Introduction
Cholangiocarcinoma is the most common malignancy of
the bile duct epithelium (1). The
global incidence of cholangiocarcinoma has increased from 0.32 to
0.85 per 100,000 individuals within last 30 years, an increase of
165% (2). Cholangiocarcinoma has
become the second primary form of liver cancer after hepatocellular
carcinoma, accounting for 10–15% of total primary liver cancer
cases (3). However, the pathogenesis
of the majority cholangiocarcinoma cases remains unclear; various
high-risk factors have been associated with disease progression,
including parasitic infection, primary sclerosing cholangitis, bile
duct cysts, intrahepatic bile duct stones, toxins, inflammatory
enteropathy, hepatitis B or C virus infection, liver cirrhosis,
diabetes, obesity, alcohol consumption, tobacco and genetic
polymorphisms (4). Cholangiocarcinoma
is characterized by latency in its early stages, which contributes
to the challenges of diagnosis, high levels of malignancy and rapid
disease progression, leading to an unfavorable prognosis (5). Therefore, the identification of accurate
novel molecular biomarkers is of substantial importance for early
disease diagnosis, determination of the tumor differentiation stage
and the prediction of prognosis.
CHD1L is an oncogene that was identified and cloned
from the 1q21 chromosome region of human liver carcinoma cells in
1991. It has a full length of 2,980 bp, encoding an 89-kDa protein.
CHD1L was observed to exert critical functions in the
transcriptional regulation, chromosomal remodeling and protein-DNA
interaction manipulation (6). Ahel
et al (7) reported that CHD1L
participated in DNA damage repair, interacting with the DNA damage
site through an ATPase domain, dissociating from repaired DNA. The
ATPase domain may loosen chromatin via interaction with poly ADP
ribose to facilitate DNA repair. However, the overexpression of
CHD1L could reduce the degree of chromatin loosening in tumor
cells, which may result in the mismatch of DNA bases, potentially
initiating tumorigenesis (7). A
previous study determined that 58–78% of primary liver cancer cells
expressed CHD1L (8). Tian et
al (9) reported that CHD1L
overexpression was associated with poorer patient prognosis. CHD1L
was also detected in colorectal cancer tissue samples by Ji et
al (10): The overexpression of
CHD1L was associated with a large tumor size, deep tumor invasion
and a high histological. Functional studies revealed that
overexpression of CHD1L could promote the transfer of cells from
G1- to S-phase and inhibit apoptosis, these results indicating that
CHD1L serves notable roles in the pathogenesis of colorectal
cancer. Su et al (11),
evidenced by quantitative polymerase chain reaction (PCR) and
western blot analyses, revealed that CHD1L was highly expressed in
gastric cancer, and the overexpression of CHD1L was closely
associated with remote metastasis and an unfavorable patient
prognosis.
The DNA mismatch repair (MMR) system is activated
once DNA damage is detected, so the integrity and stability of DNA
can be maintained (12). The loss of
function for DNA MMR could occur upon mutation of a DNA MMR system
gene, leading to increased rates of DNA base pair mismatch and
activator mutations in proto-oncogenes, or the inactivation of
tumor suppressor genes, which eventually results in tumor
progression (12). hMLH1 is one of
the most important members of the DNA MMR system, identified by
Bronner et al (13) during
their investigation into hereditary non-polyposis colorectal cancer
(HNPCC). hMLH1 is located at the 3p21.3–23 chromosomal region and
encodes a 756 amino acid-long protein. The hMLH1 gene product was
observed to interact with the mismatched gene together with repair
enzymes, enhancing DNA repair (13).
The downregulation of hMLH1 (including mutation, methylation and
loss of heterozygosity) could lead to the loss of DNA MMR function
and promote tumor progress (13).
Zhang et al (14) reported
that 90% of HNPCC cases were closely associated with mutations to
hMLH1. The rate of hMLH1 loss was associated with the invasive
depth of colon cancer, as evidenced by Gu et al (15) in their study on 195 patients with
colon cancer. The latest research findings indicate that the
methylation status of the hMLH1 gene may be of significance for
evaluating the risk of recurrence in rectal cancer (16).
The objective of the present study was to
investigate CHD1L and hMLH1 expression in patients with
cholangiocarcinoma using immunohistological analysis; this was
evaluated along with the signs of clinical manifestation and
prognosis in order to evaluate their potential prognostic
value.
