Introduction
Methotrexate (MTX), an antifolate and anticancer
agent with a narrow therapeutic window, is commonly used for
refractory rheumatoid arthritis, psoriasis, breast carcinoma, lung
and liver cancer and systemic lupus erythematosus (1,2).
However, besides its affirmative effect in the clinic, MTX has many
side effects including nausea, vomiting, mucositis, diarrhea,
stomatitis, myelosuppression (3,4) and
hepatotoxicity (5). All these side
effects limit its use, and the toxicity is so severe that >50%
patients give up the treatment (6).
Currently, methods such as folic acid
supplementation for reducing the dosage and regularly checking the
body functions are a clinical way to reduce the side effects of
MTX. However, the remedial method of detoxification after MTX
poisoning does not tend to be effective. Therefore, ethnomedicines
may be of importance, particularly if they have detoxifying
effects. For example, one of the most commonly used detoxicants is
Smilax glabra Rhizoma (SGR; Tufuling in Chinese).
SGR is a natural dietary supplement widely used in
food-making and health care in Southeast Asia, Arabian countries
and North America (7,8). Various bioactivities of SGR have been
demonstrated in in vitro and in vivo assays,
including anti-cancer (9),
antiviral (10), anti-inflammatory
(11), immunomodulatory (12), detoxification and hepatoprotective
effects (13). In the clinic,
patients with rheumatoid arthritis, cancer, nephroma and even
MTX-induced hepatotoxicity (14–16),
receive treatment with a combination of MTX and SGR or
SGR-containing herbal mixtures frequently (17,18).
Investigating the drug-drug interaction (DDI) or
drug-herb interaction (DHI) using pharmacokinetic methods has
become popular. DDI or DHI are usually induced by drug metabolism
enzyme or drug transporters. MTX enters cells primarily by
carrier-mediated uptake (19,20).
Therefore, DDI or DHI induced by MTX may mainly associate with drug
transporters. MTX is the substrate of P-glyocoprotein (gp)
(21),
multidrug-resistance-associated protein (MRP)1, 2 and 3 (22–25),
and organic anion transporters (OAT)1, 2 (26,27).
Anything which could change the activity of the above transporters
may induce DDI or DHI of MTX.
Astilbin is the major active component of SGR, and
the content in SGR usually >0.4%. Wang et al (28) reported that astilbin increased the
expression of P-gp in rats. In vivo, astilbin are further
metabolized into sulfates and glucuronides (29), which all are the substrate of MRP1,
MRP2, and MRP3 (30–32). This indicates that DHI may happen
with a combination of MTX and SGR, but this interaction requires
further study.
Therefore, in the present study, the effect of SGR
on the pharmacokinetics and tissue distribution of MTX was studied
in rats, and the potential underlying mechanism was
investigated.
Materials and methods
Chemicals and reagents
MTX was purchased from Guangzhou Lubex Biological
Technology Co., Ltd. (Guangdong, China; batch no. 100138-201104).
SGR was purchased from Kangmei Pharmaceutical Co., Ltd.,
(Guangdong, China) in February 2013 (batch no. 130800051) and was
verified by Chen Wen-liang in the Second Affiliated Hospital,
Guangzhou University of Chinese Medicine (Guangzhou, China). SPE
cartridges were supplied by Dikma Technologies, Inc. (Beijing,
China). All other materials were analytical grade or better and
used as received.
Preparation of SGR decoction
Ethanol (75%) was added to 450 g crude drug, soaked
for 30 min and then heated on a reflux extraction device. After
boiling, gentle heating was continued for 1 h, the mixture was
filtered, and the filtrate was concentrated by rotary evaporators.
The volume was kept to 150 ml and frozen at −20°C for later use.
The chromatographic fingerprint of SGR has been analyzed in our
previous study (33). The
concentration of astilbin in the extract was ~0.48%.
Animal and drug administration
A total of 54 male Sprague-Dawley (SD) rats aged 7–8
weeks, weighing 300±50 g, were supplied by Southern Medical
University (Guangzhou, China; certification no. 44002100003362).
The rats were housed in cages at 21±3°C and 50% relative humidity
on a 12-h light/dark cycle. They were acclimated to this
environment for 7 days with standard diet until the night prior to
the experiment. The rats were then fasted overnight with free
access to water. The studies were approved by the Animal Ethics
Committee of Guangzhou University of Chinese Medicine (Guangzhou,
China), and conducted in strict accordance with the recommendations
in the guide for the care and use of Laboratory Animals of the
National Institutes of Health (Bethesda, MA, USA).
Pharmacokinetic study
Pharmacokinetic studies were carried out in SD rats.
Animals were randomly divided into two groups (n=6 per group). MTX
was diluted with deionized water to obtain concentration of 0.6
mg/ml. MTX (6.0 mg/kg) was given orally to rats with and without a
concomitant oral dose of SGR (30 g/kg of crude drugs) at 5 min
before. Blood samples (0.6 ml) were collected from orbit venous
plexus into heparinized 1.5 ml polythene tubes at predetermined
time points (10, 20, 40, 60, 120, 240, 360, 480 and 540 min). The
samples were immediately centrifuged at 3,500 × g for 15 min at
room temperature, and the supernatant was gathered as plasma and
stored at −80°C until analysis.
Tissues distribution study
Tissue distribution studies were carried out in 36
male SD rats. Animals were randomly divided into two groups (n=18
per group): MTX alone and MTX combined with SGR. MTX (6.0 mg/kg)
was given orally to rats with and without a concomitant oral dose
of SGR (30 g/kg of crude drug) at 5 min beforehand. Following
intragastric administration, rats were anesthetized by 10% chloral
hydrate (4 ml/kg; Tianjin Damao Chemical Reagent Factory, Tianjin,
China) and sacrificed at predetermined time points (20, 60 and 240
min; 6 rats were sacrificed at each time point of each group).
Blood samples were obtained from the abdominal aorta; the chest and
abdominal cavity were opened and tissues of interest (heart, liver,
spleen, kidney, lung, stomach, intestine and marrow) were harvested
and rinsed with ice-cold 0.9% NaCl to remove the superficial blood.
