Introduction
Primary leiomyosarcoma (LMS) of the splenic vein is
a rare malignant tumor and there have only been three previously
reported cases (1,2). Due to the rarity of the tumor, its
imaging features have not yet been described in detail. Venous LMSs
predominately occur in middle-aged women in the fifth and sixth
decades of life (3). Clinical
manifestations depend on the tumor position in the vessel wall
(4). The symptoms of LMS include
abdominal masses, abdominal pain, nausea and fever (5). The current study presents a case report
on the magnetic resonance imaging (MRI) features of primary LMS of
the splenic vein. A solid, heterogeneous mass was located in the
tail of the pancreas. In portal phase, the splenic vein was
embedded in the mass on T1-weighted imaging (T1WI). The patient
underwent splenic pedicle tumor resection, splenectomy and liver
tumor resection with no postoperative complications. There is a
limited amount of evidence demonstrating increased survival
following adjuvant radiation, combination radiation and
chemotherapy, in addition to surgical resection (6). Further information regarding the
prognosis of the present patient is unavailable, as the patient did
not undergo further adjuvant therapy or follow-up, and unique
treatment recommendations or outcome data for such lesions remains
to be established.
Case report
In June 2013, a 52-year-old male was admitted to the
Gastroenterology Department of The Second Affiliated Hospital of
Kunming Medical University (Kunming, China) presenting with a long
history (>1 year) of intermittent epigastric pain. The pain
presented as either severe colic lasting for 20–30 min or as dull
pain, which would be relieved following squatting. The medical
history of the patient was unremarkable. A whole body positron
emission tomography scan was performed at Yuxi People's Hospital
(Yuxi, China) and revealed an irregular mass in the splenic hilum
without increased metabolism.
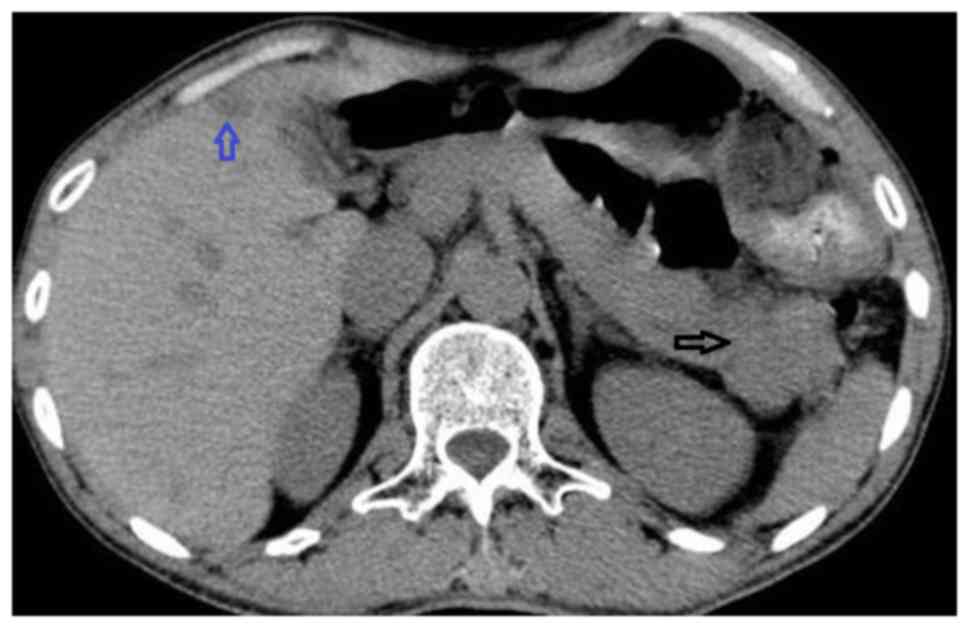
An abdominal computed tomography (CT) scan performed
at the Department of Radiology, The Second Affiliated Hospital of
Kunming Medical University identified an irregular, hypodense mass
measuring ~4.1×3.0 cm in the tail of the pancreas, while a
hypodense lesion was also observed in the right hepatic lobe
(Fig. 1). Following administration of
contrast agent, lesions exhibited peripheral enhancement and there
was a low-density zone in the center of the lesion without
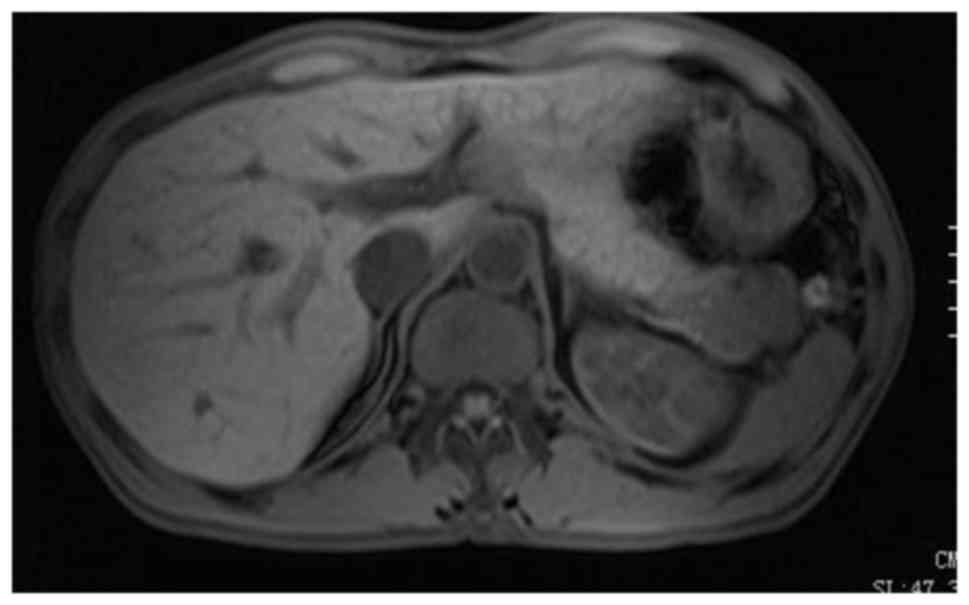
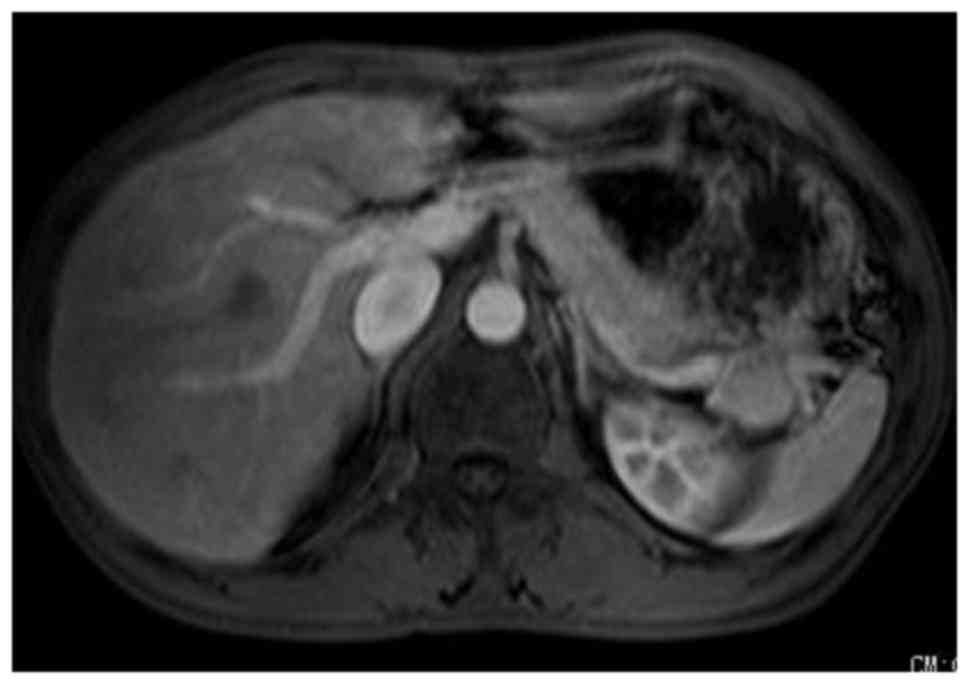
enhancement (Figs. 2 and 3). An MRI scan identified a solid,
heterogeneous mass, which had fused with two nodules measuring
1.87×2.44 cm and 2.46×2.34 cm, located in the tail of the pancreas.
