Introduction
The role of the sympathetic nervous system (SNS) in
inflammation is still not completely understood, although it is
well known that disturbed interaction between both contributes to
pathogenic chronic inflammatory diseases (1,2).
Evidence for the possibility of such interaction have been
reinforced since the discovery of the expression of
beta-2-adrenergic receptor (β2AR) on T and B lymphocytes,
macrophages, natural killer cells and neutrophils (3–6).
Coexistence of all β adrenoceptors (βAR) subtypes has been reported
in human peripheral blood mononuclear cells (PBMC) and erythrocytes
(7), but lymphocyte β1AR and β3AR
functionality in these cells has not been evidenced yet (8,9).
Stimulation of PBMC β2AR by catecholamines or selective
pharmacologic ligands differentially regulates activity depending
on cell activation and differentiation state, molecular signalling
pathway and cytokine microenvironment.
Since β2AR activity on circulating mononuclear cells
is related to the level of β2AR activity on solid tissues cells,
such as heart and skeletal muscle, mononuclear cells could be used
as markers to evaluate development and progression of systemic β2AR
(10). Recent studies suggested
that β2AR modulation could be relevant in the development of joint
diseases as rheumatoid arthritis (RA) (11–14),
adjuvant-induced arthritic (AA) (15), and immune hepatitis (16,17).
Thus, two different models of chronic inflammatory diseases were
selected (osteoarthritis (OA) and liver cirrhosis (LC)) to study
the potential relation between their progression and PBMC β2AR
functionality and genotype.
OA is the most common articular disorder
characterized by chronic inflammation of the joint lining. Although
OA inherently lacks the large scale systemic inflammatory response
that is a hallmark in rheumatoid arthritis (RA), this is suggestive
of low activation grade. In OA, the innervation pattern of
sympathetic and sensory nerve fibres is altered in adult joint
tissues and bone (18). It is now
believed that synovial inflammatory changes in OA are associated
with massive destruction of capillary and neuronal network with
preponderance of sympathetic over sensory fibres. This promotes an
increase in articular vessels adrenoceptor type towards β2AR
(19,20). Osteoblasts, osteoclasts,
mesenchymal stem cells, synovial fibroblasts, and different types
of chondrocytes produce distinct subtypes of adrenoceptors,
receptors for vasointestinal peptide, for substance P and
calcitonin gene-related peptide. Even more, cartilage integrity is
maintained by a balance from cytokine-driven anabolic and catabolic
processes (21). In fact, a novel
OA treatment consists in the use of biological molecules with
antiinflammatory properties (22,23).
Cirrhosis causes 90% of portal hypertension in the
Western world. This in turn triggers the formation of varices which
are present in 30% of patients with compensated cirrhosis and 60%
of those with decompensated cirrhosis (24). In an attempt to maintain effective
circulating volume, endogenous vasoconstrictor systems as
adrenergic are recruited. Adrenergic system releases catecholamines
as adrenaline, which binds to α (vasoconstrictor) and β
(vasodilator) adrenoceptors. Engagement of the β2AR activates a
cascade of signalling intermediates, including cAMP and protein
kinase A, leading to the phosphorylation of cellular proteins
including transcription factors that mediate metabolic processes
and gene expression (25).
Currently the most widely used modalities to prevent variceal
bleeding in LC patients are drugs as propranolol, a non-selective
beta-blocker (26–28). However, the prevalence of patients
‘non-responders’ ranges between 30 and 60%, suggesting changes in
the functional state of βAR receptors (29).
An interesting possibility is that underlying
genetic β2AR variability is involved in participant's
efficacy of beta-blockers treatment (30). Three functionally relevant
β2AR gene single-nucleotide polymorphisms (SNPs)
(Arg16Gly, rs1042713; Gln27Glu, rs1042714;
Thr164Ile, rs1800888) have been associated with joint
disorder, functional gastrointestinal disorders playing an
important role in vascular regulation (31–34)
and bronchial smooth muscle tone (35). In particular, Gln27Glu
variant is associated with bone health (36), RA (37,38),
functional gastrointestinal diagnoses and bowel symptoms severity
(39).
We analyzed β2AR functionality and genotype
(rs1042713, rs1042714, rs1800888) in PBMC in patients diagnosed
with OA and LC.
Materials and methods
Patients
A total of 30 OA and 52 LC patients, together with
26 healthy volunteers participated in the study. Blood samples were
drawn from anterocubital vein in the morning.
Ethical approval
Protocol was approved by the Clinical Research
Ethics Committee of Alicante Department of Health, General Hospital
(Alicante, Spain). All participants signed informed consent before
enrolment, and the study was performed according to the Declaration
of Helsinki.
OA patients
Patients from Primary Care of Alicante General
Hospital Department of Health with knee OA were included in this
study.
The inclusion criteria were as follows: Ages ranging
from 50 to 80 years; diagnosis of knee OA according to the criteria
established by the American College of Rheumatology (ACR) using
history, physical examination and radiographic findings, knee
X-rays in the last 12 months and a Kellgren-Lawrence (KL) OA grade
of 2 or more, based on the radiological severity (grade 1,
questionable narrowing of joint space and possible osteophytic
lipping; grade 2, definite osteophytes and possible narrowing of
joint space; grade 3, moderate multiple osteophytes, definite
narrowing of joints space, some sclerosis, and possible deformity
of bone contour; and, grade 4, large osteophytes, marked narrowing
of joint space, severe sclerosis, and definite deformity of bone
contour) (40).
Patients with infections, inflammatory diseases,
malignancies or patients using α- or β-adrenergic receptor agonists
or antagonists were excluded from the study.
Cirrhotic patients
Patients from Liver Unit of Alicante Department of
Health, General Hospital with LC were included in this study.
The inclusion criteria were as follows: Ages ranging
from 40 to 80 years; diagnosis of cirrhosis according to the
criteria established by Spanish Association for the Study of the
Liver (AEEH) and the Biomedical Research Network Center for Liver
and Digestive Diseases (CIBERehd) (41): Either liver biopsy or unequivocal
clinical, imaging and biochemical findings (e.g., complete blood
cell count, serum chemistries, liver function test, and coagulation
studies).
None of the patients had an established transjugular
intrahepatic portosystemic shunt (TIPS). Patients with systolic
blood pressure <100 mmHg bradycardia (heat rate <50/min),
obstructive airway disease or other contraindications for treatment
with propranolol were excluded from the study.
Patients were classified in two groups: Under
prophylaxis or treatment of first upper gastrointestinal bleeding
episode (‘primary prophylaxis’) or prophylaxis of recurrent
bleeding (‘secondary prophylaxis’). As non-bleeding varices are
generally asymptomatic, high hepatic venous pressure gradient
(HVPG) is the clinical gold standard for risk of formation
prediction (>12 mmHg) or rebleeding (HVPG >20 mmHg) and to
predict the response to β blocker antagonists during treatment of
portal hypertension (>20% fall from baseline of portal
pressure). Hence HVPG clinical routinely monitoring allow the
identification of patients who will be effectively protected
against the risk of bleeding (labeled as ‘responder’) and those
who, by not achieving a HVPG reduction by 20% of baseline or to ≤12
mmHg, present a very high risk of bleeding (‘non-responders’). LC
patients clinical data is presented in Table I.
 | Table I.Cirrhotic patient's demographic and
clinical data. |
Table I.
