Introduction
Oral potentially malignant lesions (OPMLs) are often
clinically categorized as leukoplakia or erythroplakia, with being
leukoplakia the most common, accounting for 85% of all these
lesions (1,2). While oral leukoplakia is defined as a
white plaque without immediate apparent cause, erythroplakia is a
bright red patch, which is rarely characterized as another
definitive disease (3).
Erythroleukoplakia has a mixed red and white appearance.
The diagnosis of these lesions is frequently made
excluding known diseases or disorders lacking increased risk for
cancer (3). These lesions precede
malignant development in 0.13–34% oral squamous cell carcinoma
(OSCC) cases (4). Histologically,
leukoplakia with dysplasia is often associated with a high risk of
malignant transformation (5),
dysplasia is currently the principal predictor of tumor
development.
Oral leukoplakia is more frequent in males; however,
the malignant transformation is significantly higher in females
(4). In addition to the presence
of OPMLs being a risk factor for OSCC, its malignant transformation
may be dependent on clinical, demographic, etiologic, histological
and/or molecular features (6).
Co-incidence of leukoplakia at the time of diagnosis of OSCC was
demonstrated in up to 60% of cases (7–9).
Patients with leukoplakia suffer frequently with
recurrence and development of new leukoplakias after the primary
treatment. The OPMLs may appear at any time, remaining stable for a
considerable length of time or may progress into malignant tumors
(10). The molecular mechanism
underlying malignant transformation of OPMLs remains to be
elucidated and biomarkers which may predict this risk have not been
identified. OPMLs have revealed several genetic alterations
associated with OSCC (11,12).
The present case report described one case of
simultaneous OSCC and adjacent oral leukoplakia and another with
erythroleukoplakia that evolved following treatment of primary
OSCC. The patients were clinically followed for ~48 months. During
this time, the patients developed local relapses of leukoplakia and
erythroleukoplakia. The genomic analysis of the tumors and OPMLs
allowed for the identification of some putative biomarkers of
malignant transformation.
Case report
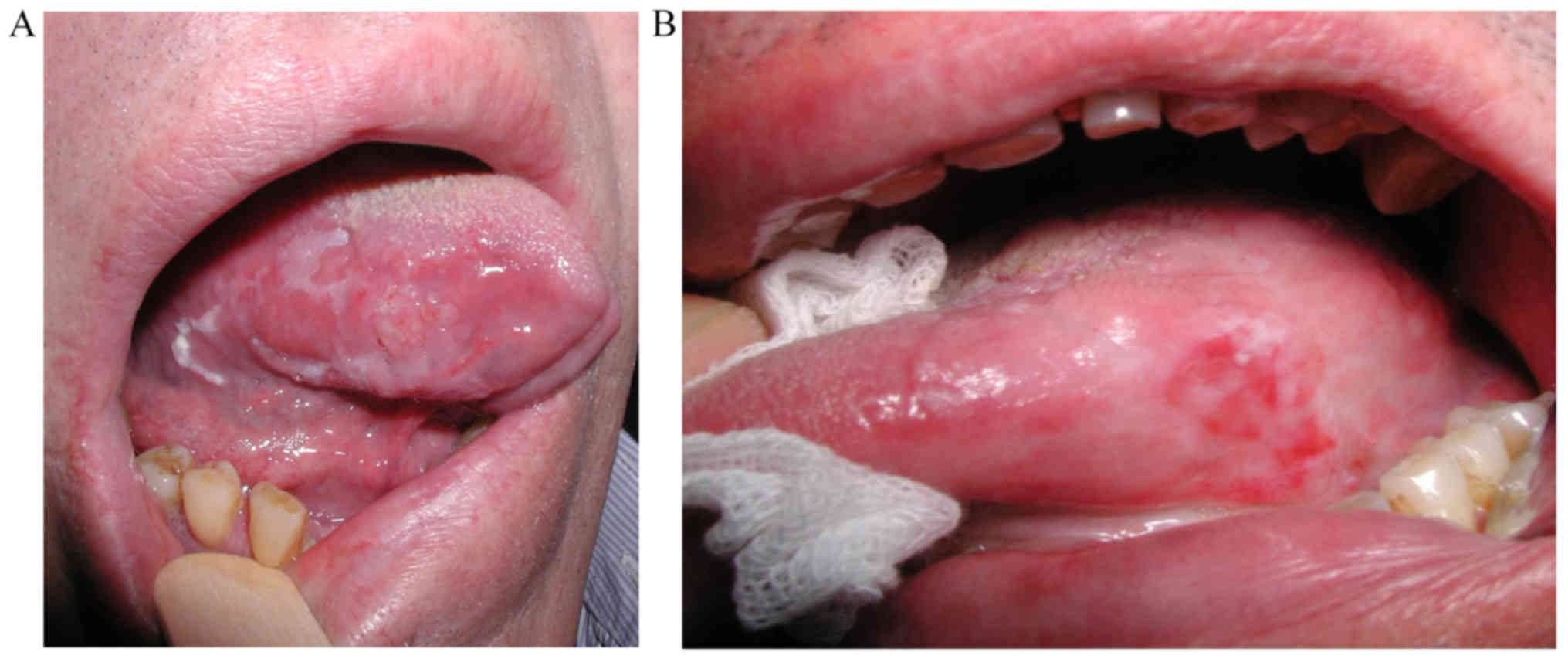
Case 1
In March 2012, a Caucasian 59-year-old man, drinker,
heavy smoker (≥20 cigarettes/day) and negative for human
papillomavirus infection, was diagnosed at the Maxillofacial
Surgery Unit, Coimbra Hospital and University Centre, EPE (Coimbra,
Portugal) with a simultaneous primary squamous cell carcinoma in
the right side of the tongue and a leukoplakia with severe
dysplasia (Fig. 1A). The diagnosis
was confirmed by a biopsy and the well differentiated tumor was
