Introduction
Synchronous cancers are characterized by the
simultaneous occurrence of multiple primary tumors in the same
patient. Synchronous malignancies most commonly occur in the colon,
with a particularly high prevalence in elderly patients (1,2). The
occurrence of synchronous colorectal cancers is extremely rare and
may be identified at any location within the large intestine
(3). Synchronous cancers are
relatively uncommon, and triple synchronous colon cancers are
particularly rare. The majority of studies have identified that
synchronous colorectal cancers more frequently occur in the right
colon when compared with single tumors (4,5).
Surgical resection is the primary treatment option
for synchronous colorectal cancers. Recently, laparoscopic surgery
has been used in synchronous colorectal cancers successfully, as
evaluated by certain studies; however, controversy remains
concerning operative procedures for multiple segmental resections,
and total or subtotal colectomy (6,7). Thus, at
present, no standard treatment for synchronous colon cancer has
been established. There is no difference in survival between
synchronous colorectal cancers and single colorectal cancers, if
resections are curative. In addition, the pathological stages
between these two types of tumor are identical (5,8,9). The present study reports the case of a
52-year-old male patient who presented with triple synchronous
cancer arising from the colon, which was successfully treated with
laparoscopic subtotal colectomy.
Case report
A 52-year-old man was admitted to Subei People's
Hospital of Jiangsu (Yangzhou, China) on October 3, 2014, and
presented with a 2-month history of abdominal pain, intermittent
hematochezia and weight loss. The patient had no significant
medical history, no family history of cancer and was a non-smoker.
Physical examination revealed deep tenderness at the left lower
quadrant of the abdomen without rebound tenderness on palpation.
Laboratory examinations revealed no significant abnormal results.
Hemoglobin and cancer tumor markers, including cancer antigen 19-9,
α-fetoprotein, carcinoembryonic antigen and prostate-specific
antigen were all within the normal ranges. In addition, chest
X-ray, electrocardiogram, ultrasonic cardiogram and pulmonary
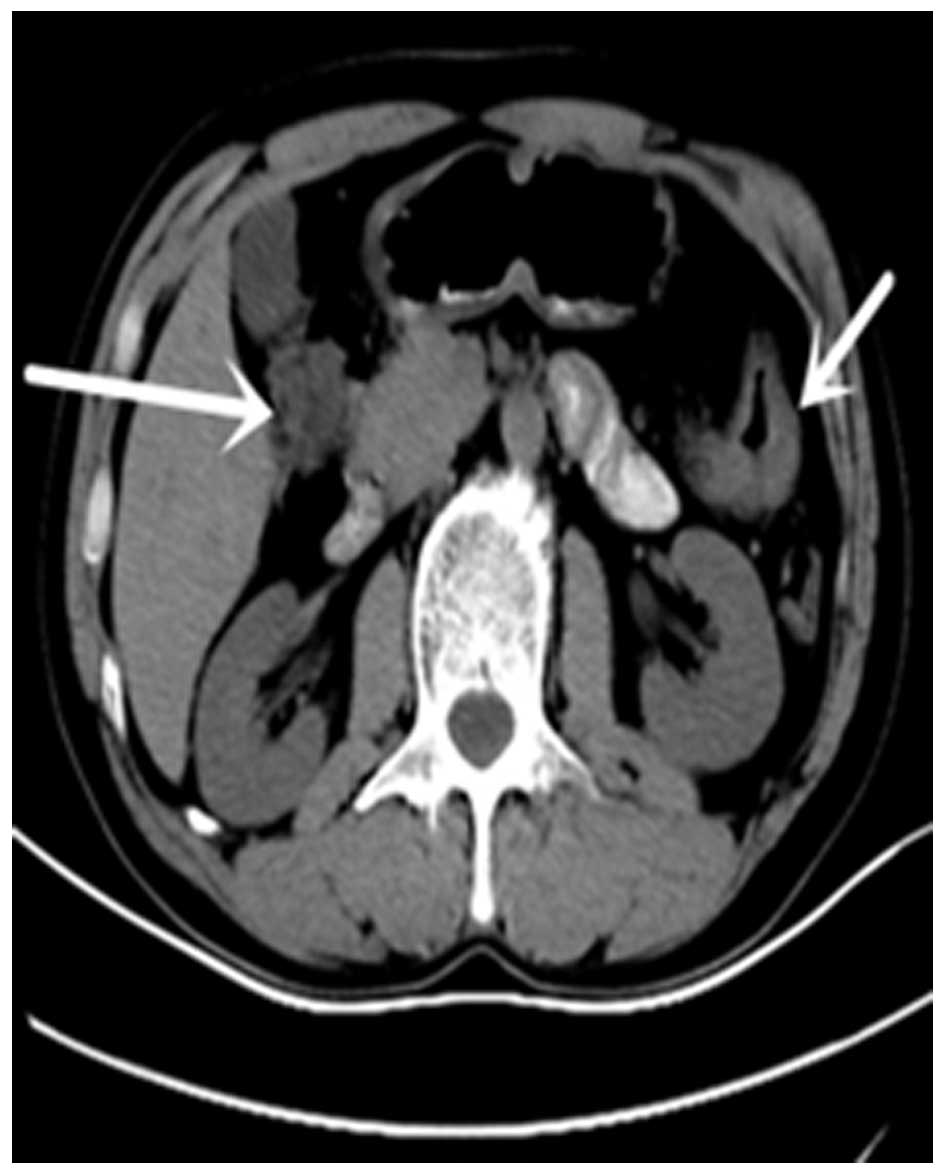
function tests were all normal. Computed tomography (CT) of the
abdomen revealed marked intestinal wall thickness in the transverse
colon and volvulus in the hepatic flexure of the colon (Fig. 1). Colon cancer was suspected.
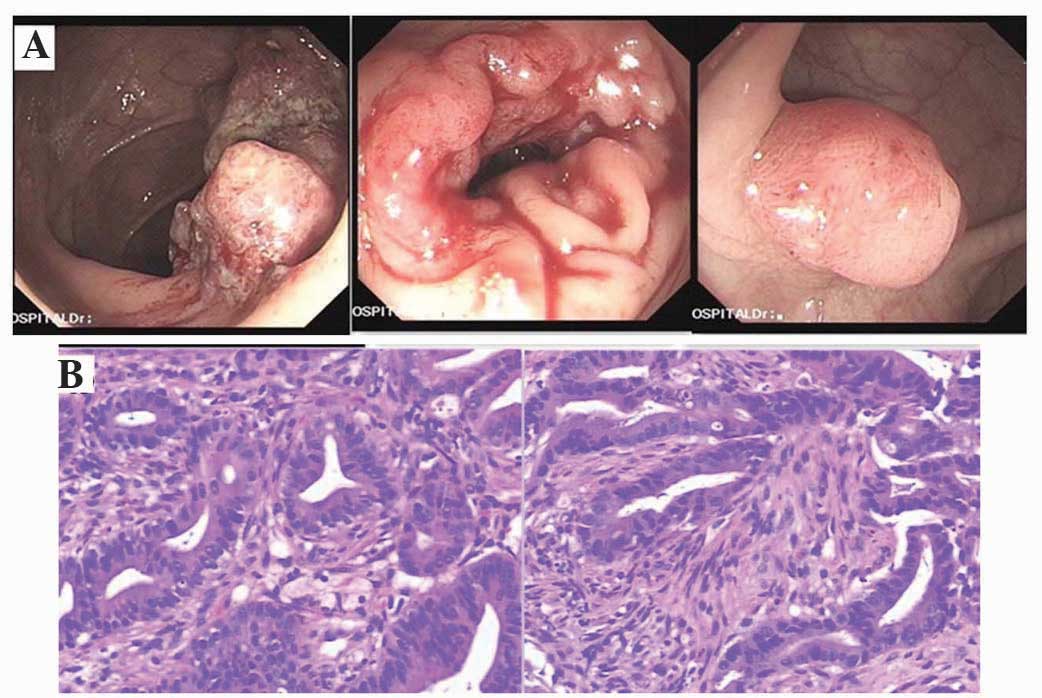
Colonoscopy identified 3 tumors: The first tumor was
located in the descending colon, with lumen stenosis observed ~60
cm from the anal verge; the second tumor was located in the hepatic
flexure of colon; and the third tumor was located in the sigmoid
colon, 23 cm from the anal verge (Fig.