Cirrhotic patient's demographic and
clinical data.
| Clinical data | Cirrhotic primary
(n=22) | Cirrhotic secondary
(n=30) |
|---|
| Ascites
(yes/no) | 5/17 | 14/17 |
| HDA | 2/20 | 27/3 |
| Previous treatment
with beta-blockers (yes/no) | 2/20 | 16/14 |
| Total bilirubin
(mg/dl) |
1,31±0.9 |
1,64±0.8 |
| Serumalbumin
(g/dl) |
3,49±0.7 |
3,18±0.4 |
| Quick (%) |
76±16 |
68±14 |
| Creatinine
(mg/dl) |
0,9±0,4 |
0,8±0,2 |
| Hemoglobin
(g/dl) | 13,02±2,1 | 11,75±2,2 |
| Hematocrit (%) |
39±6 |
36±6 |
| Platelets
(103/mm3) |
102±58 |
91±51 |
| Glucose
(mg/dl) |
113±51 |
106±28 |
| Systolic arterial
pressure (mmHg) |
128,0±17,7 |
130,2±18,7 |
| Diastolic arterial
pressure (mmHg) |
81,7±10,7 |
77,2±12,2 |
| Heartrate
(bpm) |
74,6±16,6 |
74,5±11,3 |
| Wedged hepatic
venous pressure (mmHg) |
22,9±5,4 |
25,4±4,2 |
| Free hepatic venous
pressure (mmHg) |
8,1±3,8 |
8,8±3,7 |
| Hepatic venous
pressure gradient pre (mmHg) |
15±4,9 |
17±3,3 |
| Hepatic venous
pressure gradient post (mmHg) |
12±3,6 |
15±4,3 |
In patients with previous variceal bleeding,
investigations were made at least 7 days after the complete
recovery of bleeding.
Controls subjects
A total of 26 healthy controls were recruited
through blood donors from the same geographical areas as patients,
and were matched to patients according ethnicity (at least 2
generations from the same area). None of the subjects in the
healthy control group had any clinically significant abnormality
shown by routine history, physical examination, or laboratory
tests.
Determination of basal and stimulated
intracellular cAMP
PBMC were isolated from EDTA venous blood by Percoll
density gradient centrifugation. Activation of β2AR leading to an
increase in the intracellular level of cyclic adenosine
monophosphate (cAMP, pmol/ml/106 cells) by increasing
adenylate-cyclase (AC) activity was evaluated in duplicates by cAMP
determination using a competitive Enzyme Immunoassay (EIA)
according to laboratory procedures and manufacturer guidelines
(Cayman Chemical Company, Ann Arbor, MI, USA).
Cells were counted in a Coulter Counter and with a
Neubauer chamber. Viability was determined by trypan blue exclusion
and ranged between 94–98%. Cells were incubated as described by
Sondergaard et al (42).
Aliquots of 1×106 PBMC were rinsed with
Phosphate-buffered saline (1× PBS, pH 7.4, containing 135 mM NaCl,
5.4 mM KCl, 1.4 mM MgSO4, 1.4 mM CaCl2, 0.18
mM sodium phosphate) and 3% (wt/vol) of bovine serum albumin (BSA)
fraction V (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany)
(PBS-BSA) at room temperature. Phosphodiesterases were inhibited by
preincubation at 37°C for 30 min with 1 mM isobutyl-methyl-xanthine
(IBMX) (Sigma-Aldrich; Merck KGaA). Then, cells were stimulated
with different concentrations of isoproterenol (ISO) ranging from
10−9 to 10−4 mM or vehicle for 15 min.
Stimulation was stopped at 100°C water bath for 3 min. Samples were
centrifuged for 5 min at 3500 rpm and disrupted by sonication 3×15
sec (model SM25E-MT; Branson Ultrasonics Corporation, Geneva,
Switzerland). Lysates were immediately frozen and stored at −80°C
until EIA analysis was performed as described previously.
On the day of the assay, samples were thawed at room
temperature for 25–30 min and centrifuged at 4°C at 3,500 rpm for
10 min to remove insoluble material. cAMP was measured in the
supernatant using a EIA. cAMP increase was calculated by
subtraction of values determined in IBMX preincubated samples. All
assays were performed in duplicate.
DNA extraction and beta-adrenergic
genotyping
Blood samples from OA and LC patients and healthy
controls were collected and genomic DNA was extracted from isolated
PBMC using QIAamp® DNA Midi Kit according to
manufacturer's instructions.
Genomic DNA was genotyped for SNPs within the
β2AR gene locus. Three SNPs with high frequency of
polymorphism in the human population (>20% prevalence) and
located within the coding region for gene were chosen. The known
functional SNP rs1042713, rs1042714 and rs1800888 are well-studied
common non-synonymous SNPs (43,44).
β2AR genotype at positions 16, 27 and 164 was
determined by polymerase chain reaction (PCR) and sequenced by
Thermosequenase Primer Cycle kit (Amersham Pharmacia Biotechnology,
Piscataway, NJ, USA). PCR was performed in a final volume of 25 µl
containing 100–200 ng DNA, 0.2 mM of each dNTP, 1X de reaction
buffer (50 mM KCl and 20 mM Tris-HCl, pH 8.4), 1.5 mM
MgCl2, 1 U Taq DNA polimerase, 10% DMSO and 200 nM of
each primer. Temperature cycling was 94°C for 30 sec, 61°C for 45
sec, and 72°C for 45 sec for 30 cycles. In total, 10 µl of the PCR
products were visualized on a 1% agarose gel stained with ethidium
bromide. Computer analysis of all SNP combinations in the human EST
database (dbEST release 030405, 6,053,112 human entries) was
performed using BLAST (National Library of Medicine, Bethesda, MD,
USA). Complete nucleotide sequence of β2AR gene was used (NM
000024) to design the primers (Primer 3; UCSD, San Diego, CA,
USA).
Western blotting
To determine whether cAMP concentration changes in
PBMC from patients was associated with variations in
immunodetectable β2AR protein, quantitative Western blotting
analysis was performed.
After treatment with isoproterenol, cells were lysed
and protein was extracted using RIPA buffer (50 mM Tris-HCl pH 7.4;
150 mM NaCl, 1 mM EDTA, 0.25% Na-deoxycholate, 1% NP-40, 1 mM PMSF,
1 mM sodium orthovanadate, 1 µg/ml leupeptin, 1 µg/ml aprotinin,
and 1 µg/ml pepstatin). Protein concentration was determined by BCA
assay and samples were separated on 12% SDS-PAGE gels, and
transferred onto Hybond-enhanced chemiluminescence (ECL)
nitrocellulose membranes. Membranes were probed with antibodies
against β2AR (R11E1, sc-81577; Santa Cruz Biotechnology, Inc.,
Dallas, TX, USA) of human origin. Protein bands were observed using
ECL and specific bands were detected with X-film according to
procedures of Proteomics and Genomics Division, Research Technical
Facility of University of Alicante (Alicante, Spain).
Spot detection and quantification was performed
using Progenesis Same Spots software according to manufacturer's
instructions (Nonlinear USA,. Inc., Durham, NC, USA). Two
individual gel replicates from each subject were used for the
analysis. Results were expressed as relative arbitrary units (AU)
according to procedure previously described (45), using as standard samples from 4
healthy subjects. GAPDH was used as endogenous control.