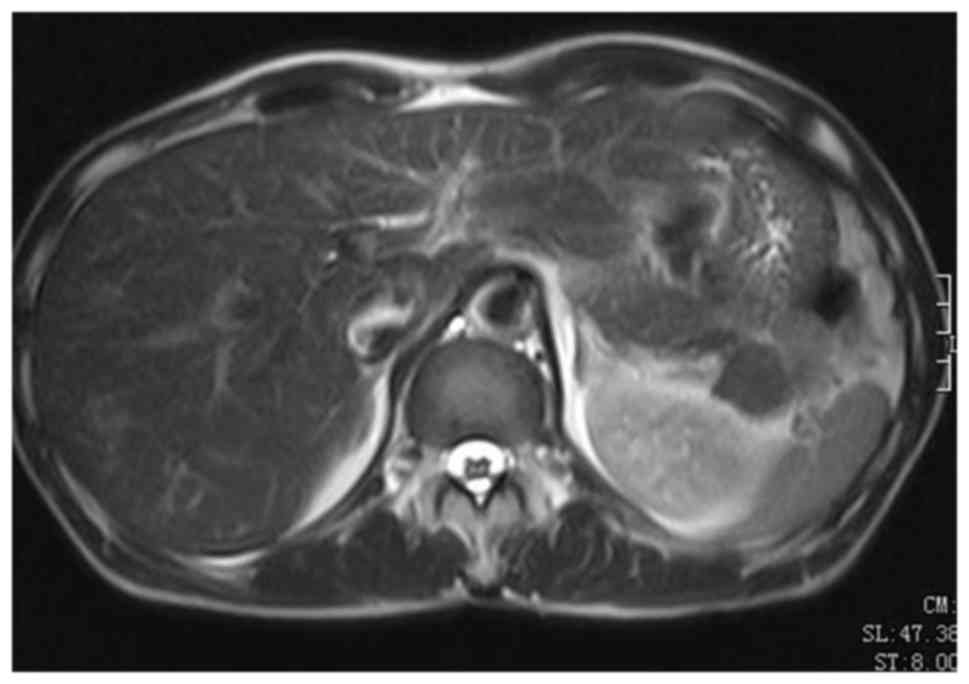
T1WI (Fig. 4) demonstrated slight
hypointensity, while T2-WI exhibited slight hyperintensity
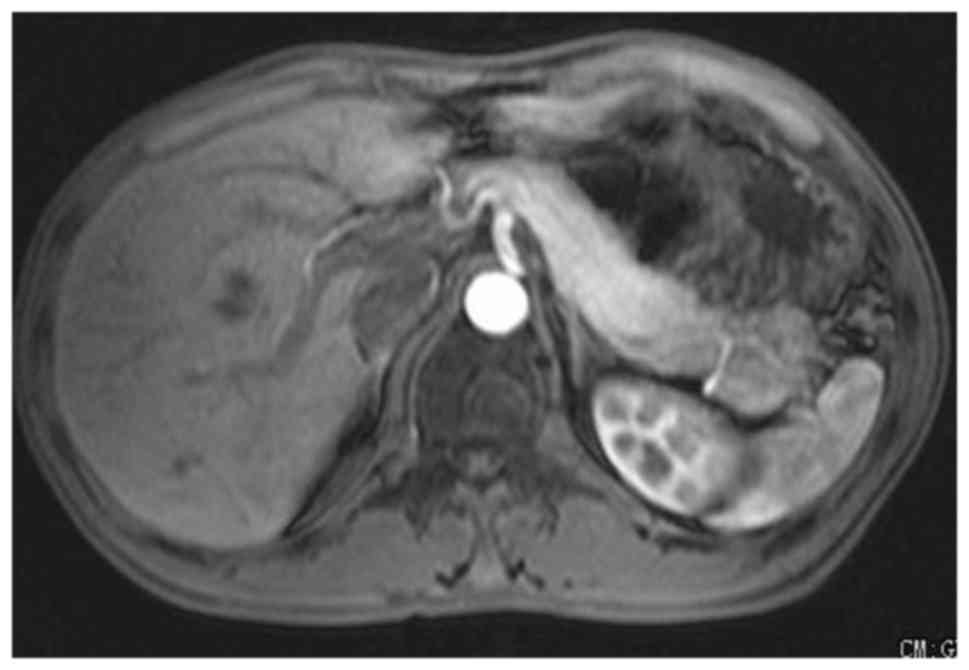
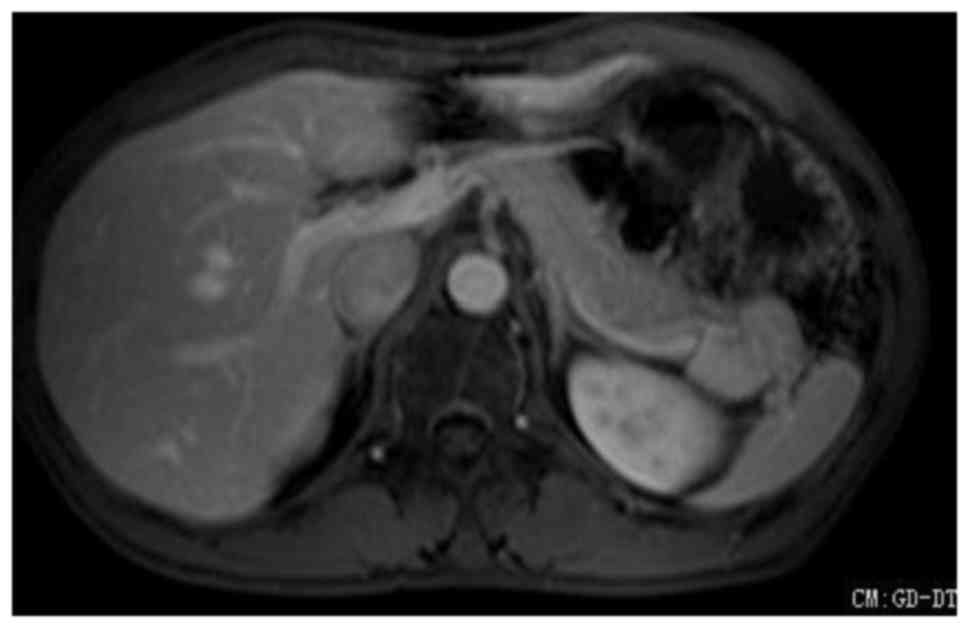
(Fig. 5). Mild inhomogeneous
enhancement was observed in the arterial phase (Fig. 6), strengthening in the portal phase
(Fig. 7) was higher than the arterial
phase and the splenic vein was embedded in the mass on T1WI
enhanced images. The delay period exhibited inhomogeneous moderate
enhancement (Fig. 8) and a small
nodule was located between the liver VI (right hepatic lobe lower
section) and the liver V (lower right anterior lobe of the liver).
The nodule in the liver exhibited slight hypointensity on T1WI,
which was similar to the liver signal on T2WI, and the lesion
demonstrated peripheral enhancement post-contrast.
