Introduction
In many countries, the majority of cancer-related
deaths occur in people with lung cancer (1). Non-small cell lung cancer (NSCLC) is the
most prominent form of lung cancer, accounting for ~85% of cases
(2). More than half of NSCLC patients
are diagnosed with advanced metastatic disease, and have a poor
prognosis (3). Identifying
non-invasive and convenient biomarkers relevant to diagnosis and
prognosis may be conducive to improving the clinical outcome of
NSCLC patients.
Circulating cell-free DNA (cfDNA) is released into
circulation by various pathological and normal physiological
mechanisms during the turnover of apoptotic and necrotic cells
(4). cfDNA in peripheral blood can be
obtained via ‘liquid biopsy’, and quantification of cfDNA can be
combined with representative tumour information in cancer patients
(5). Thus, the potential significance
of cfDNA in plasma or serum as a diagnostic or prognostic indicator
or for monitoring disease status has attracted increasing
attention. In patients suffering from cancer, higher cfDNA levels
were shown to be significantly correlated with poorer outcome
(6). Some studies have reported that
the quantification of cfDNA can be used as an effective biomarker
to discriminate patients with NSCLC from healthy individuals
(7–10). Since there is a close relationship
between the peripheral blood and lung cancer cells, cfDNA
quantification could be exploited for future diagnostic
applications in lung cancer (11).
However, as various pre-analytical factors related to blood
sampling and processing can affect cfDNA concentrations, the
optimal conditions for processing, cryopreserving and storing cfDNA
must be established before the detection of cfDNA concentration can
be applied clinically (12–15). In addition, cfDNA levels in serum and
their usefulness in predicting cancer metastases and patient
outcome have not been established.
This study was initially performed to assess the
value of cfDNA in serum samples as a diagnostic marker and
predictor of metastasis and poor prognosis in NSCLC. Furthermore,
we aimed to establish optimal conditions for processing,
cryopreserving and storing cfDNA, and to develop a standard
protocol for the quantification of circulating cfDNA by absolute
qPCR of long interspersed nuclear element-1 (LINE1). The results
lay the foundation for the development of serum cfDNA as a new
class of cancer biomarkers in liquid biopsies.
Materials and methods
Sample collection and processing
Serum samples from 60 patients with histologically
confirmed NSCLC and 68 healthy controls, were collected at the
Shanghai Sixth People's Hospital East Campus between October 2014
and June 2016. The Ethics Committee of Shanghai Sixth People's
Hospital East Affiliated to Shanghai University of Medicine &
Health Sciences (Shanghai, China) approved this study. The NSCLC
patient group consisted of 34 patients with primary lung cancer and
26 patients with recurrent lung cancer. The staging of all 60 NSCLC
patients was performed according to the tumour node metastasis
(TNM) classification of malignant tumours, and peripheral blood was
collected from these patients for cfDNA extraction. Four patients
underwent multiple blood collections over time to determine whether
the levels of cfDNA, CEA and CYFRA21-1 correlate with disease
progression. In NSCLC patients, progressive disease is defined as
an increase in target lesion size of at least 20% or the appearance
of new lesions (16). All
participants provided written informed consent. Peripheral blood
was collected from patients in separate gel pro-coagulation vacuum
tubes and EDTA vacutainer tubes (BD Biosciences, Franklin Lakes,
NJ, USA), and serum and plasma were then separated by
centrifugation at 1,200 × g for 10 min at room temperature,
transferred to new tubes and centrifuged at 16,000 × g for 10 min
at 4°C to remove cell debris. Plasma and serum were stored at −80°C
prior to DNA extraction. To determine the optimal sample
preparation and storage conditions for cfDNA quantification, venous
blood samples from 4 healthy volunteers (2 females and 2 males;
26–48 years) were simultaneously collected for the preparation of
serum samples. Serum was separated and then stored at room
temperature (25°C) for 2, 6, or 10 h; at 4°C for 24 h; at −25°C for
1 month; or at −80°C for 1, 3, or 6 months.
