Lung cancer was the most lethal type of malignant
tumor amongst humans in the global cancer statistics of 2012
(1). By morphological type, lung
cancer is primarily divided into small cell lung cancer (SCLC) and
non-SCLC (NSCLC) (2). Lung cancer
cells are sensitive to radiotherapy, and thoracic radiotherapy can
eradicate chemotherapy-resistant tumor cells (3,4). A
retrospective study demonstrated that clinical outcomes following
stereotactic body radiotherapy are equal or superior to surgery
alone for overall survival in patients with stage I–II NSCLC
(3). Two meta-analyses have indicated
a statistically significant advantage with respect to overall
survival associated with limited-disease SCLC following
radiotherapy (5,6). However, radiation-induced pulmonary
injury, local recurrence and distant metastasis have become
substantial challenges to the successful management of lung cancer
(7).
Due to its non-specificity, radiation kills rapidly
mitosing cells, irrespective of whether they are cancerous or
normal, resulting in damage to tissues that have an increased
turnover rate, including skin, lung, bone marrow and gut epithelium
(8). At present, the prognostic
factors of lung cancer therapy are widely studied (9–12). A prior
study revealed that the DiAcSpm/cutoff ratio (DASr) is
significantly increased in NSCLC, and the DASr was revealed to be
an independent negative prognostic indicator in patients with NSCLC
who underwent complete resection (13). The overexpression of SRY-box 2 may
serve as a positive prognostic factor in patients with stage III
squamous cell lung cancer receiving adjuvant radiotherapy (14). Although understanding of the molecular
mechanisms underlying the development of normal lung tissue injury
and tumor tissue response in radiotherapy has improved,
transforming growth factor β1 (TGFB1) is the most important factor
among the numerous cytokines and growth factors that contribute to
the radiation-induced injury process (15). The present study reviewed the function
of TGFB1 in radiation-induced pulmonary injury and lung cancer
response to radiotherapy, aiming to discuss the clinical use of
this cytokine in lung cancer radiotherapy.
The TGFB family is a group of pleiotropic growth
factors that activate signal transduction cascades that serve
important functions in carcinogenesis and tumor progression
(16). TGFB1, a ligand of the TGFB
signaling pathway, is present in numerous cell types. TGFB1 is most
highly concentrated in healing wounds, where it is released in
large quantities from platelets (17). TGFB1 then recruits monocytes and
macrophages to the injury site (18),
inhibits epithelial cell proliferation and enhances fibroblast
maturation into post-mitotic fibrocytes that increase fibrous
tissue production (19,20), thereby accelerating angiogenesis and
extracellular matrix formation (21–23). In
cancer cells, TGFB1 serves a dual role. Initially, it functions as
a tumor suppressor by inhibiting cell growth and inducing apoptosis
(24). However, during the later
stages of tumor development, TGFB1 functions as a tumor promoter by
inducing the epithelial-mesenchymal transition (EMT) in cancer
cells, resulting in increased invasion and metastasis (24,25).
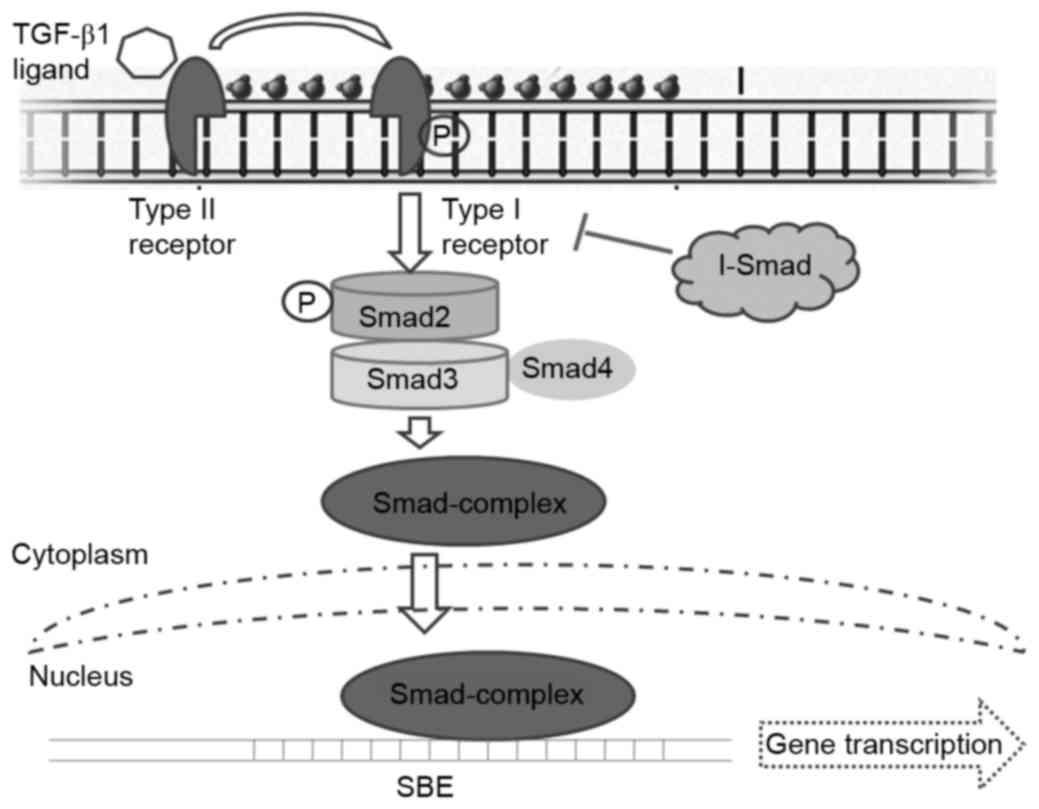
The signal transduction initiates with the TGFB1
ligand binding to and activating TGFB receptor II (TGFBRII), which
then phosphorylates TGFBRI through activating its kinase.