Materials and methods
Patients and clinicopathological
parameters
The present study was approved by the Ethics
Committee of The Second Affiliated Hospital of Nanchang University,
(Nanchang, China). The formalin-fixed (Specimens were fixed in 10%
formalin for 10 min at room temperature), 4-µm-thick
paraffin-embedded cholangiocarcinoma tissues were obtained from 108
patients who were admitted to The Second Affiliated Hospital of
Nanchang University (Nanchang, China) between the May 2005 and May
2014 [including 84 male and 24 female patients, with a mean age of
58.26 (range, 40–76 years)]. Normal bile duct tissues, collected 5
cm away from the tumor site, were obtained from 60 of the 108
patients. Written informed consent was provided by each
participant. The inclusion criteria for patients included a
diagnosis of cholangiocarcinoma prior to surgery, confirmed
postoperatively, and no preoperative chemotherapy and radiotherapy
administered. Patients with concurrent benign bile duct tumors or
hepatocellular carcinoma were excluded from the study. Data
regarding the clinicopathological parameters were also collected,
including age, gender, gallstone history, hepatitis B virus surface
antigen (HBsAg) presence, carbohydrate antigen 19-9 (CA19-9) serum
level, tumor diameter and Tumor-Node-Metastasis (TNM) stage
(Table I). TNM was assessed according
to the definitions of the American Joint Committee on Cancer
(AJCC), 7th edition (17).
 | Table I.Expression of CHD1L and hMLH1 and
their association with clinicopathological characteristics. |
Table I.
Expression of CHD1L and hMLH1 and
their association with clinicopathological characteristics.
|
|
| CHD1L | hMLH1 |
|---|
|
|
|
|
|
|---|
| Clinical
manifestation | Patients, n | Negative, n | Positive, n | P-value | Negative, n | Positive, n | P-value |
|---|
| Sex |
|
|
|
|
|
|
|
| Male | 84 | 6 | 78 | 0.178 | 12 | 72 | <0.001 |
|
Female | 24 | 0 | 24 |
| 12 | 12 |
|
| Age, years |
|
|
|
|
|
|
|
|
<60 | 78 | 6 | 72 | 0.118 | 12 | 66 | 0.006 |
| ≥60 | 30 | 0 | 30 |
| 12 | 18 |
|
| Gallstone
history |
|
|
|
|
|
|
|
| Yes | 48 | 6 | 42 | 0.005 | 6 | 42 | 0.300 |
| No | 60 | 0 | 60 |
| 18 | 42 |
|
| HBsAg |
|
|
|
|
|
|
|
|
Negative | 90 | 6 | 84 | 0.260 | 12 | 78 | <0.001 |
|
Positive | 18 | 0 | 18 |
| 12 | 6 |
|
| CA19-9, U/ml |
|
|
|
|
|
|
|
|
<400 | 30 | 6 | 24 | 0.000 | 12 | 18 | 0.006 |
| ≥400 | 78 | 0 | 78 |
| 12 | 66 |
|
| TNM stage |
|
|
|
|
|
|
|
| Stage
I | 36 | 0 | 36 | 0.000 | 12 | 24 | <0.001 |
| Stage
II | 24 | 0 | 24 |
| 0 | 24 |
|
| Stage
III | 24 | 6 | 18 |
| 12 | 12 |
|
| Stage
IV | 24 | 0 | 24 |
| 0 | 24 |
|
| Tumor diameter,
cm |
|
|
|
|
|
|
|
|
<4 | 72 | 6 | 66 | 0.075 | 12 | 60 | 0.050 |
| ≥4 | 36 | 0 | 36 |
| 12 | 24 |
|
Immunohistochemical analysis
The expression of CHD1L and hMLH1 in
cholangiocarcinoma and normal tissues was measured by using PV-9000
Two-Step Immunohistochemical Detection kit (Shanghai Ruiqi
Technology Co., Ltd., Shanghai, China).
Rabbit anti-human MLH1 polyclonal antibodies (cat.
no. 1167-1-AP; ProteinTech Group, Inc., Chicago, IL, USA; dilution,
1:100, 4°C overnight) and rabbit anti-human CHD1L polyclonal
antibodies (cat. no. PAB22069; Abnova, Taipei, Taiwan; dilution,
1:100, 4°C overnight) were used as primary antibodies, combined
with an immunohistochemical MaxVision™ kit (goat
anti-rabbit IgG polymer; cat. no. KIT-5006; dilution, 1:500; Fuzhou
Maixin Biotech Co. Ltd., Fuzhou, China), used according to the
protocol of the manufacturer, for the detection of MLH1 and CHD1L.
