Introduction
Adenocarcinomas of the esophagogastric junction
(AEGJ) are of particular interest nowadays, as numerous studies
from a range of industrialized Western countries have reported an
increased incidence of adenocarcinomas of the esophagus and the
cardia over the last 30 years, which is in contrast to the
decreasing incidence of gastric cancer (1). These tumors are sub-classified based on
the anatomical-topographical location of the tumor center according
to the Siewert classification (2).
AEGJ are currently staged according to the 7th edition of the Union
for International Cancer Control/American Joint Committee on Cancer
Tumor-Node-Metastasis (TNM) classification system (3). The overall survival (OS) rate has been
reported to be 15–20% and the 5-year survival rates are ~40%
following a complete (R0) resection (4,5).
Exocrine tumors are the most common type of
pancreatic cancer, the majority presenting with the histological
characteristics of adenocarcinoma, resembling the pancreatic ductal
cell (6). Among all cancer-related
mortalities in the United States, malignant tumors of the pancreas
rank fourth (7) and the overall
(global) mortality rate is 98% (8).
As a number of patients already present with advanced disease or
even metastasis at the time of diagnosis, only 10–20% of the
patients are eligible for surgical resection. These patients have a
5-year survival rate of 10–24% for cases with R0 resection
(9,10). This poor prognosis reflects the
particularly aggressive and lethal nature of this type of cancer.
Recurrence rates of almost 80% after have also been observed
following R0 resections (10).
Over the past decade, the detection of circulating
tumor cells (CTCs) in the peripheral blood of cancer patients has
gained more and more attention. An increasing number of trials have
suggested that those patients who tested positive for CTCs
experienced shorter survival times than those who tested negative
for CTCs. For example, primary breast cancer patients who tested
‘positive’ for CTCs (i.e., ≥5 CTCs/7.5 ml of blood) had a shorter
progression-free survival (PFS) time (2.7 vs. 7.0 months) and a
shorter OS time (10.1 vs. >18 months) compared with those who
tested ‘negative’ (i.e., <5 CTC/7.5 ml of blood) (11,12).
The CellSearch® system is a validated and
widely accepted device for the detection of CTCs in human
peripheral blood (13), which has
already gained approval by the American Food and Drug
Administration (FDA) for the detection of CTCs and as a prognostic
tool to predict PFS and OS in patients with metastatic disease
originating from the prostate, breasts and colon (14).
However, limited data regarding the feasibility of
detection of CTCs in patients with pancreatic or esophagogastric
adenocarcinoma is available. Therefore, the aim of the present
small study was to determine the feasibility and frequency of the
detection of CTCs by applying the CellSearch® system in
these two tumor entities, with the primary endpoint being the
detection of CTCs (yes or no). We hypothesized that
CellSearch® would be able to detect CTCs in the blood of
patients from the two disease groups regardless of the stage of the
disease.
Patients and methods
Study population
Following approval by the local ethics committee
(Kantonale Ethikkommission Zurich, Zurich, Switzerland), 16
consecutive patients (>18 years old) with either AEGJ or
pancreatic cancer (8 patients each) at various disease stages and
undergoing various treatments were included in the study. Patients
were only excluded in instances of any ethical contraindications or
the inability of the patient to understand the language of the
center where the study was performed (i.e., German). Written
informed consent was obtained from all patients.
Detection of CTCs using the CellSearch
system
In total, 7.5 ml of blood was drawn from each
patient into CellSave Preservative tubes (Janssen Diagnostics,
Raritan, NJ, USA). Blood collection from pancreatic cancer patients
was conducted during an office visit. For esophagogastric cancer
patients, two different time points were established to collect the
blood samples: i) Prior to chemotherapy or surgery (if eligible;
t0); and ii) 60 min after the surgical en bloc resection of the
tumor (if eligible; t1). Details about the timing of blood
collection for each patient are provided in Table I.
 | Table I.Characteristics of all 8 patients with
esophagogastric adenocarcinoma. |
Table I.