Phosphorylated TGFBRI phosphorylates the downstream elements of the
signaling pathway via the regulatory SMADs (R-SMADs) SMAD2 and
SMAD3, in the C-terminus of these R-SMADs. Phosphorylated SMAD2 may
form a stable complex with SMAD3 and the co-SMAD SMAD4 and the
resulting SMAD complex is then translocated into the nucleus
(Fig. 1). This SMAD complex interacts
with multiple transcription factors, which further increases their
binding affinity and specificity for the target gene promoters,
resulting in gene transcription alterations (24,25).
Inhibitory SMAD may bind TGFBRI and attenuate signaling pathway
activation (26). TGFB1 may also
signal via multiple alternative cascades, including the
mitogen-activated protein kinase and protein kinase B signaling
pathways (27,28), which may further mediate growth by
inhibiting cell cycle progression and inducing apoptosis (27).
Radiotherapy is the primary treatment for patients
with inoperable, locally advanced lung cancer. This conventional
treatment has been reported to induce remission in and cure
patients with the disease (29).
However, with conformal treatment planning, the side effects can
prove lethal and radiotherapy may be ineffective due to the
limitations imposed by normal tissue. This is particularly true in
tumors that require increased doses of radiation or are located
within or adjacent to sensitive organs (30). RP is considered the most serious,
dose-limiting complication of radiotherapy (30). Growth factors are synthesized and
secreted between a few h and days following irradiation, and may
then continue for months. Cytokine plasma levels, including those
of tumor necrosis factor, interleukin (IL)-1β, IL-6, and TGFB1
serve a predictive function for RP; the influence of tumor-derived
cytokine production on circulating plasma levels in irradiated
patients with NSCLC was evaluated in a previous study (30). The expression of TGFB1 increased in a
dose-dependent manner following exposure to ionizing radiation
(31). TGFB1 was reported as one of
the most important growth factors among the molecules expressed in
tissues following radiation exposure, and is associated with the
incidence of RP (32). Multiple
studies have established the positive association between the
severity of radiation-induced lung injury and TGFB1 signaling
activation (33,34). In a rat model of radiation-induced
lung injury, fibrosis developed and was accompanied by increased
expression of TGFB1 and activation of the TGFB1 signaling pathway
(35). Furthermore, TGFB1 activation
by radiation has been demonstrated to occur at decreased doses and
in an approximately dose-dependent manner between 10 cGy and 5 Gy
(36). Serially measuring plasma
TGFB1 levels has been proposed to estimate the risk of RP and to
assist in determining whether additional dose escalation may be
safely applied in chemotherapy (37,38).
Anscher et al (38) assessed
whether TGFB1 may also be used to predict the risk of developing
pulmonary injury following radiotherapy. Anscher et al
(39) performed a small clinical
trial and determined that it was feasible to use TGFB1 to guide
radiation dose selection for patients with lung cancer.
Furthermore, the expression of TGFB1 in the sputum was reported to
be a factor for predicting RP (40).
TGFB1 may be expressed in the sputum of patients with lung cancer,
in whom macrophages are the main sources of TGFB1 expression
(40). Patients with increased TGFB1
expression in the sputum following radiotherapy were associated
with an increased incidence of RP compared with those with
decreased TGFB1 expression (40). All
the aforementioned approaches resulted in decreased expression and
activation of TGFB1 and decreased activation of the SMAD-dependent
TGFB1 signaling pathway (37–40). The observations of Anscher et
al (38,39) suggests that plasma TGFB1 measurements
may assist in identifying whether patients with lung cancer are
candidates for radiation dose escalation or decrease. A previous
study also revealed that the serum expression of TGFB1 increased
significantly four weeks, and reached the highest recorded level
eight weeks, following irradiation in a rat model (41). Furthermore, downregulating TGFB1
protected against radiation-induced lung injury in the rat model
(41).