2A). Histopathological examination of biopsy specimens led to a
diagnosis of adenocarcinoma for the tumors of the descending colon
and the hepatic flexure of the colon, while the sigmoid tumor was
identified as tubulovillous adenoma with moderate epithelial
dysplasia. Biopsy specimens were fixed in formalin, embedded in
paraffin, sliced to a 5 µm-thickness and stained with hematoxylin
and eosin. The results of staining revealed atypical cells that
were adenoid with papillary or villous distribution and invasive
growth. Synchronous adenocarcinoma of the descending colon and the
hepatic flexure of colon was confirmed by colonoscopy and
pathological examination (Fig.
2B).
Subsequent laparoscopic exploration confirmed the
presence of one tumor (diameter, 6 cm) in the hepatic flexure of
the colon, a second tumor (diameter, 5 cm) in the descending colon
and a third tumor (diameter, 2 cm) in the sigmoid colon, without
serous invasion. No metastatic tumors were identified in the
abdominal cavity or liver. However, exploration revealed enlarged
lymph nodes in the mesentery proximal to the hepatic flexure of the
colon and descending colon. Subsequently, an extended hemicolectomy
from the terminal ileum to the sigmoid was performed under
laparoscopy (Fig. 3). The right half
of the colon was separated, followed by the left half, and
end-to-side anastomosis between the jejunum and sigmoid colon was
performed. The operative duration was 160 min with intraoperative
blood loss of ~100 ml.
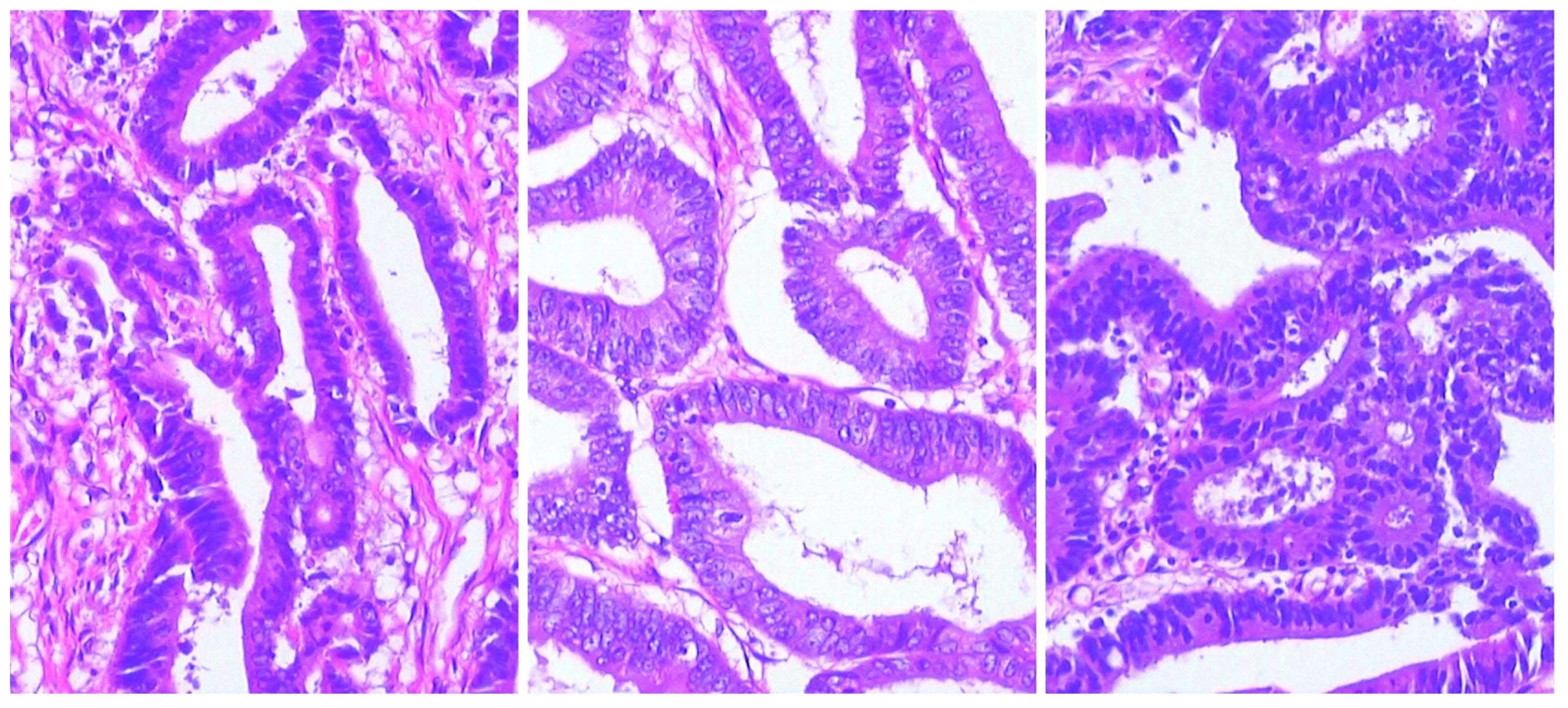
Resected tissues were were fixed in formalin,
embedded in paraffin, sliced to a 5 µm-thickness and stained with
hematoxylin and eosin. The results of staining revealed that the
cancerous cells were arranged in a tubular arrangement, and cells
had large nuclei with deep staining, with lighter staining of the
cytoplasm. Staining also revealed invasive growth.
Histopathological examination of the resected tissue specimens
revealed 3 tumors (Fig. 4). The tumor
at the hepatic flexure of the colon was identified as protruding
adenocarcinoma and a foci with mucinous adenocarcinoma, which had
invaded up to the serous membrane. Another tumor was observed at
the descending colon, which was infiltrating adenocarcinoma, which
had also invaded up to the serous membrane. The third tumor was
located in the sigmoid colon ~3.5 cm from the sigmoid valve, which
was diagnosed as adenocarcinoma with invasion of the submucosa. In
addition, 26 regional lymph nodes without any metastasis were
resected; however, hematoxylin and eosin staining and
immunohistochemical examination of the appendix indicated tumor
