Introduction
Diabetes is a serious global health burden. It is
estimated that the total number of diabetic patients worldwide was
~382 million in 2013, a figure expected to rise to ~592 million by
2035 (1). Diabetic peripheral
neuropathy is a frequent complication of diabetes that 30% of
hospitalized and 20% of community-dwelling patients with diabetes
develop (2). Clinically, peripheral
neuropathy patients often presents with symmetrical pain and
sensory abnormalities, and numbness starting from the distal end of
the lower limb is often the early typical symptom. Painful diabetic
peripheral neuropathy is present in ~20% of patients with type 2
diabetes and 5% of those with type 1 (3). Such patients often feel a prickling
pain, a burning pain, or a drilling and cutting pain, and they may
also present with hyperalgesia. The correct diagnosis of painful
diabetic peripheral neuropathy is made only after other causes,
besides diabetes mellitus, are ruled out (4). The diagnosis depends upon the
corresponding symptoms and signs, the results from nerve conduction
studies, monofilament and tuning fork examination results,
temperature perception and ankle reflex evaluation results
(5–7).
The treatment mainly includes achieving satisfactory blood glucose
control, improving microcirculation, neurotrophic drugs and other
symptomatic treatment to improve symptoms. Patients with type 2
diabetes have an increased risk of developing cancer, and the
association between diabetes and cancer is currently a popular
topic (8). The present study reports
a rare case of lung cancer that presented with paraneoplastic
neurological syndrome (PNS), which mimicked diabetic peripheral
neuropathy.
Case report
In September 2010, a 61-year-old man with diabetes
mellitus, coronary heart disease, hypertension and pulmonary
fibrosis presented at Suzhou People's Hospital (Suzhou, China),
with a sensory disturbance, and the feeling of pins and needles all
over the body. The patient presented with a 1-year history of type
2 diabetes, which was being treated with 500 mg metformin twice a
day and 2.0 mg glibenclamide twice a day for ~9 months. In August
2010, a chest computed tomography scan was performed to test for
pulmonary fibrosis, and no other symptom except for pulmonary
fibrosis was reported. Treatment with tramadol was administered for
diabetic peripheral neuropathy, but the patient's condition did not
improve. Following referral to the pain clinic of Peking Union
Medical College Hospital (Beijing, China), the patient was found to
be negative for antinuclear antibodies. Experimental treatment with
prednisone acetate 10 mg once a day for 4 days was attempted, but
the symptoms progressed, such that the patient experienced
difficulty in sleeping and lost 5 kg in weight. The patient was
therefore admitted to the Chinese People's Liberation Army Navy
General Hospital (Beijing, China) for examination and treatment in
October 2010.
Upon presentation, the patient complained of
full-body pain and numbness, and massage was found to relieve this
pain. The patient scored the pain as 10 out of 10 for severity.
Cardiovascular, respiratory, abdominal and musculoskeletal
examinations were normal. Scattered skin rashes were present on the
patient's back. A neurological examination showed that the muscle
tone was normal, the bilateral tendon reflexes were decreased and
the bilateral Babinski signs were negative. Blood testing revealed
the following: Fasting glucose, 11.7 mmol/l (normal range, 3.9–6.1
mmol/l); glycated hemoglobin (HbA1c), 9.7% (normal range,
3.0–6.3%); serum albumin, 28 g/l (normal range, 34.0–48.0 g/l);
total protein, 58 g/l (normal range, 60.0–83.0 g/l); erythrocyte
sedimentation rate, 52 mm/h (normal range, 0.00–15.0 mm/h); and
C-reactive protein, 16.4 mg/l (normal range, 0.0–8.2 mg/l). The
serum creatine kinase, creatine kinase-MB, full blood count and
renal, hepatic and autoimmune profiles were all normal.
A primary diagnosis of diabetic peripheral
neuropathy was formed and biosynthetic human insulin injection was
administered before three meals by subcutaneous injection, and
isophane protamine biosynthetic human insulin injection was
administered before bed, to treat the hyperglycemia. Thioctic acid
for injection 0.6 g once a day for 7 days and analgesics (200 mg
carbamazepine once a day before bed and 100 mg tramadol twice a day
for 10 days) were used to relieve the diffuse pain. However, there
was no improvement in the symptoms. The patient then reported
dizziness when getting up in the morning, and the recorded arterial
blood pressure dropped 40 mmHg for the systolic blood pressure and
20 mmHg for the diastolic blood pressure when the patient stood up.