cfDNA extraction and fragment
analysis
Circulating DNA was separated from 1 ml serum and
plasma samples with the PME free-circulating DNA extraction kit
(Analytik Jena AG, Jena, Germany), according to the manufacturer's
instructions for up to 1-ml extractions with the lysis solution
SE/binding solution SBS mechanism. The process consisted of several
steps as follows: i) capturing cfDNA in the polymer by mixing
serum/plasma with 30 µl of VCR-1 and 150 µl of VCR-2, followed by
centrifugation at 18,500 × g for 3 min at room temperature; ii)
washing the polymer/DNA complex with 1 ml of ddH2O; iii)
adding 400 µl of lysis solution SE to dissolve the pellet; iv)
adding 50 µl of PK and incubating the samples for 15 min at 70°C;
v) adding 400 µl of binding solution SBS and transferring the
samples to spin filters; vi) washing the samples by adding 500 µl
of washing solution GS and 650 µl of washing solution BS, followed
by centrifugation at 13,500 × g for 1 min at room temperature; and
vii) eluting cfDNA in 50 µl of water and storing the cfDNA at −80°C
until further analysis. The presence of cfDNA and its fragment size
distribution were evaluated by using the Agilent High Sensitivity
DNA kit (Agilent Technologies, Inc., Santa Clara, CA, USA) on the
2100 Bioanalyzer.
cfDNA quantification by LINE1
qPCR
Genomic LINE1 sequences are distributed over all
chromosomes; a short fragment (97 bp) of LINE1 was amplified and
quantified by absolute qPCR quantification, using the standard
curve method to indicate the total amount of serum and plasma cfDNA
(17). LINE1 primer sequences were as
follows: forward, 5′-TGGCACATATACACCATGGAA-3′; and reverse,
5′-TGAGAATGATGGTTTCCAATTTC-3′. The housekeeping gene β-actin was
amplified with forward primer 5′-CCACACTGTGCCCATCTACG-3′ and
reverse primer 5′-AGGATCTTCATGAGGTAGTCAGTCAG-3′, producing products
of 99 bp. The reaction mixture for qPCR included 10 µl of
SYBR® Premix Ex Taq II (Tli RNaseH Plus; Takara
Biotechnology Co., Ltd., Dalian, China), 2 µl of cfDNA template,
0.4 mM primer, 0.4 µl of ROX II and 6 µl of double-distilled water
in a final reaction volume of 20 µl. The qPCR was performed with an
Applied Biosystems 7500 real-time PCR system (ABI; Thermo Fisher
Scientific, Inc., Waltham, MA, USA), and was conducted by using the
following protocol: 95°C for 8 min, followed by 40 cycles of 95°C
for 5 sec and 60°C for 34 sec. A standard curve generated by serial
dilution (from 1.0–10,000 ng/ml) of the LINE1-pCEP plasmid was used
to determine the absolute equivalent amount of cfDNA in each
sample. Melting curve analysis was conducted to confirm the
amplification of a single peak. Each assay was performed in
triplicate.
Reference values of serum cfDNA, CEA
and CYFRA21-1
The levels of serum CEA and CYFRA21-1 were detected
with a CEA and Cyfra21-1 test kit (Roche Diagnostics, Shanghai,
China) by Cobas e601 Analyzer. The normal range was <4.7 ng/ml
for CEA and <3.3 ng/ml for CYFRA21-1. A receiver operating
characteristic (ROC) curve was created to quantify the diagnostic
potential of serum cfDNA, CEA and CYFRA21-1. Youden's index (YI =
sensitivity + specificity−1) was used to select cut-off values. The
area under the ROC curve (AUC) was used to measure the
discriminatory power of the test.
Statistical analysis
SPSS Statistics 19.0 (IBM Corp., Armonk, NY, USA)
and MedCalc statistical software were used to conduct the
statistical analyses. Figures were generated by using GraphPad
Prism 6.0 software (GraphPad Software, Inc., La Jolla, CA, USA).
The Mann-Whitney U test and Kruskal-Wallis H test were applied to
compare serum cfDNA concentrations between groups. Dunn's post hoc
tests were carried out on each pair of groups following
Kruskal-Wallis test. The diagnostic values of cfDNA, CEA and
CYFRA21-1 for NSCLC were assessed by using ROC curves. A univariate
Cox regression model was used to analyse survival data for
progression-free survival (PFS). The Kaplan-Meier method was used
to estimate the PFS, which was evaluated by the log-rank test.
Results were considered significant at two-tailed P<0.05.
Results
Comparison of serum and plasma
cfDNA
To compare cfDNA concentrations between plasma and
serum, we extracted cfDNA from 1 ml each of serum and plasma from
the same donor, and quantified the amount of cfDNA by LINE1 qPCR.
LINE1 is a transposable element belonging to the group of LINEs
found in all mammalian DNA, comprising ~17% of the human genome.
