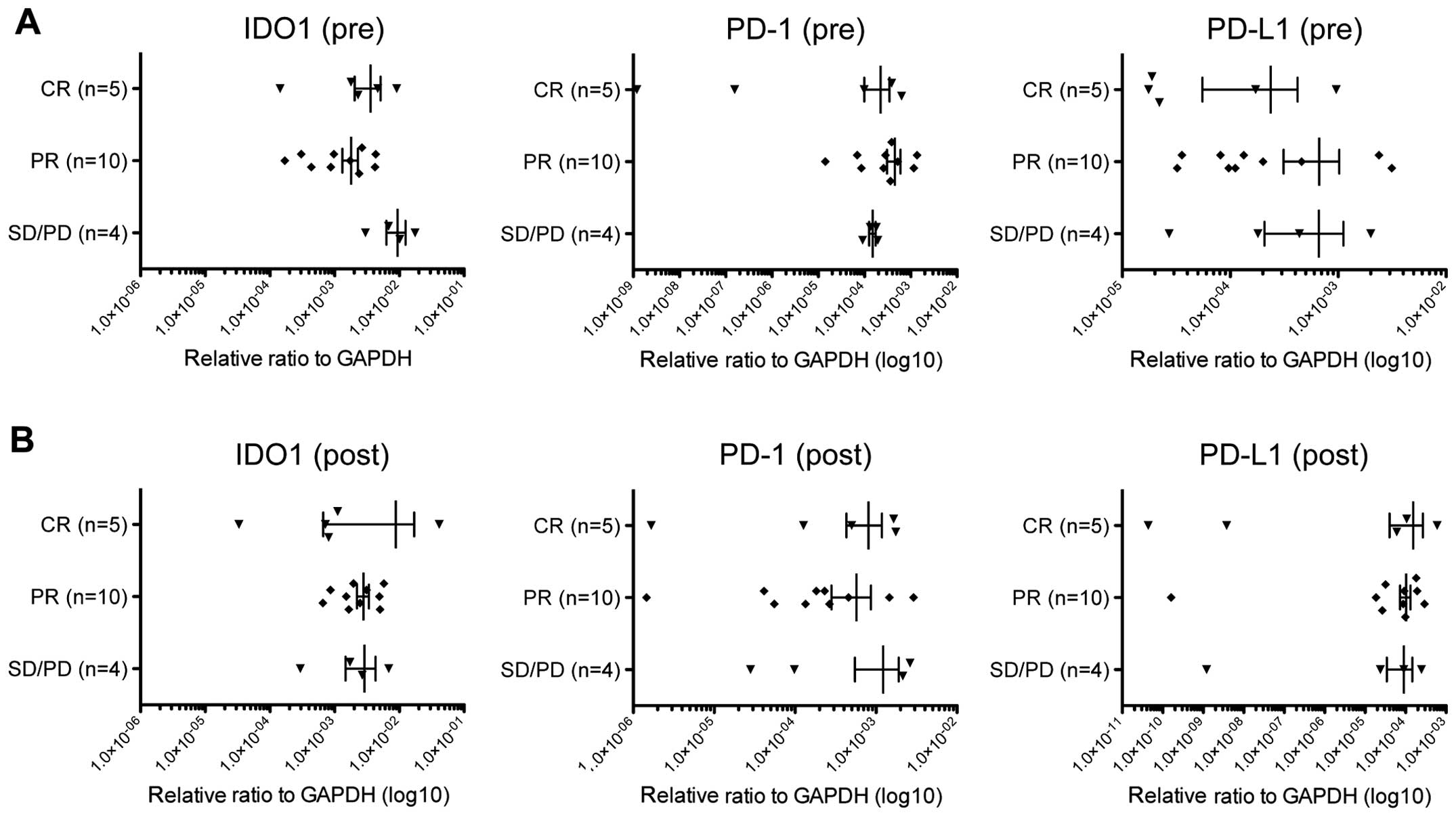
(25). We could not observe any
difference in expression levels of other immune suppressive
molecules, IDO1, PD-1 and PD-L1 among CR, PR, and
SD/PD tumors (Fig. 2).