Primary antibodies were substituted with PBS for the negative
controls and healthy tissues were used for the positive controls.
The method of analysis was adapted from that of Plevová et
al (18). The immunohistochemical
staining was defined according to the stain intensity and number of
positive cells from randomly selected five vision fields (×200
magnification) under an inverted fluorescence microscopy (CKX41;
Olympus Corporation, Tokyo, Japan).
The number of positive cells were scored as follows:
0, no positive cells; 1, ≤25% of cells positive; 2, 26–50% positive
cells; 3, 51–75% positive cells; 4, >75% positive cells. The
staining intensity was scored as follows: 0, colorless; 1, light
yellow; 2, dark yellow; 4, brown. The final number was the sum of
the scores for the proportion of positive cells and the staining
intensity: 0–3, defined as (−); 4–5, defined as (+); 6–7 defined as
(++); (+) and (++) were regarded as positive results.
Statistical analysis
SPSS v.17.0 software (SPSS, Inc., Chicago, IL, USA)
was used to perform statistical analysis in the current study. The
data were analyzed using the χ2 test. The 3-year overall
survival rate was assessed using the Kaplan-Meier method, and the
inter-group comparisons were performed using the log-rank test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Expression of CHD1L in
cholangiocarcinoma
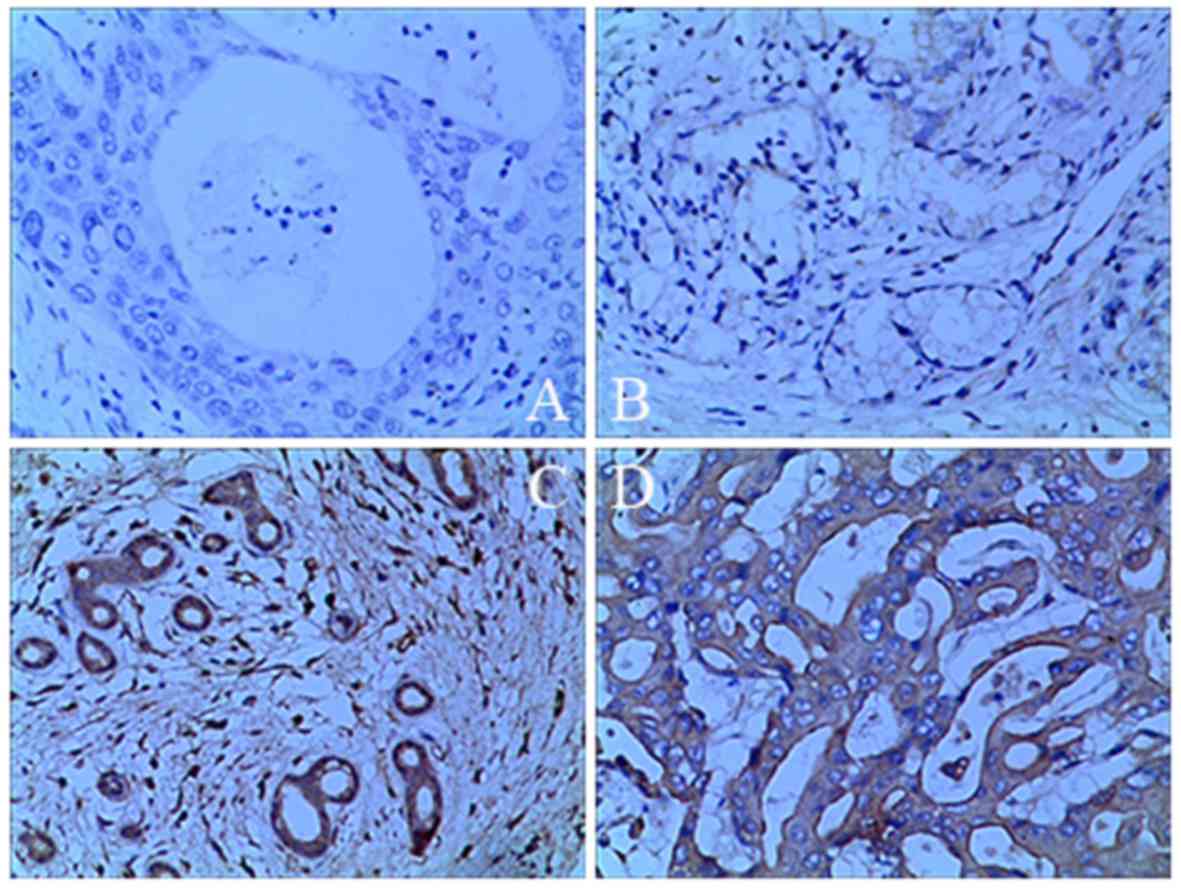
The rate of CHD1L expression was 94.44% (34/36) in
cholangiocarcinoma tissues, compared with only 40.00% (8/20) in
non-cancerous tissues, a statistically significant difference
(P<0.05; Table II; Fig. 1).
| Table II.Comparison of chromodomain
helicase/ATPase DNA binding protein 1 expression levels between
cholangiocarcinoma patients and healthy controls. |
Table II.