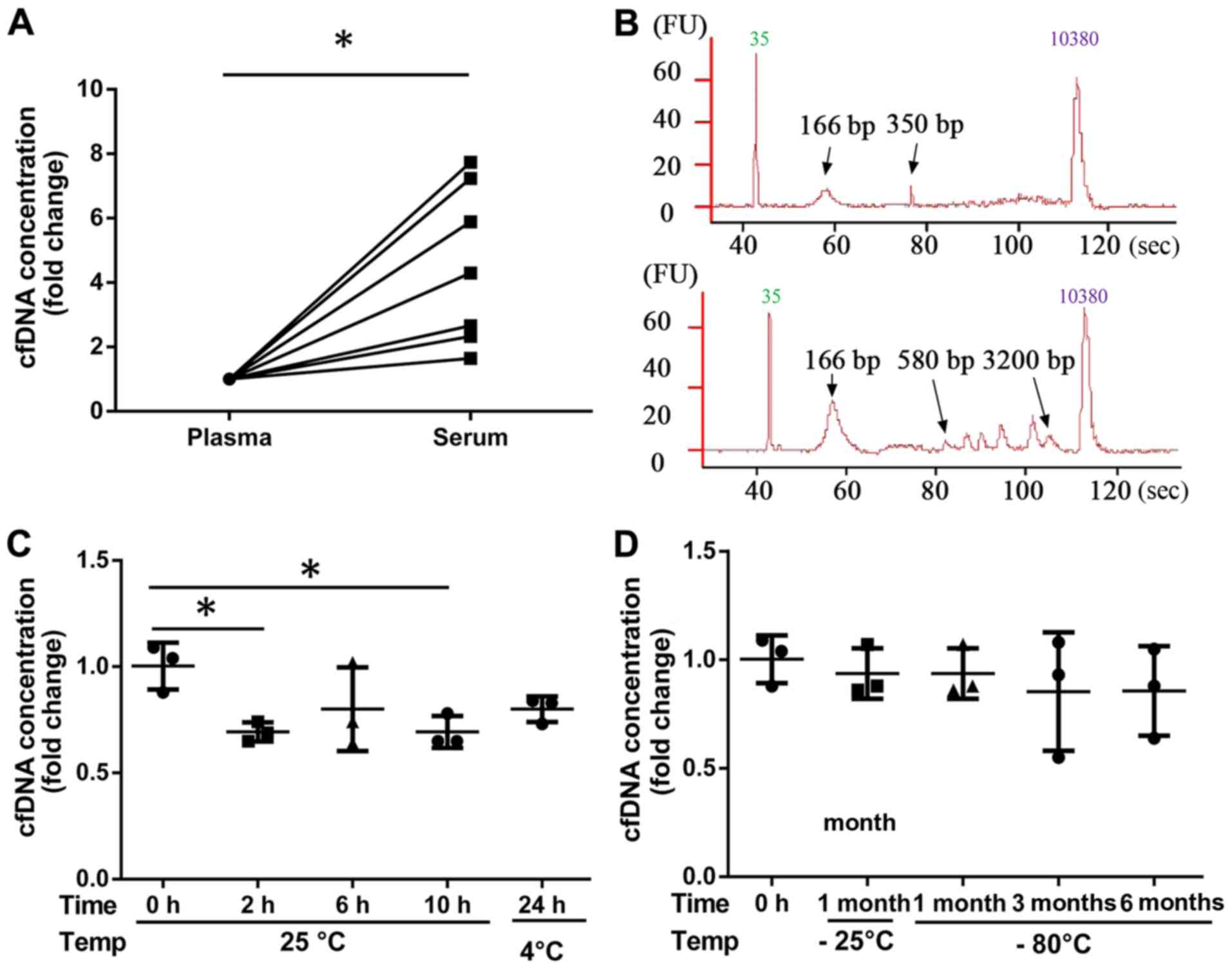
cfDNA concentrations were ~1-to 8-fold higher in serum samples than
those in plasma samples (Fig. 1A). By
fragment analysis, we observed an enrichment of plasma cfDNA
fragments at 166 bp and 350 bp in NSCLC patients (Fig. 1B; upper plot); in serum cfDNA, there
were multiple additional peaks within the range of 580-3,200 bp
(Fig. 1B; lower plot), showing that
the fragment distribution of cfDNA is more complex in serum than
that in plasma.
Effects of different storage
conditions on serum cfDNA yield
Strict standardization of blood collection and serum
preparation methods is mandatory, before serum cfDNA concentration
can be used as a potential marker of clinical disorders. The time
and temperature of blood storage after centrifugation significantly
impacted the serum cfDNA concentration (Fig. 1C and D). Compared with the cfDNA
concentration in serum prepared immediately after venepuncture (0 h
at room temperature), the cfDNA concentrations in serum decreased
after storage at room temperature for 2 or 10 h. However, the
changes in cfDNA concentration in serum after storage at 4°C for 24
h, −25°C for 1 month, or −80°C for 1, 3, or 6 months were not
significant. Based on these findings, serum samples from NSCLC
patients or normal controls were frozen at −80°C immediately after
collection.