Orthostatic hypotension was diagnosed. The results from a motor
nerve electromyography and retinopathy were normal, and the urinary
albumin level was in the normal range. The paradoxical phenomenon
of severe symptoms and a lack of any detectable cause suggested
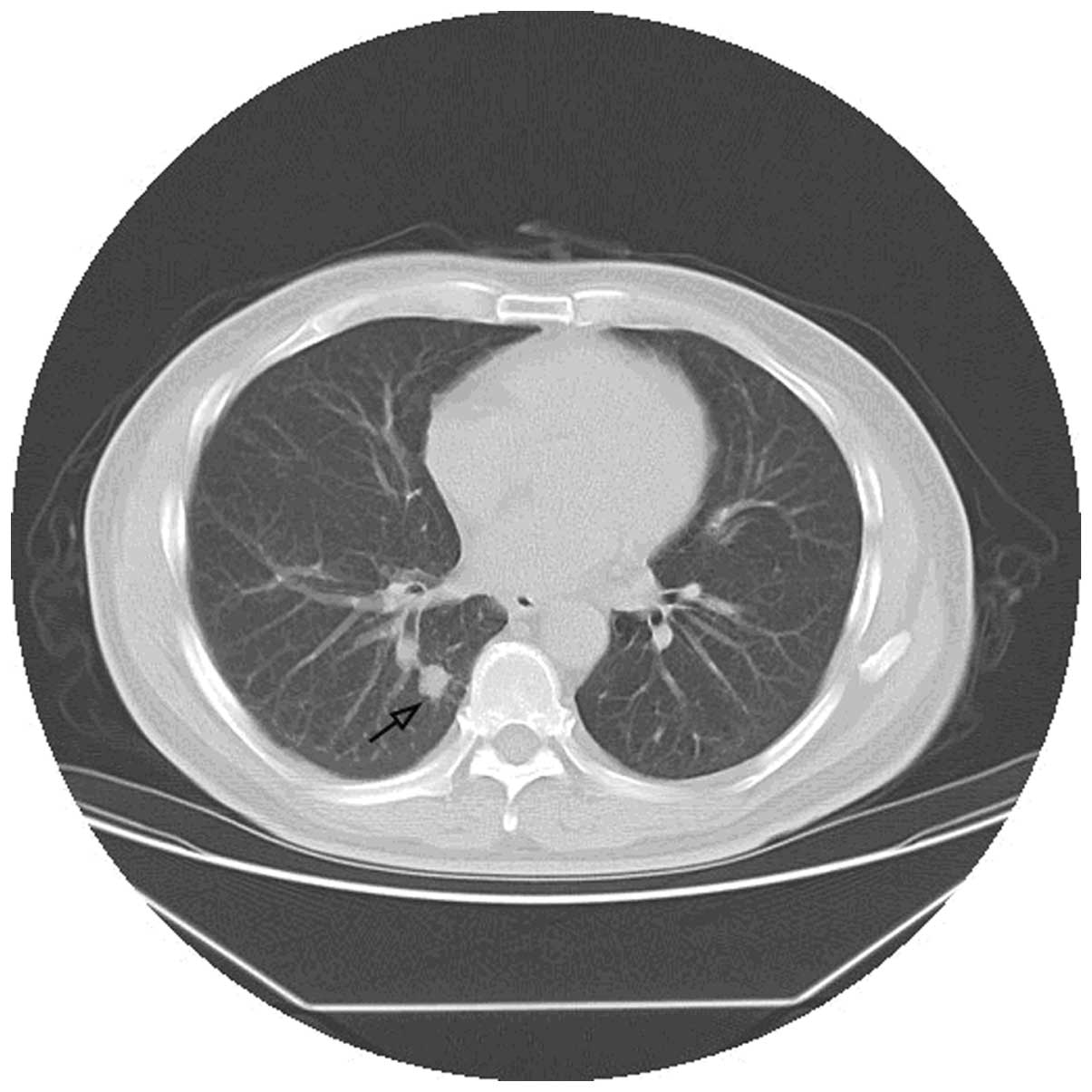
that the pain may not be caused by the diabetes. A computed
tomography scan of the chest subsequently revealed an enlarged node
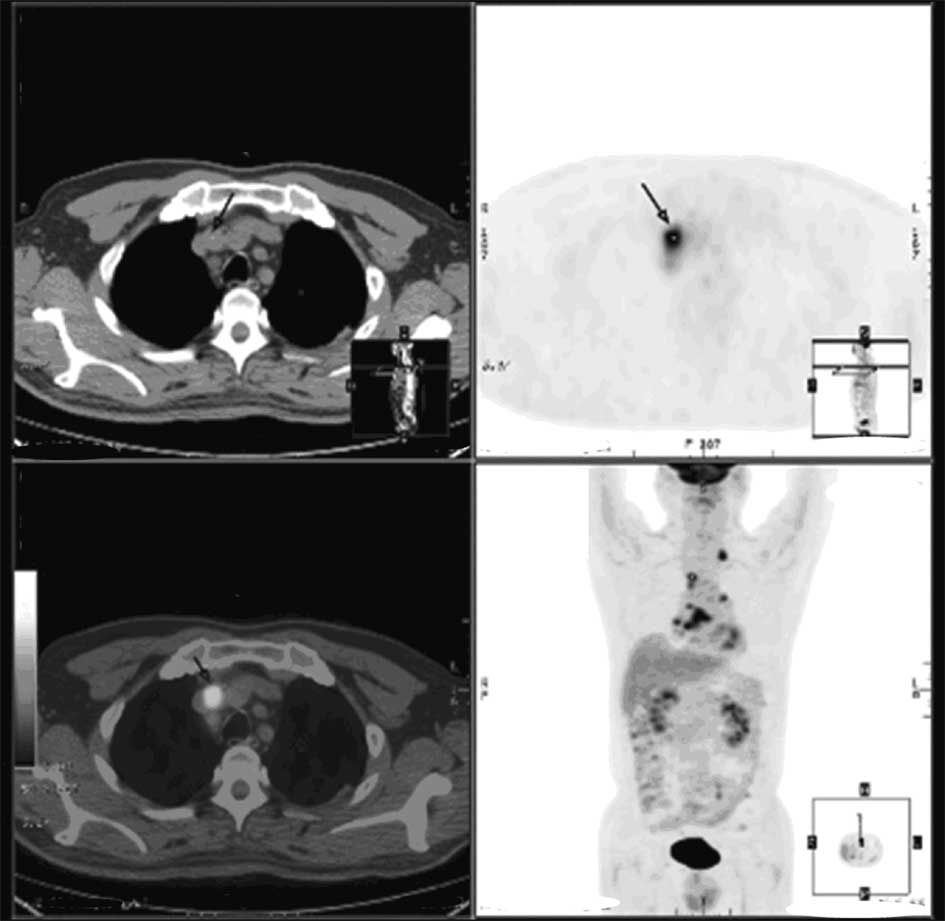
in the lower right lung close to the spine (Fig. 1). On positron emission
tomography-computed tomography, the focus nodes of tumor-specific
uptake were also observed in regions other than the lung (Fig. 2). The tumor-node-metastasis stage of
the lung tumor was T1N3Mx (9). The
patient rejected invasive examinations, such as a lymph node
biopsy. However, based on the aforementioned results, the patient
was diagnosed with sensory neuropathy resulting from PNS.
Following 6 months of chemotherapy and radiotherapy,
the symptoms were gradually reduced, but only carbamazepine could
relieve the patient's pain. In May 2012, the serum albumin, total
protein, erythrocyte sedimentation rate and C-reactive protein
levels returned to normal, however, the pain was still being
relieved with an analgesic.
Discussion
Peripheral polyneuropathy is a frequent complication
of diabetes (10). Approximately 30%
of diabetic patients develop neuropathic pain, which manifests as