Meanwhile, circulating TGFB1 levels in lung cancer
patients are elevated compared with people without cancer (42). The reason for the higher levels of
TGFB1 appears to be associated with greater production and altered
bioavailability of this cytokine (43). The mannose-6-phosphate/insulin-like
growth factor receptor type II (M6P/IGF2R) was reported to serve a
crucial function in these feedback process (44). Kong et al (45) demonstrated that if patients with lung
cancer exhibited a loss of heterozygosity in M6P/IGF2R, they were
significantly more likely to exhibit increased plasma TGFB1 levels
and to develop radiation-induced lung injury compared with those
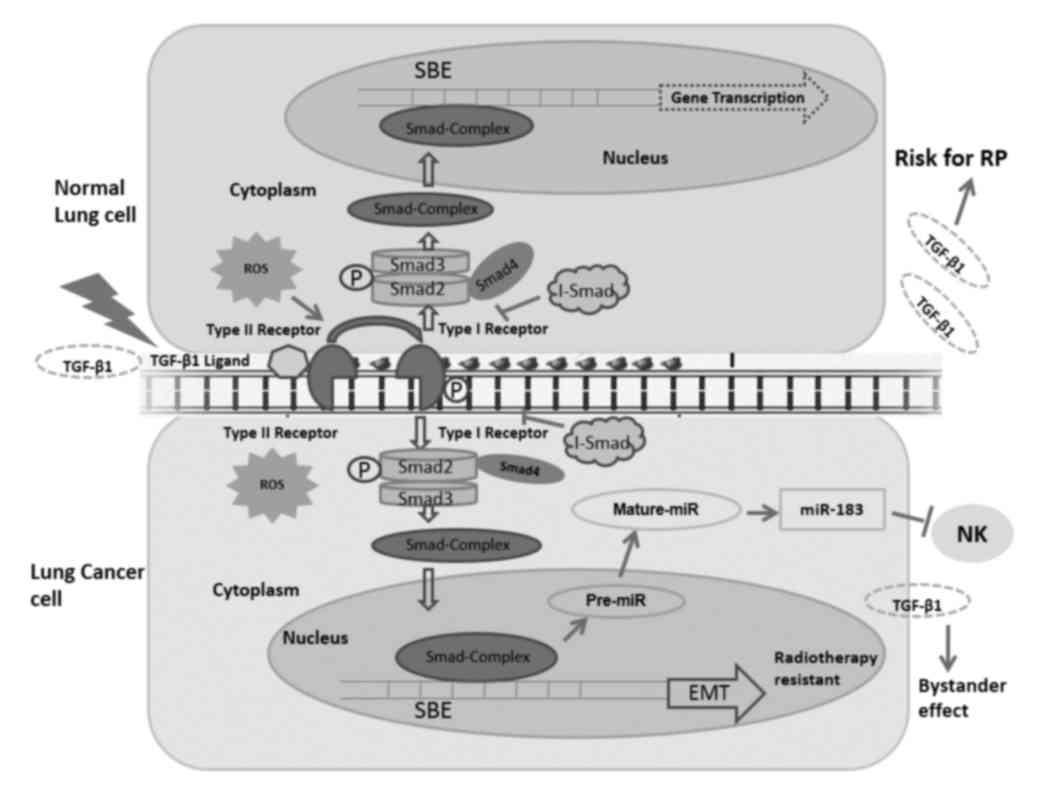
with heterozygosity in M6P/IGF2R. Reactive oxygen species (ROS) are
produced following radiation exposure (46), and have been revealed to activate
latent TGFB1 expression (Fig. 2)
(47). Mice genetically engineered to
overexpress one of the isoforms of superoxide dismutase have been
demonstrated to resist radiation-induced lung injury (48). Similarly, the administration of
superoxide dismutase mimetic has been revealed to decrease the
severity of lung injury in rats, in vivo (49).
However, the results of using TGFB1 levels to
predict the risk of lung injury have been inconsistent among
studies (50). A previous study
reported that the return of plasma TGFB1 levels to the normal range
following radiotherapy accurately predicted that patients would not
develop RP (38). Another study
failed to confirm that TGFB1 serves as a predictor of RP in lung
cancer radiotherapy (51). Jaeger
et al (37) did not confirm
that increased levels of TGFB1 following the end of radiotherapy
represented an independent additional risk factor for developing
symptomatic RP. Further study revealed that CT/CC genotypes of the
TGFB1 rs1982073:T869C gene were associated with a decreased risk of
RP in patients with lung cancer treated with definitive
radiotherapy compared with the other genotypes, and therefore may
serve as reliable predictors of RP (52).
Multiple studies have demonstrated that increased
serum levels of TGFB1 following the initiation of radiation therapy
were associated with radiation-induced lung injury, as
aforementioned (32–34). Changes in circulating TGFB1 levels
during radiation therapy may also be associated with the prognosis
of patients with locally advanced NSCLC (53). In locally advanced NSCLC, decreased
expression of TGFB1 during radiotherapy is associated with a more
favorable prognosis (54).
Radiation may trigger the synthesis and secretion of
TGFB1, and the activation of the intracellular TGFB signaling
pathway, as evidenced by the phosphorylation of SMAD and
transcriptional activation of a TGFB-responsive reporter gene in
lung cancer cells (54). Radiation
induced cells to increase their migration in response to
recombinant TGFB1, and this was accompanied by the upregulation of
TGFBR expression (54). An increasing
slope of the dose-response curve was associated with the C-509T
single nucleotide polymorphism, suggesting that a polymorphism
within the promoter region of the TGFB1 gene is associated with
radiation sensitivity (55). Breast
cancer cells pre-treated with the TGFB1 small molecule inhibitor
LY364947 were radiosensitized, irrespective of sensitivity to
TGFB1-induced growth inhibition (56). Consistent with increased clonogenic
cell death, DNA damage was significantly decreased in breast cancer
cells pretreated in vitro or in vivo with a TGFBRI
kinase inhibitor (56). Furthermore,
TGFB1-neutralizing antibodies increased radiation sensitivity and
significantly delayed tumor growth in response to single and
fractionated radiation exposure (56). These results suggest that inhibiting
TGFB1 activity prior to radiation attenuates the DNA damage
response and increases the radiosensitivity of breast cancer cells
(56). However, whether TGFB1 may
serve as an effective sensitizer in lung cancer radiotherapy has
not yet been reported.
The signaling pathway induced by TGFB1 serves an
important function in lung cancer cell growth and differentiation,
and this pathway is associated with a significant predictive value
in lung cancer radiotherapy. The present study further reviewed
reports on TGFB1-associated microRNAs (miRNA/miR) and the
mechanisms underlying EMT in lung cancer radiotherapy.