invasion. Laparoscopic surgery was considered superior to
traditional open surgery as it causes less trauma, resulting in a
quick recovery. The patient recovered well and was discharged 10
days after surgery. The patient did not undergo chemotherapy
following surgery, due to personal reasons. Subsequent to 19 months
of follow-up examinations, which consisted of CT and colonoscopy
every 6 months, the patient exhibited no signs of recurrence. The
present study was approved by the Ethical Committee of Subei
People's Hospital of Jiangsu and written informed consent was
obtained from the patient.
Discussion
Synchronous colorectal cancers are defined as tumors
that are diagnosed at the same time as or within 6 months of the
initial diagnosis of another primary tumor, excluding metastatic
lesions from other primary cancers. Generally, synchronous tumors
occur ≥4 cm from each other (10,11). With
the development of diagnostic technologies, increasing numbers of
synchronous colorectal cancers are identified clinically. The
prevalence of synchronous colorectal carcinoma has been reported to
range between 3 and 6% (10–13). However, the actual incidence is
considered to be higher as not all tumors are identified by
colonoscopy. A number of tumors may remain undetected due to bowel
obstruction or poor bowel preparation (2). Furthermore, certain tumors at early
histological stages cannot be verified by histopathological
examination of colonoscopy (14). In
the present study, a rare case of triple synchronous cancer arising
from the hepatic flexure of the colon, descending colon and the
sigmoid in a 52-year-old male was reported. Notably, the patient
had no family history of cancer or genetic predisposing
factors.
The preoperative or intraoperative diagnosis of
multiple synchronous colorectal carcinomas is extremely important,
but remains challenging. It is difficult to identify certain small
tumors on CT, and sometimes complete examination of the large
intestine cannot be conducted, due to intestinal lumen stenosis.
The combined use of CT and colonoscopy has been reported as a
useful tool for the preoperative evaluation of synchronous
colorectal carcinoma (15,16). Colonoscopic examination may provide
clear images of the whole colon. CT is also a sensitive examination
for synchronous colorectal carcinoma, particularly in patients that
have undergone incomplete colonoscopy (17); however, a number of small tumors may
be missed. In the present case, 2 tumors were identified by CT,
while colonoscopy revealed 3 tumors. (Fig. 2A). It was initially unclear whether
the lesion in the sigmoid colon was a benign or malignant tumor.