Statistical analysis
Quantitative data is expressed as mean ± standard
deviation (SD). Differences between groups were analysed using the
T-Student or non-parametric Mann-Whitney U-test according to
normality. Qualitative variables are expressed as frequency or
percentage and differences between groups were evaluated using
χ2 test. A comparison of independent single variables
between the groups was calculated by one way analysis of variance
(ANOVA) followed by Turkey's procedure. When normality test failed,
Kruskal-Wallis one-way ANOVA on ranks was used. A two-tailed
P<0.05 was considered to indicate a statistically significant
difference.
Results
Patients and control subjects
Thirty OA patients (age, 70±8 years; female, 78%;
median (min, max) OA duration, 6 (1–29)
years) were included in this study. A total of 12% were diabetic,
14% hypertensive, 8% dislipemic and 9% BMI >30 kg/m2.
Mainly category of KL radiological severity was 3–4 (90%) grades
and 15 (54%) patients required knee joint replacement (76% KL grade
4). Regular current use of analgesic (acetaminophen, dipyrone), and
non-steroidal anti-inflammatory drugs (NSAIDs: Ibuprofen, naproxen
or celecoxib) was very common (21 and 50%, respectively), followed
by chondroitin sulphate (12%), glucosamine (6%) and tramadol
(2%).
A total of 52 LC patients (age, 54±11 years;
females, 13.5%) were submitted to the hospital clinic for HVPG
determination and were included in the study. Alcohol was actively
consumed by 11.5% of patients. Scores for Model for End-stage Liver
Disease (MELD) were 11±4 and Child-Pugh 7±2, respectively. In
total, 37% patients were previously treated with beta-blockers and
50% exhibited clinical response to propranolol (46).
A total of 26 healthy human volunteers (aged 59±13
years; female 50%) participated in the present study. They had
normal blood cell counts, normal liver and kidney function test
results, and normal findings on physical examination.
Basal and stimulated intracellular
cAMP
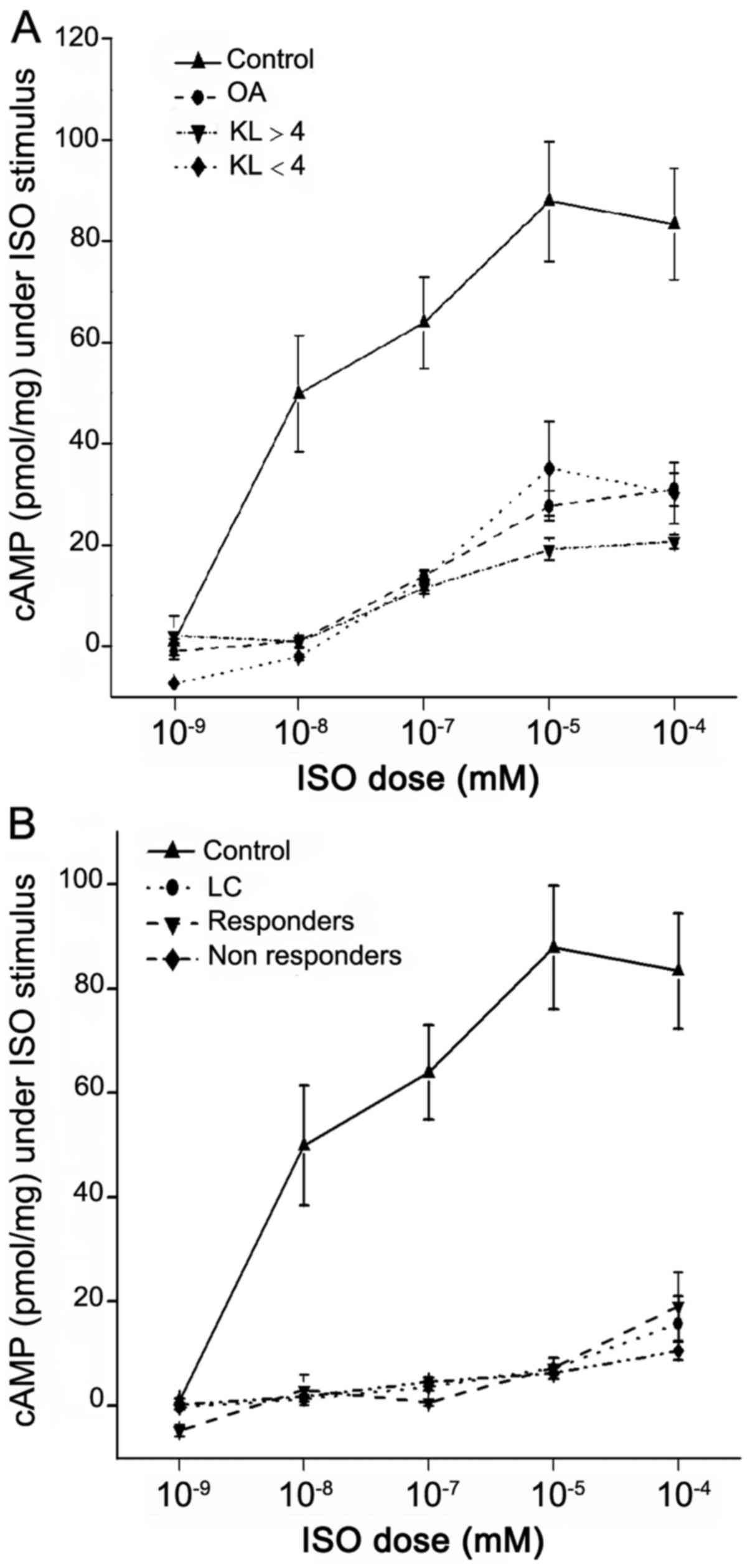
PBMC from control group stimulated with different
concentrations of isoproterenol (10−9 to 10−4
mM), showed a significant increase in cAMP production in a
dose-dependent manner with a maximum response between
10−5 to 10−4 mM (Fig. 1A and B). Isoproterenol induced a
significantly lower increase in cAMP concentration in OA and LC
patients (44±28 and 14±15.5 pmol/ml/106 cells
respectively) vs. controls (90±66 pmol/ml/106 cells,
P<0001) at isoproterenol 10−5 mM stimulus (Fig. 1A and B, respectively).
OA patients with severity KL grade 4 (n=17)
presented a smaller response than lower KL severity grades (n=6)
(38±21 and 61±42 pmol/ml/106 cells at isoproterenol
10−5 mM stimulus, respectively, P=0,06) (Fig. 1A). We observed a relevant (67%) and
significant reduction in cAMP increase in KL grade 4 with knee
replacement patients (n=12) compared with non-surgery patients
(n=5) (30±14 vs. 52±23 pmol/ml/106 cells, respectively,
P=0046).
Cirrhotic patients have a significant decrease in
β2AR-mediated AC activity stimulation, similar in patients with
primary or secondary prophylaxis and in responder or non-responder
cirrhotic patients (Fig. 1B).
β2AR genotyping
Table II shows the
genotypes frequencies, alleles, and carrier states at amino acid
positions 16, 27 and 164 of the β2AR gene.
| Table II.Polymorphisms and allele frequencies
of β2AR genotype analyzed. |
Table II.