Multiple studies have demonstrated that miRNAs are
associated with cancer development, invasion and metastasis
(57,58), suggesting they may serve a function in
lung cancer treatment. Previously, SMAD proteins of the TGFB1
signaling pathway were revealed to regulate miRNA expression
through transcriptional and post-transcriptional mechanisms
(25). Animal studies with transgenic
mouse models supported the conclusion that activating TGFB1
increased the incidence of lung metastases from breast cancer
(59), whereas blocking TGFB1
activity decreased metastatic potential (60). An in vitro study demonstrated
that the TGFB1-miR-21-ROS signaling pathway in bystander cells was
critical for bystander responses to manifest in NSCLC (Fig. 2) (61).
Jiang et al (61) demonstrated
that when NSCLC cells were irradiated with 5 Gy X-rays, the TGFB1
signaling pathway was activated and the cells released certain
signaling molecules, including TGFB1, into the surrounding medium.
These signaling molecules diffused to bystander cells and activated
the TGFB1-miR-21-ROS signaling pathway in these bystander cells
(61). A prior study also revealed
that TGFB-induced miR-183 silenced tumor-associated natural killer
(NK) cells (Fig. 2) (62). However, the tumor cells evaded NK cell
surveillance by generating an immunosuppressive environment through
multiple factors, including TGFB1 (63). NK cells and cytotoxic T lymphocytes
exposed to TGFB1 did not kill tumor cells in humans or mice,
indicating that TGFB1 exhibited an immunosuppressive function
(64). Consequently, elevated serum
TGFB1 levels were associated with poorer prognosis, and observed in
the metastatic stage of numerous types of cancer (65). In vivo depletion of TGFB1 or
blockade of the TGFB1 signaling pathway may restore the NK
cell-mediated anti-tumor response.
To improve understanding of the dual
tumor-suppressive and tumor-promoting function of TGFB1 in cancer
cells, Gal et al (66)
assessed the response of mammary epithelial cancer cells to short
and long-term TGFB1 exposure. Cell proliferation was arrested and
apoptosis was induced following exposure to TGFB1 for 2–5 days,
whereas the surviving cells underwent EMT and became resistant to
proliferation arrest and apoptosis (66). EMT was reversed using a
pharmacological TGFBRI kinase inhibitor or by ceasing TGFB1
exposure. In addition, the downregulation of TGFB-dependent
signaling pathways in the transdifferentiated (TD) cells was
reversed, and proliferation arrest and apoptosis induced, upon
ceasing TGFB1 exposure (66). This
previous study concluded that suppressing the anti-proliferative
TGFB1 signaling pathway in TD cells may permit TGFB-dependent
survival and EMT-enhancing signaling pathways to function to
stimulate proliferation, survival and EMT at low, but sufficient,
levels (66). Therefore, the TGFB1
signaling pathway may be modulated to facilitate switching from
tumor suppression to progression (66).
However, a major challenge in developing accurate
models of radiation-induced lung toxicity is inter-patient
variation in inherent radiation sensitivity. The predictive value
of TGFB1 in lung cancer radiotherapy and the mechanism underlying
how the activation of the TGFB1 signaling pathway during
radiotherapy contributes to metastasis, cancer stem cell formation
and resistance to therapy via EMT induction, require further
study.
Radiation oncologists have focused on tolerating
tissue injury by limiting the dose or volume of the normal tissue
receiving radiation (68,69). Although these dose-volume associations
have received attention to more precisely correlate dose, volume
and the risk for normal tissue injury, certain disadvantages that
may influence the risk of treatment-associated complications remain
(70). TGFB1 represents a target for
molecular therapies designed to prevent or inhibit normal tissue
injury following cancer radiotherapy (71). The evidence supporting the critical
function of TGFB1 in the development of normal tissue injury
following cancer therapy was aforementioned. The present study
further reviewed the strategies aimed at preventing normal tissue
injury and sensitizing tumor cells by targeting the TGFB1 signaling
pathway.
Due to the vast number of potential targets in the
TGFB1 signaling pathway, multiple approaches have been adopted
in vitro to prevent the binding of TGFB1 to its receptor,
including specific antibody-mediated neutralization of soluble
TGFB, or dominant-negative inhibition of TGFBRI and TGFBRII
(71,72). The TGFB-specific approaches inhibited
radiation-dependent TGFB1 secretion, the phosphorylation of SMAD
and reporter gene activity, indicating that autocrine production of
TGFB and the subsequent activation of TGFB1 induced these changes
(54). After administering a single
dose of 1.0 mg/kg anti-TGFB1 antibody, delivered with the final
fraction of the right hemithorax irradiation, to Fischer rats,
Anscher et al (72)
demonstrated that, compared with in the rats receiving radiation
alone, inhibited fibrosis, TGFB1 expression and TGFB1-induced
signaling were observed in the rats treated with a combination of
radiation and an anti-TGFB1 antibody. A TGFBRI inhibitor was also
administered daily to a group of Sprague-Dawley rats with
irradiated right lungs (72). The
drug was administered from 7 days prior to irradiation until
sacrifice, or for 3 weeks. There was significantly decreased
fibrosis, TGFB1 expression and chronic oxidative stress in the
treated irradiated group as compared with in the untreated
irradiated group (72).