Following being blotted dry with filter paper, the tissue samples
were stored at −80°C until analysis.
Sample preparation
The plasma was thawed and swirled for 10 sec, and
then 100 µl plasma was added to a pre-conditioned SPE column. After
washing with 1 ml deionized water, 1 ml washing solution [0.2%
methanoic acid-methanol (v/v)] was used. The deionized water
elution was discarded and washing solution elution was collected,
then evaporated to dryness under a stream of nitrogen at 40°C. The
residue was re-dissolved with 100 µl mobile phase and then filtered
through a 0.22-µm disposable syringe filter, of which 10 µl was
injected into the high-performance liquid chromatography (HPLC)
system for analysis. Each tissue sample weight ~300 mg after
thawing, and was homogenated in 0.9% NaCl [1:6 (w/v)]. Tissue
homogenate samples were centrifuged at 3,500 × g for 15 min at 4°C,
the supernatant was collected and conducted as plasma sample, and
10 µl supernatant was used for HPLC analysis.
HPLC analysis
The chromatographic analysis was performed on an
Agilent 1200 system (Agilent Technologies, Inc., Santa Clara, CA,
USA) with a VWD detector at 302 nm. Samples were analyzed on a
Diamonsil C18 column (250×4.6 mm I.D, 5 µm; Dikma Technologies
Inc.) at 30°C. The mobile phase consisted of 0.1% formic acid
aqueous solution (A) and methanol (B), using a gradient elution (0
min: 10% B, 8 min: 60% B, 10 min: 100% B) at a flow rate of 1.0
ml/min, and the injection volume was 10 µl.
Preparation of standard solution and
quality control samples
Standard solution of MTX was prepared by using 0.1%
formic acid water containing 5% methanol; the working concentration
was 200 mg/l. This was stored at 4°C in a dark place until use.
Appropriate amounts of the standard solution were added to 100 µl
blank rat plasma or tissue homogenates to prepare the calibration
standards of MTX, the final calibration standard concentrations
were 0.052, 0.104, 0.157, 0.313, 0.626, 1.252, 2.503 and 5.006 mg/l
for plasma samples and 0.020, 0.039, 0.078, 0.156, 0.3125, 0.625,
1.25, 2.5 and 5 mg/l for tissue samples. Quality control (QC)
samples were prepared at the lower limit of quantification (LLOQ);
low, medium and high concentrations of 0.052, 0.313, 1.252 and
5.006 mg/l for plasma samples and 0.020, 0.078, 0.3125 and 1.25
mg/l for tissue samples.
Method validation
The specificity of the assay was assessed by
comparing the chromatograms of blank sample with the corresponding
spiked samples, and each blank sample was tested to ensure that it
had no interference on the elution of MTX. The calibration curves
were constructed from the peak area of each standard solution
against homographic concentrations using eight-level nonzero
standards and a linearly weighed (1/x) least squares regression
model. The accuracy and precision were determined by replicate
analysis (n=6) of QC samples on three different time points.
Relative standard deviation (RSD)% was used to evaluate the
accuracy and the intra- and inter-day precision. The extract
recovery of MTX at QC levels were evaluated by assaying the samples
as described above and comparing peak areas with those obtained
from the compounds dissolved in the supernatant of the processed
blank plasma. The stability of plasma and tissues was investigated
by analyzing of the samples at QC levels (n=6) under different
conditions.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Tissues were homogenized in RNAiso Plus
(Sigma-Aldrich; Merck KGaA, Darmstadt, Germany) to extract total
RNA according to the manufacturer's protocol. The quality and
concentration of RNA were determined using the OD260/280 ratio
measured by the Thermo NanoDrop 2000c (Thermo Fisher Scientific,
Inc., Waltham, MA, USA) and stored at −80°C prior to use. cDNA was
synthesized from total RNA (1 µg; 20 µl final reaction volume) with
oligo(dT) priming using M-MLV platinum Green qPCR Super Mix-UDG
(Invitrogen; Thermo Fisher Scientific, Inc.) according to the
manufacturer's protocol, then performed on Veriti 96 Well Thermal
Cycler (Applied Biosystems; Thermo Fisher Scientific, Inc.).
qPCR was performed on an ABI Prism TM 7500 Real Time
qPCR system (Applied Biosystems; Thermo Fisher Scientific, Inc.)
using the SYBR Select Mastermix (Applied Biosystems; Thermo Fisher
Scientific, Inc.). The experiment was carried out using optical
96-well reaction plates covered with plate sealers. Samples were
treated following the instructions of SYBR Select Mastermix
(Applied Biosystems; Thermo Fisher Scientific, Inc.): Each tube of
reaction mix consisted of 2 µl of RT cDNA, forward and reverse
primers (each 0.4 µl), 10 µl SYBR Select Mastermix and 7.2 µl no
enzyme water (20 µl final reaction volume). Primer sequences used
for RT-qPCR are listed in Table I.
Cycling parameters were as follows: 50°C for 2 min, 95°C for 1 min,
then 40 cycles of 95°C for 15 sec and 60°C for 1 min. A melting
temperature-determining dissociation step was performed at 96°C for
15 sec, 60°C for 1 min, and 95°C for 15 sec, for a total of 45
cycles in a procedure.
 | Table I.Primer sequences used in reverse
transcription-quantitative polymerase chain reaction. |
Table I.