Comparison of chromodomain
helicase/ATPase DNA binding protein 1 expression levels between
cholangiocarcinoma patients and healthy controls.
| Group | Negative | Positive | Total | Positive rate,
% | P-value |
|---|
|
Cholangiocarcinoma | 6 | 102 | 108 | 94.44 | <0.001 |
| Normal tissue | 36 | 24 | 60 | 40.00 |
|
Association between the expression of
CHD1L or hMLH1 in cholangiocarcinoma and clinical
manifestations
The expression of CHD1L was significantly associated
with a history of gallstones, the serum CA19-9 level and TNM
staging (P<0.05). No significant association was determined to
be present with gender, age, the presence of HBsAg or the tumor
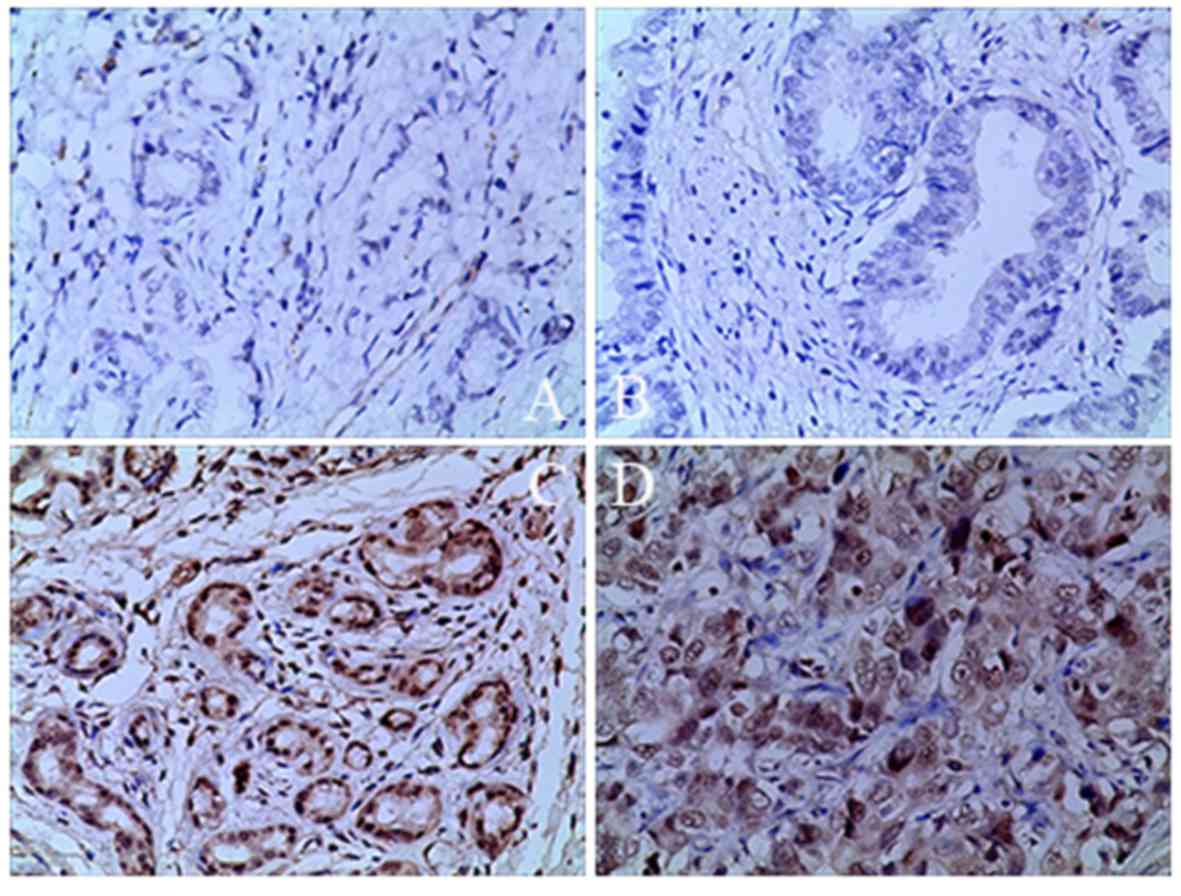
diameter (P>0.05). hMLH1 expression levels in cholangiocarcinoma
(28/36, 77.78%) were significantly lower than those in
non-cancerous bile duct tissues (58/60, 96.67%), as determined via
the aforementioned immunohistological analysis (Table III; Fig.