An initial diagnosis of pancreatic cancer was
considered and surgery was scheduled. The patient subsequently
underwent splenic pedicle tumor resection, splenectomy and liver
tumor resection. Following surgical resection, specimens were fixed
in 10% neutral formalin for 12 h, embedded in paraffin and cut into
4 µm-thick sections. These sections were subsequently stained with
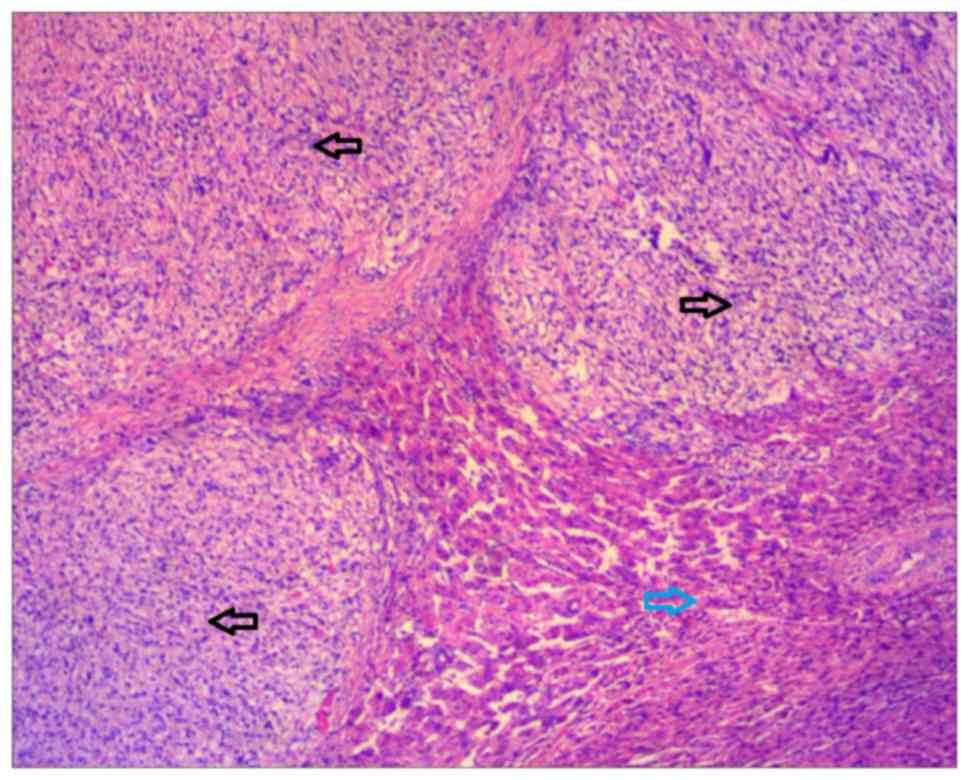
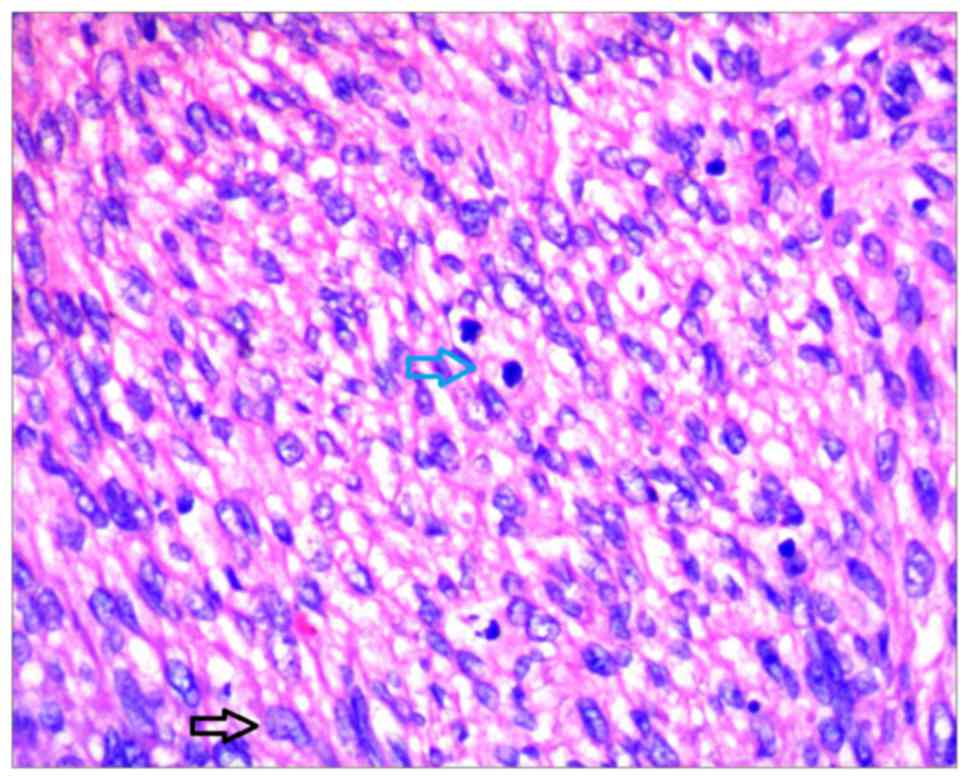
hematoxylin and eosin. The tumor was composed of bundles of
staggered and spindle cells with necrosis. Atypia and mitosis were
easily observable. For immunohistochemistry, paraffin-embedded
sections were dewaxed, rehydrated and incubated with the following
primary antibodies for 1 h at 37°C: Anti-vimentin (catalog no.