Characteristics of all 8 patients with
esophagogastric adenocarcinoma.
| Case no. | Age/gender | Siewert type | Time point | No. of CTCs | TNM stage (34) | Metastasis | Prior
chemotherapy | Prior radiation | Prior surgery | Relevant medical
history (ref) |
|---|
| 1 | 41/M | I | t0 | 0 | ypT3 ypN1 M0 | None | None | None | None | None |
| 2 | 69/M | II | t1 | 0 | cT4 cN1 cM0 | None | 4 cycles of FLOT | None | Diagnostic
laparoscopy | COPD GOLD III
(35) |
| 3 | 52/F | I | t1 | 0 | cT3 cN+ cM1 | Deep cervical lymph
nodes | 5 cycles of
carboplatin/paclitaxel | 42 Gy | None | Diffuse large cell
lymphoma (stage IIIb), arterial HTN |
| 4 | 62/M | III | t1 | 0 | ypT3 ypN3 ycM0 | None | 4 cycles of
FLOT | None | Diagnostic
laparoscopy | Endocarditis of the
aortic valve, CAD/NSTEMI |
| 5 | 72/F | I | t0 | 3 | uT2 uN0 cM1 | Bone
(singular) | None | None | None | Stroke |
| 6 | 82/M | I | t0+t1 | 0 | cT3 cN1 cM0 | None | None | None | None | Aortic
regurgitation |
| 7 | 76/F | I | t0+t1 | 0 | cT3 N1 M0 | None | None | None | None | Bladder carcinoma,
hypertensive CM |
| 8 | 65/M | I | t0+t1 | 0 | cT2 N+ M0 | None | 4 weekly doses of
cisplatin/docetaxel | 45 Gy | Diagnostic
laparoscopy | OSA, arterial HTN;
hypothyroidism, TIA |
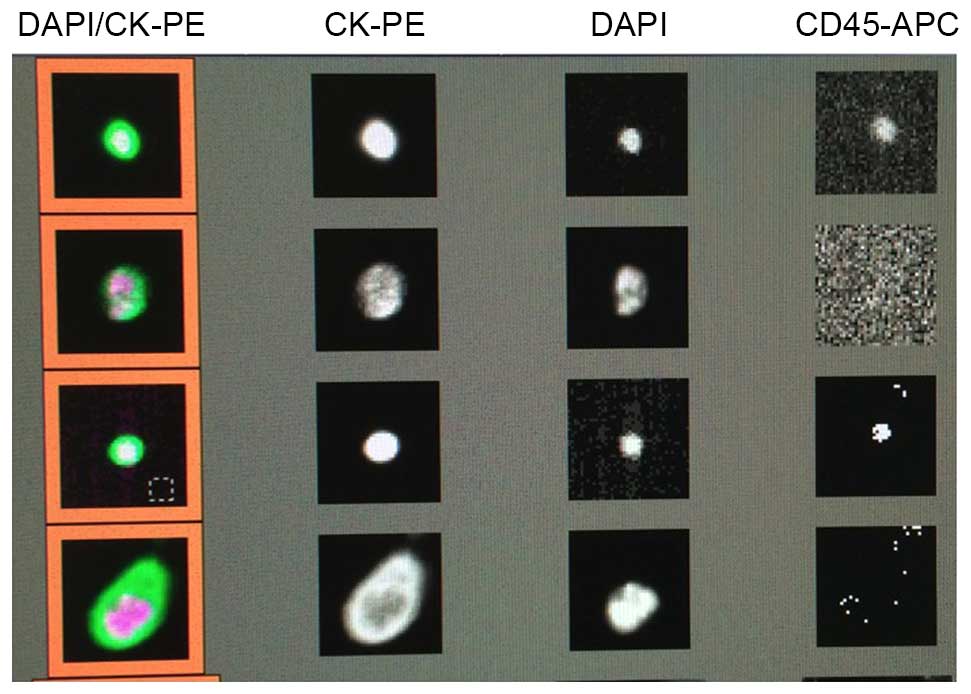
CTC analysis was conducted in accordance with the
manufacturer's instructions (Janssen Diagnostics). Briefly, the
cells were initially centrifuged at room temperature at 800 × g for
10 min. Subsequently, further processing of the blood cells was
performed with the automated CellTracks®
Autoprep® System (Janssen Diagnostics), which uses
ferrofluid nanoparticles coated with an antibody against epithelial
cell adhesion molecule (EpCAM) for the enrichment of CTC, as well
as fluorescent staining against cytokeratin and the cell surface
marker cluster of differentiation 45 (CD45). Cell nuclei were
stained using 4′,6-diamidino-2-phenylindole. Finally, cells
captured in the MagNest cassette were analyzed with CellTracks
Analyzer II®. Nucleated cells, which stained positive
for cytokeratin and negative for CD45 (Fig. 1) were counted as CTCs by two specially
trained individuals.