spontaneous pain, hyperalgesia and allodynia (11). Several studies have identified other
potential causes of neuropathy in individuals with diabetes
(4). A total of 10–50% of individuals
with diabetes and peripheral neuropathy may have a separate cause
of peripheral neuropathy, including neurotoxic medications, vitamin
B12 deficiency, alcohol abuse, chronic inflammatory demyelinating
neuropathy, renal disease, inherited neuropathy and vasculitis, and
certain patients may even have more than one of these causes
(4). Paraneoplastic neuropathies are
also a potential cause (12).
The patient in the present study did not display the
classical characteristics of diabetic neuropathy, such as
hyperalgesia and allodynia, which was brought on by the light
pressure of wearing socks, stockings or bedclothes, but displayed
unusual symptoms, such as pain that could be relieved by massage.
Additionally, the patient did not display clinical features of
diabetic retinopathy or diabetic kidney disease and therefore, the
diagnosis of diabetic neuropathy was not supported (12). The patient exhibited the
characteristics of classical paraneoplastic sensory neuropathy,
which corresponded to the following criteria (13): Sub-acute development in <12 weeks,
a Rankin severity score of ≥3 (moderate disability), the onset of
numbness with frequent pain and sensory disturbance, affected arms
and legs (the so-called gloves and stockings areas), and a
frequently asymmetrical onset (13).