Polymorphisms and allele frequencies
of β2AR genotype analyzed.
|
|
| Osteoarthritis | Liver
cirrhosis |
|---|
|
|
|
|
|
|---|
| SNP | Control | Naïve joint
replacement | Knee joint
replacement | Total | Responder | Non-responder | Total |
|---|
| Gly16Arg |
|
|
|
|
|
|
|
| AA | 19 (73%) | 10 (76%) | 9
(64%) | 19 (70%) | 9
(43%) | 17 (55%) | 26 (58%) |
| GA | 0 | 0 | 0 | 0 | 2
(9.5%) | 3
(10%) | 5
(11%) |
| GG | 7
(27%) | 3
(24%) | 5
(36%) | 8
(30%) | 7
(33%) | 7
(22%) | 14 (31%) |
| Allele
G (Gly16) | 27% | 23% | 36% | 30% | 44% | 31% | 37% |
| Gln27Glu |
|
|
|
|
|
|
|
| CC | 16 (62%) | 9
(69%) | 6
(42%) | 15 (58%) | 10 (47%) | 15 (48%) | 25 (55%) |
| CG | 6
(23%) | 1 (7%) | 5
(36%) | 6
(23%) | 6
(28%) | 7
(23%) | 13 (29%) |
| GG | 4
(15%) | 2
(14%) | 3
(21%) | 5
(19%) | 2
(9,5%) | 5
(16%) | 7
(16%) |
| Allele
G (Glu27) | 27% | 19% | 42% | 31% | 28% | 31% | 30% |
| Thr164Ile |
|
|
|
|
|
|
|
| CC | 21 (81%) | 13
(100%) | 12 (92%) | 25 (96%) | 17 (81%) | 26 (84%) | 43 (96%) |
| CT | 2 (8%) | 0 | 1 (7%) | 1 (4%) | 1
(65%) | 1 (3%) | 2 (4%) |
| TT | 3
(11%) | 0 | 0 | 0 | 0 | 0 | 0 |
| Allele
T (Thr164) | 15% | 0% | 4% | 2% | 3% | 2% | 2% |
The distribution of expected and observed
frequencies of the different genotypes at the different amino acid
positions followed the Hardy-Weinberg equilibrium both in patients
and controls. Minor allele frequencies in our Caucasian Spanish
sample from Alicante Department of Health, General Hospital were
Gly16 (allele G, 0, 24-0, 44), Glu27 (allele G, 0, 19-0, 38) and
Ile164 (allele T, 0, 00-0, 15).
Carriage of Arg16, Gln27 and Ile164 was more
prevalent in controls, OA and LC patients. Even though we observed
some differences in allele frequency i.e., a higher frequency of G
allele (Gly16) in LC patients, especially in responders; however,
none of these differences were statistically significant probably
due to the reduced sample size.
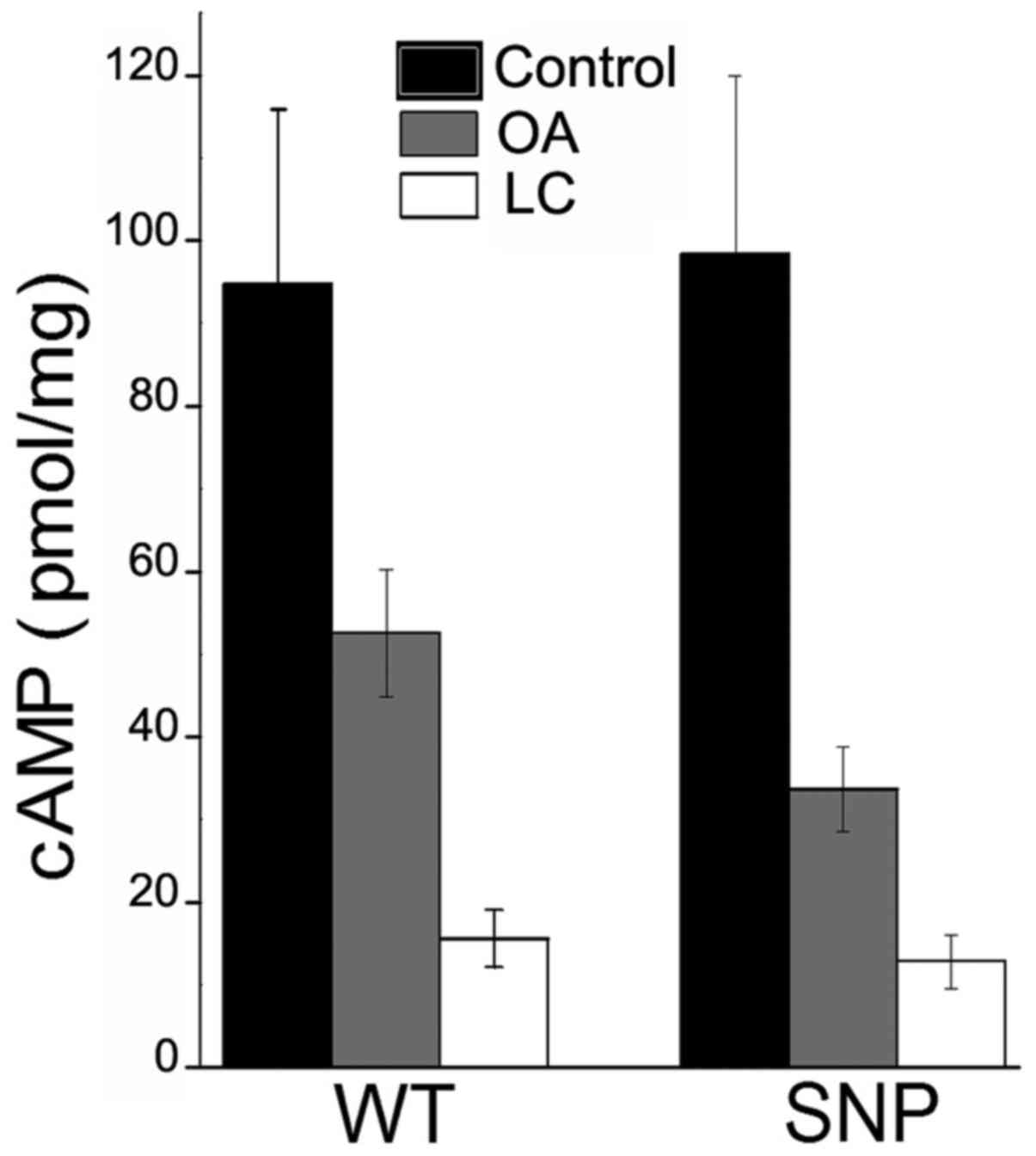
In global, subjects with any of the β2AR SNPs
analyzed shown a non-significant decrease in cAMP increase (mean ±
SD) at isoproterenol 10−5 mM vs. wild type (WT)
(Fig. 2): In controls (94±70 vs.
85±64 pmol/ml/106 cells, P=0.753), OA (52±31 vs. 34±19
pmol/ml/106 cells, P=0.054) and LC patients (15±17 vs.