Primer sequences used in reverse
transcription-quantitative polymerase chain reaction.
| Gene | Forward primer
(5′-3′) | Reverse primer
(5′-3′) |
|---|
| Rat-P-gp |
ATGAAACTGCCCCACAAATT |
CTTTCTGTGTCCAAGGCTGA |
| Rat-OAT1 |
CCATGCTGTGGTTTGCCACTA |
ACAAACTTGGCAGGCAGGTC |
| Rat-OAT2 |
TGGCCTATGCCATTCCAGAC |
GGGATTCTGGGACAAACCAGT |
| Rat-GAPDH |
ATGATTCTACCCACGGCAAG |
CTGGAAGATGGTGATGGGTT |
| Rat-MRP1 |
AGGTTGGTATTGTGGGTCGTA |
GATGGTGATCTTGAAGCGCAGGTT |
| Rat-MRP2 |
GGGACTCCAACCTGACTGTAT |
CCTCTGGGCAAGGATTTGT |
| Rat-MRP3 |
TCAGCATCCTCATCAGGTTTATT |
ATGATAGCAGTCCGTATCCTCAA |
The data were analyzed by the comparative Cq method
(34). Cq was recorded for the
expression of each gene assayed in the RT-qPCR. All the Cq values
were means of triplicate samples tested. GAPDH was chosen as the
reference gene for the internal control. Differences between the Cq
values of the target gene and the internal control gene (∆Cq = Cq
target - Cq internal control) were calculated to normalize the
differences. Differences between ∆Cq of each sample and calibrator
∆∆Cq = (Cq calibrator - ∆Cq) were calculated. The change
in the gene expression was calculated as 2−∆∆Cq.
Statistical analysis
DAS software version 2.0 (DAS for eCDM; Shanghai
University of Traditional Chinese Medicine, Shanghai, China) was
used to calculate the pharmacokinetic parameters by
non-compartmental model. Concentrations below the lower limit of
quantify were treated as 0. Data analysis was performed using SPSS
version 19.0 software (IBM Corp., Armonk, NY, USA). One-way
analysis of variance was used for multiple comparisons, and post
hoc testing was performed using Tukey if necessary, or comparisons
between two groups were made using Student's t-test. Data are
expressed as the mean ± standard deviation and mean ± standard
error of the mean. P<0.05 was considered to indicate a
statistically significant difference.
Results
Method validation (Tables II and III)
No endogenous interference was observed at retention
times of MTX. The calibration curves were linear over the
concentration range of 0.052–5.006 mg/l with correlation
coefficients of 0.9983 for plasma samples and 0.020–5.000 mg/l for
tissue samples, with correlation coefficients over 0.9981. RSD in
rat plasma and tissues were measured to be ranged between 2.3–6.3%
for intra-day precision, and 3.1–9.4% for inter-day precision. The
accuracy obtained was between 87.3 and 109.8% with RSD <8.6%.
The extraction recoveries of MTX in plasma and various tissues were
ranged from 77–102% with RSD <8.1%. Stability study demonstrated
that after 24 h at room temperature, three freeze-thaw cycles and 2
weeks of storage, the sample was stable and the RSD were within
9.8%.
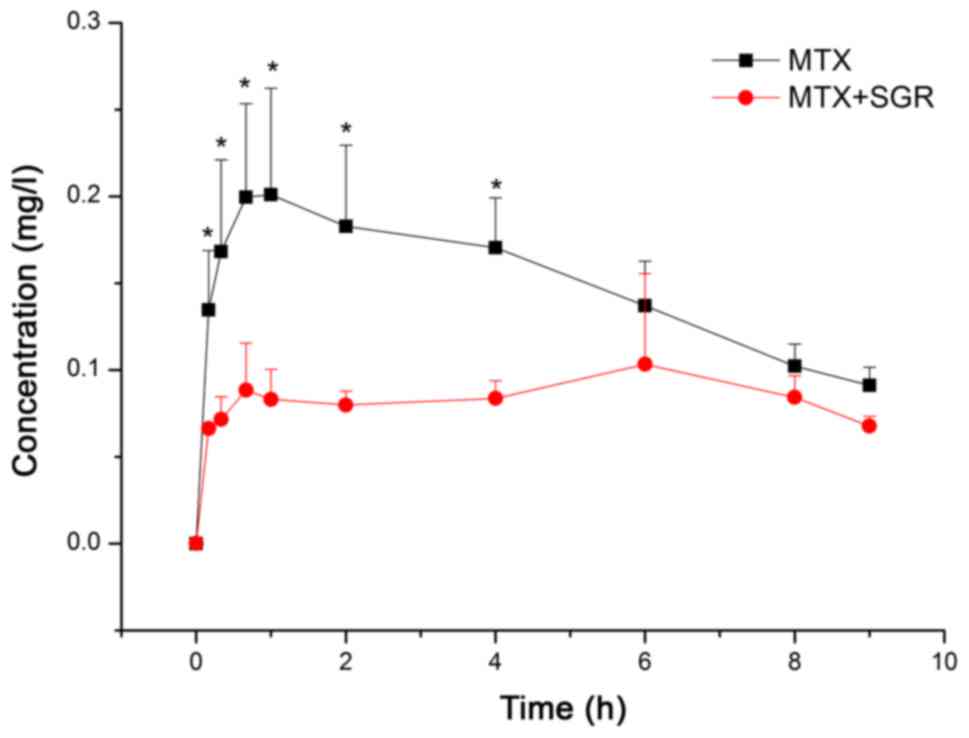
SGR affects the pharmacokinetics of
MTX significantly
The pharmacokinetics of mean concentration-time
curves of MTX are presented in Fig.
1. In general, the maximal MTX concentration in serum occurred
in 1 h and then gradually decreased to below detectable levels.
This is consistent with previous studies (35,36).
The plasma concentration profiles of MTX demonstrated nonlinear
pharmacokinetics. The corresponding pharmacokinetic parameters are
listed as the mean ± standard deviation and presented in Table IV. When co-administrated with SGR,
MTX demonstrated a much lower concentration than when used alone.
The Cmax was significantly decreased by 44.5% and the
T1/2, Tmax were significantly prolonged by
92.8 and 398.9%, respectively. Although SGR significantly decreased
AUC0-t of MTX (P<0.001), it still had marginal effect
on AUC0-∞, demonstrating an elimination inhibiting
effect. The concentration-time profile of MTX in the combination
group remained level, and very similar to the profile of sustained
release pharmaceuticals, in which the flat profile is as a result
of continuous slow absorption. Concentration levels peaked at 6 h,
indicating that there may be circulation between the gut and liver
(Fig. 1).
| Table IV.Pharmacokinetic parameters of MTX in
rats orally administered MTX alone and in combination with SGR (n=6
per group). |
Table IV.