Chemotherapy induces changes in TCR
repertoire
To further characterize infiltrated T cells in
breast tumors, we performed TCR repertoire analysis using the next
generation sequencing technologies. We isolated RNA from tumor
tissue samples, generated TCRB cDNA, performed PCR amplification,
and then sequenced with the Ion Torrent PGM sequencer.
Subsequently, we performed quantitative analysis for the frequency
of individual TCRB clonotypes with a unique V-D-J combination and
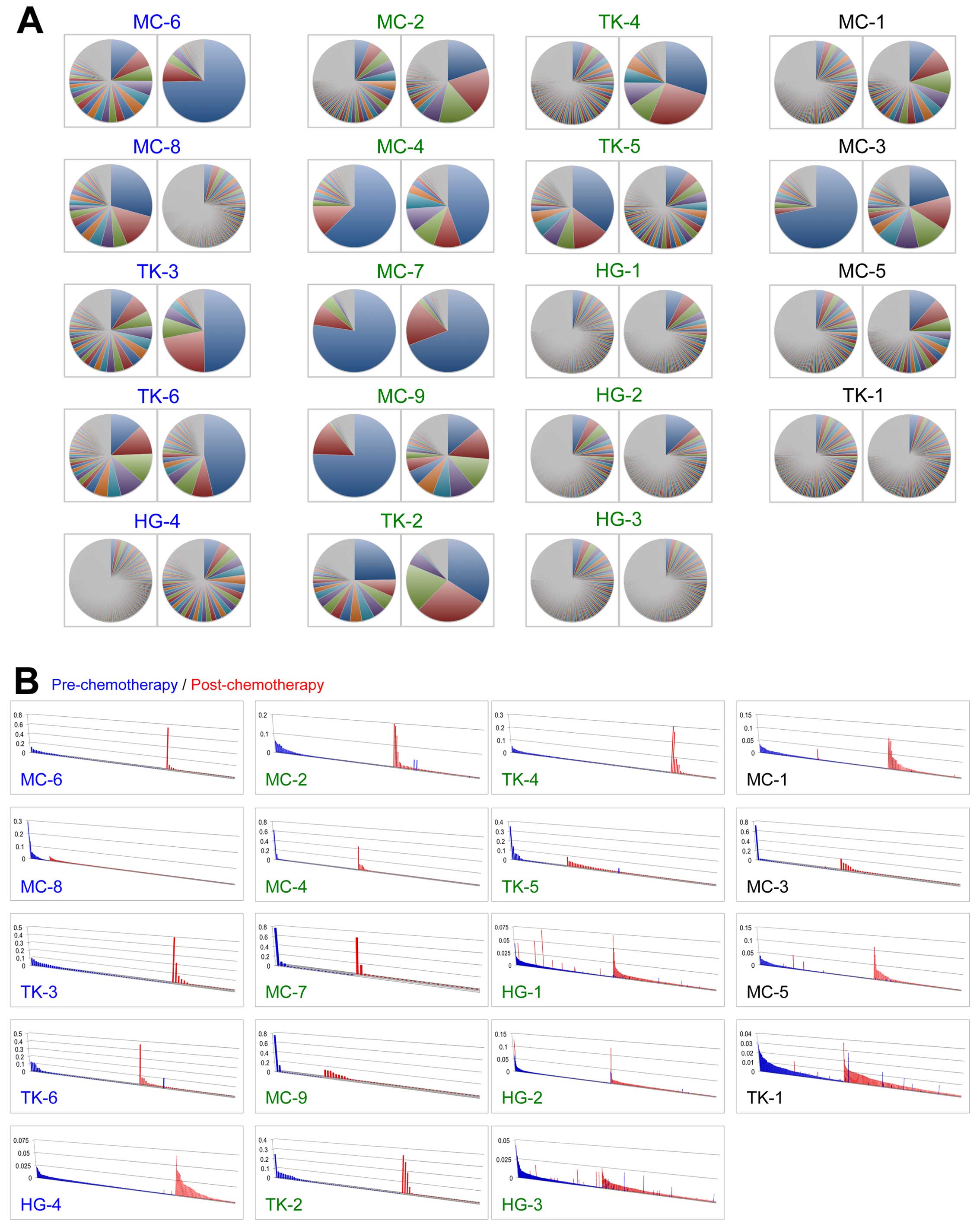
CDR3 sequences, and compared TCR repertoire in tumors of pre- and
post-NAC. Of note, the TCRB repertoire was markedly changed during
NAC and we observed in some cases significant expansion of certain
clonotypes through the NAC (Fig.