Results
Patient characteristics
A total of 8 patients (3 females and 5 males), with
locally-advanced (cT2-4, N any, M any) AEGJ and a median age of 67
years (range, 41–82 years) were included in the study (Table I). Loco-regional lymph nodes (cN+)
were detected in 7 out of 8 (87.5%) patients and distant metastases
(lymph node or bone) were present in 2 out of 8 patients (25.0%)
(Table I). Additionally, 4 out of 8
(50.0%) patients received chemotherapy prior to the blood
collection for CTC detection. Of these, 2 patients received 4
cycles of a 5-fluorouracil, leucovorin, oxaliplatin and docetaxel
regimen, 1 patient underwent pre-treatment with 5 cycles of
carboplatin and paclitaxel, and 1 patient received 4 weekly doses
of a cisplatin and docetaxel-based regimen. Of the 8 patients, 2
(25.0%) were subjected to concurrent pre-operative local
radiotherapy (42–45 Gy), and 3 (37.5%) had undergone a diagnostic
laparoscopy during the staging process (Table I).
The characteristics of the patients with pancreatic
adenocarcinoma are summarized in Table
II. For this group, 8 consecutive patients (2 females and 6
males) at different disease stages were enrolled in the study. The
patients had a median age of 60 years at the time of study entry
(range, 35–73 years). In total, 6 out of 8 (75.0%) patients
presented with loco-regional lymph node metastases and 4 out of 8
(50.0%) patients exhibited distant metastases, as specified in
Table II. With regard to treatment,
5 out of 8 patients (62.5%) received chemotherapy prior to CTC
detection. The majority of patients received the folinic acid,
5-fluorouracil, irinotecan and oxaliplatin (FOLFIRINOX) regimen; in
4 patients, a median of 8 cycles (range, 1–13 cycles) were used,
representing the standard of care for metastatic pancreatic
adenocarcinoma. Prior to FOLFIRINOX, 2 patients had received 6
cycles of gemcitabine (weekly), whereas 1 patient had undergone 5
cycles of gemcitabine + chloroquine (within a phase II clinical
trial) only. Radiation therapy was administered to 3 (37.5%)
patients prior to the CTC measurement (median, 30 Gy; range, 20–50
Gy). Surgical interventions had been conducted in 5 out of 8