2). The expression of hMLH1 was significantly associated with
gender (P<0.001), age (P=0.006), serum CA19-9 level (P=0.006),
the presence of HBsAg (P<0.001), TNM staging and the tumor
diameter (P<0.05), but not with a history of gallstones
(P>0.05).
| Table III.Comparison of human mutL homolog 1
expression levels between cholangiocarcinoma patients and healthy
controls. |
Table III.
Comparison of human mutL homolog 1
expression levels between cholangiocarcinoma patients and healthy
controls.
| Group | Negative | Positive | Total | Positive rate,
% | P-value |
|---|
|
Cholangiocarcinoma | 24 | 84 | 108 | 77.78 | <0.01 |
| Normal tissue | 2 | 58 | 60 | 96.67 |
|
Survival analysis for the
CHD1L-positive and -negative groups, and the hMLH1-positive and
-negative groups
A total of 50 patients were randomly selected from
the 108 and were followed up for between 1 and 3 years. In total,
26/50 patients were lost during follow-up, and subsequently
excluded from the analysis. Of the remaining 24 patients, 18 were
CHD1L-positive and 6 were CHD1L-negative patients and 12 were
hMLH1-positive and 12 were hMLH1-negative patients. Of these 9/24
patients (37.5%) survived to the end of the follow-up period, of
whom 4 were CHD1L-positive and 5 were CHD1L-negative, 7 were
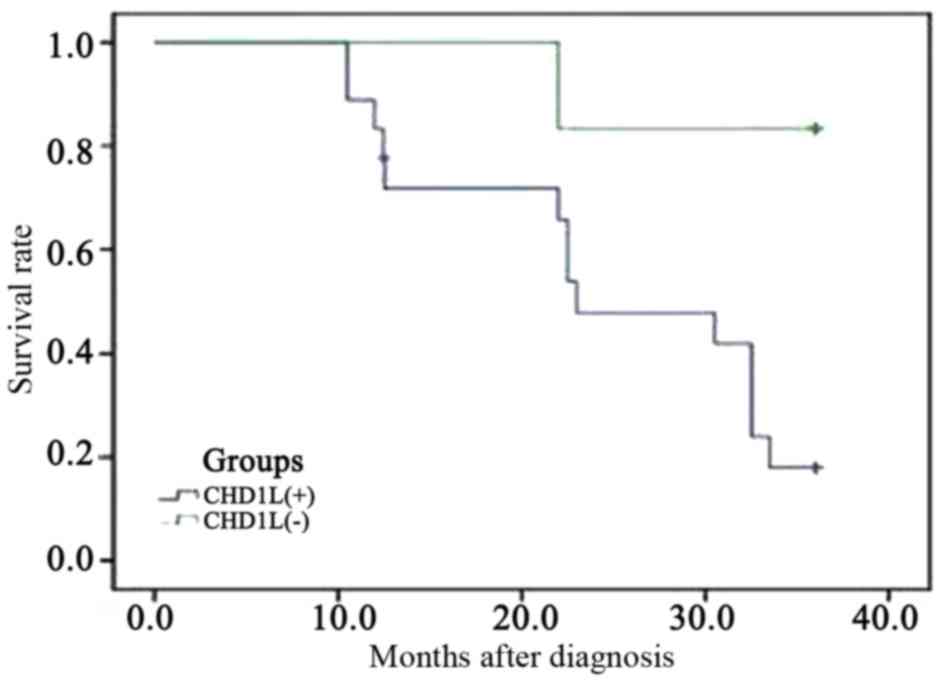
hMLH1-positive and 2 were hMLH1-negative. The Kaplan-Meier survival
curve indicated that the 3-year accumulative survival rate of
CHD1L-positive patients was 17.90%, which was significantly lower
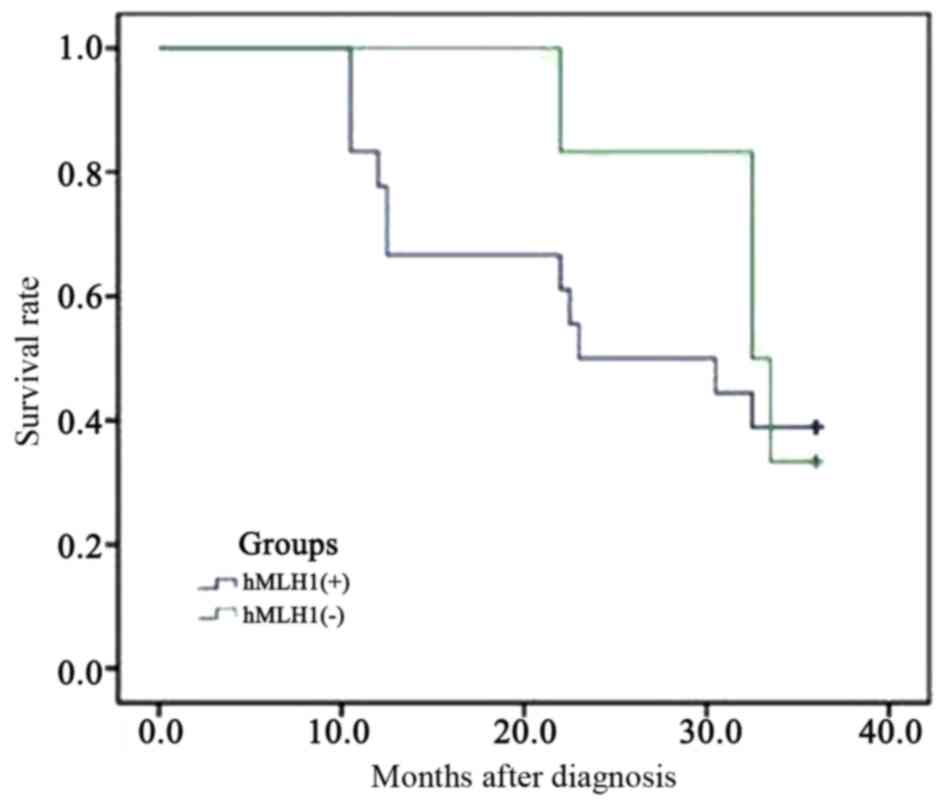
than for CHD1L-negative patients (83.33%; P<0.05; Fig. 3). Furthermore, the 3-year overall
survival rate of the hMLH1-positive patients was 38.90%, higher
than for the hMLH1-negative patients (33.30%), although this was
not a statistically significant difference (P>0.05; Fig. 4).
Discussion
The genesis and development of cholangiocarcinoma
are complicated processes with multiple steps and factors involved,
including oncogene activation and the loss of tumor suppressor
genes (19). Elucidation of the genes
essential for cholangiocarcinoma initiation and progression would
be of considerable value for disease diagnosis, prognosis and