Pharmacokinetic parameters of MTX in
rats orally administered MTX alone and in combination with SGR (n=6
per group).
| Parameters | MTXMTX + SGR |
|---|
|
AUC0-t/mg/h/l |
1.353±0.169 |
0.751±0.163c |
|
AUC0-∞/mg/h/l |
2.698±0.403 |
2.871±1.488 |
|
MRT0-t/h |
4.008±0.309 |
4.551±0.274 |
|
T1/2/h |
9.884±3.283 |
19.058±10.616a |
|
Cmax/mg/l |
0.218±0.059 |
0.113±0.047b |
| CL/L/h/kg |
2.271±0.370 |
2.663±1.440 |
|
Tmax/h |
0.902±0.683 |
4.5±2.665a |
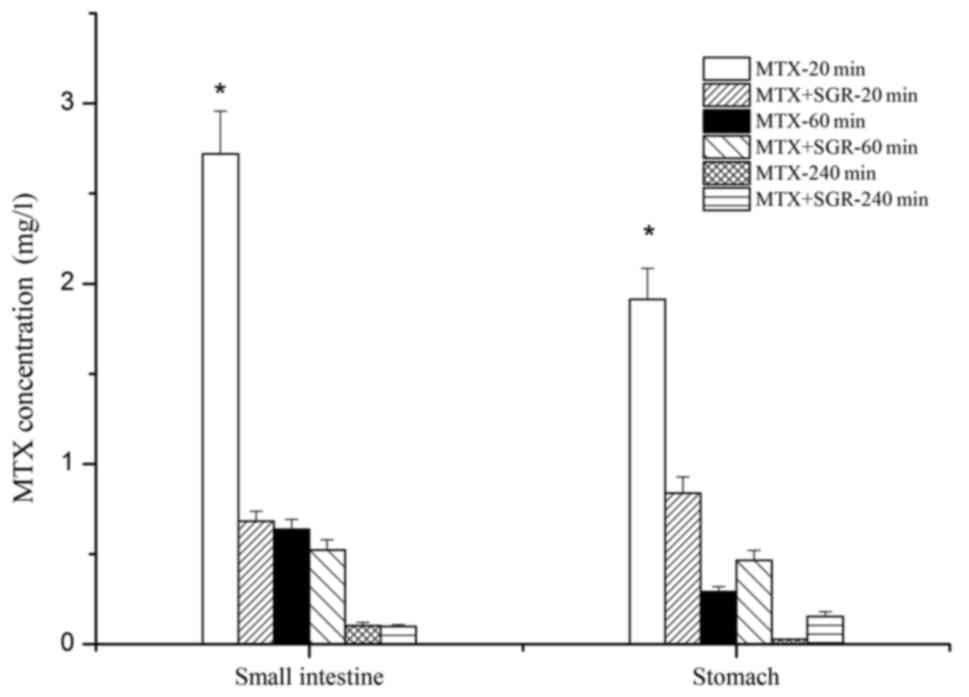
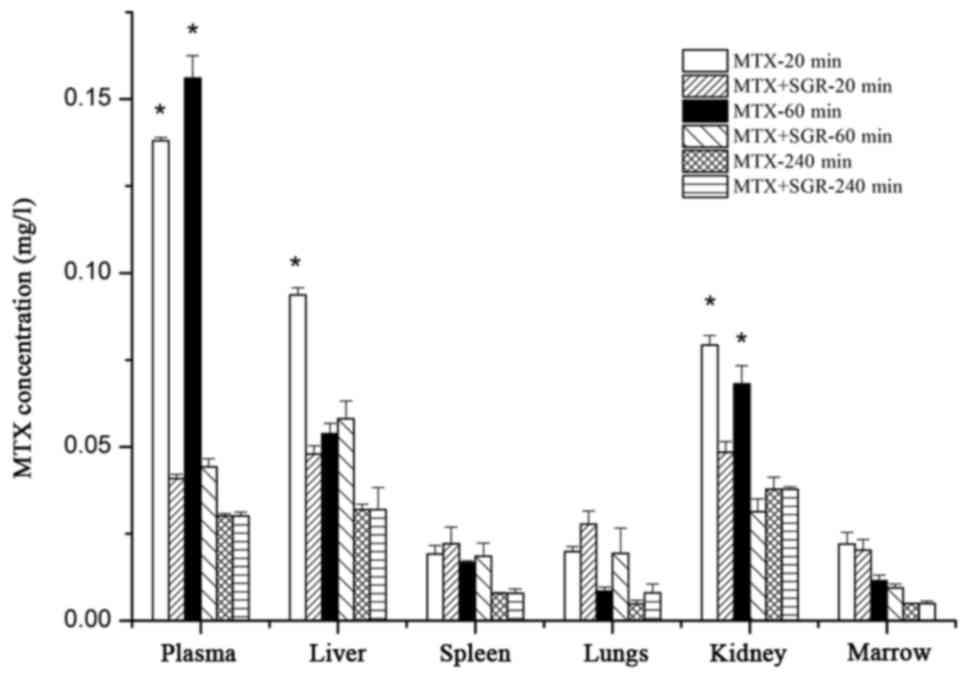
SGR affects tissue distribution of MTX
with a tissue dependent manner
The concentration of MTX in tissue homogenate at 20,
60 and 240 min after oral administration are presented in Figs. 2 and 3. When MTX was used alone, the
Cmax in majority tissues were 20 min, indicating that
MTX underwent a rapid and wide distribution from blood to tissues,
and this is in accordance with its wide curative effect to
different diseases. The highest concentration of MTX was observed
in the small intestine and stomach (Fig. 2), followed by the plasma, liver,
and kidney (Fig. 3). MTX
concentrations were relatively low in the lung, spleen and marrow
(Fig. 3), and the concentration of
MTX in the heart was too low to test, which is roughly consistent
with previous studies (37,38).