patients (62.5%), with the majority of those being strictly
palliative (Table II).
| Table II.Characteristics of all 8 patients
with pancreatic adenocarcinoma included in the study. |
Table II.
Characteristics of all 8 patients
with pancreatic adenocarcinoma included in the study.
| Case no. | Age/gender | No. of CTCs | TNMa | Metastasis | Prior
chemotherapy | Prior
radiation | Prior surgery | Relevant medical
history (ref) | Comments |
|---|
| 1 | 73/M | 1 | cT4 cN1 M1 | Peritoneum | None | None | None | Dilatative CM,
arterial HTN, DM type 2 |
|
| 2 | 35/M | 25 | cT4 cN1 cM0 | None | 12 cycles of
FOLFIRINOX | None | Nanoknife | None |
|
| 3 | 47/M | 42 | cT2 cN0 cM0 | None | 6 cycles of
gemcitabine (weekly), 4 cycles of FOLFIRINOX | 50 Gy | Gastric bypass
(palliative) | Arterial HTN |
|
| 4 | 64/M | 2 | pT3 pN1 M0 | None | 1 cycle of
FOLFIRINOX | None | None | Arterial HTN,
hypertensive CM, DVT |
|
| 5 | 70/F | 2 | cT4 cNx cM0 | None | 5 cycles of
gemcitabine + chloroquine | None | Y-Roux anastomosis,
hepatico-jejunostomy, gastro-enterostomy | Cachexia,
hyperthyreosis, malignant melanoma |
|
| 6 | 66/M | 83 | cT4 cN+ M1 | Bone, lung, liver,
brain | None | 20 Gy | None | DM type 2, PAOD,
COPD GOLD II (35) | Succumbed 4 days
after CTC analysis |
| 7 | 56/M | 0 | cT4 cN1 pM1 | Lung, liver | None | None | Wedge resection
(metastasis) lower lobe left lung | HIV, hepatitis B
(chronic) |
|
| 8 | 53/F | 7 | pT3 pN1 M1 | Liver, brain,
bone | 6 cycles of
gemcitabine, 13 cycles of FOLFIRINOX | 30 Gy |
Duodeno-pancreatectomy | PBC |
|
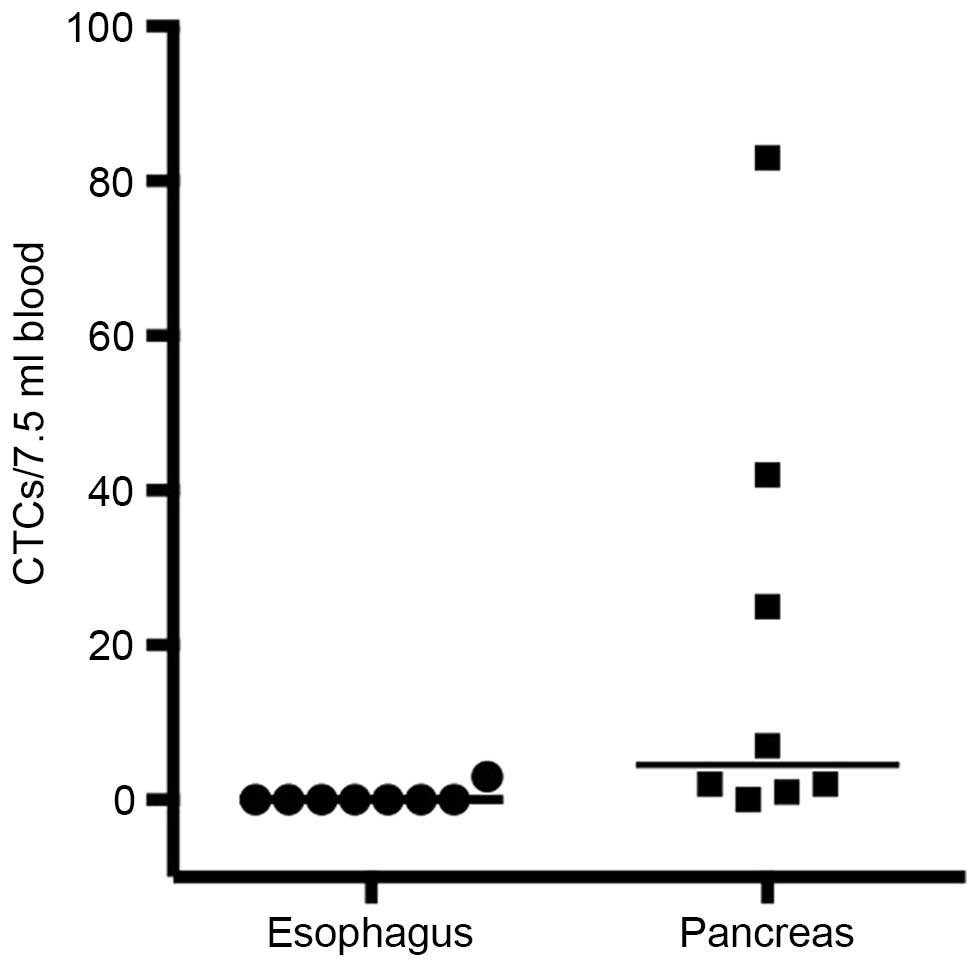
Detection of CTCs
CTCs were detected (CTC count ≥1/7.5 ml of blood) in
the circulation of only 1 out of the 8 patients with AEGJ (12.5% of
total; median CTC count of 3/7.5 ml of blood; Table I). However, CTCs were detected in 7
out of 8 patients (87.5%) with pancreatic adenocarcinoma, where a
median overall CTC count of 4.5/7.5 ml of blood (range, 0–83/7.5 ml
of blood; Table II) was recorded
(Fig. 2).
Discussion
Thus far, the CellSearch® device has only
been approved by the FDA for the detection of CTCs and as a
prognostic tool to predict PFS and OS times in metastatic breast,
colon and prostate cancer (14).