RMA-0547; no dilution), anti-smooth muscle actin (catalog no.
Kit-0006; no dilution), anti-desmin (catalog no. Kit-0023; no
dilution), anti-H-caldesmon (catalog no. MAB-0634; no dilution) and
anti-Ki-67 (catalog no. Kit-0005; no dilution; Fuzhou Maixin
Biotech. Co., Ltd., Fuzhou, China). The sections were subsequently
incubated with the biotin-labeled secondary antibody (catalog no.,
Kit-9730; no dilution; Fuzhou Maixin Biotech. Co., Ltd.) for 0.5 h
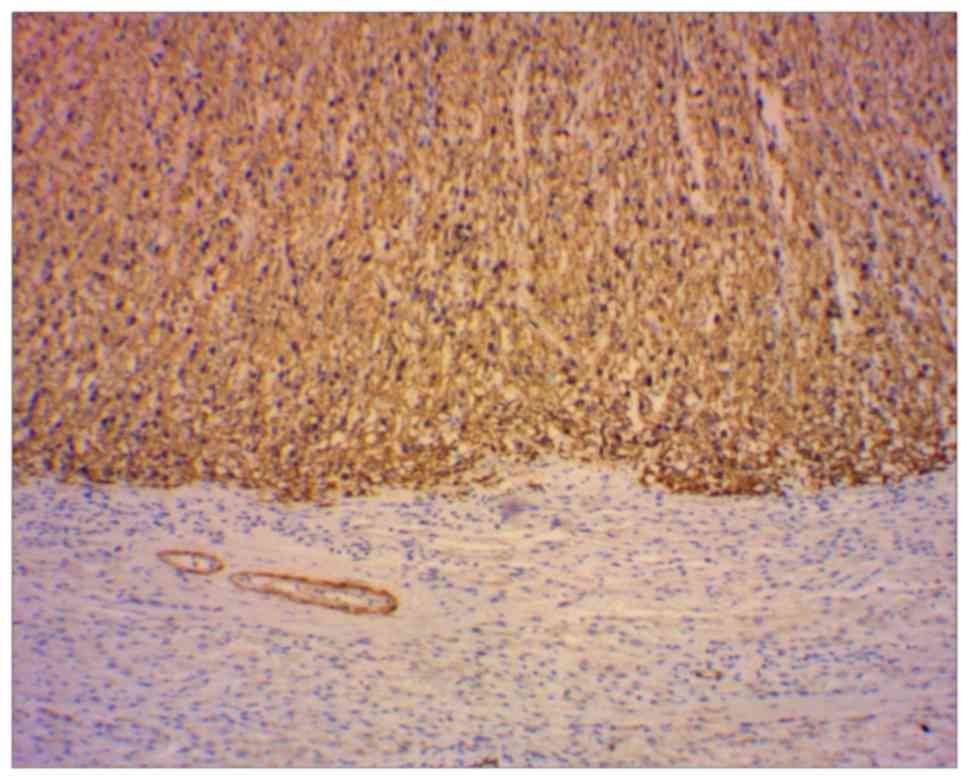
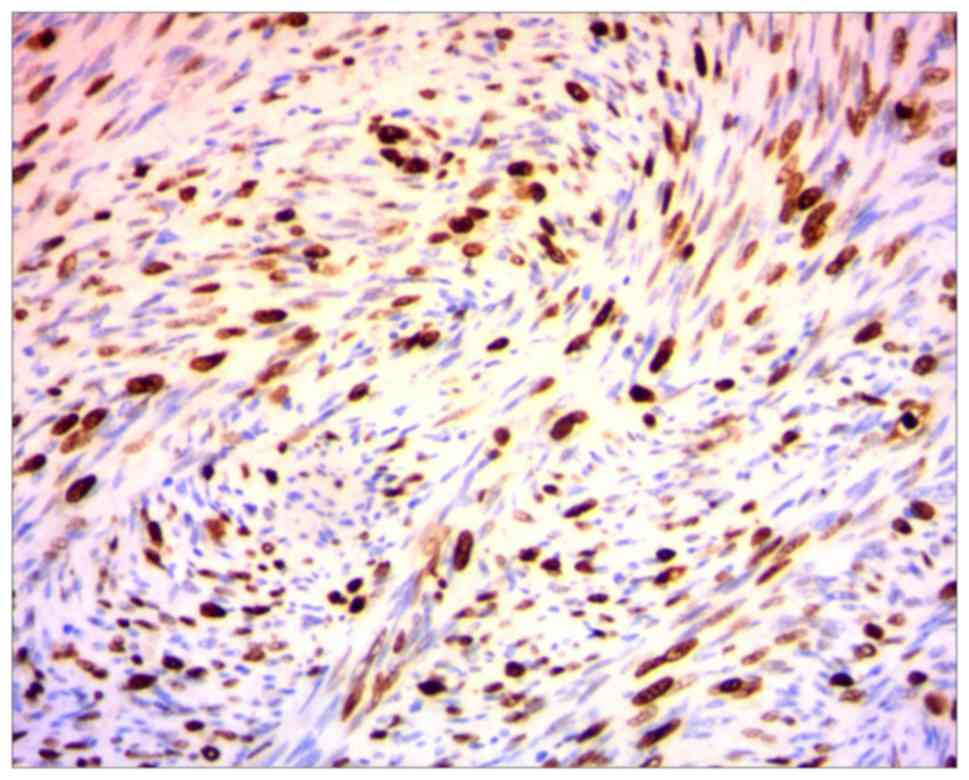
at 37°C. Immunohistochemistry demonstrated positive expression of
vimentin, smooth muscle actin, desmin, H-caldesmon, Ki-67 and
cluster of differentiation 34 (Figs.
9 and 10). Finally,
histopathological examinations confirmed both tumors were
intermediate-grade LMSs (Figs. 11
and 12).
Discussion
LMSs are rare, malignant, mesenchymal tumors derived
from smooth muscle that usually appear in the retroperitoneum space
behind the abdominal cavity or the uterus (3). LMSs may occur intra-abdominally in the
retroperitoneum, mesentery or omentum (40–45%), in subcutaneous or
deep soft tissue of the limbs (20–30%), in the arrector pili muscle
of the skin (15–20%), or in blood vessel walls (5%) (1). LMSs are rare and aggressive neoplasms
that arise from the blood vessel walls, and vascular LMSs occur
more commonly in veins (3). Previous
studies have demonstrated that vascular LMSs occur in veins five
times more often than in arteries (3). The inferior vena cava locates 50% of
large-vessel LMSs and the retroperitoneal veins close to the