Serum cfDNA concentration in NSCLC
patients with different clinical characteristics
To determine whether cfDNA concentration correlates
with NSCLC status or any other clinical parameters, we quantified
cfDNA in serum specimens from 60 NSCLC patients and 68 normal
controls in good health by LINE1 qPCR. Analysis of cfDNA in
different subgroups of NSCLC patients indicated that serum cfDNA is
independent of sex and age: there was no significant difference
(P>0.05) in serum cfDNA concentration between NSCLC patients
aged 39–60 years or 61–85 years, or between NSCLC patients of
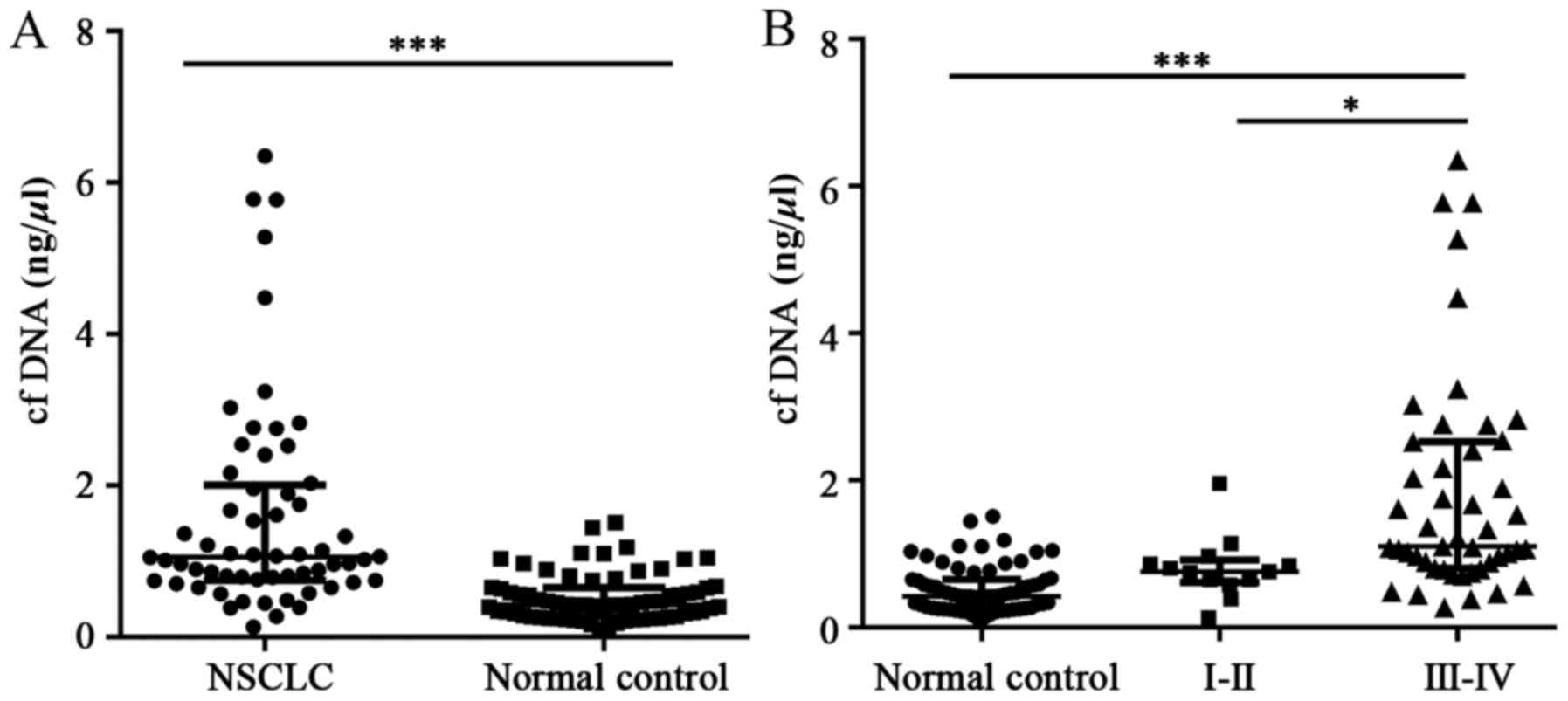
different sex (35 males and 25 females) (Table I). When patients were stratified by
NSCLC status, the results showed that the cfDNA concentration was
significantly higher in NSCLC patients [1.06 (0.75–2.01) ng/µl]
than that in normal controls [0.42 (0.27–0.65) ng/µl] (Fig. 2A). NSCLC patients with more advanced
disease (stage III–IV) had considerably higher cfDNA concentrations
than those in either normal controls or patients with stage I–II
disease (Fig. 2B). In line with the
finding that patients with stage III–IV disease have higher cfDNA
levels; NSCLC patients with lymph node metastasis and distant
metastases also had significantly higher cfDNA levels than patients
without metastasis (Table I).
 | Table I.The clinical characteristics of 60
NSCLC patients. |
Table I.