When co-administered with SGR, the concentration of
MTX in tissues changed in a tissue- and time-dependent manner.
Although the Tmax was at 20 min, the Cmax
decreased significantly compared with MTX used alone.
Cmax in the small intestine, stomach, plasma, liver and
kidney were decreased by 74.9, 56.2, 70.4, 48.9 and 40.0%,
respectively, at 20 min. Following that, the effect of SGR seemed
to weaken; at the 1-h time point, SGR decreased the concentration
of MTX in the plasma and kidney markedly, but increased the
concentration of MTX in the stomach and lung; no obvious
differences of MTX concentration were observed between the two
groups at 240 min. This indicated a much slower elimination in most
tissues when combined with SGR, and which is accorded with the
pharmacokinetic study.
On the whole, the total exposure of MTX was also
significantly reduced in the small intestine, stomach, plasma and
kidney by 61.6, 34.7, 63.3 and 46.1%, respectively. Notably, the
total exposure of MTX in the lung and spleen were increased by 82.9
and 21.0%, respectively. However, was no obvious change was
observed in the marrow.
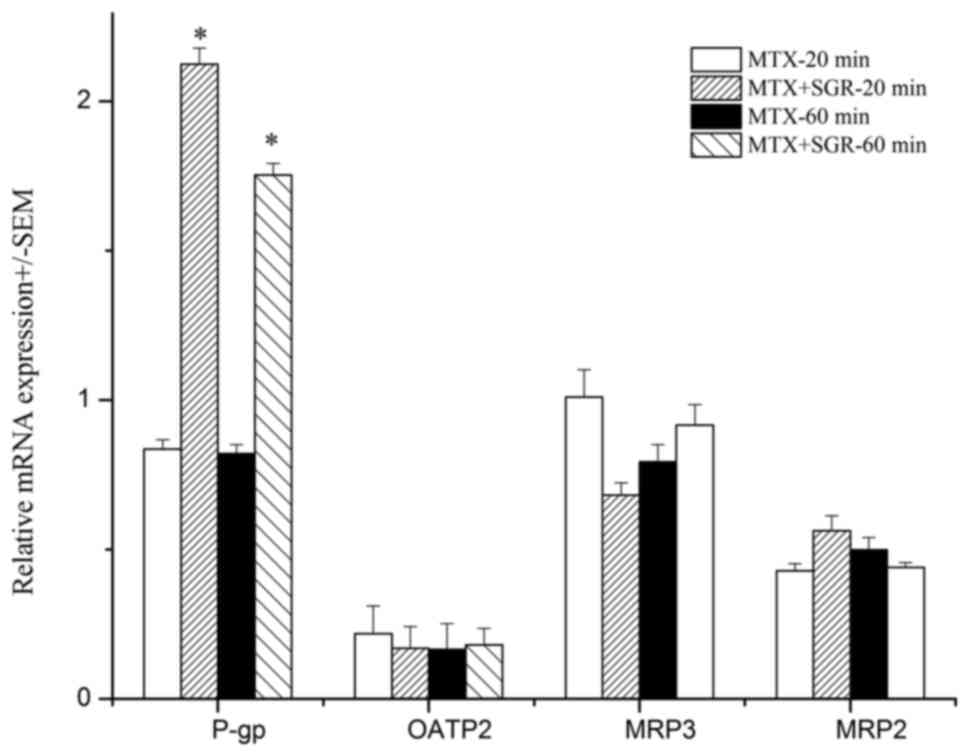
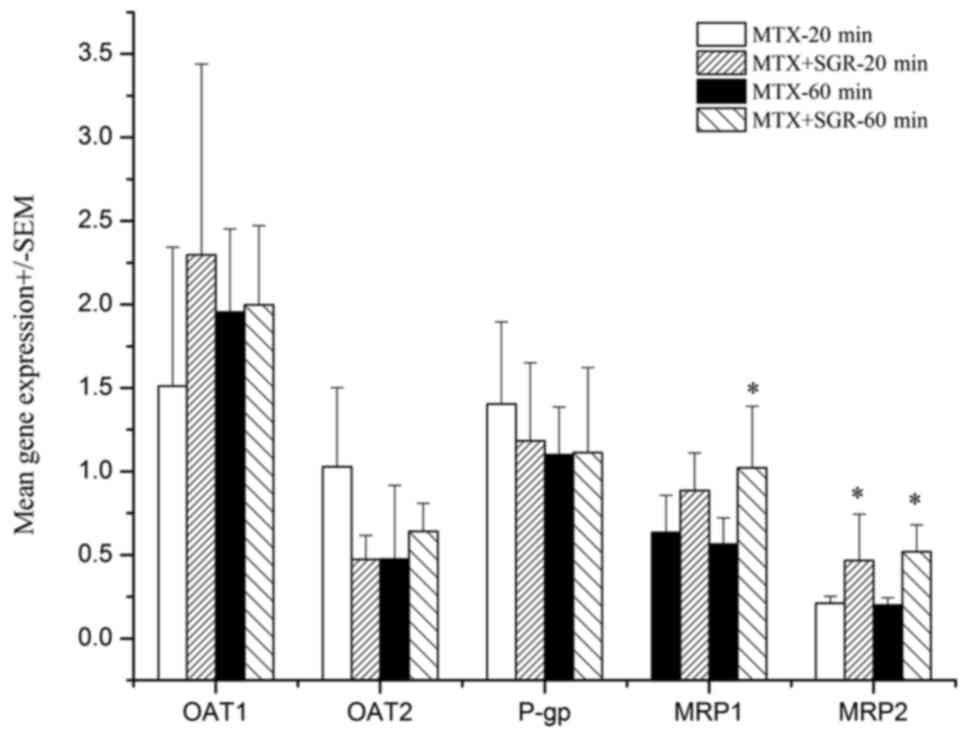
SGR enhances P-gp gene expression in
intestine but has a marginal effect on other transporters
As the effect of SGR on the in vivo behavior
of MTX mainly focused on absorption and excretion, the gene
expression of transporters which all transport MTX such as P-gp,
MRP3, organic anion transporting polypeptide (OATP2), MRP2 in the
intestine and P-gp, OAT1, OAT2, MRP1 and MRP2 in the kidney, were
studied. The results are presented in Figs. 4 and 5.