However, as there is only limited literature available regarding
the use of CellSearch® in patients with esophagogastric
or pancreatic cancer (15–18), the present study aimed to determine
whether CTCs are detectable by the CellSearch® system in
these particular patient groups. AEGJ and pancreatic cancer were
chosen due to their epithelial cell characteristic, an increasing
incidence in the Western world and the rather high mortality even
after surgical and/or chemotherapeutic treatments. Therefore,
developing a prognostic tool would be of high clinical importance,
maybe even in order to guide therapeutic decisions. CTCs were
identified in 7 out of 8 pancreatic cancer patients (87.5%), while
detection of CTCs originating from an AEGJ was only possible in 1
out of 8 patients (12.5%). The current study, even though the
number of subjects included was low, offered the advantage of no
inclusion bias, as the patients were randomly screened. At the same
time, it allowed a 1:1 comparison of the two tumor entities. CTCs
were determined using one single device under similar circumstances
within the same period of time at a single university center.
The impact of the presence of CTCs in the
circulation on patient outcome and survival has been studied
extensively over the last years. A recently published meta-analysis
pooling >6,800 patients investigated the prognostic value of
CTCs in breast cancer (19): CTCs
were associated with an increased risk of recurrence of the disease
[hazard ratio (HR), 2.86; 95% confidence interval (CI), 2.19–3.75]
and with significantly higher mortality rates (HR, 2.78; 95% CI,
2.22–3.48). The analysis also provided evidence that the presence
of CTCs was associated with a poorer prognosis in early-stage and
metastatic breast cancer, regardless of the detection method
[CellSearch® assay or reverse-transcriptase polymerase
chain reaction (RT-PCR)] (19). There
have been numerous studies trying to determine a cutoff-value for
the CTC count as a prognostic decision point. Studies have
suggested a CTC count of ≥5/7.5 ml of blood to be valid for
metastatic breast cancer (11,20), and a
count of ≥3/7.5 ml of blood for metastatic colorectal cancer
(21). However, the statistical
determination method of these cutoff-values along with their
prognostic and clinical importance are sources of controversy
(22).
Thus far, the detection of CTCs in the circulation
of patients with AEGJ has been based on anecdotal findings and case
reports (15). A recent study
reported the successful detection of CTCs (≥2 CTCs/7.5 ml of blood)
in 8 out of 18 patients (44.4%) with gastric or esophageal cancer
(16), which could not be confirmed
by the present small series. Notably, the only patient who tested
positive in the current study presented with distant metastases,
whereas CTCs could not be detected in any of the 6 patients staged
M0 [in accordance with the TNM classification (3)]. We may therefore hypothesize that the
stage of the disease could have an impact on the detection (or even
the presence) of CTCs in patients with AEGJ. This would also be in
accordance with the results of a recent study in patients with
esophageal squamous cell carcinoma demonstrating a correlation
between the stage of the disease, the presence of distant
metastasis and the detection of CTCs (16), which has also been shown in patients
with colorectal cancer (23).
For pancreatic cancer, there are also only a few
studies evaluating CTCs. There is certain supporting evidence that
CTCs originating from pancreatic adenocarcinoma can not only be
detected, but may have a prognostic value as well (17): Kurihara et al (17) clearly showed a correlation between
survival times and the presence of CTCs (≥1 CTC/7.5 ml of blood) in
patients with advanced pancreatic carcinoma: In cases where CTCs
were detected, patients with disease stage IV had a mean survival
time of only 53 days, as opposed to 308 days for the CTC-negative
patients (0 CTCs/7.5 ml of blood). Notably, the patient with the
highest number of CTCs (105 CTCs/7.5 ml of blood) succumbed to the
disease 5 days after the measurement. In the present study, the
highest CTC value found was 83 CTCs/7.5 ml of blood. This patient
also succumbed to the disease 4 days after the CTC measurement.
In a larger study (79 patients), Bidard et al
(18) not only showed that
CTC-positive patients with locally advanced pancreatic cancer
(tested prior to and after chemotherapy) experienced shorter
survival times, but also that the tumors of these patients were
poorly-differentiated compared with those of CTC-negative patients.
It has been shown that pancreatic endocrine tumors usually present
with a relatively stable expression of EpCAM, thus making it
possible to detect CTCs of these tumors with any EpCAM-based
enrichment method (24).
A recent study has suggested that the site where the
blood for CTC determination is drawn could also be of importance.