3A). Next, we focused on unique clonotypes with the read
frequency of >0.001 and found that TILs with some unique
clonotypes were significantly increased or decreased during the NAC
(Fig. 3B), implying that cancer
cell death by the neoadjuvant chemotherapy might influence the T
cell population in tumors.
Clonal expansion of antitumor T cells in
the tumors of CR patients
To assess the chemotherapy-induced changes in TIL
population, we employed a statistical approach to measure
significance of the temporal clonal changes in the identified TCR
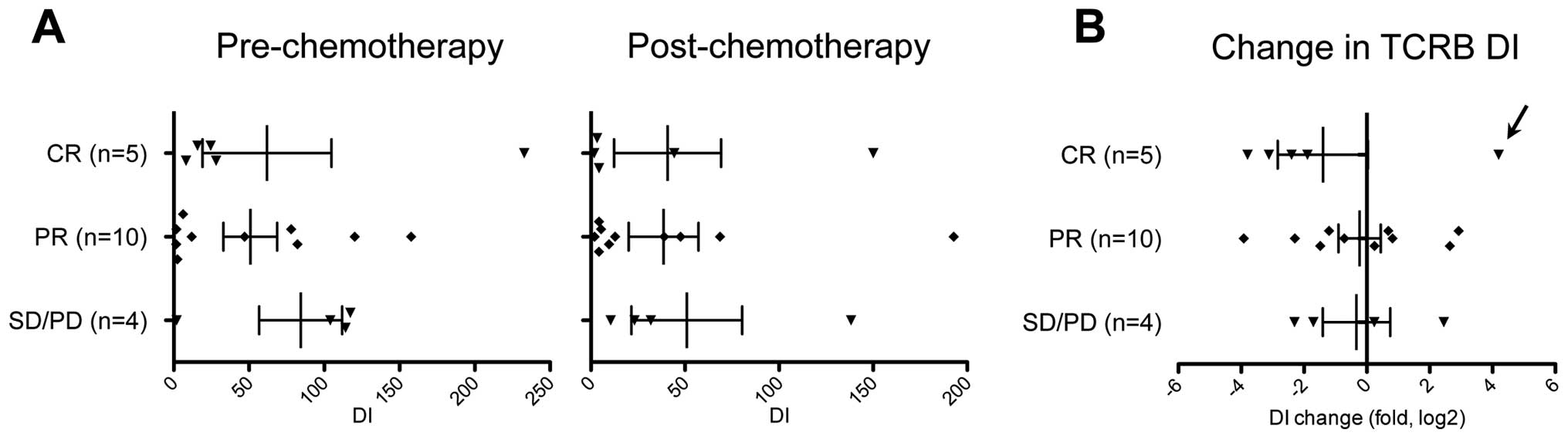
sequences. We calculated the diversity index (DI) of TCRB
repertoire to represent clonality of T cells in cancer tissues
(15). The DI values are reduced
when T cell clones with certain TCRB are expanded while they are
elevated when TCRB clonotypes are evenly distributed. The mean DI
value for TCRB was 60.8 (range of 1.65–233) in tumor samples of
pre-treatment. The mean DI was decreased to 41.8 (range of
1.77–193) by NAC. We subsequently compared DI values of TCRB
according to NAC response (Fig.