identifying disease progression (1).
Recent studies have revealed that the expression levels of CHD1L
are high in cases of glioma (20) and
lung adenocarcinoma (21), and are
associated with tumor diagnosis, advanced clinical stage and
prognosis (22). In the current
study, the high expression levels of CHD1L in cholangiocarcinoma
and the low expression levels in non-cancerous tissues were
detected with immunohistochemical analysis. Further analysis
indicated that high expression of CHD1L was significantly
associated with gallstone history, CA19-9 level and TNM stage
(P<0.05), and negatively associated with the overall patient
survival rate.
According to a number of studies, hMLH1 was
expressed in multiple types of malignancies at relatively low
levels (23–26). Giedl et al (23) established that expression of hMLH1 was
decreased in early onset bladder cancer, as confirmed by
immunohistological analyses. Park et al (24) also obtained similar results using
samples of sporadic rectal cancer tissues collected from 318
patients. In addition, decreased expression of hMLH1 was detected
in primary non-small cell lung cancer cells using quantitative
polymerase chain reaction (25).
Through various immunohistochemical methods, Nam et al
(26) determined that the low
expression levels of hMLH1 in esophageal squamous cell carcinoma
cells are associated with patient prognosis.
In the current study, the expression of hMLH1 in
cholangiocarcinoma and non-cancerous tissues was assessed
immunohistochemically. The expression of hMLH1 was significantly
lower in cholangiocarcinoma tissues than in the adjacent normal
tissues. Further analysis of expression patterns combined with
clinicopathological characteristics including sex, age, gallstone
history, HBsAg, CA19-9, TNM stage and tumor diameter, revealed that
low expression levels of hMLH1 are significantly associated with
age, gender, CA19-9 level, the presence of HBsAg, the TNM stage and
tumor diameter. Kaplan-Meier survival curve analysis indicated that
patients with lower expression levels of hMLH1 had shorter overall
survival periods compared with patients with higher expression
levels of hMLH1, although this was not a significant difference.