A prior study indicated that the TGFB1 signaling
pathway may induce the overproduction of fibrous tissue in response
to radiation through SMAD-independent signaling pathways, including
the ABL proto-oncogene (ABL)1 signaling pathway (71). The drug imatinib, which inhibits the
ABL1 signaling pathway, was reported to inhibit the development of
pulmonary fibrosis in NIH-3T3 and AKR-2B MEFs and in mice models
(73). TGFB1 was also revealed to
signal via the Ras homolog family member D (RHOD)/Rho associated
coiled-coil containing protein kinase (ROCK) signaling pathway,
independent of the SMAD signal transduction cascade (74,75).
Targeting of the RHOD/ROCK signaling pathway has been revealed to
protect against radiation enteritis. In addition, administering
superoxide dismutase mimics has been revealed to decrease the
severity of lung injury in a Fisher-344 rat model (49). Radiation sensitized cells and further
upregulated the expression of TGFBRI and TGFBRII, resulting in an
increase in lung and pancreatic carcinoma cell migration via EMT
(54). Strategies for inhibiting EMT
and inhibitors of TGFBRI and TGFBRII should be taken into
consideration for minimizing radiotherapy side-effects in clinical
practice. Otherwise, deregulation of the TGFB1 signaling pathway
may be induced by oscillating miRNA levels, such as miR-183.
Therefore, the use of therapeutic agents that facilitate the TGFB1
signaling pathway and silence the expression of miR-183 may
represent a promising strategy for activating the immune system in
lung therapy (62). These types of
approach result in decreased activation of TGFB1 and the
SMAD-dependent TGFB1 signaling pathway, and inhibit ROS
production.
To conclude, information regarding multiple aspects
of the TGFB1 signaling pathway in carcinogenesis has increased over
the past years. TGFB1 is considered a critical cytokine in the
development of late normal tissue injury following lung cancer
radiotherapy (37–39). Monitoring TGFB1 in the plasma and
screening for TGFB1 polymorphisms may assist in identifying normal
tissue injury risk in patients with lung cancer (38,52,55).
Although the molecular mechanisms underlying the TGFB1 signaling
pathway and the SMAD effector complex have been previously
established (24,25), upstream regulators of the TGFB1
signaling pathway and the mechanisms by which they regulate the
components of the pathway as the tumor develops require further
study. Strategies targeting TGFB1 have been demonstrated to
decrease the severity of normal tissue injury in animal models
(41,76). However, determining how such
strategies may be effectively and safely applied in humans requires
further clinical assessment.
The present study was supported by Scientific
Program of Jiangsu Province (grant nos. BE2015631 and BK20151174),
Changzhou Scientific Program (grant nos. CJ20160015 and QN201503);
Changzhou Municipal Commission of Health and Family Planning (grant
nos. QN201604 and ZD201602) and Changzhou High Level Medical
Talents Training Project (2016CZLJ026).
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2015. CA Cancer J Clin. 65:5–29. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chang JY, Senan S, Paul MA, Mehran RJ,
Louie AV, Balter P, Groen HJ, McRae SE, Widder J, Feng L, et al:
Stereotactic ablative radiotherapy versus lobectomy for operable
stage I non-small-cell lung cancer: A pooled analysis of two
randomised trials. Lancet Oncol. 16:630–637. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Adamowicz K and Goszczynska-Matysiak E:
Combining systemic therapies with radiation in non small cell lung
cancer. Klin Onkol. 28:321–331. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pignon JP, Arriagada R, Ihde DC, Johnson
DH, Perry MC, Souhami RL, Brodin O, Joss RA, Kies MS, Lebeau B, et
al: A meta-analysis of thoracic radiotherapy for small-cell lung
cancer. N Engl J Med. 327:1618–1624. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Warde P and Payne D: Does thoracic
irradiation improve survival and local control in limited-stage
small-cell carcinoma of the lung? A meta-analysis. J Clin Oncol.
10:890–895. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wan L, Pantel K and Kang Y: Tumor
metastasis: Moving new biological insights into the clinic. Nat
Med. 19:1450–1464. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ma Y, Yang Y, Wang F, Wei Q and Qin H:
Hippo-YAP signaling pathway: A new paradigm for cancer therapy. Int
J Cancer. 137:2275–2286. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gazdar AF: Epidermal growth factor
receptor inhibition in lung cancer: The evolving role of
individualized therapy. Cancer Metastasis Rev. 29:37–48. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tang Y, Geng Y, Luo J, Shen W, Zhu W, Meng
C, Li M, Zhou X, Zhang S and Cao J: Downregulation of ubiquitin
inhibits the proliferation and radioresistance of non-small cell
lung cancer cells in vitro and in vivo. Sci Rep. 5:94762015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sridhar SS, Seymour L and Shepherd FA:
Inhibitors of epidermal-growth-factor receptors: A review of
clinical research with a focus on non-small-cell lung cancer.
Lancet Oncol. 4:397–406. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hirsch FR, Varella-Garcia M, Cappuzzo F,
McCoy J, Bemis L, Xavier AC, Dziadziuszko R, Gumerlock P, Chansky
K, West H, et al: Combination of EGFR gene copy number and protein
expression predicts outcome for advanced non-small-cell lung cancer
patients treated with gefitinib. Ann Oncol. 18:752–760. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Takahashi Y, Sakaguchi K, Horio H,
Hiramatsu K, Moriya S, Takahashi K and Kawakita M: Urinary N1,
N12-diacetylspermine is a non-invasive marker for the diagnosis and
prognosis of non-small-cell lung cancer. Br J Cancer.