inferior vena cava, including the iliac, renal, and spermatic and
ovarian veins, may be additional sites of occurrence (7). Cases of visceral vein LMSs also exist,
however, those derived from the splenic vein are exceedingly rare
with only a few previously documented cases (1,2,8).
Venous LMSs predominately occur in middle-aged women
in the fifth and sixth decades of life, and usually arise from the
inferior vena cava or large veins in the lower extremities
(4). Clinical manifestations depend
on the tumor position in the vessel wall, venous obstruction and
compression of the surrounding organs by the mass, including
palpable abdominal masses and symptoms associated with thrombosis
or embolism of the splenic vein, such as abdominal pain, nausea and
fever (9,10). Sarcomas of the great vessels are
classified into luminal and mural tumors according to their site of
origin (5). Luminal sarcomas of the
blood vessels are more common in arteries than veins and they are
characterized by rapid growth and the earlier onset of distant
metastases due to intraluminal growth (5,11). By
contrast, mural sarcomas of the blood vessels are more common in
veins, and unlike luminal sarcomas, they have more positive
prognosis due to their slow and extraluminal growth (11). With regard to treatment, the majority
of soft-tissue sarcomas undergo surgical resection for localized
primary tumors; therefore resection offers the only opportunity for
complete cure in the absence of disseminated disease. Additionally,
tumor extent and histological examination to determine
classification and grade is also important in guiding adjunct
treatment.
