Introduction
Prostate cancer (PCa), one of the malignant tumors
of the prostate gland, is frequently found in the lateral and
posterior lobes of the prostate as well as in the glands. It has a
high incidence in the middle-aged and elderly men. It ranks 3rd
among the highest incidence of male tumors. The mortality rate
ranks 6th, and there are also regional differences in incidence of
PCa. According to statistics, the global incidence and mortality
gap is approximately 25 times and 10 times, respectively (1–3). Another
study shows that (4), it is
speculated that by 2030 in China PCa incidence and mortality will
double on the existing basis, an average of >5% annual increase.
At present, the early diagnosis of PCa is mainly biopsy and serum
prostate specific antigen (PSA), but in the paracancerous benign
prostatic hyperplasia and prostatitis, the PSA expression will also
increase, indicating that PSA has a high sensitivity but poor
specificity, which may lead to some bias towards the diagnosis of
clinicians, and the presence of gray areas makes it not a good
indicator of the prognosis of patients (5,6). Thus, we
need to find a way to diagnose PCa, to reduce the clinical
misdiagnosis and missed diagnosis.
MicroRNAs (miRNAs) are a class of endogenous
non-coding single-stranded small molecule RNAs that regulate the
expression of target genes at the post-transcriptional level, and
are involved in the regulation of various physiological and
pathological functions (7).
Bioinformatics data show that a single miRNA can bind to hundreds
of target mRNAs, and thus play an important role in various
biological processes (8). There is
growing evidence that there is a link between miRNAs and
tumorigenesis. miR-29b and miR-30c are members of the miRNA family.
TCGA database indicated that miR-29b and miR-30c show low
expression in PCa cancer tissues.
Therefore, we explored the expression of miR-29b and
miR-30c in PCa tissue, in order to provide a basis for the
diagnosis and treatment of PCa.
Materials and methods
For this investigation cancer tissues and adjacent
tissues of 187 cases of PCa by prostatectomy were collected from
March 2011 to February 2013 in the Department of Urology of Jining
First People's Hospital (Jining, China). Samples were excised and
frozen in liquid nitrogen within 5 min for preservation. There was
a total of 187 male patients, aged from 47–65 years, mean age
52.05±8.47 years. Patients were divided according to the 7th
edition of TNM staging standard of 2009; PCa by Union for
International Cancer Control (UICC) (9): 55 cases in stage I, 60 cases in stage II
and 72 cases in stage III–IV. Pathological type of all specimens
obtained was PCa. Clinical specimens were collected with the
approval of Jining First People's Hospital Medical Ethics Committee
(Jining, China), and patients signed informed consent.
The main reagents
TRIzol reagent and miRNA reverse transcriptase kit
were purchased from Invitrogen company (Thermo Fisher Scientific,
Inc., Carlsbad, CA, USA); SYBR-Green Master Mix was purchased from
Applied Biosystems (Thermo Fisher Scientific, Inc.). ABI StepOne
Plus fluorescence quantitative PCR instrument was purchased from
Applied Biosystems. NanoDrop 2000 spectrophotometer, miR-29b and
miR-30c primer sequence were designed and synthesized by the
Shanghai Sangon Biological Engineering Co., Ltd. (Shanghai, China)
(Table I).
 | Table I.Primer sequences. |
Table I.
Primer sequences.
| Genes | Upstream
sequences | Downstream
sequences |
|---|
| U6 internal
reference |
5′-CTCGCTTCGGCAGCACA-3′ |
5′-AACGCTTCACGAATTTGCGT-3′ |
| miR-29b |
5′-GCGCGCTAGCACCATTTG-3′ |
5′-CAGTGCAGGGTCCGAGGT-3′ |
| miR-30c | 5′––3′ |
5′-AGATGAGCATTGGCAGCGAG-3′ |
Method
RT-qPCR assay
The collected PCa cancer tissue and PCa adjacent
tissues was performed with total RNA extraction by using TRIzol
reagent, in strict accordance with the instructions for extraction.
The concentration and purity of extracted RNA were detected by UV
spectrophotometer (Hitachi, Tokyo, Japan). The OD value of the
total RNA solution: A260/A280 ranged from 1.8–2.1, and if not, it
was extracted again. The integrity of RNA was detected by 1%
denaturing agarose gel electrophoresis. The total RNA was subjected
to reaction system disposition and reverse transcription to cDNA by
miRNA reverse transcription kit instructions (and stored at −20°C
for later use). ABI StepOne Plus fluorescence quantitative PCR
instrument was adopted, and the reaction system was according to
the instructions. Reaction conditions: 95°C for 5 min; 95°C for 45
sec; 60°C for 60 sec; 72°C for 45 sec and 45 cycles. U6 was used as
internal reference. The experiment was repeated 3 times, and the
results were analyzed by using the 2−ΔΔCq method
(10).