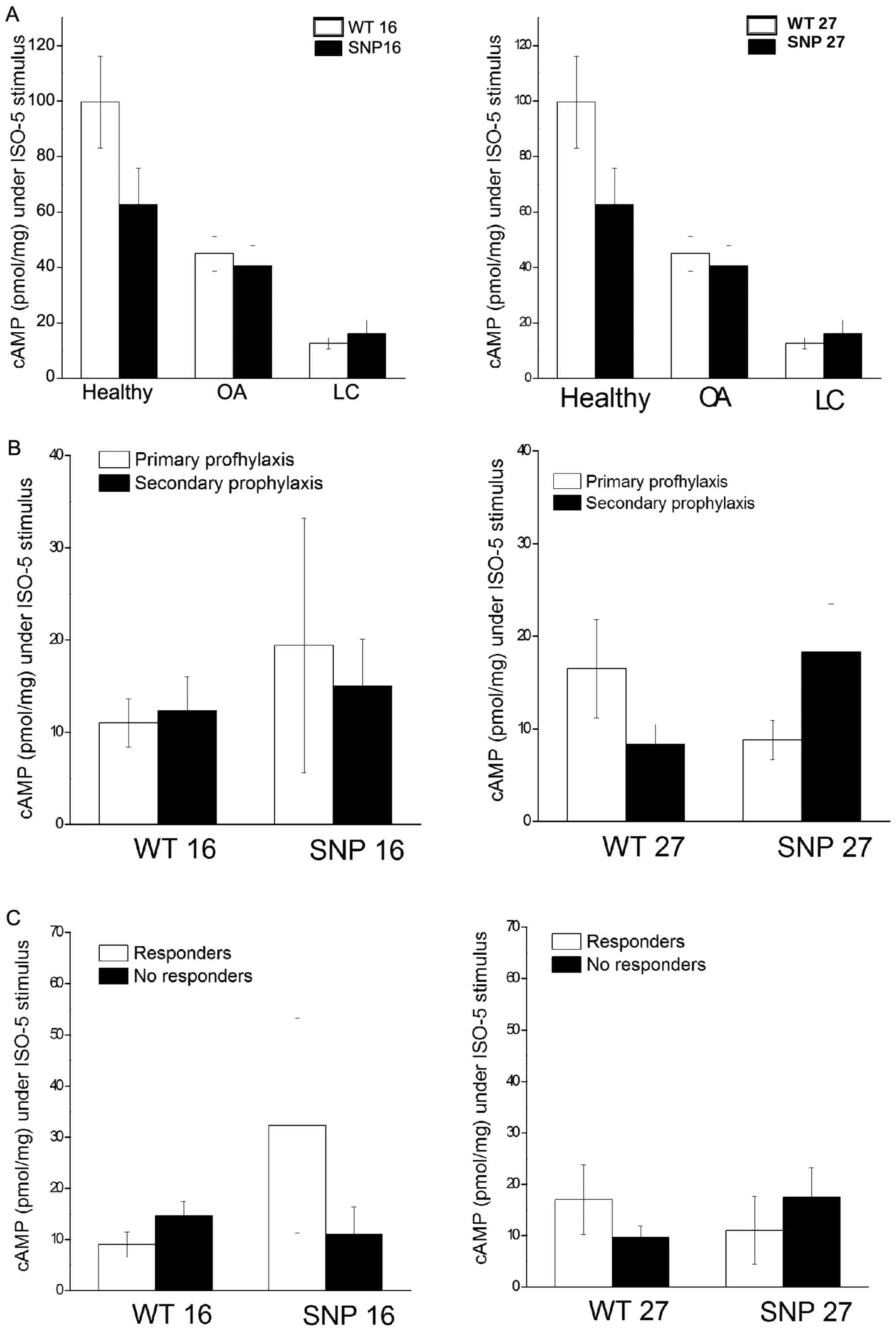
13±16 pmol/ml/106 cells, P=0.718) (Fig. 3A). The prevalence of the different
genotypes did not differed between patients according to any
clinical variable in both models of chronic inflammation (Fig. 3B and C). Combination of
Arg16+-Gln27+ shown a decreased cAMP increase
stimulus in controls (n=5), OA (n=13) and cirrhotic (n=6) (50±32,
38±21 and 14±19 pmol/ml/106 cells, respectively,
P=0.094) (data not shown). The bigger decrease AC stimulus was
evidenced for the Arg16+-Gln27+ in controls
(48% β2AR agonism stimulus blocked) and for
Arg16−-Gln27+ in OA (51% agonism stimulus
blocked). In cirrhotic (13% agonism stimulus blocked) the stimulus
was the same for both Arg16−-Gln27+ or
Arg16+-Gln27+.
β2AR expression
Western blot detection of β2AR showed a decreased
expression above 0.411-fold for OA and 0.845-fold for LC compared
to healthy controls (data not shown).
Discussion
In this study we showed that the functional activity
of PBMC β2AR from patients with different types of chronic
inflammatory diseases (OA and LC) was significantly decreased in
comparison with healthy volunteers. According to severity of
diseases, OA patients receptor showed a higher loss of
functionality in KL grade 4 and knee joint replacement. However, in
LC patients there was no significant relation between β2AR
functionality and severity of disease. These differences were not
related to the β2AR genotype analyzed.
We evaluated mononuclear cell β2AR responsiveness to
isoproterenol to test the hypothesis that patients with chronic
inflammatory diseases have a β2AR abnormality. In basal conditions
(no pharmacologic stimulation of the receptor), intracellular cAMP
levels showed no significant difference between OA and LC patients
and controls. However, the response to β2AR stimulation with an
agonist was significantly lower in patients. At high isoproterenol
concentrations (10−5 mM) AC activation response were a
50 and 85% lower than controls in OA and LC patients, respectively.
These findings suggest that β2AR function itself is disturbed in
patients with chronic inflammatory diseases. These blunted cAMP
responses could be mainly caused by a decrease in receptor density
(downregulation) (47) and/or by
functional uncoupling (desensitization) (48,49).
Some studies suggested that β2AR responsiveness decreases with age
subsequently decreasing β2AR function (50). No significant differences for age
were found between controls and LC patients that could explained
the differences in β2AR responsiveness. However, OA is an
age-related disorder and OA patients in our study were
significantly older than control and LC groups, we could not
discard that differences in β2AR function are due to the advanced
age in OA individuals, so further studies with age matched controls
should be performed.
Previous studies showed that β2AR density and
increase in intracellular cAMP levels in response to stimulation
were decreased on PBMC in patients with chronic joint diseases
(51,52). Wahle et al (53) showed a reduction of β2AR densities
on B lymphocytes mirrored by an impaired intracellular cAMP
generation in patients with chronic rheumatic diseases (RA,
systemic lupus erythematosus, and systemic sclerosis) and chronic
muscle pain disorders such as fibromyalgia and regional myofascial
pain (48,54,55).
It is not clear whether this phenomenon occurs in response to the
inflammatory process or precedes exacerbations of chronic rheumatic
diseases. According to this, in our study, receptor levels were
decreased above 41% for OA and 85% for LC compared to healthy
standard, in a similar way that percentage of receptor agonism
stimulus reduction.
Agonist binding to the β2AR causes the receptor to
interact with and activate G-protein, which in turns activates AC.
AC catalyzes the conversion of adenosine triphosphate (ATP) to cAMP
activating dependent protein kinase. This results in
phosphorylation of particular proteins and specific actions that
depend on the cells and tissue (56). Then continuous stimulation of β2AR
on PBMC, by elevated circulating catecholamine, may trigger a
sympathetic adaptive mechanism.
Animal studies indicated that prior elevation of
adrenaline and repeated stress down-regulate sympathetic responses
to new stress, whereas prior exposure to β2AR agonist and intensive
exercise reduce beta-adrenergic sensitivity (57,58).