classified as early stage (I), pT1, pN0, pMx, without compromised
margins. The primary tumor and leukoplakia were simultaneously
removed by surgery in April 2012 and the leukoplakia reached the
surgical margins. Nine months after the initial diagnosis and
surgery, the patient presented a leukoplakia, histopathologically
classified as severe dysplasia. A local relapse of squamous
carcinoma was diagnosed 28 months after the primary tumor diagnosis
and total surgical excision was performed. The patient is alive and
without signs of disease 48 months after the primary diagnosis.
Case 2
In June 2012, a Caucasian 66-year-old man, drinker,
smoker (<20 cigarettes/day) and negative for human
papillomavirus infection, was diagnosed at the Maxillofacial
Surgery Unit, Coimbra Hospital and University Centre, EPE with a
primary squamous cell carcinoma in the left side of the tongue
(photography unavailable). The diagnosis was confirmed by a biopsy
and the well-differentiated tumor was classified as early stage
(II), pT2, pN0, pMx, with close but non-compromised margins. In
June 2012, the patient underwent glossectomy and ipsilateral neck
dissection, followed by braquitherapy at 60 Gy between 27 August
and 3 September 2012. The patient presented an erythroleukoplakia
without dysplasia 15 months after the primary tumor diagnosis
(Fig. 1B). A local relapse was
suspected 46 months after the primary diagnosis; however, the
patient refused biopsy and was lost to follow-up.
Genomic study
The present study was approved by the Ethics in
Research Committee of the Faculty of Medicine of the University of
Coimbra (ref: 030-CE-2015) and written informed consent from the
patients was obtained. All the experiments were performed according
to the regulations of Helsinki Declaration. From patient 1, samples
of tumor tissue, macroscopically tumor-free tissue from surgical
margins and from leukoplakia were simultaneously collected during
surgery. From patient 2 samples of tumor tissue and macroscopically
tumor-free tissue from surgical margins were simultaneously
collected during surgery. Sample from the erythroleukoplakia that
evolved after the treatment of primary tumor was obtained during
the biopsy of patient 2. All samples were immediately stored in
liquid nitrogen until use. DNA extraction was performed using a
High Pure PCR Template Preparation kit (Roche GmbH, Mannheim,
Germany) according to the manufacturer's protocol.
The genomic profile of all samples was analyzed
through array Comparative Genomic Hybridization (aCGH) using
Agilent SurePrint G3 Human Genome microarray 180K, (Agilent
Technologies, Santa Clara, CA, USA) as previously described
(13). Reference male DNA provided
by Agilent was used as control.