Patients undergoing surgery for pancreatic cancer who presented
with CTCs in portal venous blood exhibited a significantly higher
rate of liver metastases 3 years after surgery compared with
CTC-negative patients, whereas the presence of CTCs in the systemic
circulation had no impact (25).
However, it is possible that CTCs escape the
detection process, even in patients with advanced and metastatic
disease, due to a loss in EpCAM expression, e.g., as found in
breast cancer (26). This
downregulation of EpCAM expression by CTCs is most likely due to
the process of epithelial-to-mesenchymal transition (27), which is a crucial step during the
process of the liberation of CTCs into the circulation (28). This may also explain the fact that the
detection rate of CTCs differs significantly between the different
methods used. The isolation by size of epithelial tumors technique,
which is based on the filtration of cellular blood components
through a membrane microfilter device (29), was able to detect CTCs originating
from pancreatic adenocarcinomas not only more frequently, but also
at higher numbers than the CellSearch® system
[frequency, 93 vs. 40%; median, 9 CTCs/7.5 ml of blood (range,
0–240) vs. 0 CTCs/7.5 ml of blood (range, 0–144, respectively)
(30). Similar findings were reported
for CTCs from esophagogastric adenocarcinoma, where another
size-based enrichment method (MetaCell®) was able to
detect CTCs in 15 out of 20 patients (75.0%) (31).
The number of patients included in the present
preliminary study was small (n=8). It was chosen based on a
reasonable balance between cost effectiveness and the opportunity
to test our hypothesis. No solid conclusions can therefore be drawn
from this finding in comparison with previous studies reporting
larger sample sizes ranging from 16 to 79 patients (17,18,25,30,32).
However, this was also not the overall goal of this study. Instead,
the study aimed to evaluate whether it is generally possible to
detect CTCs in patients with either AEGJ or pancreatic
adenocarcinoma, regardless of the stage of the disease. In
addition, due to the randomly screened nature and the fact that
patients were chosen at various stages of the respective disease,
any form of inclusion bias can definitely be excluded for the
current study, which clearly demonstrates that CTCs originating
from pancreatic adenocarcinoma can be detected by the
CellSearch® device at various stages of the disease. A
direct comparison between the detection rates of CTCs in the AEGJ
and pancreatic patients in the present study may be inadequate, as
the two groups were different in terms of the stage of the disease
(only 2 out of 8 AEGJ patients with distant metastases vs. 4 out of
8 patients in the pancreatic cancer group). However, it can be
concluded that the detection of CTCs in patients with AEGJ at early
stages may be difficult.
Due to the small number of patients in the present
study, we can only speculate about a correlation between the
presence and detection of CTCs in these patients with the stage of
the disease. Therefore, the feasibility of the
CellSearch® system for this particular type of cancer
remains questionable at this point. Recent studies in combination
with the results from the present study suggest that size-based
filtration methods may be superior to the CellSearch®
method for the detection of CTCs in patients with esophagogastric
cancer (31).
Despite its limitations, CellSearch®
offers a good method for the detection of CTCs in several tumor
entities. In addition to the FDA-approved application in breast,
colorectal and prostate cancer, the present study underlines the
possibility that pancreatic adenocarcinoma may be another tumor
entity with solid CTC detection rates (17). The main advantage of the system is its
easy practicability: the blood sample can be stored up to 96 h at
room temperature. In addition, the majority of the steps during the
detection are automated and therefore less prone to human error.
This clearly offers the possibility of performing large multicenter
trials. However, as already discussed, the price for this increase
in practicability may be a loss in sensitivity when compared with
size-based filtration methods (30)
or RT-PCR (33).
In summary, the results of this small pilot study
may be important for the design of future studies with regard to
the number of patients to be included. The preliminary data for
this observational feasibility study suggested that the
CellSearch® system may become a valuable tool for the
detection of CTCs in patients with pancreatic adenocarcinoma,
whereas the usefulness in patients with early-stage esophagogastric
adenocarcinoma may be limited. While large trials focusing on
patients with pancreatic adenocarcinomas may be feasible, further
pilot studies are warranted for esophagogastric tumors.
References
|
1
|
Devesa SS, Blot WJ and Fraumeni JF Jr:
Changing patterns in the incidence of esophageal and gastric
carcinoma in the United States. Cancer. 83:2049–2053. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siewert JR and Stein HJ: Classification of
adenocarcinoma of the oesophagogastric junction. Br J Surg.