However, the findings of the present study indicated that hMLH1
could be considered as a potential biomarker for prognosis of
cholangiocarcinoma.
In conclusion, the results of the present study
indicated that high expression levels of CHD1L and low expression
levels of hMLH1 are present in cholangiocarcinoma tissues, and that
their abnormal expression profile is closely associated with
disease development and an unfavorable prognosis. However, the
current study was retrospective, and further in vivo and
in vitro studies are required in order to investigate the
mechanisms by which CHD1L and hMLH1 are involved in the
pathological process and affect the tumor invasion and clinical
prognosis. Comprehensive research on CDH1L and hMLH1 could
contribute to the development of novel advanced methods for the
diagnosis and treatment of cholangiocarcinoma.
Acknowledgements
The authors would like to thank the Second
Affiliated Hospital of Nanchang University for assistance with the
experiments.
Funding
This work was supported by the Natural Science
Foundation of Jiangxi province, China (grant no. 20151512070090),
the Science and Technology Program of Health and Planning
Commission in Jiangxi Province (grant no. 20161048) and the
Graduate Innovation Fund for Nanchang University (grant no.
cx2015203).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
CH was responsible for the experimental design, the
funding application and the supervision and management of the
project. JH contributed to the execution of experiments, data
statistics, manuscript composition and submission. SL participated
in performing the experiment in the manuscript mapping, the
discussion and data interpretation. All authors have contributed to
and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Second Affiliated Hospital of Nanchang University,
(Nanchang, China). Written informed consent was provided by each
participant.
Patient consent for publication
Written informed consent was provided by each
participant for publication.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ghouri YA, Mian I and Blechacz B: Cancer
review: Cholangiocarcinoma. J Carcinog. 14:12015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wadsworth CA, Lim A, Taylor-Robinson SD
and Khan SA: The risk factors and diagnosis of cholangiocarcinoma.
Hepatol Int. 7:377–393. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Eckel F, Brunner T and Jelic S: ESMO
Guidelines Working Group: Biliary cancer: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Ann Oncol. 22
Suppl 6:vi40–vi44. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tyson GL and El-Serag HB: Risk factors for
cholangiocarcinoma. Hepatology. 54:173–184. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schweitzer N and Vogel A: Systemic therapy
of cholangiocarcinoma: From chemotherapy to targeted therapies.
Best Pract Res Clin Gastroenterol. 29:345–353. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen L, Chan TH, Yuan YF, Hu L, Huang J,
Ma S, Wang J, Dong SS, Tang KH, Xie D, et al: CHD1L promotes
hepatocellular carcinoma progression and metastasis in mice and is
associated with these processes in human patients. J Clin Invest.
120:1178–1191. 2010. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ahel D, Horejsí Z, Wiechens N, Polo SE,
Garcia-Wilson E, Ahel I, Flynn H, Skehel M, West SC, Jackson SP, et
al: Poly(ADP-ribose)-dependent regulation of DNA repair by the
chromatin remodeling enzyme ALC1. Science. 325:1240–1243. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
He WP, Zhou J, Cai MY, Xiao XS, Liao YJ,
Kung HF, Guan XY, Xie D and Yang GF: CHD1L protein is overexpressed
in human ovarian carcinomas and is a novel predictive biomarker for
patients survival. BMC Cancer. 12:4372012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tian F, Xu F, Zhang ZY, Ge JP, Wei ZF, Xu
XF and Cheng W: Expression of CHD1L in bladder cancer and its
influence on prognosis and survival. Tumour Biol. 34:3687–3690.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ji X, Li J, Zhu L, Cai J, Zhang J, Qu Y,
Zhang H, Liu B, Zhao R and Zhu Z: CHD1L promotes tumor progression
and predicts survival in colorectal carcinoma. J Surg Res.
185:84–91. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Su Z, Zhao J, Xian G, Geng W, Rong Z, Wu Y
and Qin C: CHD1L is a novel independent prognostic factor for
gastric cancer. Clin Transl Oncol. 16:702–707. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yan S, Sorrell M and Berman Z: Functional
interplay between ATM/ATR-mediated DNA damage response and DNA
repair pathways in oxidative stress. Cell Mol Life Sci.