Discussion
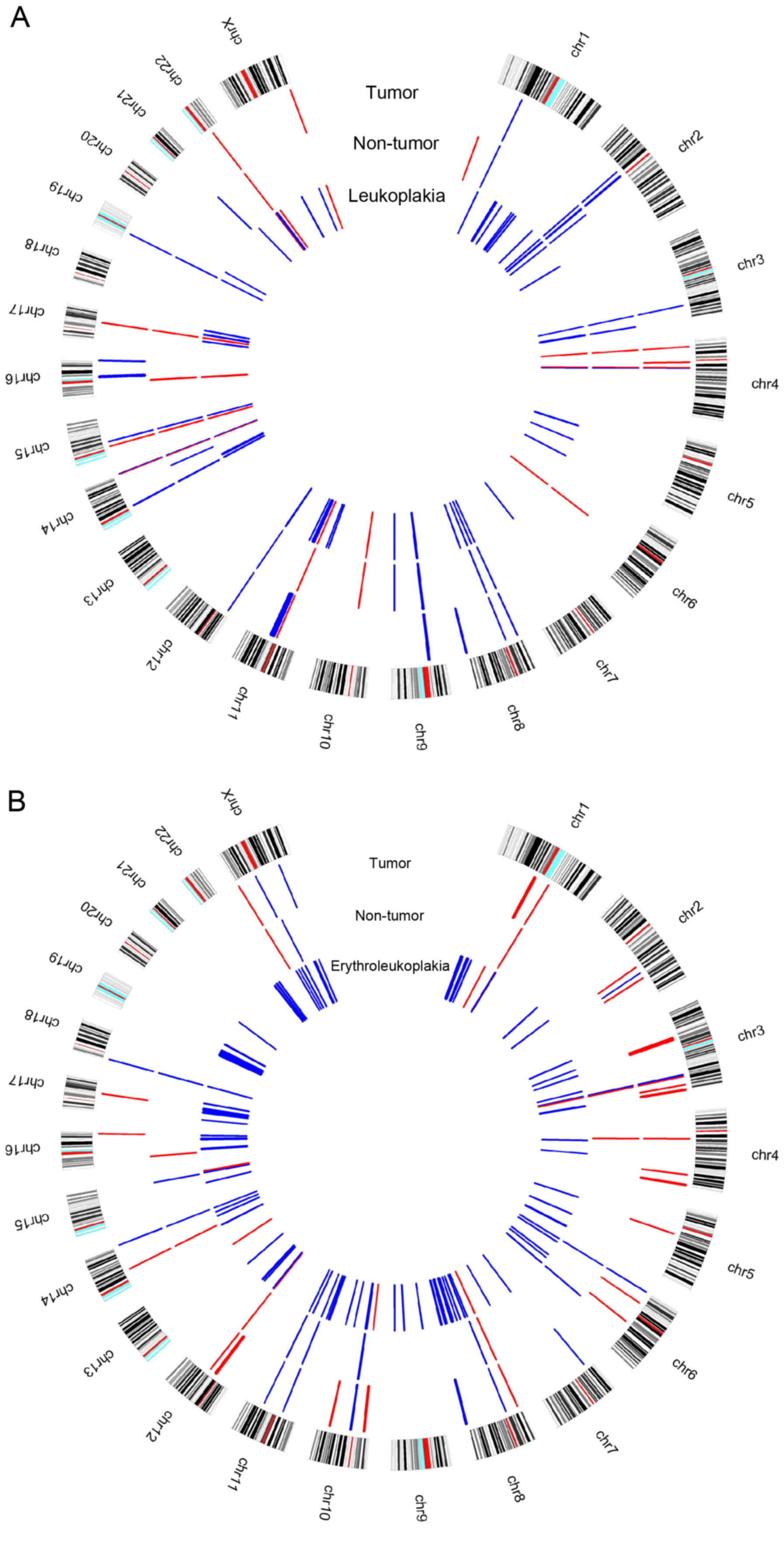
In case 1 it was observed that samples from tumor,
non-tumor and simultaneous leukoplakia shared copy number
alterations (CNAs) in some chromosomal regions, gains were
identified at 1p31.1; 2p12, 2p11.2-p11.1; 3q26.1; 4q13.2; 8p23.1;
8p11.22; 9p13.1p11.2; 12p13.31; 14q11.2; 14q32.33; 15q14; 19p12,
and losses at 4p15.32; 4q13.2; 11q11; 14q32.33; 15q11.2; 17q21.31
and 22q11.23 (Fig. 2A). In several
of these regions the present study identified some relevant genes
regarding their known function described in the University of
California, Santa Cruz (UCSC) genome browser (https://genome.ucsc.edu/) and their relationship with
oral carcinogenesis process, including FBXL5 (4p15.32),
UGT2B15 and UGT2B28 (4q13.2), KANSL1
(17q21.31) and GSTT1 (22q11.23). Additionally, gains at
11q13.3-q13.4 were specifically observed in tumor and leukoplakia
samples, which harbor the CCND1, ORAOV1,
FGF19, FGF4, FGF3, FADD, CTTN,
FOLR3, INPPL1, ARAP1 and P2RY2 genes.
These chromosomal regions and genes have been associated with
cancer, apoptosis, proliferation and OSCC (14–16).