4A), and found that DI values of TCRB seemed to be more
strikingly decreased in CR cases than in PR or SD/PD cases
(Fig. 4B) while one exceptional CR
case, MC-8, showed an 18.2-fold increase (from 8.18 to 150) in DI
values of TCRB by NAC treatment (possibly by antigen spreading).
Our findings suggest that a certain population of TIL was expanded
in the tumors showing strong response by NAC. Moreover, considering
the high expression ratio of CD8/FoxP3 in CR tumors
(Fig. 1D), these results
collectively suggest that antitumor T cells were likely to be
clonally expanded in the tumors of CR patients by the chemotherapy
treatment.
Discussion
A tumor consists of a mixture of cancer cells and
noncancerous cells, of which immune cells are considered to play
critical roles in tumor progression/metastasis as well as in
response to cancer treatment (25). For example, infiltration of T cells
is frequently observed in breast cancer and generally a higher
number of T cell populations (particularly CD8+ T cells)
in tumors are associated with better response to chemotherapy and
better prognosis (9). Accumulating
evidence has shown that effective chemotherapy induces cancer cell
death and in turn enhances tumor-specific immune responses
(26). For example, dead cancer
cells are recognized and phagocytosed by antigen presenting cells
such as dendritic cells (DCs) which subsequently present
tumor-specific antigens. Such chemotherapy-induced cancer cell
death is very immunogenic because dead cancer cells release
high-mobility group box 1 protein (HMGB1) that promotes the
cross-presentation of tumor-derived antigens to T cells (27). The activated DCs migrate to the
draining lymph node, where they activate naïve T cells to memory T
cells or cytotoxic T cells acting on tumor antigens on cancer
cells. These activated T cells are released to blood circulation,
infiltrate into tumor area by chemotaxis, and then kill cancer
cells that will become additional source of tumor antigens. In
addition, chemotherapy was shown to induce intratumoral expression
of certain chemokines (e.g. CCL2, CCL5, CXCL8, CXCL9, and CXCL10),
allowing more T cells to infiltrate the tumor lesion (28).
In this study, we conducted expression analysis of
immune-related molecules including CD4, CD8, and
FoxP3, followed by detailed analysis of clonotypes of TILs
by the deep TCR sequencing. At first, we examined whether
infiltration of CD8+ T cells and FoxP3+ Treg
cells in tumor was associated with clinical response to NAC. In
concordance with a previous report (9), we found that the CD8/FoxP3
expression ratios in CR cases were higher than those in PR or SD/PD
cases. This relationship was more obvious comparing the tumor bed
and residual tumors post-NAC. The tumor tissues of CR cases showed
the highest CD8/FoxP3 expression ratio with very low
FoxP3 expression, implying that NAC shifted the
anti-tumor/pro-tumor T cell balance to generate strong antitumor
immunity. It might be caused by the release of higher levels of
tumor antigens from dead cancer cells and by the secretion of
certain chemokines/cytokines that preferentially expanded
CD8+ antitumor T cells in the CR cases. It was also
suggested that NAC might decrease systemic Tregs and then restore
antitumor immunity of the pre-existing CTLs leading to high CR rate
(29,30). Breast cancer patients with CR
showed that the number of CD8+ T cells remained high in
the tumor beds but that of FoxP3+ Treg cells
significantly decreased after chemotherapy (31).
Secondly, our results revealed that NAC induced
expansion of a certain population of TILs strongly in the tumor
beds that displayed CR. This finding might be concordant to a
recent paper reporting that significant clonal expansion of TILs
was observed in human melanoma patients who showed better response
to PD-1 blockade (pembrolizumab) treatment (10). When we consider these results with
our observations in the gene expression analysis, chemotherapy
might induce selective expansion of CD8+ antitumor CTLs
in the tumor beds of CR cases. Moreover, since such a low TCR DI
and high CD8/Foxp3 expression was associated with better
relapse-free survival of muscle-invasive bladder cancer patients
(20), the oligoclonal expansion
of CD8+ antitumor TILs may contribute to long-lasting
disease-free survival of breast cancer patients. However, at
present, we are unable to validate the antitumor activity of
individual TIL subclones that we have identified. Further study of
TIL subclones using a single cell analysis is expected to identify
the TCR α and β pairing and to assess their killing effects against
target cancer cells (32).