The clinical characteristics of 60
NSCLC patients.
| Clinical
characteristics | No. | cfDNA (ng/µl) median
(IQR 25–75) | P-value |
|---|
| All | 60 | 1.055
(0.751–2.011) |
|
| Age (years) |
|
|
|
|
39–60 | 21 | 1.061
(0.752–1.923) | 0.859 |
|
61–85 | 39 | 1.020
(0.748–2.164) |
|
| Sex |
|
|
|
| Male | 35 | 1.092
(0.792–2.538) | 0.132 |
|
Female | 25 | 1.012
(0.678–1.271) |
|
| Tumour stage
(TNM) |
|
|
|
| I–II | 13 | 0.757
(0.615–0.914) | 0.0032 |
|
III–IV | 47 | 1.100
(0.801–2.523) |
|
| N0 | 26 | 0.825
(0.634–1.040) | 0.0002 |
|
N1-N3 | 34 | 1.449
(0.100–2.756) |
|
| M0 | 20 | 0.825
(0.653–1.122) | 0.0109 |
| M1 | 40 | 1.156
(0.822–2.535) |
|
Diagnostic utility of serum cfDNA in
NSCLC patients
ROC curves were generated to distinguish NSCLC
patients from normal healthy controls based on serum cfDNA, CEA or
CYFRA21-1 levels (Fig. 3). CEA and
CYFRA21-1 are established biomarkers for the diagnosis of NSCLC
(18). The AUC of cfDNA for
distinguishing NSCLC patients from normal controls was 0.848 (95%
CI: 0.774–0.905), which was comparable to that of CEA [0.829 (95%
CI: 0.753–0.890)] and CYFRA21-1 [0.833 (95% CI: 0.756–0.893)]. No
obvious differences were found between the AUC values of each
indicator (P>0.05). YI was the largest at 0.67 ng/µl cfDNA,
which was defined as the cut-off value of cfDNA, and yielded a
sensitivity of 81.67% and a specificity of 77.94%. By comparison,
at the cut-off values of CEA and CYFRA21-1, the sensitivity of CEA
was 61.67% with a specificity of 97.06%, and the sensitivity of
CYFRA21-1 was 63.33% with a specificity of 91.18%. To determine
whether cfDNA quantification could be used in combination with
existing biomarkers to maximize the diagnostic efficiency for NSCLC
patients, the ROC AUC was calculated after combining CEA and
CYFRA21-1 with cfDNA. The integration of cfDNA with CEA and
CYFRA21-1 (AUC 0.915; sensitivity 83.33%; and specificity 85.29%)
resulted in an improved diagnostic efficiency for NSCLC (Table II).