Regarding the clinical outcome, gains at CTTN and
FADD were associated with lymph node metastasis (17,18)
and reduced overall survival (19). Additionally, gain in the
CCND1 was associated with poor prognosis, recurrence and
metastasis (20). CCND1
amplification in OPMLs was associated with 8-fold increase in
malignant transformation risk (21). In the tumor sample from case 1 a
gain was observed at 16q24.3 harboring the FANCA gene, which
is associated with locoregional progression-free survival (22). The presence of these CNAs in tumor
or in leukoplakia may suggest poor prognosis and a
recurrence/metastasis risk. Additionally, gain at the 3q29 that
mapped the PAK2 gene and loss at 6q14.1, 10q11.22 and
16p11.2 were specifically identified in the non-tumor and
leukoplakia samples. The present study specifically identified some
CNAs in the non-tumor sample, namely loss at 1p36.33, mapped the
CDK11B and CDK11A genes and gains at 2q13, mapped
ZC3H8 gene, 14q24.3 and 21q11.2. The genomic imbalances
observed in non-tumor tissue, similar to the ones observed in the
tumors, may explain the local relapse observed, since these
morphological normal cells presented already genomic aberrations
characteristic of malignancy process; therefore, being able to
suffer clonal expansion during the multistep process of
malignization. This is particularly relevant for the oral
carcinogenesis, since this patient has the traditional risk
factors, tobacco and alcohol abuse, which may lead to local relapse
disease through the field cancerization concept (23,24).
It is on note that the present study observed more genomic
imbalances in the leukoplakia compared with the tumor sample
(Fig. 2A). Chromosomes 5, 7 and 10
did not present genomic imbalances in this tumor sample and
chromosomes 13, 18 and 20 did not presented imbalances in both
samples, tumor and leukoplakia.
In this case, distinct chromosomal changes and genes
have been described that may have a strong prognostic potential to
predict patients' outcome and tumor transformation. However,
further studies in larger cohorts are required in order to validate
these findings.
In case 2 it was observed that tumor, non-tumor and
the erythroleukoplakia that developed following primary tumor
treatment shared CNAs in some chromosomal regions, particularly
gains at 3q25.32, 8p11.22, 10q11.22, 11p12, 11q14.3, 14q32.33 and
18p11.32, and losses at 3q26.1, 6p25.3, 8p23.1, 12q14.2 and
Yq11.223 (Fig. 2B). Taking the
known function of the genes mapped in these regions into account
DUP22 (6p25.3) may be the stronger putative candidate gene
for the oral carcinogenesis process. Downregulation of DUP22
suggests its putative role as tumor suppressor gene; however, its
function in cancer remains to be elucidated. This gene has been
previously identified as a regulator of JNK signaling and with
ability to dephosphorylate MAPKs (25). DUSP22 may also regulate
metastasis, as its overexpression inhibited cell migration and
reduced FAK phosphorylation (26).
The present study observed losses at 1q21.2, 4q13.2, 14q21.1,
Xp22.33 and Yp11.32 in tumor and non-tumor samples and in non-tumor
and erythroleukoplakia samples gain was observed at 6q22.1 and
Xq11.1. Tumor and erythroleukoplakia samples shared copy number
gains at 8q24.3, which harbored GSDMD, SCRIB,
PUF60, GRINA, SHARPIN and SCRT1. The
8q24.3 chromosomal band is frequently amplified in OSCC (15,16),
which may suggest its importance for malignant transformation.
These genes may be important predictors of tumor transformation
risk, warranting further investigation. Copy number losses in
Yq11.23 were also observed in both of these samples. MYC
(8q24.21) and PTK2 (8q24.3) were detected only in the
erythroleukoplakia sample and have already been associated with
OSCC. A previous study revealed that overexpression of MYC
was linked with malignant transformation and poor survival
(27). PTK2 has been
associated with resistance to radiotherapy (28). The presence of these genomic
imbalances in the erythroleukoplakia, diagnosed 15 months following
the primary tumor, may be the trigger for the development of
relapse. There is no histological confirmation of relapse in this
patient, as he refused to performed biopsy to verify the clinical
suspicion. Additionally, these genes seem to be important
candidates for the OSCC prognosis and especially for the prediction
of the risk of relapse. The present study observed in the tumor,
non-tumor and erythroleukoplakia collected from this patient, that
was treated by surgery and braquitherapy several genomic
alterations which were previously identified by Van den Broek et
al (29) with
chemoradioresistance and some with chemoradiosensitivity (Table I). Additionally, the present study
highlighted some putative genes for these regions based in its
known function described at the UCSC, including DUSP22 and
JARID2 (Table I). Genomic
imbalances in non-tumor tissues may indicate the presence of
altered clones of cells even in the surrounding clinically and
histologically normal oral mucosa, originating a progression to
malignancy. Additionally, the present study detected more
imbalances associated with chemoradiotherapy in erythroleukoplakia
compared with the primary tumor sample, which may suggest that
these alterations occurred following the treatment for the primary
tumor or there was a selection of radioresistant cell populations
due to the treatment.
 | Table I.Chromosomal regions described in the
study of Van den Broek et al (29), as associated with
chemoradioresistance and chemoradiosensitivity and some putative
candidate genes for these regions identified in the patient 2. |
Table I.