113:1493–1501. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yoon HI, Park KH, Lee EJ, Keum KC, Lee CG,
Kim CH and Kim YB: Overexpression of SOX-2 is associated with
better overall survival in squamous cell lung cancer patients
treated with adjuvant radiotherapy. Cancer Res Treat. 48:473–482.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Anscher MS, Chen L, Rabbani Z, Kang S,
Larrier N, Huang H, Samulski TV, Dewhirst MW, Brizel DM, Folz RJ
and Vujaskovic Z: Recent progress in defining mechanisms and
potential targets for prevention of normal tissue injury after
radiation therapy. Int J Radiat Oncol Biol Phys. 62:255–259. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Blahna MT and Hata A: Smad-mediated
regulation of microRNA biosynthesis. FEBS Lett. 586:1906–1912.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Passaretti F, Tia M, D'Esposito V, De
Pascale M, Del Corso M, Sepulveres R, Liguoro D, Valentino R,
Beguinot F, Formisano P and Sammartino G: Growth-promoting action
and growth factor release by different platelet derivatives.
Platelets. 25:252–256. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ashcroft GS: Bidirectional regulation of
macrophage function by TGF-beta. Microbes Infect. 1:1275–1282.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Boyd FT and Massagué J: Transforming
growth factor-beta inhibition of epithelial cell proliferation
linked to the expression of a 53-kDa membrane receptor. J Biol
Chem. 264:2272–2278. 1989.PubMed/NCBI
|
|
20
|
Hakenjos L, Bamberg M and Rodemann HP:
TGF-beta1-mediated alterations of rat lung fibroblast
differentiation resulting in the radiation-induced fibrotic
phenotype. Int J Radiat Biol. 76:503–509. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fajardo LF, Prionas SD, Kwan HH, Kowalski
J and Allison AC: Transforming growth factor beta1 induces
angiogenesis in vivo with a threshold pattern. Lab Invest.
74:600–608. 1996.PubMed/NCBI
|
|
22
|
Phillips GD, Whitehead RA, Stone AM,
Ruebel MW, Goodkin ML and Knighton DR: Transforming growth factor
beta (TGF-B) stimulation of angiogenesis: An electron microscopic
study. J Submicrosc Cytol Pathol. 25:149–155. 1993.PubMed/NCBI
|
|
23
|
Roberts AB, McCune BK and Sporn MB:
TGF-beta: Regulation of extracellular matrix. Kidney Int.
41:557–559. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Heldin CH and Moustakas A: Role of Smads
in TGFβ signaling. Cell Tissue Res. 347:21–36. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Santos JI, Teixeira AL, Dias F, Gomes M,
Nogueira A, Assis J and Medeiros R: Restoring TGFβ1 pathway-related
microRNAs: Possible impact in metastatic prostate cancer
development. Tumor Biol. 35:6245–6253. 2014. View Article : Google Scholar
|
|
26
|
Bierie B and Moses HL: Transforming growth
factor beta (TGF-beta) and inflammation in cancer. Cytokine Growth
Factor Rev. 21:49–59. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Connolly EC, Freimuth J and Akhurst RJ:
Complexities of TGF-β targeted cancer therapy. Int J Biol Sci.
8:964–978. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Massagué J and Gomis RR: The logic of
TGFbeta signaling. FEBS Lett. 580:2811–2820. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Koh PK, Faivre-Finn C, Blackhall FH and De
Ruysscher D: Targeted agents in non-small cell lung cancer (NSCLC):
Clinical developments and rationale for the combination with
thoracic radiotherapy. Cancer Treat Rev. 38:626–640. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Rube CE, Palm J, Erren M, Fleckenstein J,
König J, Remberger K and Rübe C: Cytokine plasma levels: Reliable
predictors for radiation pneumonitis? PLoS One. 3:e28982008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Anscher MS, Crocker IR and Jirtle RL:
Transforming growth factor-beta 1 expression in irradiated liver.
Radiat Res. 122:77–85. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhang XJ, Sun JG, Sun J, Ming H, Wang XX,
Wu L and Chen ZT: Prediction of radiation pneumonitis in lung
cancer patients: A systematic review. J Cancer Res Clin Oncol.
138:2103–2116. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Anscher MS, Marks LB, Shafman TD, Clough
R, Huang H, Tisch A, Munley M, Herndon JE, Garst J, Crawford J and
Jirtle RL: Risk of long-term complications after TFG-beta1-guided
very-high-dose thoracic radiotherapy. Int J Radiat Oncol Biol Phys.
56:988–995. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Novakova-Jiresova A, Van Gameren MM,
Coppes RP, Kampinga HH and Groen HJ: Transforming growth
factor-beta plasma dynamics and post-irradiation lung injury in
lung cancer patients. Radiother Oncol. 71:183–189. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chen L, Brizel DM, Rabbani ZN, Samulski
TV, Farrell CL, Larrier N, Anscher MS and Vujaskovic Z: The
protective effect of recombinant human keratinocyte growth factor
on radiation-induced pulmonary toxicity in rats. Int J Radiat Oncol
Biol Phys. 60:1520–1529. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Portess DI, Bauer G, Hill MA and O'Neill
P: Low-dose irradiation of nontransformed cells stimulates the
selective removal of precancerous cells via intercellular induction
of apoptosis. Cancer Res. 67:1246–1253. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
De Jaeger K, Seppenwoolde Y, Kampinga HH,
Boersma LJ, Belderbos JS and Lebesque JV: Significance of plasma
transforming growth factor-beta levels in radiotherapy for
non-small-cell lung cancer. Int J Radiat Oncol Biol Phys.