The effect of SGR on gene expression demonstrated a
time-, transporter- and tissue-dependent manner. SGR increased P-gp
mRNA expression in the small intestine by 2.54 times (P<0.05) at
both 20 and 60 min time points, but had marginal effects on the
gene expression of OATP2, MRP2 and MRP3 in the intestine at all the
time points (Fig. 4), indicating
that upregulation of P-gp expression is the main effect of
SGR-induced MTX absorption decreasing. However, different from the
results in intestine, SGR had a marginal effect on P-gp, OAT1 and
OAT2 expression in the kidney, but increased the expression of MRP2
and MRP3. The result is coincidence with the concentration
decreasing of MTX in kidney (Fig.
5). This indicated that SGR prolonged the retention time of MTX
in plasma by increasing the expression of MRP1 and MRP2. This may
be one of the reasons of the flat profile and low elimination rate
of MTX in plasma.
Discussion
SGR was originally recorded by ‘Diannan Materia
Medica’ in the Ming Dynasty of China (1368–1644), and officially
listed in the Chinese Pharmacopeia (2015 edition) (39). The stipulated prescription dose is
15–60 g, and when SGR is generally consumed in tea or soup, the
dosage often exceeds the prescribed dose. MTX and SGR are
frequently used combination in the clinic; however, the benefits
remain unclear (40). To the best
of our knowledge, the present study was the first to examine the
in vivo effects of SGR on the fate of MTX, and the results
demonstrated that SGR affected the absorption, distribution and
elimination significantly, and may induce significant DHI.
Drug concentration in plasma is significantly
reduced in the intestines, stomach, liver and kidney, and it was
hypothesized that SGR may affect the MTX treatment effect when used
in the treatment of psoriasis, digestive tract cancer and systemic
lupus erythematosus. Additionally, when patients are receiving MTX
therapy and taking SGR at the same time, it is suggested that the
dosing interval should be extended to prevent unnecessary toxic
effect, due to the significant inhibition of the elimination of MTX
by SGR.
In the present study, although SGR significantly
decreased the concentration of MTX in most tissues, its
concentration in the lung, spleen and marrow were not reduced; it
increased the drug concentration of MTX in lung and spleen
significantly. Therefore, in the treatment of various types of
cancer, such splenic carcinoma, osteosarcoma, acute leucocythemia,
malignant lymphoma and multiple myeloma (41), MTX co-administration with SGR may
be helpful to enhance its tumoricidal effect while decreasing the
toxicity such as nausea, vomiting, diarrhea and stomatitis.
MTX is the substrate of many transporters, as
previously described. The efficacy and toxicity of MTX may be
changed drugs used in combination affect transporter activity
(42). Transporters have different
expression levels in different tissues, and our previous study
demonstrated that the effect of drugs on the activity of
transporters depends on the protein amount (data not shown)
(43,44). The RT-qPCR results indicated that
SGR increased P-gp expression by 2.5 times in the intestine; thus,
it was hypothesized that SGR-induced gene expression of P-gp may be
the reason for MTX low absorption in intestine, and much lower
Cmax in blood. This is consistent with a previous report
that P-gp is associated with clinical responses to MTX (45,46)
On the other hand, in the present study, SGR increased the
expression of MRP1 and MRP2 in the kidney, but had a marginal
effect on P-gp. This may be because P-gp had much higher expression
in the intestine than in the kidney, and vice versa. This may
partially explain the flat profile of MTX concentration over time.
Elimination of drugs from blood is the total effect of all tissues,
so the mechanism requires further study.
In recent years, flavonoids-rich botanical products
have been used as dietary supplements worldwide. However, their
safety remains unanswered (47).
Additionally, the pharmacokinetics of other acidic pharmaceuticals
such as probenecid, ciprofloxacin and penicillin, which ware
putative substrates of P-gp, may also be affected by concurrent use
of SGR (48,49) As the side effect of drugs raised
concern, herbal treatment has attracted increasing attention,
particularly a combination of herbs and drugs. Therefore,
investigations into herb-drug interactions HDI are urgently
required.
In conclusion, to the best of our knowledge, the
present study demonstrated for the first time the potential
benefits of co-administration of MTX with SGR. Co-administration of
SGR may be beneficial for therapy of lung cancer and splenic
carcinoma, osteosarcoma, and liver diseases, but may reduce the
therapeutic effect of treating cancer in the digestive tract,
systemic lupus erythematosus and psoriasis (50–54).
The herb-drug interaction may be associated with the activity
change of transporters.
Acknowledgements
The present study was supported by the Science and
Technology Department Program of Guangdong Province of China (grant
no. 2013B090700015), the Teamwork Project of Natural Science
Foundation of Guangdong Province of China (grant no.
S2013030011515) and the project of Traditional Chinese Medicine
Hospital of Guangdong Province (grant nos. YK2013B1N11 and
YN2014ZHR211).
References
|
1
|
Jolivet J, Cowan KH, Curt GA, Clendeninn
NJ and Chabner BA: The pharmacology and clinical use of
methotrexate. N Engl J Med. 309:1094–1104. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Samarasekera E, Sawyer L, Parnham J and
Smith CH: Guideline Development Group: Assessment and management of
psoriasis: Summary of NICE guidance. BMJ. 345:e67122012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kuroda T, Namba K, Torimaru T, Kawashima K
and Hayashi M: Species differences in oral bioavailability of
methotrexate between rats and monkeys. Biol Pharm Bull. 23:334–338.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Carneiro-Filho BA, Lima IP, Araujo DH,
Cavalcante MC, Carvalho GH, Brito GA, Lima V, Monteiro SM, Santos
FN, Ribeiro RA and Lima AA: Intestinal barrier function and
secretion in methotrexate-induced rat intestinal mucositis. Dig Dis
Sci. 49:65–72. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Duman DG, Kumral ZN, Ercan F, Deniz M, Can
G and Cağlayan Yeğen B: Saccharomyces boulardii ameliorates
clarithromycin- and methotrexate-induced intestinal and hepatic
injury in rats. Br J Nutr. 110:493–499. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Alarcón GS, Tracy IC and Blackburn WD Jr:
Methotrexate in rheumatoid arthritis. Toxic effects as the major
factor in limiting long-term treatment. Arthritis Rheum.