Statistical analysis
The study used SPSS 20.0 software package (Version
X; IBM, Armonk, NY, USA) to perform statistical analysis for all
the results collected. GraphPad Prism 5 software was adopted for
image rendering. The enumeration data are expressed as a percentage
(%). The Students t-test was used for comparisons between the two
groups. The measurement data are expressed as mean ± standard error
(SE), and the ROC curve of miR-29b and miR-30c was plotted.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Expression of miR-29b and miR-30c in
PCa tissues
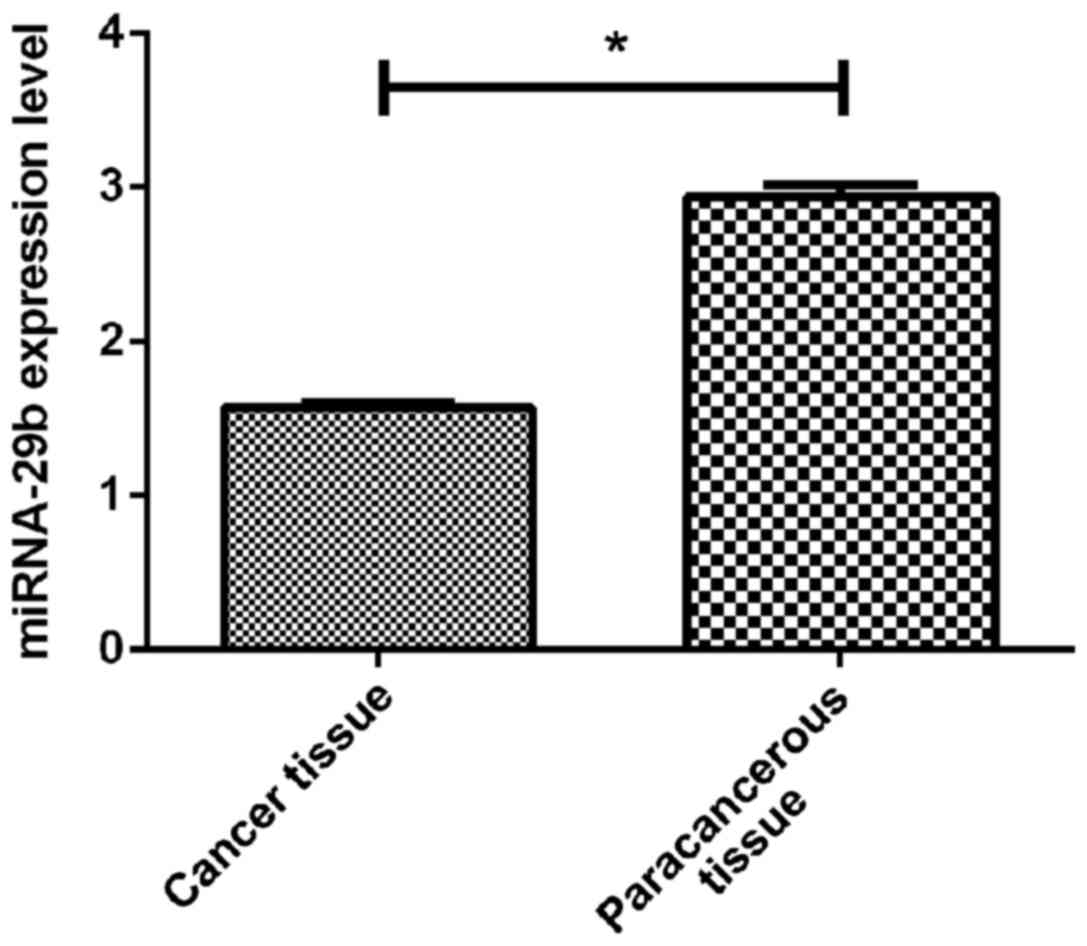
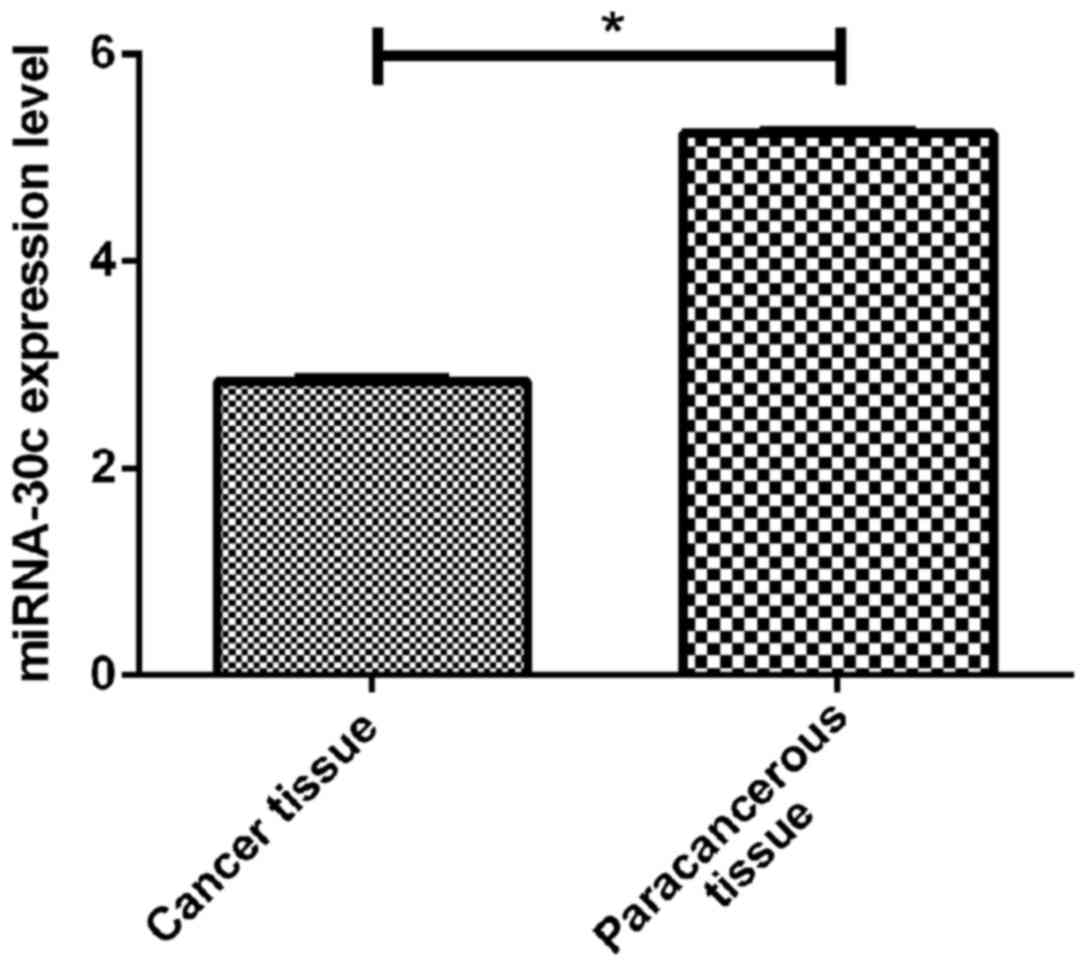
By RT-qPCR, we detected the expression of miR-29b in
cancer tissues of PCa and adjacent tissues. The results showed that
miR-29b was significantly lower in the PCa tissues (1.57±0.48) than
that in the paracancerous tissues (2.94±1.08) (p<0.05). However,
the expression of miR-30c was also lower in PCa patients
(2.84±0.57) than that in paracancerous tissues (5.24±0.42)
(p<0.05) (Figs. 1 and 2).
The relationship between the low
expression of miR-29b and miR-30c and clinicopathological features
in PCa patients
By comparing the expression of miR-29b and miR-30c
and clinical data in PCa patients with cancer, we found that there
was no correlation between age and smoking and TNM staging of
miR-29b and miR-30c (p>0.05), while lymph node metastasis, bone
metastasis, Gleason score were correlated with miR-29b and miR-30c
expression (p<0.01) (Table
II).
| Table II.Correlation of miR-29b and miR-30c low
expression and clinicopathological features of PCa patients. |
Table II.