Radiotherapy has been considered for the treatment
of high-grade soft tissue sarcomas located in the extremities,
intermediate-grade tumors of the limbs with close or positive
histological margins and as a treatment for recurring low-grade
sarcomas. Chemotherapy may be administered when systemic control is
the primary therapeutic aim, however, the sensitivity of sarcomas,
including LMSs, to chemotherapy appears to be poor (12). Therefore, as a form of adjuvant
treatment for LMS, chemotherapy does not produce an evident
increase in patient survival (12).
There is a limited amount of evidence demonstrating increased
survival following adjuvant radiation, combination radiation and
chemotherapy, in addition to surgical resection. However, whether
these treatment modalities should be incorporated in the general
treatment of LMS is still being debated.
The current study describes a case of LMS derived
from the splenic vein with concurrent liver metastasis.
Histopathological examination confirmed the lesions to be
intermediate-grade LMSs. An association between the masses in the
spleen, splenic hilum and splenic vein was confirmed; however, the
distal pancreas parenchyma did not appear to be involved. The
patient underwent splenic pedicle tumor resection, splenectomy and
liver tumor resection with no postoperative complications. Further
information regarding patient prognosis is unavailable, as the
patient did not undergo further adjuvant therapy or follow-up. LMSs
of splenic vein origin are extremely rare; therefore, unique
treatment recommendations or outcome data for such lesions has not
been established. General management principles should follow
established guidelines for other vascular LMSs and LMSs in
general.
In conclusion, LMS of the splenic vein is extremely
rare, and occurs predominantly in middle-aged individuals. There
have not been enough documented cases to establish optimum
treatment guidelines to improve patient prognosis in the short- and
long-term. Therefore, the aforementioned case may enable
practitioners to avoid the misdiagnosis of such patients in the
future.
References
|
1
|
Niver BE, Megibowa AJ, Faust MJ and
Rosenkrantz AB: Multidetector CT appearance of leiomyosarcoma of
the splenic vein. Clin Radiol. 66:688–690. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Gage MJ, Newman E, Maldonado TS and Hajdu
CH: Leiomyosarcoma of the splenic vein. J Vasc Surg. 55:1485–1487.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Weiss SW and Goldblum JR:
LeiomyosarcomaEnzinger and Weiss's Soft Tissue Tumors. 4th. Mosby;
St. Louis, MO: 2001
|
|
4
|
Tilkorn DJ, Hauser J, Ring A, Goertz O,
Stricker I, Steinau HU and Kuhnen C: Leiomyosarcoma of
intravascular origin-a rare tumor entity: Clinical pathological
study of twelve cases. World J Surg Oncol. 8:1032010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Burke AP and Virmani R: Sarcomas of the
great vessels. A clinicopathologic study. Cancer. 71:1761–1773.
1993.
|
|
6
|
Hines OJ, Nelson S, Quinones-Baldrich WJ
and Eilber FR: Leiomyosarcoma of the inferior vena cava: Prognosis
and comparison with leiomyosarcoma of other anatomic sites. Cancer.
85:1077–1083. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Killoran TP, Wells WA, Barth RJ and
Goodwin DW: Leiomyosarcoma of the popliteal vein. Skeletal Radiol.
32:174–178. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fletcher CDM: Diagnostic Histopathology of
Tumors. 3rd. Churchill Livingstone Elsevier; Philadelphia, PA:
2007
|
|
9
|
Tilkorn DJ, Lehnhardt M, Hauser J,
Daigeler A, Hebebrand D, Mentzel T, Steinau HU and Kuhnen C:
Intravascular leiomyosarcoma of the brachiocephalic region-report
of an unusual tumour localisation: Case report and review of the
literature. World J Surg Oncol. 6:1132008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Subramaniam MM, Martinez-Rodriguez M,
Navarro S, Rosaleny JG and Bosch AL: Primary intravascular myxoid
leiomyosarcoma of the femoral vein presenting clinically as deep
vein thrombosis: A case report. Virchows Arch. 450:235–237. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Székely E, Kulka J, Miklós I and Kaliszky
P: Leiomyosarcomas of great vessels. Pathol Oncol Res. 6:233–236.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Clark MA, Fisher C, Judson I and Thomas
JM: Soft-tissue sarcomas in adults. N Engl J Med. 353:701–711.
2005. View Article : Google Scholar : PubMed/NCBI
|