Although a massive amount of genetic information has
been accumulated in cancer research, it is critically necessary to
understand patient's systemic and local immune conditions to better
understand the detailed molecular mechanism in cancer therapy, not
only immunotherapy, but also in radiation therapy, chemotherapy,
and molecular-targeted therapy (33). Integration of whole exome/genome
sequencing, transcriptome analysis, antigen presentation machinery,
and comprehensive characterization of the immune environment will
improve our understanding of cancer treatment and should also
improve the quality of cancer treatment (33). Our previous TCR repertoire analyses
have shown that the TCR sequencing is a rational approach to
examine T cell-mediated immune response in a wide range of cancers
(15–20). As shown by our results, we
successfully isolated potent TCR sequences of antitumor T cells
that may have high affinity to oncoantigens (oncogenic proteins
with high immunogenicity) or neoantigens (derived from
non-synonymous mutation in cancer cells). These TCR sequences can
be applied to generate genetically-engineered T cells for adoptive
T cell therapy, as examplified by a recent trial of the
NY-ESO-1-specific TCR-engineered T cells that led to favorable
clinical responses in 16 out of 20 multiple myeloma patients
(34).
In conclusion, this study offers renewed evidence
that clonal expansion of antitumor T cells is associated with
better response to chemotherapy in breast cancer. Future studies in
functional validation of the enriched antitumor TILs as well as
identification of cancer-derived antigens corresponding to their
TCRs will accelerate cancer immunotherapies, such as adoptive T
cell therapy.
Acknowledgements
We thank Drs Rui Yamaguchi, Seiya Imoto, and Satoru
Miyano of The University of Tokyo for developing the algorithm of
TCR repertoire analysis and helpful support in data management. The
super-computing resource (http://sc.hgc.jp/shirokane.html) was provided by Human
Genome Center, the Institute of Medical Science, The University of
Tokyo. This work was also supported by the following grants: Mayo
Clinic Center for Individualized Medicine, Nadia's Gift Foundation,
John P. Guider, The Eveleigh Family, Pharmacogenomics Research
Network (U10GM 61388-15) (R.W., L.W., M.G.), R01 GM28157 (R.W.),
R01 CA196648 (L.W.), CA 15083-40A2 (M.G.), George M. Eisenberg
Foundation for Charities, and Mayo Clinic Breast SPORE P50CA
116201-9 (K.K., V.S., M.G.).
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Early Breast Cancer Trialists'
Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal
therapy for early breast cancer on recurrence and 15-year survival:
An overview of the randomised trials. Lancet. 365:1687–1717. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kaufmann M, Hortobagyi GN, Goldhirsch A,
Scholl S, Makris A, Valagussa P, Blohmer JU, Eiermann W, Jackesz R,
Jonat W, et al: Recommendations from an international expert panel
on the use of neoadjuvant (primary) systemic treatment of operable
breast cancer: An update. J Clin Oncol. 24:1940–1949. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
von Minckwitz G, Untch M, Blohmer JU,
Costa SD, Eidtmann H, Fasching PA, Gerber B, Eiermann W, Hilfrich
J, Huober J, et al: Definition and impact of pathologic complete
response on prognosis after neoadjuvant chemotherapy in various
intrinsic breast cancer subtypes. J Clin Oncol. 30:1796–1804. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Printz C: I-SPY 2 may change how clinical
trials are conducted: Researchers aim to accelerate approvals of
cancer drugs. Cancer. 119:1925–1927. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Cortazar P, Zhang L, Untch M, Mehta K,
Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L,
Valagussa P, et al: Pathological complete response and long-term
clinical benefit in breast cancer: The CTNeoBC pooled analysis.