Correlation of miR-29b and miR-30c low
expression and clinicopathological features of PCa patients.
| Clinical
features | n | miR-29b
expression | Statistics | P-value | miR-30c
expression | Statistics | P-value |
|---|
| Age (years) |
| ≥55 | 88 | 1.52±0.32 | 1.389 | 0.166 | 2.74±0.42 | 1.314 | 0.191 |
| <55 | 99 | 1.59±0.38 |
|
| 2.82±0.43 |
|
| Smoking |
| Yes | 180 | 1.42±0.59 | 0.133 | 0.894 | 2.54±0.38 | 0.948 | 0.344 |
| No | 7 | 1.45±0.36 |
|
| 2.68±0.47 |
|
|
| Lymph node
metastasis |
| Yes | 104 | 1.53±0.35 | 2.092 | 0.004 | 2.64±0.32 | 2.900 | 0.004 |
| No | 83 | 1.66±0.50 |
|
| 2.88±0.34 |
|
|
| Bone metastasis |
| Yes | 133 | 1.43±0.27 | 3.955 | 0.001 | 2.72±0.22 | 2.943 | 0.004 |
| No | 54 | 1.61±0.31 |
|
| 2.84±0.32 |
|
|
| TNM staging |
| I | 55 | 1.72±0.31 |
|
| 2.94±0.37 |
|
|
| II | 60 | 1.69±0.37 | 0.626 | 0.535 | 2.88±0.22 | 2.895 | 0.058 |
| III+IV | 72 | 1.66±0.22 |
|
| 2.82±0.24 |
|
|
| Gleason score |
| ≥8 | 107 | 1.33±0.20 | 3.642 | 0.004 | 2.44±0.29 | 3.315 | 0.001 |
| <8 | 80 | 1.44±0.21 |
|
| 2.60±0.37 |
|
|
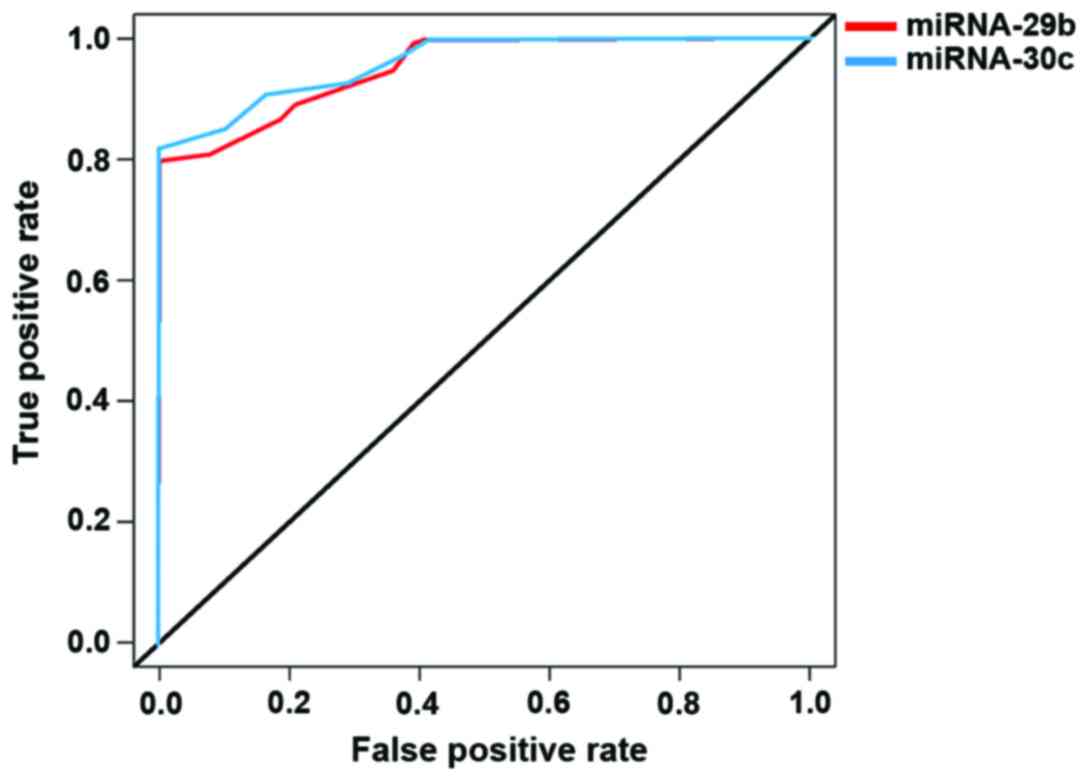
The clinical value of miR-29b and
miR-30c in the diagnosis of PCa
To compare the expression levels of miR-29b and
miR-30c in PCa patients with cancer tissues and adjacent tissues,
we plotted the ROC curve, which indicated that miR-29b, AUC was
0.924, and the 95% CI was 0.824–0.967; the specificity was 84.4%,
and the sensitivity was 76.5%; while for miR-30c, AUC was 0.944,
and 95% CI was 0.798–0.972; the specificity was 80.2%, and the
sensitivity was 72.3%. The two miRNAs were effective in
differentiating cancer tissues from paracancerous tissues with high
specificity and sensitivity (Fig.