71:3951–3967. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bronner CE, Baker SM, Morrison PT, Warren
G, Smith LG, Lescoe MK, Kane M, Earabino C, Lipford J, Lindblom A,
et al: Mutation in the DNA mismatch repair gene homologue hMLH1 is
associated with hereditary non-polyposis colon cancer. Nature.
368:258–261. 1994. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang R, Qin W, Xu GL, Zeng FF and Li CX:
A meta-analysis of the prevalence of somatic mutations in the hMLH1
and hMSH2 genes in colorectal cancer. Colorectal Dis. 14:e80–e89.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gu MJ, Bae YK, Kim A, Hong SM, Yu E, Kim
J, Jang KT, Chang HK, Jung ES, Bae HI, et al: Expression of hMLH1,
hMSH2 and hMSH6 in small intestinal carcinomas.
Hepatogastroenterology. 59:2228–2232. 2012.PubMed/NCBI
|
|
16
|
Kuan JC, Wu CC, Sun CA, Chu CM, Lin FG,
Hsu CH, Kan PC, Lin SC, Yang T and Chou YC: DNA methylation
combinations in adjacent normal colon tissue predict cancer
recurrence: Evidence from a clinical cohort study. PLoS One.
10:e01233962015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kamarajah SK, Burns WR, Frankel TL, Cho CS
and Nathan H: Validation of the American Joint Commission on Cancer
(AJCC) 8th Edition Staging System for Patients with Pancreatic
Adenocarcinoma: A Surveillance, Epidemiology and End Results (SEER)
Analysis. Ann Surg Oncol. 24:2023–2030. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Plevová P, Krepelová A, Papezová M,
Sedláková E, Curík R, Foretová L, Navrátilová M, Novotný J,
Zapletalová J, Palas J, et al: Immunohistochemical detection of the
hMLH1 and hMSH2 proteins in hereditary non-polyposis colon cancer
and sporadic colon cancer. Neoplasma. 51:275–284. 2004.PubMed/NCBI
|
|
19
|
Gil-García B and Baladrón V: The complex
role of NOTCH receptors and their ligands in the development of
hepatoblastoma, cholangiocarcinoma and hepatocellular carcinoma.
Biol Cell. 108:29–40. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sun J, Zhang L, Zhao H, Qiu X, Chen W,
Wang D, Ban N, Fan S, Shen C, Xia X, et al: CHD1L regulates cell
cycle, apoptosis, and migration in glioma. Cell Mol Neurobiol.
36:565–576. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
He LR, Ma NF, Chen JW, Li BK, Guan XY, Liu
MZ and Xie D: Overexpression of CHD1L is positively associated with
metastasis of lung adenocarcinoma and predicts patients poor
survival. Oncotarget. 6:31181–31190. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wu J, Zong Y, Fei X, Chen X, Huang O, He
J, Chen W, Li Y, Shen K and Zhu L: Presence of CHD1L
over-expression is associated with aggressive tumor biology and is
a novel prognostic biomarker for patient survival in human breast
cancer. PLoS One. 9:e986732014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Giedl J, Schneckenpointner R, Filbeck T,
Ruemmele P, Hofstaedter F, Burger M, Hartmann A and Stoehr R: Low
frequency of HNPCC-associated microsatellite instability and
aberrant MMR protein expression in early-onset bladder cancer. Am J
Clin Pathol. 142:634–639. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Park JW, Chang HJ, Park S, Kim BC, Kim DY,
Baek JY, Kim SY, Oh JH, Choi HS, Park SC and Jeong SY: Absence of
hMLH1 or hMSH2 expression as a stage-dependent prognostic factor in
sporadic colorectal cancers. Ann Surg Oncol. 17:2839–2846. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Vageli D, Daniil Z, Dahabreh J, Karagianni
E, Vamvakopoulou DN, Ioannou MG, Scarpinato K, Vamvakopoulos NC,
Gourgoulianis KI and Koukoulis GK: Phenotypic mismatch repair hMSH2
and hMLH1 gene expression profiles in primary non-small cell lung
carcinomas. Lung Cancer. 64:282–288. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nam TK, Lee JH, Cho SH, Chung IJ, Ahn SJ,
Song JY, Yoon MS, Chung WK and Nah BS: Low hMLH1 expression prior
to definitive chemoradiotherapy predicts poor prognosis in
esophageal squamous cell carcinoma. Cancer Lett. 260:109–117. 2008.
View Article : Google Scholar : PubMed/NCBI
|