Norepinephrine is released locally from sympathetic nerve terminals
in synapse like junctions with immune cells and could exert down
regulatory autocrine effects counteracting the chronicity of the
disease in the inflamed joint synovium (59), determining for example, the disease
onset, progression, and severity in RA and and OA (1,11–13).
In the chronic phase of RA, the SNS has a strong anti-inflammatory
role, reducing both bone destruction and inflammation in RA
(60). Very similar effects were
described in two models of chronic inflammatory bowel disease as
Cohn's disease and diverticulitis (61).
Our data shows that patients with cirrhosis, varices
and clinical decompensation had a reduced β2AR signalling in PBMC,
suggesting the existence of changes of this cellular signalling
pathway associated to the progression of this pathology. New
studies with higher sample size are needed to clarify if this
phenomenon could be considered as a molecular biomarker.
In our study, impairment of β2AR occurs in an
independent way of the genetic profile. β2AR decreased
functionality is not correlated to the presence of any SNP
analyzed. A number of polymorphisms of the β2AR have been described
that appear to alter the behaviour of the receptor following
agonist exposure. These include Arg16Gly, Glu27Gln, and Thr164lle.
Our sample has an Arg16 and Glu27 similar frequency to those
showed in different Caucasian populations (Arg16
(0,38–0,46), Glu27 (0,35–0,46) and Ile164
(0,02–0,04)) (62,63).
Presence of Glu27 (allele G) is associated
with a decreased agonist-promoter down-regulation, less receptor
desensitization being more sensitive to endogenous catecholamine
and showing a greater susceptibility to stress-induced augmentation
of visceral and somatic sensory function. On the contrary
Gly16 (allele G) showed an increased receptor
desensitization and Ile164 (allele T) a decreased affinity
agonist binding (64,65). In this way, previous results have
shown that SNPs at Arg16+-Glu27+ can
modulated disease activity in RA, asthma and myasthenia gravis
(38,66,67).
In our sample, severity of disease was not associated with any
particular genotype. Subjects (OA and controls) with sustained
ability to cAMP reacted to isoproterenol stimulus evidencing the
highest cAMP blockade for the Gln27. Other studies in asthma had
shown that Glu27 avoid downregulation and thus, it was associated
with less reactive airways (68).
The Gly16 receptor variant downregulates to a
greater extent and is associated with increased airway
hyperactivity and greater susceptibility to stress-induced
augmentation of visceral and somatic sensory function, compared
with those homozygous for Arg16 (39). The receptors homozygous for Ile164
had markedly decreased ligand binding and coupling properties
compared with those homozygous for Thr164. However, an individual
can be homozygous or heterozygous for given polymorphisms, and
large populations will have to be analysed to determine their
importance on clinical phenotypes (69).
Although the amount of adrenergic receptor on
lymphocytes has been shown to be related to the number of
adrenergic receptors on heart tissue (70), future studies should employ a more
direct assessment on liver and joint. A definitive evaluation of
the relationship between the effects of β2AR polymorphism and
functionality requires large prospective multicenter trials to
enable simultaneous consideration of single and multiple
genotypes.
In conclusion, decreased β2AR functionality in
patients with OA and LC was independent of patient's β2AR
genotype.
Acknowledgements
We would like to thank to Paula Giménez Martínez
from the CIBERehd for her technical support with the EIA and cell
culture and Bioiberica (Barcelona) for the financial support to
develop this project.
References
|
1
|
Baerwald CG, Burmester GR and Krause A:
Interactions of autonomic nervous, neuroendocrine, and immune
systems in rheumatoid arthritis. Rheum Dis Clin North Am.
26:841–857. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bergquist J, Tarkowski A, Ekman R and
Ewing A: Discovery of endogenous catecholamines in lymphocytes and
evidence for catecholamine regulation of lymphocyte function via an
autocrine loop. Proc Natl Acad Sci USA. 91:12912–12916. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lorton D, Lubahn C and Bellinger DL:
Potential use of drugs that target neural-immune pathways in the
treatment of rheumatoid arthritis and other autoimmune diseases.
Curr Drug Targets Inflamm Allergy. 2:1–30. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Felsner P, Hofer D, Rinner I, Mangge H,
Gruber M, Korsatko W and Schauenstein K: Continuous in vivo
treatment with catecholamines suppresses in vitro reactivity of rat
peripheral blood T-lymphocytes via alpha-mediated mechanisms. J
Neuroimmunol. 37:47–57. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Elenkov IJ, Papanicolaou DA, Wilder RL and
Chrousos GP: Modulatory effects of glucocorticoids and
catecholamines on human interleukin-12 and interleukin-10
production: Clinical implications. Proc Assoc Am Physicians.
108:374–381. 1996.PubMed/NCBI
|
|
6
|
Panina-Bordignon P, Mazzeo D, Lucia PD,
D'Ambrosio D, Lang R, Fabbri L, Self C and Sinigaglia F:
Beta2-agonists prevent Th1 development by selective inhibition of
interleukin 12. J Clin Invest. 100:1513–1519. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hernández FT, Zapater P, De-Madaria E,
Palazón JM, Pascual S, Irurzun J, Such J, Perez-Mateo M and Horga
JF: Functional status of beta-2-adrenoceptor in isolated membranes
of mature erythrocytes from patients with cirrhosis and oesophageal
varices. Vascul Pharmacol. 44:464–468. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brodde OE, Zerkowski HR, Doetsch N,
Motomura S, Khamssi M and Michel MC: Myocardial beta-adrenoceptor
changes in heart failure: Concomitant reduction in beta 1- and beta
2-adrenoceptor function related to the degree of heart failure in
patients with mitral valve disease. J Am Coll Cardiol. 14:323–331.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yu XY, Lin SG, Wang XM, Liu Y, Zhang B,
Lin QX, Yang M and Zhou SF: Evidence for coexistence of three
beta-adrenoceptor subtypes in human peripheral lymphocytes. Clin
Pharmacol Ther. 81:654–658. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xu B, Yi Q, Pirskanen R, Matell G, Eng H
and Lefvert AK: Decreased beta2-adrenergic receptor density on
peripheral blood mononuclear cells in myasthenia gravis. J
Autoimmun. 10:401–406. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Levine JD, Goetzl EJ and Basbaum AI:
Contribution of the nervous system to the pathophysiology of
rheumatoid arthritis and other polyarthritides. Rheum Dis Clin
North Am. 13:369–383. 1987.PubMed/NCBI
|
|
12
|
Härle P, Möbius D, Carr DJ, Schölmerich J
and Straub RH: An opposing time-dependent immune-modulating effect
of the sympathetic nervous system conferred by altering the
cytokine profile in the local lymph nodes and spleen of mice with
type II collagen-induced arthritis. Arthritis Rheum. 52:1305–1313.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Härle P, Pongratz G, Albrecht J, Tarner IH
and Straub RH: An early sympathetic nervous system influence
exacerbates collagen-induced arthritis via CD4+CD25+ cells.
Arthritis Rheum. 58:2347–2355. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Malfait AM, Malik AS, Marinova-Mutafchieva
L, Butler DM, Maini RN and Feldmann M: The beta2-adrenergic agonist
salbutamol is a potent suppressor of established collagen-induced
arthritis: Mechanisms of action. J Immunol. 162:6278–6283.