85:1457–1459. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sobin LH, Gospodarowicz MK and Wittekind
C: International union against cancer: TNM classification of
malignant tumours. Wiley-Blackwell. Chichester, West Sussex, UK:
2010.
|
|
4
|
Enzinger PC and Mayer RJ: Esophageal
cancer. N Engl J Med. 349:2241–2252. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schiesser M and Schneider PM: Surgical
strategies for adenocarcinoma of the esophagogastric junction.
Recent Results Cancer Res. 182:93–106. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Esposito I, Konukiewitz B, Schlitter AM
and Klöppel G: Pathology of pancreatic ductal adenocarcinoma:
Facts, challenges and future developments. World J Gastroenterol.
20:13833–13841. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hidalgo M: Pancreatic cancer. N Engl J
Med. 362:1605–1617. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Raimondi S, Maisonneuve P and Lowenfels
AB: Epidemiology of pancreatic cancer: An overview. Nat Rev
Gastroenterol Hepatol. 6:699–708. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Arvold ND, Ryan DP, Niemierko A,
Blaszkowsky LS, Kwak EL, Wo JY, Allen JN, Clark JW, Wadlow RC, Zhu
AX, et al: Long-term outcomes of neoadjuvant chemotherapy before
chemoradiation for locally advanced pancreatic cancer. Cancer.
118:3026–3035. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cristofanilli M, Budd GT, Ellis MJ,
Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ,
Terstappen LW and Hayes DF: Circulating tumor cells, disease
progression and survival in metastatic breast cancer. N Engl J Med.
351:781–791. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hayes DF, Cristofanilli M, Budd GT, Ellis
MJ, Stopeck A, Miller MC, Matera J, Allard WJ, Doyle GV and
Terstappen LW: Circulating tumor cells at each follow-up time point
during therapy of metastatic breast cancer patients predict
progression-free and overall survival. Clin Cancer Res.
12:4218–4224. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
de Wit S, van Dalum G and Terstappen LW:
Detection of circulating tumor cells. Scientifica (Cairo).
2014:8193622014.PubMed/NCBI
|
|
14
|
Gorges TM and Pantel K: Circulating tumor
cells as therapy-related biomarkers in cancer patients. Cancer
Immunol Immunother. 62:931–939. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tu Q, Bittencourt Mde C, Cai H, Bastien C,
Lemarie-Delaunay C, Bene MC and Faure GC: Case Report: Detection
and quantification of tumor cells in peripheral blood and ascitic
fluid from a metastatic esophageal cancer patient using the
CellSearch (R) technology. F1000Res. 3:122014.PubMed/NCBI
|
|
16
|
Matsushita D, Uenosono Y, Arigami T,
Yanagita S, Nishizono Y, Hagihara T, Hirata M, Haraguchi N, Arima
H, Kijima Y, et al: Clinical significance of circulating tumor
cells in peripheral blood of patients with esophageal squamous cell
carcinoma. Ann Surg Oncol. 22:3674–3680. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kurihara T, Itoi T, Sofuni A, Itokawa F,
Tsuchiya T, Tsuji S, Ishii K, Ikeuchi N, Tsuchida A, Kasuya K, et
al: Detection of circulating tumor cells in patients with
pancreatic cancer: A preliminary result. J Hepatobiliary Pancreat
Surg. 15:189–195. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Bidard FC, Huguet F, Louvet C, Mineur L,
Bouché O, Chibaudel B, Artru P, Desseigne F, Bachet JB, Mathiot C,
et al: Circulating tumor cells in locally advanced pancreatic
adenocarcinoma: The ancillary CirCe 07 study to the LAP 07 trial.
Ann Oncol. 24:2057–2061. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhang L, Riethdorf S, Wu G, Wang T, Yang
K, Peng G, Liu J and Pantel K: Meta-analysis of the prognostic
value of circulating tumor cells in breast cancer. Clin Cancer Res.
18:5701–5710. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Botteri E, Sandri MT, Bagnardi V, Munzone
E, Zorzino L, Rotmensz N, Casadio C, Cassatella MC, Esposito A,
Curigliano G, et al: Modeling the relationship between circulating
tumour cells number and prognosis of metastatic breast cancer.