Chromosomal regions described in the
study of Van den Broek et al (29), as associated with
chemoradioresistance and chemoradiosensitivity and some putative
candidate genes for these regions identified in the patient 2.
| Chromosomal
region | Type of
alteration | Clinical
association | Patient
2-tumor | Patient
2-non-tumor | Patient
2-leukoplakia | Putative candidate
genes |
|---|
| 3q21-q26.1 | Gain |
Chemoradioresistance |
|
| 3q25.32 |
|
| 6p11-pter |
|
| 6p25.3 |
| 6p25.3;
6p23-p22.3 | DUSP22,
JARID2 |
| 6q22-q27 |
|
|
| 6q22.1 | 6q22.1 |
|
| Xq11-qter |
|
|
| Xq11.1 | Xq11.1 |
|
|
|
|
| Xq25 |
| Xq25 |
|
| 7p11.2–12 | Amplification |
|
|
| 7p11.2 | SEPT14,
CHCHD2 |
| 8p11.1–12 |
|
| 8p11.22 | 8p11.22 | 8p11.22 |
|
| 12q15 |
|
|
|
| 12q15 | RAP1B,
MDM2 |
| 15q21 |
|
|
|
| 15q21.2 |
|
| 18p11.3 |
|
| 18p11.32 | 18p11.32 | 18p11.32 |
|
| 3p11-pter | Loss |
| 3p14.2-p14.1 |
|
| FHIT, PTPR6,
ADAMTS9 |
| 5q11-q12 | Gain |
Chemoradiosensitivity |
|
| 5q11.2 |
|
| 10q11-q22 |
|
| 10q11.22 | 10q11.22 | 10q11.22;
10q11.21 |
|
| 14q distal |
|
| 14q32.33 | 14q32.33 | 14q32.33 |
|
| 14q13 | Amplification |
|
|
| 14q13.1-q13.2 | EAPP |
| 2q22-q25 | Loss |
| 2q23.3-q24.1 |
|
|
|
Overall, leukoplakia and erythroleukoplakia samples
of the two patients presented more CNAs than the respective primary
tumor. The erythroleukoplakia sample presented more CNAs than
leukoplakia one (Fig. 1A and B),
which may be due to the fact that erythroleukoplakia is associated
with significantly higher rates of dysplasia, carcinoma in
situ and invasive carcinoma compared with leukoplakia (30). As this patient presented an
erythroleukoplakia without dysplasia, it is possible that
erythroleukoplakia occurred following braquitherapy, which may
induce several of the genomic alterations detected. CNAs were
identified in several genes in these two OPMLs, which were
associated with cancer and hallmarks of the carcinogenesis process,
including cell cycle, cell growth, proliferation, differentiation,
angiogenesis, apoptosis/cell death, DNA repair and
invasion/migration (Fig. 3A and
B). The present study observed that common genes altered in
both cases, namely gains in BNIPL, MCL1, CSPP1 and
ZNRF3 genes. These specific genes may represent important
players in the malignant transformation of OPMLs into tumors, as
these two patients relapsed. Further investigation is required to
validate these results. Additionally, in the non-tumor sample of
patient 1 and in the erythroleukoplakia sample of patient 2 a loss
at 1p36.33 was identifies, where the CDK11B and
CDK11A genes, which are associated with cell cycle and
apoptosis, are mapped.