1999.PubMed/NCBI
|
|
15
|
Lorton D, Bellinger DL, Schaller JA,
Shewmaker E, Osredkar T and Lubahn C: Altered sympathetic-to-immune
cell signaling via β2-adrenergic receptors in adjuvant
arthritis. Clin Dev Immunol. 2013:7643952013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Neuhuber WL and Tiegs G: Innervation of
immune cells: Evidence for neuroimmunomodulation in the liver. Anat
Rec A Discov Mol Cell Evol Biol. 280:884–892. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tiegs G, Bang R and Neuhuber WL:
Requirement of peptidergic sensory innervation for disease activity
in murine models of immune hepatitis and protection by
beta-adrenergic stimulation. J Neuroimmunol. 96:131–143. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Grässel SG: The role of peripheral nerve
fibers and their neurotransmitters in cartilage and bone physiology
and pathophysiology. Arthritis Res Ther. 16:4852014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eitner A, Pester J, Nietzsche S, Hofmann
GO and Schaible HG: The innervation of synovium of human
osteoarthritic joints in comparison with normal rat and sheep
synovium. Osteoarthritis Cartilage. 21:1383–1391. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Najafipour H and Niazmand S: Alteration in
alpha- and beta- adrenoceptor profile of rabbit-knee-joint blood
vessels due to chronic inflammation. Pflugers Arch. 453:23–32.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Beckmann J, Knödl M, Bauser E, Tingart M,
Grifka J and Straub RH: Loss of sympathetic nerve fibers in vital
intertrochanteric bone cylinders lateral to osteonecrosis of the
femoral head. Joint Bone Spine. 80:188–194. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fernandes JC, Martel-Pelletier J and
Pelletier JP: The role of cytokines in osteoarthritis
pathophysiology. Biorheology. 39:237–246. 2002.PubMed/NCBI
|
|
23
|
Malemud CJ: Anticytokine therapy for
osteoarthritis: Evidence to date. Drugs Aging. 27:95–115. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
D'Amico G and Luca A: Natural history.
Clinical-haemodynamic correlations. Prediction of the risk of
bleeding. Baillieres Clin Gastroenterol. 11:243–256. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sanders VM: The beta2-adrenergic receptor
on T and B lymphocytes: Do we understand it yet? Brain Behav Immun.
26:195–200. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Biecker E: Portal hypertension and
gastrointestinal bleeding: Diagnosis, prevention and management.
World J Gastroenterol. 19:5035–5050. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pateron D, Tazi KA, Sogni P, Heller J,
Chagneau C, Poirel O, Philippe M, Moreau R and Lebrec D: Role of
aortic nitric oxide synthase 3 (eNOS) in the systemic vasodilation
of portal hypertension. Gastroenterology. 119:196–200. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Tazi KA, Barrière E, Moreau R, Heller J,
Sogni P, Pateron D, Poirel O and Lebrec D: Role of shear stress in
aortic eNOS up-regulation in rats with biliary cirrhosis.
Gastroenterology. 122:1869–1877. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Karadsheh Z and Allison H: Primary
prevention of variceal bleeding: Pharmacological therapy versus
endoscopic banding. N Am J Med Sci. 5:573–579. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lemaitre RN, Heckbert SR, Sotoodehnia N,
Bis JC, Smith NL, Marciante KD, Hindorff LA, Lange LA, Lumley TS,
Rice KM, et al: beta1- and beta2-adrenergic receptor gene
variation, beta-blocker use and risk of myocardial infarction and
stroke. Am J Hypertens. 21:290–296. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Heckbert SR, Hindorff LA, Edwards KL,
Psaty BM, Lumley T, Siscovick DS, Tang Z, Durda JP, Kronmal RA and
Tracy RP: Beta2-adrenergic receptor polymorphisms and risk of
incident cardiovascular events in the elderly. Circulation.
107:2021–2024. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sotoodehnia N, Siscovick DS, Vatta M,
Psaty BM, Tracy RP, Towbin JA, Lemaitre RN, Rea TD, Durda JP, Chang
JM, et al: Beta2-adrenergic receptor genetic variants and risk of
sudden cardiac death. Circulation. 113:1842–1848. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Stanzione R, Di Angelantonio E,
Evangelista A, Barbato D, Marchitti S, Zanda B, Pirisi A, Quarta G,
Volpe M and Rubattu S: Beta2-adrenergic receptor gene polymorphisms
and risk of ischemic stroke. Am J Hypertens. 20:657–662. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lanfear DE, Jones PG, Marsh S, Cresci S,
McLeod HL and Spertus JA: Beta2-adrenergic receptor genotype and
survival among patients receiving beta-blocker therapy after an
acute coronary syndrome. JAMA. 294:1526–1533. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tan S, Hall IP, Dewar J, Dow E and
Lipworth B: Association between beta 2-adrenoceptor polymorphism
and susceptibility to bronchodilator desensitisation in moderately
severe stable asthmatics. Lancet. 350:995–999. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Gianfagna F, Cugino D, Ahrens W, Bailey
ME, Bammann K, Herrmann D, Koni AC, Kourides Y, Marild S, Molnár D,
et al: Understanding the links among neuromedin U gene,
beta2-adrenoceptor gene and bone health: An observational study in
European children. PLoS One. 8:e706322013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Malysheva O, Pierer M, Wagner U, Wahle M,
Wagner U and Baerwald CG: Association between beta2 adrenergic
receptor polymorphisms and rheumatoid arthritis in conjunction with
human leukocyte antigen (HLA)-DRB1 shared epitope. Ann Rheum Dis.
67:1759–1764. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Xu B, Arlehag L, Rantapää-Dahlquist SB and
Lefvert AK: Beta2-adrenergic receptor gene single-nucleotide
polymorphisms are associated with rheumatoid arthritis in northern
Sweden. Scand J Rheumatol. 33:395–398. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Kushnir VM, Cassell B, Gyawali CP,
Newberry RD, Kibe P, Nix BD, Sabzpoushan A, Kanuri ND and Sayuk GS:
Genetic variation in the beta-2 adrenergic receptor (ADRB2)
predicts functional gastrointestinal diagnoses and poorer
health-related quality of life. Aliment Pharmacol Ther. 38:313–323.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kellgren JH and Lawrence JS: Radiological
assessment of osteo-arthrosis. Ann Rheum Dis. 16:494–502. 1957.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Bosch J, Abraldes JG, Albillos A, Aracil
C, Bañares R, Berzigotti A, Calleja JL, de la Peña J, Escorsell A,
García-Pagán JC, et al: Portal hypertension: Recommendations for
evaluation and treatment: Consensus document sponsored by the
Spanish association for the study of the liver (AEEH) and the
biomedical research network center for liver and digestive diseases
(CIBERehd). Gastroenterol Hepatol. 35:421–450. 2012.(In Spanish).
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sondergaard SB, Knudsen JH and Christensen
NJ: Regulation of cAMP in a lymphocyte preparation isolated from
peripheral venous blood in human subjects: The significance of
residual thrombocytes, noradrenaline and prostaglandins. Clin Sci
(Lond). 95:377–383. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Drysdale CM, McGraw DW, Stack CB, Stephens
JC, Judson RS, Nandabalan K, Arnold K, Ruano G and Liggett SB:
Complex promoter and coding region beta 2-adrenergic receptor
haplotypes alter receptor expression and predict in vivo
responsiveness. Proc Natl Acad Sci USA. 97:10483–10488. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Belfer I, Buzas B, Hipp H, Phillips G,
Taubman J, Lorincz I, Evans C, Lipsky RH, Enoch MA, Max MB and
Goldman D: Haplotype-based analysis of alpha 2A, 2B, and 2C
adrenergic receptor genes captures information on common functional
loci at each gene. J Hum Genet. 50:12–20. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Campello L, Esteve-Rudd J, Bru-Martinez R,
Herrero MT, Fernández-Villalba E, Cuenca N and Martín-Nieto J:
Alterations in energy metabolism, neuroprotection and visual signal
transduction in the retina of Parkinsonian, MPTP-treated monkeys.