3).
Discussion
As a malignant tumor that seriously affects the
quality of life of men, the pathogenesis and causes of PCa are
complicated (11). Studies have found
that the conditions of family heredity and environmental factors of
PCa patients can lead to the occurrence and development of PCa, and
the incidence in men under 50 is not high, but the incidence of PCa
after the age of 50 years increases exponentially (12). Another study shows that (13) if the early PCa is timely treated, the
prognosis will be better. PSA is widely used as a primary screening
tool for PCa in early clinical diagnosis. However, PSA specificity
is low; PSA increases in a variety of common prostatic diseases,
and there is also considerable controversy regarding whether PSA
testing can reduce PCa mortality. Therefore, we must find a more
suitable biomarker to improve the diagnosis of PCa, providing a
more reliable method for clinical treatment and diagnosis.
miRNAs are a class of endogenous, non-coding,
short-chain RNAs that degrade target genes and suppress translation
of target genes, thereby silencing a gene transcription (14). Studies have shown that nearly 30% of
the encoded proteins in the human body are influenced and regulated
by miRNAs (15). miRNAs are
differentially expressed in tumors, and can be repressed or
promoted by the regulation of target genes. It has been reported in
the literature (16–18) that the biological functions of miR-29b
and miR-30c have an important effect on the pathophysiological and
pathological changes of tumor cells, and play a regulatory role in
various functions such as proliferation, differentiation and
apoptosis of cancer cells.
In this study, we detected the expression levels of
miR-29b and miR-30c in 187 cases of PCa by RT-qPCR, and found that
the expression of miR-29b in cancer tissues was significantly lower
than that in adjacent non-cancerous tissues. Similarly, miR-30c
expression in cancer tissues was significantly lower than that in
paracancerous tissues. Through the correlation analysis of the two
miRNAs low expression and clinical records data, we found that
lymph node metastasis, bone metastasis, and Gleason score were
correlated with the expression of miR-29b and miR-30c, and by
plotting ROC cure of miR-29b and miR-30c resulted in miR-29b AUC,
0.924; 95% CI, 0.824–0.967, and miR-30c AUC, 0.944; and 95% CI,
0.798–0.972. This is a good illustration that both miRNAs have a
very good diagnostic value in the diagnosis of PCa. Forty-four
patients with PCa were detected by RT-qPCR by Huang et al
(19), they found that the cancerous
tissues of 44 PCa patients were significantly downregulated
compared with the results of our present experiment, there were
some differences but not significant, which may be caused by the
difference of the patient's area and the experimental design, and
the ROC curve plotted is basically the same as the ROC curve drawn
by us. In the study by Zhang et al (20), miR-30c was found to be highly
effective in inhibiting proliferation, migration and invasion of
PCa cells. In the study of Steele et al (21), miR-29b was found to have low
expression in PCa cells, and was significantly lower in PCa tissues
than that in adjacent non-cancerous tissues. It was also found that
N-cadherin, Twist and Snail protein expression was significantly
downregulated, which is also a good illustration that miR-29b and
miR-30c are potential biomarkers for the treatment and diagnosis of
PCa.
However, this study also has some shortcomings. Only
the expression of miRNAs in PCa tissues was examined, and did not
follow up the patients. In addition, the sample size was small.
Whether the regional differences would bias the experimental
results is not known. Therefore, we hope that in future trials, we
will increase the number of specimens, increase the control group
of cancer adjacent tissue group and follow up the patients promptly
in the hope of better verifying the correctness of this
investigation.