| Table II.Diagnostic value of serum cfDNA, CEA
and CYFRA21-1 for NSCLC patients. |
Table II.
Diagnostic value of serum cfDNA, CEA
and CYFRA21-1 for NSCLC patients.
| Marker | AUC | Sensitivity
(%) | Specificity
(%) | Positive predictive
value (%) | Negative predictive
value (%) |
|---|
| cfDNA | 0.85 | 81.67 | 77.94 | 76.60 | 82.80 |
| CEA | 0.83 | 61.67 | 97.06 | 94.90 | 74.20 |
| CYFRA21-1 | 0.83 | 63.33 | 91.18 | 86.40 | 73.80 |
| CEA +
CYFRA21-1 | 0.87 | 70.00 | 94.12 | 91.30 | 78.00 |
| cfDNA + CEA | 0.908a | 75.00 | 92.65 | 90.00 | 80.80 |
| cfDNA +
CYFRA21-1 | 0.894a | 73.33 | 92.65 | 89.80 | 79.70 |
| cfDNA + CEA +
CYFRA21-1 | 0.915a | 83.33 | 85.29 | 83.30 | 85.30 |
Connection between serum cfDNA and
clinical NSCLC progression
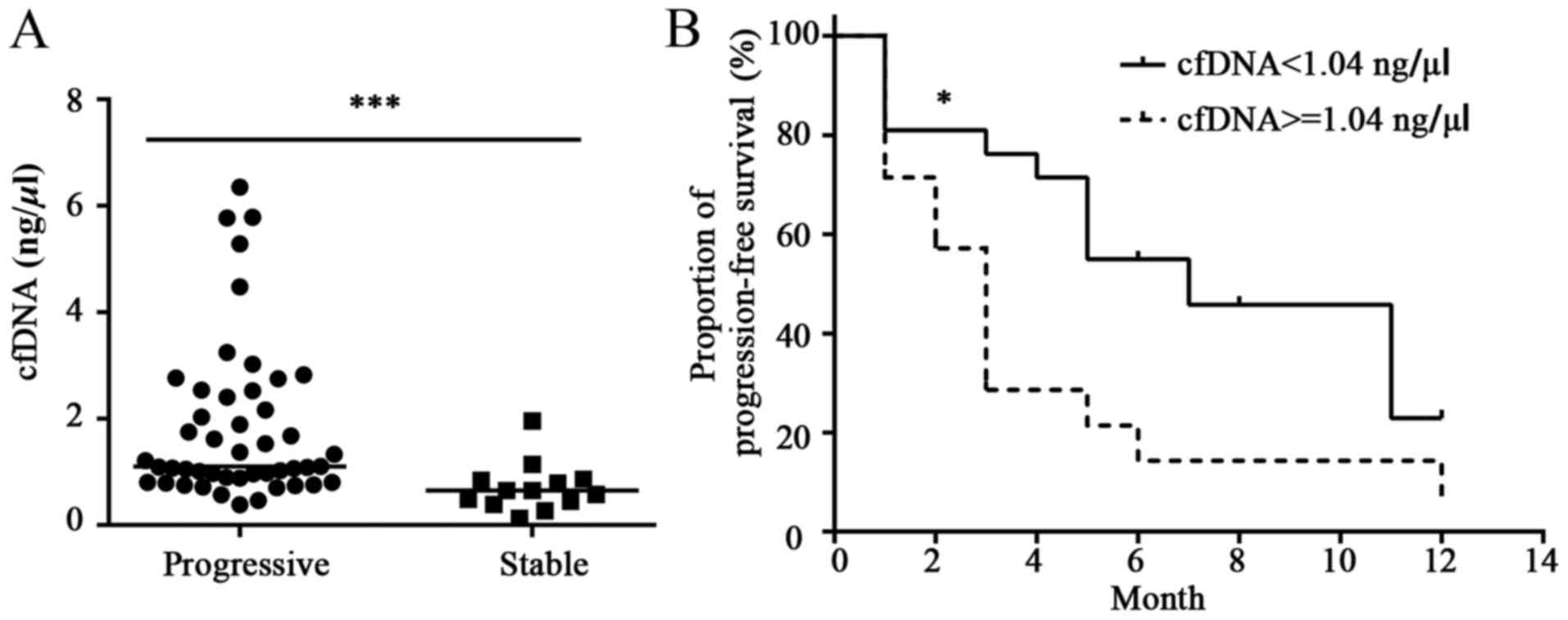
To assess whether the cfDNA concentration is
different in samples obtained from NSCLC patients with progressive
rather than stable disease, the 60 NSCLC patients were divided into
the progression and stable groups. The cfDNA concentration was
higher in NSCLC patients with progressive disease than that in
patients with stable disease (Fig.
4A). In addition, the Kaplan-Meier curve revealed that serum
cfDNA ≥1.04 ng/µl was related to poorer PFS than serum cfDNA
<1.04 ng/µl (median PFS: 7.0 vs. 3.0 months, hazard ratio [HR],
0.43; 95% confidence interval [CI]: 0.19–0.96, P<0.05) (Fig. 4B).
Serum cfDNA level dynamics in NSCLC
patients
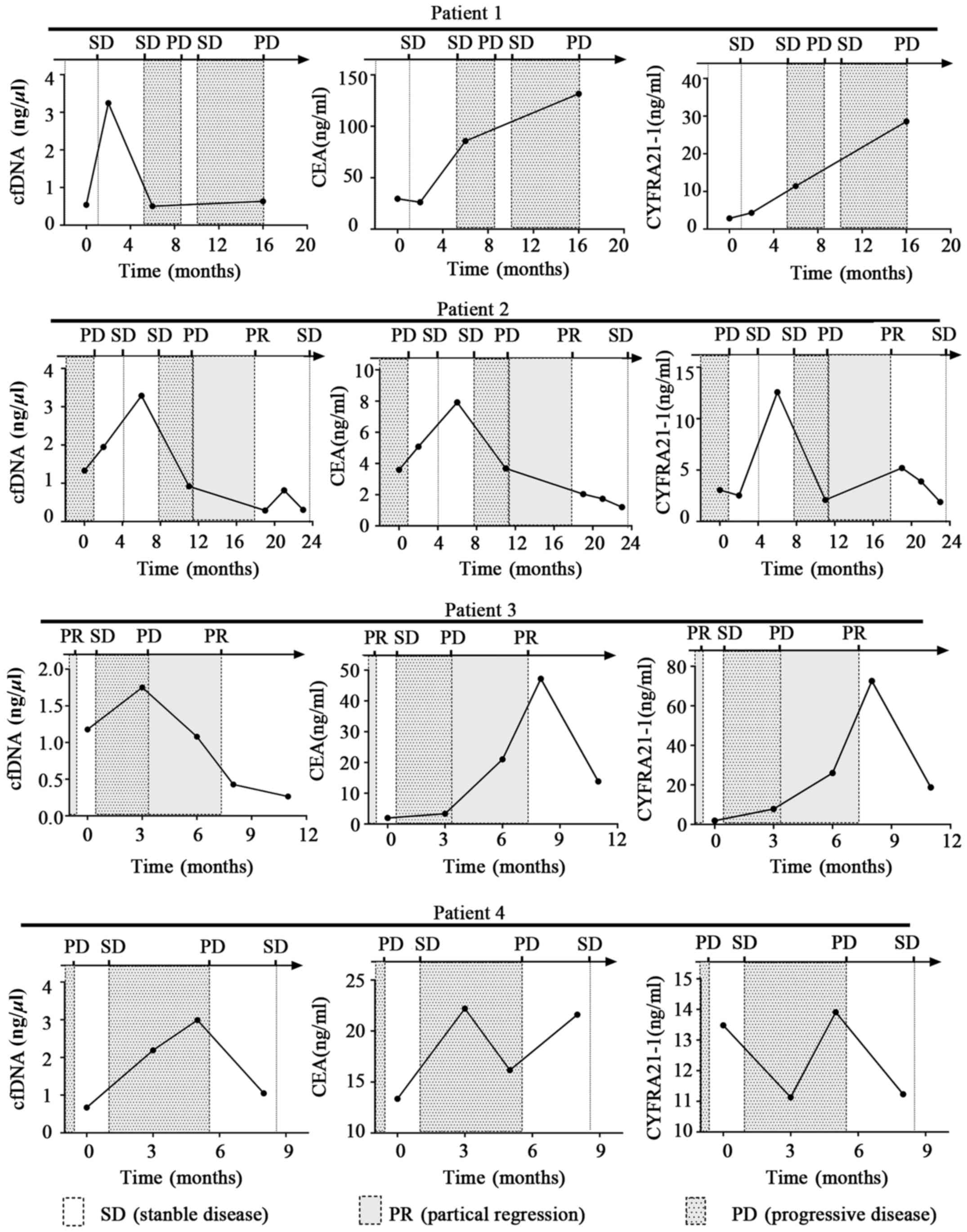
To identify the predictive value of cfDNA in NSCLC
progression, cfDNA, CEA and CYFRA21-1 levels were analysed in serum
samples from 4 NSCLC patients with progressive disease at several
time-points. The line charts were plotted to describe the changes
in cfDNA, CEA and CYFRA21-1 levels during cancer progression. As
shown in Fig. 5, the time-dependent
changes in the three markers in patient 2 were nearly identical,
but were inconsistent with the changes in the other 3 NSCLC
patients. During the course of the disease, there was a general