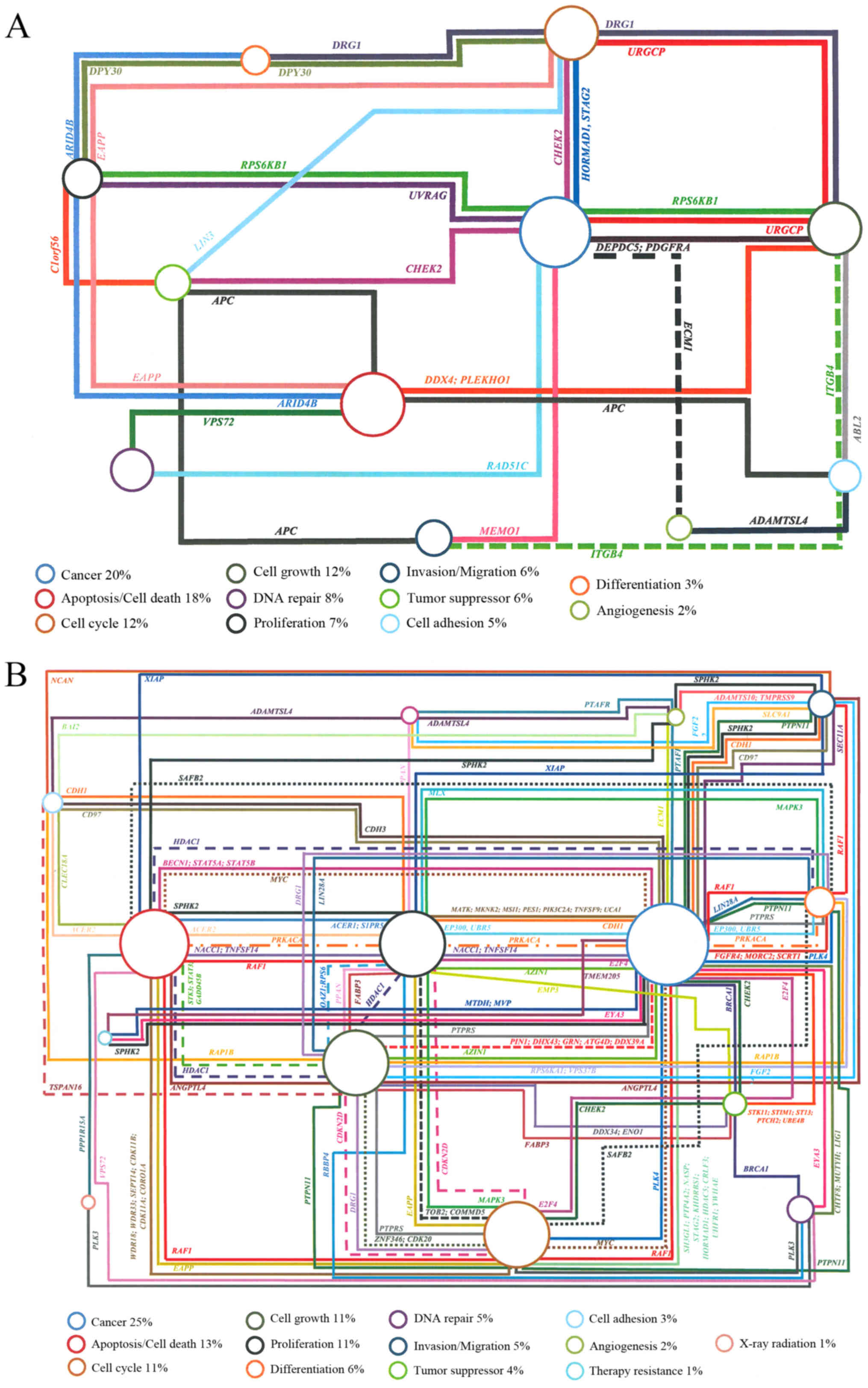 | Figure 3.Genes associated to diverse biological
processes with impact on cancer development according to UCSC
genome browser. The percentage represents the number of genes
associated with each biological process. (A) Genes identified
specifically in leukoplakia of patient 1. The following genes are
associated only with one specific biological process: DNA repair:
C11orf30, CHAF1B, GTF2H1, POLD3, RNF169. Apoptosis/cell
death: ANO1, BIRC6, BNIPL, DAP3, MCL1, SAP30BP, SUMO2, PAK2,
PTRH2. Cancer: SERPINH1, STAG2, TRIM37, WNT11, GSTT1, PPME1,
PRUNE. Cell cycle: CCNO, COPS5, CSPP1.
Invasion/migration: LLGL2, RAB25. Tumor suppressor:
ZNRF3. X-ray radiation: XRRA1. (B) Genes identified
specifically in erythroleukoplakia of patient 2. The following
genes are associated only with one specific biological process: DNA
repair: KIAA0146, MCM4, NSMCE2, PRKDC, RNF168, SF3B3, SIRT6,
UIMC1, XRCC2, XRCC6. Apoptosis/cell death: ATAD5, BAX, BBC3,
BCL2L13, BNIPL, CARD8, HCHD2, DAPK3, GRINA, IFI6, MAP15, MCL1,
PYCARD, RDM25, RERE, TAOK2, TMEM161A, TRADD, TRIAP1.
Angiogenesis: CCR10. Cancer: ALDH2, CREB3L3, CTCF, OX6C,
DPP9, DUSP22, ELAVL1, EWSR1, FAM83A, GAL3ST1, HIGD1B, MDM2, MTSS1,
NQO1, PGPEP1, PIK3CB, POUSF1B, PRDX1, PRDX2, PVT1, RFX1, RNF139,
RPS15, RPS8, S100PBP, SAFB, SELENBP1, SPIN1, WWP2. Proliferation:
ANGPTL6, CIB1, DLG1, HDGFRP3, FUT3, PLA2G1B, RASL10A, S1PR2.