58:1378–1387. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Anscher MS, Kong FM, Andrews K, Clough R,
Marks LB, Bentel G and Jirtle RL: Plasma transforming growth factor
beta1 as a predictor of radiation pneumonitis. Int J Radiat Oncol
Biol Phys. 41:1029–1035. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Anscher MS, Marks LB, Shafman TD, Clough
R, Huang H, Tisch A, Munley M, Herndon JE II, Garst J, Crawford J
and Jirtle RL: Using plasma transforming growth factor beta-1
during radiotherapy to select patients for dose escalation. J Clin
Oncol. 19:3758–3765. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wang J, Qiao XY, Lu FH, Zhou ZG, Song YZ,
Huo JJ and Liu X: TGF-beta1 in serum and induced sputum for
predicting radiation pneumonitis in patients with non-small cell
lung cancer after radiotherapy. Chin J Cancer. 29:325–329. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lu Z, Ma Y, Zhang S, Liu F, Wan M and Luo
J: Transforming growth factor-β1 small interfering RNA inhibits
growth of human embryonic lung fibroblast HFL-I cells in vitro and
defends against radiation-induced lung injury in vivo. Mol Med Rep.
11:2055–2061. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Barthelemy-Brichant N, David JL, Bosquée
L, Bury T, Seidel L, Albert A, Bartsch P, Baugnet-Mahieu L and
Deneufbourg JM: Increased TGFbeta1 plasma level in patients with
lung cancer: Potential mechanisms. Eur J Clin Invest. 32:193–198.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Dennis PA and Rifkin DB: Cellular
activation of latent transforming growth factor beta requires
binding to the cation-independent mannose 6-phosphate/insulin-like
growth factor type II receptor. Proc Natl Acad Sci USA. 88:580–584.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Yang L, Tredget EE and Ghahary A:
Activation of latent transforming growth factor-beta1 is induced by
mannose 6-phosphate/insulin-like growth factor-II receptor. Wound
Repair Regen. 8:538–546. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kong FM, Anscher MS, Sporn TA, Washington
MK, Clough R, Barcellos-Hoff MH and Jirtle RL: Loss of
heterozygosity at the mannose 6-phosphate insulin-like growth
factor 2 receptor (M6P/IGF2R) locus predisposes patients to
radiation-induced lung injury. Int J Radiat Oncol Biol Phys.
49:35–41. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Riley PA: Free radicals in biology:
Oxidative stress and the effects of ionizing radiation. Int J
Radiat Biol. 65:27–33. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Barcellos-Hoff MH and Dix TA:
Redox-mediated activation of latent transforming growth factor-beta
1. Mol Endocrinol. 10:1077–1083. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Kang SK, Rabbani ZN, Folz RJ, Golson ML,
Huang H, Yu D, Samulski TS, Dewhirst MW, Anscher MS and Vujaskovic
Z: Overexpression of extracellular superoxide dismutase protects
mice from radiation-induced lung injury. Int J Radiat Oncol Biol
Phys. 57:1056–1066. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Vujaskovic Z, Batinic-Haberle I, Rabbani
ZN, Feng QF, Kang SK, Spasojevic I, Samulski TV, Fridovich I,
Dewhirst MW and Anscher MS: A small molecular weight catalytic
metalloporphyrin antioxidant with superoxide dismutase (SOD)
mimetic properties protects lungs from radiation-induced injury.
Free Radic Biol Med. 33:857–863. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Anscher MS, Kong FM, Marks LB, Bentel GC
and Jirtle RL: Changes in plasma transforming growth factor beta
during radiotherapy and the risk of symptomatic radiation-induced
pneumonitis. Int J Radiat Oncol Biol Phys. 37:253–258. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Barthelemy-Brichant N, Bosquée L, Cataldo
D, Corhay JL, Gustin M, Seidel L, Thiry A, Ghaye B, Nizet M, Albert
A, et al: Increased IL-6 and TGF-beta1 concentrations in
bronchoalveolar lavage fluid associated with thoracic radiotherapy.
Int J Radiat Oncol Biol Phys. 58:758–767. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Yuan X, Liao Z, Liu Z, Wang LE, Tucker SL,
Mao L, Wang XS, Martel M, Komaki R, Cox JD, et al: Single
nucleotide polymorphism at rs1982073:T869C of the TGFbeta 1 gene is
associated with the risk of radiation pneumonitis in patients with
non-small-cell lung cancer treated with definitive radiotherapy. J
Clin Oncol. 27:3370–3378. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Zhao L, Ji W, Zhang L, Ou G, Feng Q, Zhou
Z, Lei M, Yang W and Wang L: Changes of circulating transforming
growth factor-beta1 level during radiation therapy are correlated
with the prognosis of locally advanced non-small cell lung cancer.
J Thorac Oncol. 5:521–525. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Carl C, Flindt A, Hartmann J, Dahlke M,
Rades D, Dunst J, Lehnert H, Gieseler F and Ungefroren H: Ionizing
radiation induces a motile phenotype in human carcinoma cells in
vitro through hyperactivation of the TGF-beta signaling pathway.