Additional imaging examinations, such as magnetic resonance
colonography and positron emission tomography-CT have also been
reported as useful tools for the diagnosis of synchronous
colorectal carcinoma (18,19).
Surgical resection is the most common treatment for
synchronous colorectal cancers. However, initial surgical
procedures for multiple colorectal carcinomas remain controversial;
surgical procedures for multiple lesions or cancers should be
individualized according to the tumor location, depth of invasion
and the general health of the patient. Previous studies have
recommended the use of total or subtotal colectomy to resect any
potential existing synchronous tumors or polyps that have not been
detected in patients exhibiting lesions in separate segments
(20–23). However, another study reported that
traditional surgical methods should be used for multiple segmental
resections to preserve the normal colon (24). In patients with tumors in adjacent
segments, a more extensive resection, including removal of the
proximal intestinal and local lymph nodes, is required (5). Radical curative surgery for synchronous
triple colorectal cancer aims to remove all tumors. Certain studies
have recommended that intraoperative colonoscopy should be
conducted to confirm that no additional tumors are present
(2,25). However, the effectiveness of
intraoperative colonoscopy is controversial as the procedure
increases the risk of infection (26). In the present case, an extended
hemicolectomy from the terminal ileum to sigmoid was performed
under laparoscopy with ileosigmoidostomy anastomosis, and thus we
hypothesized that subtotal colectomy would ensure that all tumors
were removed. Histopathological examination of the resected tissue
specimens confirmed that all tumors had been resected.
A previous study indicated that subtotal colectomy
may increase defecation frequency as the normal colon cannot be
preserved (27). In the present case,
the patient exhibited normal defecation by the third postoperative
day without diarrhea. Thus, in the present case laparoscopic
subtotal colectomy was successful in removing all 3 tumors without
any serious side effects.
In summary, the present study reported a case of
triple synchronous colorectal cancer in a patient with no family
history of cancer. The first tumor was located in the descending
colon with lumen stenosis, ~60 cm from the anal verge, the second
tumor was located in the hepatic flexure of colon and the third
lesion was located in the sigmoid colon, 23 cm from the anal verge.
All three tumors were removed by laparoscopic subtotal colectomy.
Therefore, laparoscopic subtotal colectomy presents an effective
surgical approach for synchronous colorectal cancer following
imaging and endoscopic diagnosis.
Acknowledgements
This study was supported by The Department of
Gastrointestinal Surgery of Subei People's Hospital.
References
|
1
|
Fukatsu H, Kato J, Nasu JI, Kawamoto H,
Okada H, Yamamoto H, Sakaguchi K and Shiratori Y: Clinical
characteristics of synchronous colorectal cancer are different
according to tumour location. Dig Liver Dis. 39:40–46. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yeh CC, Hsi SC, Chuu CP and Kao YH:
Synchronous triple carcinoma of the colon and rectum. World J Surg
Oncol. 11:662013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang J, Peng JY and Chen W: Synchronous
colorectal cancers: A review of clinical features, diagnosis,
treatment, and prognosis. Dig Surg. 28:379–385. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chen HS and Sheen-Chen SM: Synchronous and
“early” metachronous colorectal adenocarcinoma: Analysis of
prognosis and current trends. Dis Colon Rectum. 43:1093–1099. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Passman MA, Pommier RF and Vetto JT:
Synchronous colon primaries have the same prognosis as solitary
colon cancers. Dis Colon Rectum. 39:329–334. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hirano Y, Hattori M, Sato Y, Maeda K,
Douden K and Hashizume Y: Concurrent single-incision laparoscopic
right hemicolectomy and sigmoidectomy for synchronous carcinoma:
Report of a case. Indian J Surg. 75:293–295. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Bardakcioglu O and Ahmed S: Single
incision laparoscopic total abdominal colectomy with ileorectal
anastomosis for synchronous colon cancer. Tech Coloproctol.