Cell cycle: ARID3A, BRD4, CDK2AP1, CSPP1, FZR1, GADD4SGIP1,
NAE1, NPEPPS, PPP6C. Invasion/migration: ELMO3, MRI1,
PARD6A, SCAI, ZRANB1. Cell growth: ARHGEF18, CD37, CDIPT,
DDX19B, DDX20, DDX28, PPAN-P2RY11, PTK2, SESN2. Tumor
suppressor: ADAM11, APC2, MAPKAPK5, ZNRF3. Tumor growth:
ANXA13, KLF10, PDF. Differentiation: PUM1. |
Identifying accurately and prospectively the OPMLs
likely to progress to tumor is of paramount clinical significance.
The present study identified the chromosomal regions and genes with
CNAs in OSCCs and in OPMLs, such as FBXL5, UGT2B15,
UGT2B28, KANSL1, GSTT1 and DUSP22 in
the two patients presented. Leukoplakia and erythroleukoplakia had
a high genomic heterogeneity with several genes altered; the genes
that were altered were consistent across the two cases that were
investigated specifically gains in BNIPL, MCL1, STAG2, CSPP1
and ZNRF3. Therefore, the current study identified several
genes that may be associated with malignant transformation. The
present study also highlighted several putative genes that may be
associated with chemoradioresistance, particularly DUSP22
and JARID2.
Acknowledgements
The present study was in part supported by the
Center of Investigation on Environment Genetics and Oncobiology,
Faculty of Medicine, University of Coimbra. Ribeiro I.P. has a PhD
fellowship (grant. no. SFRH/BD/52290/2013) supported by the
Portuguese Foundation for Science and Technology.
References
|
1
|
Warnakulasuriya S: Lack of molecular
markers to predict malignant potential of oral precancer. J Pathol.
190:407–409. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vigneswaran N and Williams MD:
Epidemiologic trends in head and neck cancer and aids in diagnosis.
Oral Maxillofac Surg Clin North Am. 26:123–141. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dionne KR, Warnakulasuriya S, Zain RB and
Cheong SC: Potentially malignant disorders of the oral cavity:
Current practice and future directions in the clinic and
laboratory. Int J Cancer. 136:503–515. 2015.PubMed/NCBI
|
|
4
|
Warnakulasuriya S and Ariyawardana A:
Malignant transformation of oral leukoplakia: A systematic review
of observational studies. J Oral Pathol Med. 45:155–166. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kobayashi T, Maruyama S, Abé T, Cheng J,
Takagi R, Saito C and Saku T: Keratin 10-positive orthokeratotic
dysplasia: A new leucoplakia-type precancerous entity of the oral
mucosa. Histopathology. 61:910–920. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
William WN Jr: Oral premalignant lesions:
Any progress with systemic therapies? Curr Opin Oncol. 24:205–210.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bouquot JE, Weiland LH and Kurland LT:
Leukoplakia and carcinoma in situ synchronously associated with
invasive oral/oropharyngeal carcinoma in Rochester, Minn.,
1935–1984. Oral Surg Oral Med Oral Pathol. 65:199–207. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gupta PC, Mehta FS, Daftary DK, Pindborg
JJ, Bhonsle RB, Jalnawalla PN, Sinor PN, Pitkar VK, Murti PR, Irani
RR, et al: Incidence rates of oral cancer and natural history of
oral precancerous lesions in a 10-year follow-up study of Indian
villagers. Community Dent Oral Epidemiol. 8:283–333. 1980.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reibel J: Prognosis of oral pre-malignant
lesions: Significance of clinical, histopathological, and molecular
biological characteristics. Crit Rev Oral Biol Med. 14:47–62. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Neville BW, Dann DD, Allen CM and Bouqout
JE: Patologia epitelialPatologia Oral & Maxilofacial. Guanabara
Koogan Brazil; pp. 1–423. 2009
|
|
11
|
Califano J, Westra WH, Meininger G, Corio
R, Koch WM and Sidransky D: Genetic progression and clonal
relationship of recurrent premalignant head and neck lesions. Clin
Cancer Res. 6:347–352. 2000.PubMed/NCBI
|
|
12
|
Ha PK and Califano JA: The molecular
biology of mucosal field cancerization of the head and neck. Crit
Rev Oral Biol Med. 14:363–369. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pinto-Leite R, Carreira I, Melo J,
Ferreira SI, Ribeiro I, Ferreira J, Filipe M, Bernardo C,
Arantes-Rodrigues R, Oliveira P and Santos L: Genomic
characterization of three urinary bladder cancer cell lines:
Understanding genomic types of urinary bladder cancer. Tumour Biol.