In summary, miR-29b and miR-30c play an important
role in the occurrence and development of PCa, which is expected to
become a novel marker for early diagnosis and prognosis of PCa.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
CZ drafted this manuscript. CZ and WW were
responsible for the conception and design of the study. XH
collected the patients data, and revised the manuscript critically
for important intellectual content. JZ and CJ analyzed and
interpreted the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Jining First People's Hospital (Jining, China). Signed written
informed consents were obtained from the patients or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wolff JM and Mason M: Drivers for change
in the management of prostate cancer - guidelines and new treatment
techniques. BJU Int. 109 Suppl 6:33–41. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sfanos KS, Yegnasubramanian S, Nelson WG
and De Marzo AM: The inflammatory microenvironment and microbiome
in prostate cancer development. Nat Rev Urol. 15:11–24. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kenfield SA, Tat D and Chan JM: The
potential benefits of diet and physical activity among active
surveillance patients with low-burden prostate cancer. In: Active
Surveillance for Localized Prostate CancerCurrent clinical urology.
Klotz L: Humana Press; Totowa, NJ: 2012
|
|
4
|
Baade PD, Youlden DR, Cramb SM, Dunn J and
Gardiner RA: Epidemiology of prostate cancer in the Asia-Pacific
region. Prostate Int. 1:47–58. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Esfahani M, Ataei N and Panjehpour M:
Biomarkers for evaluation of prostate cancer prognosis. Asian Pac J
Cancer Prev. 16:2601–2611. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Marantz PR, Hall CB and Derby CA: Radical
prostatectomy versus watchful waiting. N Engl J Med. 353:1298–1300.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Carthew RW: Gene regulation by microRNAs.
Curr Opin Genet Dev. 16:203–208. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Iorio MV and Croce CM: MicroRNA
dysregulation in cancer: Diagnostics, monitoring and therapeutics.
A comprehensive review. EMBO Mol Med. 4:143–159. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ferretti S, Patriarca S, Carbone A and
Zanetti R: TNM classification of malignant tumours, VII edition
2009. Changes and practical effects on cancer epidemiology.
Epidemiol Prev. 34:125–128. 2010.(In Italian). PubMed/NCBI
|
|
10
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
White A, Joseph D, Rim SH, Johnson CJ,
Coleman MP and Allemani C: Colon cancer survival in the United
States by race and stage (2001–2009): Findings from the CONCORD-2
study. Cancer. 123 Suppl 24:5014–5036. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Thorstenson A, Garmo H, Adolfsson J and
Bratt O: Cancer specific mortality in men diagnosed with prostate
cancer before age 50 years: A nationwide population based study. J
Urol. 197:61–66. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pokharel SS, Patel NU, Garg K, La Rosa FG,
Arangua P, Jones C and Crawford ED: Multi-parametric MRI findings
of transitional zone prostate cancers: Correlation with
3-dimensional transperineal mapping biopsy. Abdom Imaging.
40:143–150. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ha M and Kim VN: Regulation of microRNA
biogenesis. Nat Rev Mol Cell Biol. 15:509–524. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Carthew RW: Gene regulation by microRNAs.
Curr Opin Genet Dev. 16:203–208. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nishikawa R, Goto Y, Kojima S, Enokida H,
Chiyomaru T, Kinoshita T, Sakamoto S, Fuse M, Nakagawa M, Naya Y,
et al: Tumor-suppressive microRNA-29s inhibit cancer cell migration
and invasion via targeting LAMC1 in prostate cancer. Int J Oncol.
45:401–410. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Moltzahn F, Olshen AB, Baehner L, Peek A,
Fong L, Stöppler H, Simko J, Hilton JF, Carroll P and Blelloch R:
Microfluidic-based multiplex qRT-PCR identifies diagnostic and
prognostic microRNA signatures in the sera of prostate cancer
patients. Cancer Res. 71:550–560. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ling XH, Han ZD, Xia D, He HC, Jiang FN,
Lin ZY, Fu X, Deng YH, Dai QS, Cai C, et al: MicroRNA-30c serves as
an independent biochemical recurrence predictor and potential tumor
suppressor for prostate cancer. Mol Biol Rep. 41:2779–2788. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Huang Z, Zhang L, Yi X and Yu X:
Diagnostic and prognostic values of tissue hsa-miR-30c and
hsa-miR-203 in prostate carcinoma. Tumour Biol. 37:4359–4365. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang J, Wang X, Wang Y, Peng R, Lin Z,
Wang Y, Hu B, Wang J and Shi G: Low expression of microRNA-30c
promotes prostate cancer cells invasion involved in downregulation
of KRAS protein. Oncol Lett. 14:363–368. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Steele R, Mott JL and Ray RB: MBP-1
upregulates miR-29b that represses Mcl-1, collagens, and
matrix-metalloproteinase-2 in prostate cancer cells. Genes Cancer.
1:381–387. 2010. View Article : Google Scholar : PubMed/NCBI
|