32:671–676. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang J, Li Q, Ivanochko G and Huang Y:
Anticancer effect of extracts from a North American medicinal
plant-wild sarsaparilla. Anticancer Res. 26:2157–2164.
2006.PubMed/NCBI
|
|
8
|
Galhena PB, Samarakoon SR, Thabrew MI,
Weerasinghe GA, Thammitiyagodage MG, Ratnasooriya WD and Tennekoon
KH: Anti-inflammatory activity is a possible mechanism by which the
polyherbal formulation comprised of Nigella sativa (seeds),
Hemidesmus indicus (root), and Smilax glabra (rhizome) mediates its
antihepatocarcinogenic effects. Evid Based Complement Alternat Med.
2012:1086262012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gao Y, Su Y, Qu L, Xu S, Meng L, Cai SQ
and Shou C: Mitochondrial apoptosis contributes to the anti-cancer
effect of Smilax glabra Roxb. Toxicol Lett. 207:112–120. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ooi LS, Sun SS, Wang H and Ooi VE: New
mannose-binding lectin isolated from the rhizome of sarsaparilla
Smilax glabra Roxb. (Liliaceae). J Agric Food Chem. 52:6091–6095.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lu CL, Zhu W, Wang M, Xu XJ and Lu CJ:
Antioxidant and anti-inflammatory activities of phenolic-enriched
extracts of Smilax glabra. Evid Based Complement Alternat Med.
2014:9104382014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Jiang J and Xu Q: Immunomodulatory
activity of the aqueous extract from rhizome of Smilax glabra in
the later phase of adjuvant-induced arthritis in rats. J
Ethnopharmacol. 85:53–59. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Xia D, Fan Y, Zhang P, Fu Y, Ju M and
Zhang X: Protective effects of the flavonoid-rich fraction from
rhizomes of Smilax glabra Roxb. On carbon tetrachloride-induced
hepatotoxicity in rats. J Membr Biol. 246:479–485. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Roubille C, Richer V, Starnino T, McCourt
C, McFarlane A, Fleming P, Siu S, Kraft J, Lynde C, Pope J, et al:
The effects of tumour necrosis factor inhibitors, methotrexate,
non-steroidal anti-inflammatory drugs and corticosteroids on
cardiovascular events in rheumatoid arthritis, psoriasis and
psoriatic arthritis: A systematic review and meta-analysis. Ann
Rheum Dis. 74:480–489. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen L, Yin Y, Yi H, Xu Q and Chen T:
Simultaneous quantification of five major bioactive flavonoids in
Rhizoma Smilacis Glabrae by high-performance liquid chromatography.
J Pharm Biomed Anal. 43:1715–1720. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shi L, Xu L, Yang Y, Song H, Pan H and Yin
L: Suppressive effect of modified Simiaowan on experimental gouty
arthritis: An in vivo and in vitro study. J Ethnopharmacol.
150:1038–1044. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Smith CH and Barker JN: Psoriasis and its
management. BMJ. 333:380–384. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Y: Clinical observation of combining
traditional Chinese and western medicine treatment rheumatoid
arthritis. J New Chin Med. 47:103–105. 2015.
|
|
19
|
Goldman ID and Matherly LH: The cellular
pharmacology of methotrexate. Pharmacol Ther. 28:77–102. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Henderson GB: Folate-binding proteins.
Annu Rev Nutr. 10:319–335. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
de Graaf D, Sharma RC, Mechetner EB,
Schimke RT and Roninson IB: P-glycoprotein confers methotrexate
resistance in 3T6 cells with deficient carrier-mediated
methotrexate uptake. Proc Natl Acad Sci USA. 93:1238–1242. 1996;
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Masuda M, I'Izuka Y, Yamazaki M, Nishigaki
R, Kato Y, Ni'inuma K, Suzuki H and Sugiyama Y: Methotrexate is
excreted into the bile by canalicular multispecific organic anion
transporter in rats. Cancer Res. 57:3506–3510. 1997.PubMed/NCBI
|
|
23
|
Kusuhara H and Sugiyama Y: Role of
transporters in the tissue-selective distribution and elimination
of drugs: Transporters in the liver, small intestine, brain and
kidney. J Control Release. 78:43–54. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ranganathan P and McLeod HL: Methotrexate
pharmacogenetics: The first step toward individualized therapy in
rheumatoid arthritis. Arthritis Rheum. 54:1366–1377. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
El-Sheikh AA, van den Heuvel JJ,
Koenderink JB and Russel FG: Interaction of nonsteroidal
anti-inflammatory drugs with multidrug resistance protein (MRP)
2/ABCC2- and MRP4/ABCC4-mediated methotrexate transport. J
Pharmacol Exp Ther. 320:229–235. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sweet DH, Bush KT and Nigam SK: The
organic anion transporter family: From physiology to ontogeny and
the clinic. Am J Physiol Renal Physiol. 281:F197–F205.
2001.PubMed/NCBI
|
|
27
|
Sweet DH: Organic anion transporter
(Slc22a) family members as mediators of toxicity. Toxicol Appl
Pharmacol. 204:198–215. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang XD, Meng MX, Gao LB, Liu T, Xu Q and
Zeng S: Permeation of astilbin and taxifolin in Caco-2 cell and
their effects on the P-gp. Int J Pharm. 378:1–8. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Piskula MK: Factors affecting flavonoids
absorption. Biofactors. 12:175–180. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
O'Leary KA, Day AJ, Needs PW, Mellon FA,
O'Brien NM and Williamson G: Metabolism of quercetin-7- and
quercetin-3-glucuronides by an in vitro hepatic model: The role of
human beta-glucuronidase, sulfotransferase,
catechol-O-methyltransferase and multi-resistant protein 2 (MRP2)
in flavonoid metabolism. Biochem Pharmacol. 65:479–491. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Van Aubel RA, Masereeuw R and Russel FG:
Molecular pharmacology of renal organic anion transporters. Am J
Physiol Renal Physiol. 279:F216–F232. 2000.PubMed/NCBI
|
|
32
|
Hirohashi T, Suzuki H and Sugiyama Y:
Characterization of the transport properties of cloned rat
multidrug resistance-associated protein 3 (MRP3). J Biol Chem.