Lancet. 384:164–172. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Denkert C, Loibl S, Noske A, Roller M,
Müller BM, Komor M, Budczies J, Darb-Esfahani S, Kronenwett R,
Hanusch C, et al: Tumor-associated lymphocytes as an independent
predictor of response to neoadjuvant chemotherapy in breast cancer.
J Clin Oncol. 28:105–113. 2010. View Article : Google Scholar
|
|
8
|
Jochems C and Schlom J: Tumor-infiltrating
immune cells and prognosis: The potential link between conventional
cancer therapy and immunity. Exp Biol Med (Maywood). 236:567–579.
2011. View Article : Google Scholar
|
|
9
|
Mao Y, Qu Q, Zhang Y, Liu J, Chen X and
Shen K: The value of tumor infiltrating lymphocytes (TILs) for
predicting response to neoadjuvant chemotherapy in breast cancer: A
systematic review and meta-analysis. PLoS One. 9:e1151032014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tumeh PC, Harview CL, Yearley JH, Shintaku
IP, Taylor EJ, Robert L, Chmielowski B, Spasic M, Henry G, Ciobanu
V, et al: PD-1 blockade induces responses by inhibiting adaptive
immune resistance. Nature. 515:568–571. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Qi Q, Liu Y, Cheng Y, Glanville J, Zhang
D, Lee JY, Olshen RA, Weyand CM, Boyd SD and Goronzy JJ: Diversity
and clonal selection in the human T-cell repertoire. Proc Natl Acad
Sci USA. 111:13139–13144. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Scaviner D and Lefranc MP: The human T
cell receptor alpha variable (TRAV) genes. Exp Clin Immunogenet.
17:83–96. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Folch G and Lefranc MP: The human T cell
receptor beta variable (TRBV) genes. Exp Clin Immunogenet.
17:42–54. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Clambey ET, Davenport B, Kappler JW,
Marrack P and Homann D: Molecules in medicine mini review: The αβ T
cell receptor. J Mol Med Berl. 92:735–741. 2014. View Article : Google Scholar
|
|
15
|
Fang H, Yamaguchi R, Liu X, Daigo Y, Yew
PY, Tanikawa C, Matsuda K, Imoto S, Miyano S and Nakamura Y:
Quantitative T cell repertoire analysis by deep cDNA sequencing of
T cell receptor α and β chains using next-generation sequencing
(NGS). Oncoimmunology. 3:e9684672015. View Article : Google Scholar
|
|
16
|
Liu X, Venkataraman G, Lin J, Kiyotani K,
Smith S, Montoya M, Nakamura Y and Kline J: Highly clonal
regulatory T-cell population in follicular lymphoma - inverse
correlation with the diversity of CD8(+) T cells. Oncoimmunology.
4:e10027282015. View Article : Google Scholar
|
|
17
|
Jang M, Yew PY, Hasegawa K, Ikeda Y,
Fujiwara K, Fleming GF, Nakamura Y and Park JH: Characterization of
T cell repertoire of blood, tumor, and ascites in ovarian cancer
patients using next generation sequencing. Oncoimmunology.
4:e10305612015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yew PY, Alachkar H, Yamaguchi R, Kiyotani
K, Fang H, Yap KL, Liu HT, Wickrema A, Artz A, van Besien K, et al:
Quantitative characterization of T-cell repertoire in allogeneic
hematopoietic stem cell transplant recipients. Bone Marrow
Transplant. 50:1227–1234. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Tamura K, Hazama S, Yamaguchi R, Imoto S,
Takenouchi H, Inoue Y, et al: Characterization of T cell repertoire
in tumor tissues and blood in advanced colorectal cancers through
deep T cell receptor sequencing. Oncol Lett. (In press).
|
|
20
|
Choudhury NJ, Kiyotani K, Yap KL,
Campanile A, Antic T, Yew PY, Steinberg G, Park JH, Nakamura Y and
O'Donnell PH: Low T cell receptor diversity, high somatic mutation
burden, and high neoantigen load as predictors of clinical outcome
in muscle-invasive bladder cancer. Eur Urol Focus. Oct 8–2015.