Cell Mol Life Sci. 73:427–443. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kelsey CR, Jackson L, Langdon S, Owzar K,
Hubbs J, Vujaskovic Z, Das S and Marks LB: A polymorphism within
the promoter of the TGFβ1 gene is associated with radiation
sensitivity using an objective radiologic endpoint. Int J Radiat
Oncol Biol Phys. 82:e247–e255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Bouquet F, Pal A, Pilones KA, Demaria S,
Hann B, Akhurst RJ, Babb JS, Lonning SM, DeWyngaert JK, Formenti SC
and Barcellos-Hoff MH: TGFβ1 inhibition increases the
radiosensitivity of breast cancer cells in vitro and promotes tumor
control by radiation in vivo. Clin Cancer Res. 17:6754–6765. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Guz M, Rivero-Müller A, Okoń E,
Stenzel-Bembenek A, Polberg K, Słomka M and Stepulak A:
MicroRNAs-role in lung cancer. Dis Markers. 2014:2181692014.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Chan SH and Wang LH: Regulation of cancer
metastasis by microRNAs. J Biomed Sci. 22:92015. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Muraoka-Cook RS, Kurokawa H, Koh Y, Forbes
JT, Roebuck LR, Barcellos-Hoff MH, Moody SE, Chodosh LA and Arteaga
CL: Conditional overexpression of active transforming growth factor
beta1 in vivo accelerates metastases of transgenic mammary tumors.
Cancer Res. 64:9002–9011. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Muraoka RS, Dumont N, Ritter CA, Dugger
TC, Brantley DM, Chen J, Easterly E, Roebuck LR, Ryan S, Gotwals
PJ, et al: Blockade of TGF-beta inhibits mammary tumor cell
viability, migration, and metastases. J Clin Invest. 109:1551–1559.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Jiang Y, Chen X, Tian W, Yin X, Wang J and
Yang H: The role of TGF-β1-miR-21-ROS pathway in bystander
responses induced by irradiated non-small-cell lung cancer cells.
Br J Cancer. 111:772–780. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Donatelli SS, Zhou JM, Gilvary DL,
Eksioglu EA, Chen X, Cress WD, Haura EB, Schabath MB, Coppola D,
Wei S and Djeu JY: TGF-β-inducible microRNA-183 silences
tumor-associated natural killer cells. Proc Natl Acad Sci USA.
111:4203–4208. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Flavell RA, Sanjabi S, Wrzesinski SH and
Licona-Limón P: The polarization of immune cells in the tumor
environment by TGFbeta. Nat Rev Immunol. 10:554–567. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ikushima H and Miyazono K: TGFbeta
signalling: A complex web in cancer progression. Nat Rev Cancer.
10:415–424. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Gal A, Sjöblom T, Fedorova L, Imreh S,
Beug H and Moustakas A: Sustained TGF beta exposure suppresses Smad
and non-Smad signalling in mammary epithelial cells, leading to EMT
and inhibition of growth arrest and apoptosis. Oncogene.
27:1218–1230. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Shintani Y, Okimura A, Sato K, Nakagiri T,
Kadota Y, Inoue M, Sawabata N, Minami M, Ikeda N, Kawahara K, et
al: Epithelial to mesenchymal transition is a determinant of
sensitivity to chemoradiotherapy in non-small cell lung cancer. Ann
Thorac Surg. 92:1794–1804. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Mehta V: Radiation pneumonitis and
pulmonary fibrosis in non-small-cell lung cancer: Pulmonary
function, prediction, and prevention. Int J Radiat Oncol Biol Phys.
63:5–24. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Kong FM, Pan C, Eisbruch A and Ten Haken
RK: Physical models and simpler dosimetric descriptors of radiation
late toxicity. Semin Radiat Oncol. 17:108–120. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Milano MT, Constine LS and Okunieff P:
Normal tissue tolerance dose metrics for radiation therapy of major
organs. Semin Radiat Oncol. 17:131–140. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Anscher MS: Targeting the TGF-beta1
pathway to prevent normal tissue injury after cancer therapy.
Oncologist. 15:350–359. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Anscher MS, Thrasher B, Rabbani Z, Teicher
B and Vujaskovic Z: Antitransforming growth factor-beta antibody
1D11 ameliorates normal tissue damage caused by high-dose
radiation. Int J Radiat Oncol Biol Phys. 65:876–881. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Daniels CE, Wilkes MC, Edens M, Kottom TJ,
Murphy SJ, Limper AH and Leof EB: Imatinib mesylate inhibits the
profibrogenic activity of TGF-beta and prevents bleomycin-mediated
lung fibrosis. J Clin Invest. 114:1308–1316. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Haydont V, Mathé D, Bourgier C, Abdelali
J, Aigueperse J, Bourhis J and Vozenin-Brotons MC: Induction of
CTGF by TGF-beta1 in normal and radiation enteritis human smooth
muscle cells: Smad/Rho balance and therapeutic perspectives.
Radiother Oncol. 76:219–225. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Haydont V, Riser BL, Aigueperse J and
Vozenin-Brotons MC: Specific signals involved in the long-term
maintenance of radiation-induced fibrogenic differentiation: A role
for CCN2 and low concentration of TGF-beta1. Am J Physiol Cell
Physiol. 294:C1332–C1341. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Rabbani ZN, Anscher MS, Zhang X, Chen L,
Samulski TV, Li CY and Vujaskovic Z: Soluble TGFbeta type II
receptor gene therapy ameliorates acute radiation-induced pulmonary
injury in rats. Int J Radiat Oncol Biol Phys. 57:563–572. 2003.
View Article : Google Scholar : PubMed/NCBI
|