274:15181–15185. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang M, Chen W, Wang Z, Lu C and Zhu W:
HP-20 macroporous adsorption resin enrichment and purification of
total flavonoids of glabrous greenbrier rhizome. Chin Tradit Patent
Med. 37:2074–2078. 2015.(In Chinese).
|
|
34
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Jacobs SA, Stoller RG, Chabner BA and
Johns DG: 7-Hydroxymethotrexate as a urinary metabolite in human
subjects and rhesus monkeys receiving high dose methotrexate. J
Clin Invest. 57:534–538. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Kuijpers AL and van de Kerkhof PC:
Risk-benefit assessment of methotrexate in the treatment of severe
psoriasis. Am J Clin Dermatol. 1:27–39. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Oliverio VT and Zaharko DS: Tissue
distribution of folate antagonists. Ann N Y Acad Sci. 186:387–399.
1971. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Scheufler E, Zetler G and Iven H:
Pharmacokinetics and organ distribution of methotrexate in the rat.
Pharmacology. 23:75–81. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Chinese Pharmacopoeia Commission:
Pharmacopoeia of the People's Republic of China 2015. China Medical
Science and Technology Press; Bejing: 2015, (In Chinese).
|
|
40
|
Chinese Pharmacopoeia Commission:
Pharmacopoeia of the People's Republic of China, the First
Division. China Medical Science and Technology Press; Bejing: 2010,
(In Chinese).
|
|
41
|
Aquerreta I, Aldaz A, Giráldez J and
Sierrasesúmaga L: Methotrexate pharmacokinetics and survival in
osteosarcoma. Pediatr Blood Cancer. 42:52–58. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Chiang HM, Fang SH, Wen KC, Hsiu SL, Tsai
SY, Hou YC, Chi YC and Chao PD: Life-threatening interaction
between the root extract of Pueraria lobata and methotrexate in
rats. Toxicol Appl Pharmacol. 209:263–268. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhao R, Liu L, Wang Y and Xiao Z:
Vinegar-baked Radix Bupleuri modulates the cell membrane
constituents and inhibits the P-gp activity in rat hepatocytes. BMC
Complement Altern Med. 14:3572014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhao Y, Feng LM, Liu LJ, Zhang X and Zhao
RZ: Clerosterol from vinegar-baked radix bupleuri modifies drug
transport. Oncotarget. 8:21351–21361. 2017.PubMed/NCBI
|
|
45
|
Takatori R, Takahashi KA, Tokunaga D, Hojo
T, Fujioka M, Asano T, Hirata T, Kawahito Y, Satomi Y, Nishino H,
et al: ABCB1 C3435T polymorphism influences methotrexate
sensitivity in rheumatoid arthritis patients. Clin Exp Rheumatol.
24:546–554. 2006.PubMed/NCBI
|
|
46
|
Grabar P Bohanec, Logar D, Lestan B and
Dolzan V: Genetic determinants of methotrexate toxicity in
rheumatoid arthritis patients: A study of polymorphisms affecting
methotrexate transport and folate metabolism. Eur J Clin Pharmacol.
64:1057–1068. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Boušová I and Skálová L: Inhibition and
induction of glutathione S-transferases by flavonoids: Possible
pharmacological and toxicological consequences. Drug Metab Rev.
44:267–286. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Lin SP, Tsai SY, Hou YC and Chao PD:
Glycyrrhizin and licorice significantly affect the pharmacokinetics
of methotrexate in rats. J Agric Food Chem. 57:1854–1859. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Yang SY, Juang SH, Tsai SY, Chao PD and
Hou YC: St. John's wort significantly increased the systemic
exposure and toxicity of methotrexate in rats. Toxicol Appl
Pharmacol. 263:39–43. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Hirota BC, Paula CD, de Oliveira VB, da
Cunha JM, Schreiber AK, Ocampos FM, Barison A, Miguel OG and Miguel
MD: Phytochemical and antinociceptive, anti-inflammatory, and
antioxidant studies of Smilax larvata (Smilacaceae). Evid Based
Complement Alternat Med. 2016:98946102016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
She T, Zhao C, Feng J, Wang L, Qu L, Fang
K, Cai S and Shou C: Sarsaparilla (Smilax glabra Rhizome) extract
inhibits migration and invasion of cancer cells by suppressing
TGF-β1 pathway. PLoS One. 10:e01182872015. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
She T, Qu L, Wang L, Yang X, Xu S, Feng J,
Gao Y, Zhao C, Han Y, Cai S and Shou C: Sarsaparilla (Smilax glabra
Rhizome) extract inhibits cancer cell growth by S phase arrest,
apoptosis, and autophagy via redox-dependent ERK1/2 pathway. Cancer
Prev Res (Phila). 8:464–474. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Samarakoon SR, Thabrew I, Galhena PB and
Tennekoon KH: Modulation of apoptosis in human hepatocellular
carcinoma (HepG2 cells) by a standardized herbal decoction of
Nigella sativa seeds, Hemidesmus indicus roots and Smilax glabra
rhizomes with anti-hepatocarcinogenic effects. BMC Complement
Altern Med. 12:252012. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Ooi LS, Wong EY, Chiu LC, Sun SS and Ooi
VE: Antiviral and anti-proliferative glycoproteins from the rhizome
of Smilax glabra Roxb (Liliaceae). Am J Chin Med. 36:185–195. 2008.
View Article : Google Scholar : PubMed/NCBI
|