View Article : Google Scholar
|
|
21
|
Ellingson MS, Hart SN, Kalari KR, Suman V,
Schahl KA, Dockter TJ, Felten SJ, Sinnwell JP, Thompson KJ, Tang X,
et al: Exome sequencing reveals frequent deleterious germline
variants in cancer susceptibility genes in women with invasive
breast cancer undergoing neoadjuvant chemotherapy. Breast Cancer
Res Treat. 153:435–443. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Giudicelli V, Chaume D and Lefranc MP:
IMGT/GENE-DB: A comprehensive database for human and mouse
immunoglobulin and T cell receptor genes. Nucleic Acids Res.
33:D256–D261. 2005. View Article : Google Scholar :
|
|
23
|
Langmead B and Salzberg SL: Fast
gapped-read alignment with Bowtie 2. Nat Methods. 9:357–359. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bolotin DA, Shugay M, Mamedov IZ,
Putintseva EV, Turchaninova MA, Zvyagin IV, Britanova OV and
Chudakov DM: MiTCR: Software for T-cell receptor sequencing data
analysis. Nat Methods. 10:813–814. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Turley SJ, Cremasco V and Astarita JL:
Immunological hallmarks of stromal cells in the tumour
microenvironment. Nat Rev Immunol. 15:669–682. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Park JH: Immune microenvironment to
predict response of cancer chemotherapy and radiotherapy.
Immunopharmacogenomics. Nakamura Y: Springer; Tokyo: pp. 143–155.
2015, View Article : Google Scholar
|
|
27
|
Gebremeskel S and Johnston B: Concepts and
mechanisms underlying chemotherapy induced immunogenic cell death:
Impact on clinical studies and considerations for combined
therapies. Oncotarget. 6:41600–41619. 2015.PubMed/NCBI
|
|
28
|
Hong M, Puaux A-L, Huang C, Loumagne L,
Tow C, Mackay C, Kato M, Prévost-Blondel A, Avril MF, Nardin A, et
al: Chemotherapy induces intratumoral expression of chemokines in
cutaneous melanoma, favoring T-cell infiltration and tumor control.
Cancer Res. 71:6997–7009. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Oda N, Shimazu K, Naoi Y, Morimoto K,
Shimomura A, Shimoda M, Kagara N, Maruyama N, Kim SJ and Noguchi S:
Intratumoral regulatory T cells as an independent predictive factor
for pathological complete response to neoadjuvant paclitaxel
followed by 5-FU/epirubicin/cyclophosphamide in breast cancer
patients. Breast Cancer Res Treat. 136:107–116. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Matsushita N, Pilon-Thomas SA, Martin LM
and Riker AI: Comparative methodologies of regulatory T cell
depletion in a murine melanoma model. J Immunol Methods.
333:167–179. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ladoire S, Arnould L, Apetoh L, Coudert B,
Martin F, Chauffert B, Fumoleau P and Ghiringhelli F: Pathologic
complete response to neoadjuvant chemotherapy of breast carcinoma
is associated with the disappearance of tumor-infiltrating
foxp3+ regulatory T cells. Clin Cancer Res.
14:2413–2420. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Han A, Glanville J, Hansmann L and Davis
MM: Linking T-cell receptor sequence to functional phenotype at the
single-cell level. Nat Biotechnol. 32:684–692. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nakamura Y: Challenges and future
directions of immunopharmacogenomics. Immunopharmacogenomics.
Nakamura Y: Springer; Tokyo: pp. 159–162. 2015, View Article : Google Scholar
|
|
34
|
Rapoport AP, Stadtmauer EA, Binder-Scholl
GK, Goloubeva O, Vogl DT, Lacey SF, Badros AZ, Garfall A, Weiss B,
Finklestein J, et al: NY-ESO-1-specific TCR-engineered T cells
mediate sustained antigen-specific antitumor effects in myeloma.
Nat Med. 21:914–921. 2015. View Article : Google Scholar : PubMed/NCBI
|