14:257–261. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Latournerie M, Jooste V, Cottet V, Lepage
C, Faivre J and Bouvier AM: Epidemiology and prognosis of
synchronous colorectal cancers. Br J Surg. 95:1528–1533. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nikoloudis N, Saliangas K, Economou A,
Andreadis E, Siminou S, Manna I, Georgakis K and Chrissidis T:
Synchronous colorectal cancer. Tech Coloproctol 8 Suppl.
1:s177–179. 2004. View Article : Google Scholar
|
|
10
|
Cunliffe WJ, Hasleton PS, Tweedle DE and
Schofield PF: Incidence of synchronous and metachronous colorectal
carcinoma. Br J Surg. 71:941–943. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mulder SA, Kranse R, Damhuis RA, de Wilt
JH, Ouwendijk RJ, Kuipers EJ and van Leerdam ME: Prevalence and
prognosis of synchronous colorectal cancer: A Dutch
population-based study. Cancer Epidemiol. 35:442–447. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Welch JP: Multiple colorectal tumors. An
appraisal of natural history and therapeutic options. Am J Surg.
142:274–280. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Derwinger K and Gustavsson B: A study of
aspects on gender and prognosis in synchronous colorectal cancer.
Clin Med Insights Oncol. 5:259–264. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hancock RJ: Synchronous carcinoma of the
colon and rectum. Am Surg. 41:560–563. 1975.PubMed/NCBI
|
|
15
|
Kim MS and Park YJ: Detection and
treatment of synchronous lesions in colorectal cancer: The clinical
implication of perioperative colonoscopy. World J Gastroenterol.
13:4108–4111. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
McArthur DR, Mehrzad H, Patel R, Dadds J,
Pallan A, Karandikar SS and Roy-Choudhury S: CT colonography for
synchronous colorectal lesions in patients with colorectal cancer:
Initial experience. Eur Radiol. 20:621–629. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pang EJ, Liu WJ, Peng JY, Chen NW and Deng
JH: Prediction of synchronous colorectal cancers by computed
tomography in subjects receiving an incomplete colonoscopy: A
single-center study. World J Gastroenterol. 21:1857–1864. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Achiam MP, Holst Andersen LP, Klein M,
Chabanova E, Thomsen HS and Rosenberg J: Preoperative evaluation of
synchronous colorectal cancer using MR colonography. Acad Radiol.
16:790–797. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kinner S, Antoch G, Bockisch A and
Veit-Haibach P: Whole-body PET/CT-colonography: A possible new
concept for colorectal cancer staging. Abdom Imaging. 32:606–612.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang HZ, Huang XF, Wang Y, Ji JF and Gu J:
Clinical features, diagnosis, treatment and prognosis of multiple
primary colorectal carcinoma. World J Gastroenterol. 10:2136–2139.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Slater G, Aufses AH Jr and Szporn A:
Synchronous carcinoma of the colon and rectum. Surg Gynecol Obstet.
171:283–287. 1990.PubMed/NCBI
|
|
22
|
Easson AM, Cotterchio M, Crosby JA,
Sutherland H, Dale D, Aronson M, Holowaty E and Gallinger S: A
population-based study of the extent of surgical resection of
potentially curable colon cancer. Ann Surg Oncol. 9:380–387. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Enker WE and Dragacevic S: Multiple
carcinomas of the large bowel: A natural experiment in etiology and
pathogenesis. Ann Surg. 187:8–11. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Adloff M, Arnaud JP, Bergamaschi R and
Schloegel M: Synchronous carcinoma of the colon and rectum:
Prognostic and therapeutic implications. Am J Surg. 157:299–302.
1989. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kaibara N, Kimura O, Nishidoi H, Miyano Y
and Koga S: Intraoperative colonoscopy for the diagnosis of
multiple cancers of the large intestine. Jpn J Surg. 12:117–121.
1982. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Torralba JA, Robles R, Parrilla P, Lujan
JA, Liron R, Piñero A and Fernandez JA: Subtotal colectomy vs.
intraoperative colonic irrigation in the management of obstructed
left colon carcinoma. Dis Colon Rectum. 41:18–22. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Holubar SD, Wolff BG, Poola VP and Soop M:
Multiple synchronous colonic anastomoses: Are they safe? Colorectal
Dis. 12:135–140. 2010. View Article : Google Scholar : PubMed/NCBI
|