PLoS One. 8:e744392013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Garcia-Tsao G, Sanyal AJ, Grace ND and
Carey W: Practice Guidelines Committee of the American Association
for the Study of Liver Diseases; Practice Parameters Committee of
the American College of Gastroenterology: Prevention and management
of gastroesophageal varices and variceal hemorrhage in cirrhosis.
Hepatology. 46:922–938. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Jeanningros R, Mazzola P, Azorin JM,
Samuelian-Massa C and Tissot R: Beta-adrenoceptor density of intact
mononuclear leukocytes in subgroups of depressive disorders. Biol
Psychiatry. 29:789–798. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Maekawa K, Twe C, Lotaif A, Chiappelli F
and Clark GT: Function of beta-adrenergic receptors on mononuclear
cells in female patients with fibromyalgia. J Rheumatol.
30:364–368. 2003.PubMed/NCBI
|
|
49
|
Leineweber K, Rohe P, Beilfuss A, Wolf C,
Sporkmann H, Bruck H, Jakob HG, Heusch G, Philipp T and Brodde OE:
G-protein-coupled receptor kinase activity in human heart failure:
Effects of beta-adrenoceptor blockade. Cardiovasc Res. 66:512–519.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Scarpace PJ, Tumer N and Mader SL:
Beta-adrenergic function in aging. Basic mechanisms and clinical
implications. Drugs Aging. 1:116–129. 1991.PubMed/NCBI
|
|
51
|
Krause A, Henrich A, Beckh KH, Von Wichert
P and Baerwald C: Correlation between density of beta 2-adrenergic
receptors on peripheral blood mononuclear cells and serum levels of
soluble interleukin-2 receptors in patients with chronic
inflammatory diseases. Eur J Clin Invest. 22 Suppl 1:S47–S51.
1992.
|
|
52
|
Baerwald C, Graefe C, Muhl C, Von Wichert
P and Krause A: Beta 2-adrenergic receptors on peripheral blood
mononuclear cells in patients with rheumatic diseases. Eur J Clin
Invest. 22 Suppl 1:S42–S46. 1992.
|
|
53
|
Wahle M, Kölker S, Krause A, Burmester GR
and Baerwald CG: Impaired catecholaminergic signalling of B
lymphocytes in patients with chronic rheumatic diseases. Ann Rheum
Dis. 60:505–510. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Maekawa K, Kuboki T, Inoue E,
Inoue-Minakuchi M, Suzuki K, Yatani H and Clark GT: Function of
beta 2-adrenergic receptors in chronic localized myalgia. J Orofac
Pain. 17:140–144. 2003.PubMed/NCBI
|
|
55
|
Maekawa K, Clark GT and Kuboki T:
Intramuscular hypoperfusion, adrenergic receptors, and chronic
muscle pain. J Pain. 3:251–260. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Lefkowitz RJ, Caron MG and Stiles GL:
Mechanisms of membrane-receptor regulation. Biochemical,
physiological, and clinical insights derived from studies of the
adrenergic receptors. N Engl J Med. 310:1570–1579. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
de Galan BE, Rietjens SJ, Tack CJ, van der
Werf SP, Sweep CG, Lenders JW and Smits P: Antecedent adrenaline
attenuates the responsiveness to but not the release of
counterregulatory hormones during subsequent hypoglycemia. J Clin
Endocrinol Metab. 88:5462–5467. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Baerwald CG, Laufenberg M, Specht T, von
Wichert P, Burmester GR and Krause A: Impaired sympathetic
influence on the immune response in patients with rheumatoid
arthritis due to lymphocyte subset-specific modulation of beta
2-adrenergic receptors. Br J Rheumatol. 36:1262–1269. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Ader R, Cohen N and Felten D:
Psychoneuroimmunology: Interactions between the nervous system and
the immune system. Lancet. 345:99–103. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Capellino S, Cosentino M, Wolff C, Schmidt
M, Grifka J and Straub RH: Catecholamine-producing cells in the
synovial tissue during arthritis: Modulation of sympathetic
neurotransmitters as new therapeutic target. Ann Rheum Dis.
69:1853–1860. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Straub RH, Grum F, Strauch U, Capellino S,
Bataille F, Bleich A, Falk W, Schölmerich J and Obermeier F:
Anti-inflammatory role of sympathetic nerves in chronic intestinal
inflammation. Gut. 57:911–921. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Brodde OE, Bruck H and Leineweber K:
Cardiac adrenoceptors: Physiological and pathophysiological
relevance. J Pharmacol Sci. 100:323–337. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Kirstein SL and Insel PA: Autonomic
nervous system pharmacogenomics: A progress report. Pharmacol Rev.
56:31–52. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Diatchenko L, Anderson AD, Slade GD,
Fillingim RB, Shabalina SA, Higgins TJ, Sama S, Belfer I, Goldman
D, Max MB, et al: Three major haplotypes of the beta2 adrenergic
receptor define psychological profile, blood pressure, and the risk
for development of a common musculoskeletal pain disorder. Am J Med
Genet B Neuropsychiatr Genet. 141B:449–462. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Small KM, McGraw DW and Liggett SB:
Pharmacology and physiology of human adrenergic receptor
polymorphisms. Annu Rev Pharmacol Toxicol. 43:381–411. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Zuurhout MJ, Vijverberg SJ, Raaijmakers
JA, Koenderman L, Postma DS, Koppelman GH and Maitland-van der Zee
AH: Arg16 ADRB2 genotype increases the risk of asthma exacerbation
in children with a reported use of long-acting β2-agonists: Results
of the PACMAN cohort. Pharmacogenomics. 14:1965–1971. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Bengtsson K, Orho-Melander M, Melander O,
Lindblad U, Ranstam J, Råstam L and Groop L: Beta(2)-adrenergic
receptor gene variation and hypertension in subjects with type 2
diabetes. Hypertension. 37:1303–1308. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Martinez FD, Graves PE, Baldini M, Solomon
S and Erickson R: Association between genetic polymorphisms of the
beta2-adrenoceptor and response to albuterol in children with and
without a history of wheezing. J Clin Invest. 100:3184–3188. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Gjesing AP, Andersen G, Burgdorf KS,
Borch-Johnsen K, Jørgensen T, Hansen T and Pedersen O: Studies of
the associations between functional beta2-adrenergic receptor
variants and obesity, hypertension and type 2 diabetes in 7,808
white subjects. Diabetologia. 50:563–568. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Qing F, Rahman SU, Hayes MJ, Rhodes CG,
Ind PW, Jones T and Hughes JM: Effect of long-term beta2-agonist
dosing on human cardiac beta-adrenoceptor expression in vivo:
Comparison with changes in lung and mononuclear leukocyte
beta-receptors. J Nucl Cardiol. 4:532–538. 1997. View Article : Google Scholar : PubMed/NCBI
|