The diagnosis of paraneoplastic peripheral neuropathies should be
considered in this patient, even though it is a rare
neuroimmunological complication of malignancy. The manifestation of
paraneoplastic sensory neuropathy is restricted to the peripheral
nervous system in 24% of patients. The tumors that are typically
associated with these syndromes are lymphoma, thymoma, and breast,
ovarian and small cell lung carcinoma. The most common autoantibody
marker of paraneoplastic neuropathies is anti-Hu (also known as
type 1 anti-neuronal nuclear antibody).
In the current patient, lung cancer was found 2
months after the characteristics of classical paraneoplastic
sensory neuropathy occurred. The patient's pain was significantly
improved following treatment for lung cancer without concomitant
immunotherapy. PNS was diagnosed based on the diagnostic criteria
established for the disease by an international panel of
neurologists (14,15). However, paraneoplastic antibodies were
not detected in the serum or pathological samples.
This case highlights the importance of forming a
differential diagnosis that considers conditions other than
diabetic complications in diabetic patients who present with
neurological symptoms, particularly in the presence of non-typical
features, such as generalized aching. Diabetes should not be
assumed to be the only cause of painful neuropathy in diabetic
patients.
Acknowledgements
The authors would like to thank Edanz for providing
an English editing service.
References
|
1
|
Guariguata L, Whiting D, Hambleton I,
Beagley J, Linnenkamp U and Shaw J: Global estimates of diabetes
prevalence for 2013 and projections for 2035. Diabetes Res Clin
Pract. 103:137–149. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vinik AI and Casellini CM: Guidelines in
the management of diabetic nerve pain: Clinical utility of
pregabalin. Diabetes Metab Syndr Obes. 6:57–78. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hartemann A, Attal N, Bouhassira D, Dumont
I, Gin H, Jeanne S, Said G and Richard JL: Working Group on the
Diabetic Foot from the French-speaking Society of Diabetology:
Painful diabetic neuropathy: Diagnosis and management. Diabetes
Metab. 37:377–388. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Freeman R: Not all neuropathy in diabetes
is of diabetic etiology: Differential diagnosis of diabetic
neuropathy. Curr Diab Rep. 9:423–431. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hirschfeld G, von Glischinski M,
Blankenburg M and Zernikow B: Screening for peripheral neuropathies
in children with diabetes: A systematic review. Pediatrics.
133:e1324–e1330. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shehab DK, Al-Jarallah KF, Abraham M,
Mojiminiyi OA, Al-Mohamedy H and Abdella NA: Back to basics: Ankle
reflex in the evaluation of peripheral neuropathy in type 2
diabetes mellitus. QJM. 105:315–320. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Feng Y, Schlösser FJ and Sumpio BE: The
Semmes Weinstein monofilament examination as a screening tool for
diabetic peripheral neuropathy. J Vasc Surg. 50:675–682. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang PH, Chen ZW, Lv D, Xu YY, Gu WL,
Zhang XH, Le YL, Zhu HH and Zhu YM: Increased risk of cancer in
patients with type 2 diabetes mellitus: A retrospective cohort
study in China. BMC Public Health. 12:5672012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wohlschläger J, Wittekind C and Theegarten
D: New TNM classification of malignant lung tumours. Pathologe.
31:355–360. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Azulay JP and Pouget J: Diabetic
neuropathies. Rev Prat. 51:1783–1787. 2001.(Article in French).
PubMed/NCBI
|
|
11
|
Wang D, Couture R and Hong Y: Activated
microglia in the spinal cord underlies diabetic neuropathic pain.
Eur J Pharmacol. 728:59–66. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tesfaye S, Vileikyte L, Rayman G, Sindrup
SH, Perkins BA, Baconja M, Vinik AI and Boulton AJ: Toronto Expert
Panel on Diabetic Neuropathy: Painful diabetic peripheral
neuropathy: Consensus recommendations on diagnosis, assessment and
management. Diabetes Metab Res Rev. 27:629–638. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kanaji N, Watanabe N, Kita N, Bandoh S,
Tadokoro A, Ishii T, Dobashi H and Matsunaga T: Paraneoplastic
syndromes associated with lung cancer. World J Clin Oncol.
5:197–223. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Honnorat J and Antoine JC: Paraneoplastic
neurological syndromes. Orphanet J Rare Dis. 2:222007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Graus F, Delattre JY, Antoine JC, Dalmau
J, Giometto B, Grisold W, Honnorat J, Smitt PS, Vedeler Ch,
Verschuuren JJ, et al: Recommended diagnostic criteria for
paraneoplastic neurological syndromes. J Neurol Neurosurg
Psychiatry. 75:1135–1140. 2004. View Article : Google Scholar : PubMed/NCBI
|