35:4599–4617. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jin C, Jin Y, Gisselsson D, Wennerberg J,
Wah TS, Strömbäck B, Kwong YL and Mertens F: Molecular cytogenetic
characterization of the 11q13 amplicon in head and neck squamous
cell carcinoma. Cytogenet Genome Res. 115:99–106. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ribeiro IP, Marques F, Caramelo F, Ferrão
J, Prazeres H, Julião MJ, Rifi W, Savola S, de Melo JB, Baptista IP
and Carreira IM: Genetic imbalances detected by multiplex
ligation-dependent probe amplification in a cohort of patients with
oral squamous cell carcinoma-the first step towards clinical
personalized medicine. Tumour Biol. 35:4687–4695. 2014.PubMed/NCBI
|
|
16
|
Ribeiro IP, Marques F, Caramelo F, Pereira
J, Patrício M, Prazeres H, Ferrão J, Julião MJ, Castelo-Branco M,
de Melo JB, et al: Genetic gains and losses in oral squamous cell
carcinoma: Impact on clinical management. Cell Oncol (Dordr).
37:29–39. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Rothschild BL, Shim AH, Ammer AG, Kelley
LC, Irby KB, Head JA, Chen L, Varella-Garcia M, Sacks PG, Frederick
B, et al: Cortactin overexpression regulates actin-related protein
2/3 complex activity, motility, and invasion in carcinomas with
chromosome 11q13 amplification. Cancer Res. 66:8017–8025. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pattje WJ, Melchers LJ, Slagter-Menkema L,
Mastik MF, Schrijvers ML, Gibcus JH, Kluin PM, Hoegen-Chouvalova O,
Van Der Laan BF, Roodenburg JL, et al: FADD expression is
associated with regional and distant metastasis in squamous cell
carcinoma of the head and neck. Histopathology. 63:263–270. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Freier K, Hofele C, Knoepfle K, Gross M,
Devens F, Dyckhoff G, Plinkert P, Lichter P and Herold-Mende C:
Cytogenetic characterization of head and neck squamous cell
carcinoma cell lines as model systems for the functional analyses
of tumor-associated genes. J Oral Pathol Med. 39:382–389.
2010.PubMed/NCBI
|
|
20
|
Ruiz C, Martins JR, Rudin F, Schneider S,
Dietsche T, Fischer CA, Tornillo L, Terracciano LM, Schreiber R,
Bubendorf L and Kunzelmann K: Enhanced expression of ANO1 in head
and neck squamous cell carcinoma causes cell migration and
correlates with poor prognosis. PLoS One. 7:e432652012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Poh CF, Zhu Y, Chen E, Berean KW, Wu L,
Zhang L and Rosin MP: Unique FISH patterns associated with cancer
progression of oral dysplasia. J Dent Res. 91:52–57. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bauer VL, Braselmann H, Henke M, Mattern
D, Walch A, Unger K, Baudis M, Lassmann S, Huber R, Wienberg J, et
al: Chromosomal changes characterize head and neck cancer with poor
prognosis. J Mol Med (Berl). 86:1353–1365. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rettori MM, de Carvalho AC, Longo AL, de
Oliveira CZ, Kowalski LP, Carvalho AL and Vettore AL: TIMP3 and
CCNA1 hypermethylation in HNSCC is associated with an increased
incidence of second primary tumors. J Transl Med. 11:3162013.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Slaughter DP, Southwick HW and Smejkal W:
Field cancerization in oral stratified squamous epithelium;
clinical implications of multicentric origin. Cancer. 6:963–968.
1953. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chen AJ, Zhou G, Juan T, Colicos SM,
Cannon JP, Cabriera-Hansen M, Meyer CF, Jurecic R, Copeland NG,
Gilbert DJ, et al: The dual specificity JKAP specifically activates
the c-Jun N-terminal kinase pathway. J Biol Chem. 277:36592–36601.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li JP, Fu YN, Chen YR and Tan TH: JNK
pathway-associated phosphatase dephosphorylates focal adhesion
kinase and suppresses cell migration. J Biol Chem. 285:5472–5478.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gollin SM: Chromosomal alterations in
squamous cell carcinomas of the head and neck: Window to the
biology of disease. Head Neck. 23:238–253. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Skinner HD, Giri U, Yang L, Woo SH, Story
MD, Pickering CR, Byers LA, Williams MD, El-Naggar A, Wang J, et
al: Proteomic profiling identifies PTK2/FAK as a driver of
radioresistance in HPV-negative head and neck cancer. Clin Cancer
Res. 22:4643–4650. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
van den Broek GB, Wreesmann VB, van den
Brekel MW, Rasch CR, Balm AJ and Rao PH: Genetic abnormalities
associated with chemoradiation resistance of head and neck squamous
cell carcinoma. Clin Cancer Res. 13:4386–4391. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Thomas G, Hashibe M, Jacob BJ, Ramadas K,
Mathew B, Sankaranarayanan R and Zhang ZF: Risk factors for
multiple oral premalignant lesions. Int J Cancer. 107:285–291.
2003. View Article : Google Scholar : PubMed/NCBI
|