trend of cfDNA concentration decreasing or remaining stable before
periods of disease stability, and increasing before periods of
disease progression. Interestingly, cfDNA levels often peaked
before a period of disease progression, and the lead time was 1–7
months compared with clinical medical imaging. Alterations in serum
levels of CEA and CYFRA21-1 occurred in line with disease
progression, and did not show such peaks.
Discussion
In this study, we established optimal conditions for
processing, cryopreserving, and storing cfDNA and developed a
standard protocol for the quantification of circulating cfDNA by
absolute LINE1 qPCR. We utilized this approach to examine serum
cfDNA levels in 60 NSCLC patients with different stage disease and
68 normal controls to determine whether changes in serum cfDNA
levels have diagnostic and predictive value for NSCLC, and we
compared the diagnostic value of serum cfDNA, CEA and CYFRA21-1 by
ROC curve analysis. Furthermore, we examined the time-dependent
changes in serum cfDNA levels in 4 NSCLC patients during cancer
progression.
There is some controversy about the optimal source
of cfDNA for analysis. Previous studies suggested that plasma may
be a more reliable source than serum owing to higher background
levels of non-tumour wild-type DNA in serum (19). However, there are some other studies
that have suggested the use of serum cfDNA in the diagnosis of
malignancies such as hepatocellular carcinoma and endometrial
cancer (20,21). In addition, serum samples are prepared
without anticoagulants, and there is no need for specialized blood
collection tubes, as there is for plasma. Serum is still considered
as the gold standard, and used more widely than plasma in clinical
laboratory. Therefore, we extracted cfDNA from serum samples for
analysis, and showed that the quantification of circulating cfDNA
levels in serum have value as a diagnostic for NSCLC or for
monitoring disease progression.