Breast Cancer Res Treat. 122:211–217. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sastre J, Vidaurreta M, Gómez A, Rivera F,
Massutí B, López MR, Abad A, Gallen M, Benavides M, Aranda E, et
al: Prognostic value of the combination of circulating tumor cells
plus KRAS in patients with metastatic colorectal cancer treated
with chemotherapy plus bevacizumab. Clin Colorectal Cancer.
12:280–286. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fehm T and Sauerbrei W: Information from
CTC measurements for metastatic breast cancer prognosis-we should
do more than selecting an ‘optimal cut point’. Breast Cancer Res
Treat. 122:219–220. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Romiti A, Raffa S, Di Rocco R, Roberto M,
Milano A, Zullo A, Leone L, Ranieri D, Mazzetta F, Medda E, et al:
Circulating tumor cells count predicts survival in colorectal
cancer patients. J Gastrointestin Liver Dis. 23:279–284.
2014.PubMed/NCBI
|
|
24
|
Khan MS, Tsigani T, Rashid M, Rabouhans
JS, Yu D, Luong TV, Caplin M and Meyer T: Circulating tumor cells
and EpCAM expression in neuroendocrine tumors. Clin Cancer Res.
17:337–345. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bissolati M, Sandri MT, Burtulo G, Zorzino
L, Balzano G and Braga M: Portal vein-circulating tumor cells
predict liver metastases in patients with resectable pancreatic
cancer. Tumour Biol. 36:991–996. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Königsberg R, Obermayr E, Bises G, Pfeiler
G, Gneist M, Wrba F, de Santis M, Zeillinger R, Hudec M and
Dittrich C: Detection of EpCAM positive and negative circulating
tumor cells in metastatic breast cancer patients. Acta Oncol.
50:700–710. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gorges TM, Tinhofer I, Drosch M, Röse L,
Zollner TM, Krahn T and von Ahsen O: Circulating tumour cells
escape from EpCAM-based detection due to epithelial-to-mesenchymal
transition. BMC Cancer. 12:1782012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Gonzalez DM and Medici D: Signaling
mechanisms of the epithelial-mesenchymal transition. Sci Signal.
7:re82014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Vona G, Sabile A, Louha M, Sitruk V,
Romana S, Schütze K, Capron F, Franco D, Pazzagli M, Vekemans M, et
al: Isolation by size of epithelial tumor cells: A new method for
the immunomorphological and molecular characterization of
circulating tumor cells. Am J Pathol. 156:57–63. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Khoja L, Backen A, Sloane R, Menasce L,
Ryder D, Krebs M, Board R, Clack G, Hughes A, Blackhall F, et al: A
pilot study to explore circulating tumour cells in pancreatic
cancer as a novel biomarker. Br J Cancer. 106:508–516. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bobek V, Matkowski R, Gürlich R, Grabowski
K, Szelachowska J, Lischke R, Schützner J, Harustiak T, Pazdro A,
Rzechonek A and Kolostova K: Cultivation of circulating tumor cells
in esophageal cancer. Folia Histochem Cytobiol. 52:171–177. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Allard WJ, Matera J, Miller MC, Repollet
M, Connelly MC, Rao C, Tibbe AG, Uhr JW and Terstappen LW: Tumor
cells circulate in the peripheral blood of all major carcinomas but
not in healthy subjects or patients with nonmalignant diseases.
Clin Cancer Res. 10:6897–6904. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Gervasoni A, Sandri MT, Nascimbeni R,
Zorzino L, Cassatella MC, Baglioni L, Panigara S, Gervasi M, Di
Lorenzo D and Parolini O: Comparison of three distinct methods for
the detection of circulating tumor cells in colorectal cancer
patients. Oncol Rep. 25:1669–1703. 2011.PubMed/NCBI
|
|
34
|
Sobin LH, Gospodarowicz MK and Wittekind
C: International Union Against Cancer: TNM Classification of
Malignant Tumours. Wiley-Blackwell. Chichester: 2010.
|
|
35
|
Vestbo J, Hurd SS, Agusti AG, Jones PW,
Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ,
Nishimura M, et al: Global strategy for the diagnosis, management,
and prevention of chronic obstructive pulmonary disease: GOLD
executive summary. Am J Respir Crit Care Med. 187:347–365. 2013.
View Article : Google Scholar : PubMed/NCBI
|