There are no clear criteria for blood collection or
storage conditions for cfDNA analysis. There is a concern, for
instance, that the in vitro lysis of leukocytes during the
coagulation/fibrinolysis phase of sample preparation will lead to
higher serum cfDNA concentrations. In our study, compared with the
cfDNA concentrations in serum prepared immediately after
venepuncture (0 h at room temperature), the cfDNA concentrations in
serum samples were decreased when serum was stored at room
temperature up to 10 h, but were not significantly different after
storage at lower temperatures, such as 4, −25 or −80°C. This
phenomenon may be due to the degradation of cfDNA at room
temperature by DNase activity, which is inhibited at lower
temperatures. According to these results, serum samples for cfDNA
quantification were frozen at −8°C immediately after collection.
Two main sources of cfDNA have been proposed: release from
apoptotic or necrotic cells or release of intact cells in the
bloodstream (22). In our study, the
size profile of cfDNA in plasma samples showed a major peak at 166
bp and another outstanding peak at 350 bp. Interestingly, serum
cfDNA profiling showed more peak diversity. In addition to the
relatively short 166-bp cfDNA fragments, cfDNA fragment peaks were
observed ranging from 580 to 3,200 bp. We propose that the 166-bp
peak probably represents DNA coiled around a nucleosome core unit
(~146 bp) with a linker section of DNA (~20 bp), while the
remaining peaks likely result from inter-nucleosome cleavage of
genomic DNA.
cfDNA levels can be quantified by several
techniques, including DNA Dipstick, PicoGreen, Agilent 2100
Bioanalyzer and real-time PCR. Moreover, several studies have
quantified cfDNA by using real-time PCR with various reference
genes such as human β-actin, hTERT, GAPDH, ALU and LINE-1 (10,23). In
our study, we carried out a pre-experiment to optimize
quantification of cfDNA before formal test. The pre-experiment
results demonstrated that the levels of cfDNA of NSCLC patients
quantified by qPCR results using primer of β-actin and LINE-1 have
the same varying trend. Also, the amplification efficiency was
greater with LINE-1 primer (data not shown). Therefore, we used
absolute qPCR analysis of LINE-1 to quantify serum and plasma cfDNA
in the present study. The cfDNA concentrations were 1- to 8-fold
higher in fresh serum samples than those in fresh plasma samples,
which is consistent with previous reports that serum samples
contain 2- to 24-fold higher levels of cfDNA than plasma samples
(24,25). Moreover, the cfDNA level in NSCLC
patients [1.06 (0.75–2.01) ng/µl] was significantly higher than
that in normal controls [0.47 (0.23–0.86) ng/µl], which is
consistent with the previous reports.
In the present study, we also found that NSCLC
patients with lymph node metastasis and distant metastases had a
significantly higher cfDNA level. Furthermore, NSCLC patients with
advanced stage (III–IV) disease had considerably higher cfDNA
levels than that in normal controls or patients with stage I–II
disease, which was consistent with previous reports. Importantly,
no significant differences were detected between normal controls
and patients with stage I–II disease or between NSCLC patients of
different ages or sex. We suspect that serum cfDNA may not be
sensitive enough for early detection of NSCLC patients, further
studies are needed to confirm this hypothesis. Previous studies
have suggested the cfDNA levels are affected by cancer-dependent
variables, including tumour size, location, and stage, as well as
other elements related to risk and prognosis (6). Consequently, while it is evident that
serum cfDNA levels are correlated with advanced tumour stage and
metastasis in NSCLC patients, they are not closely related to age
or sex.
Tumour biomarkers in serum from NSCLC patients, such
as CEA and CYFRA21-1, are not sufficient to diagnose or monitor
lung cancer due to the lack of sensitivity and specificity to a
particular type of cancer, and the levels of these factors may be
increased by irrelevant issues (26,27).
According to the results, the AUC of serum cfDNA for distinguishing
NSCLC patients from normal controls was comparable to that of CEA
and CYFRA21-1. In addition, compared with the diagnostic efficiency
of serum cfDNA, serum CEA or CYFRA21-1 alone, the combination of
these three factors into one indicator improved the diagnostic
efficiency for NSCLC. This result indicates that cfDNA is a good
screening tool for NSCLC that may be used in combination with
existing biomarkers to improve the diagnostic efficacy.
Our results also showed that the serum cfDNA
concentration was higher in NSCLC patients with progressive disease
than that in those with stable disease. In addition, higher serum
cfDNA levels were related to poorer PFS in patients with NSCLC. In
patients suffering from different carcinomas, higher cfDNA
concentrations have been shown to be an independent predictor of a
worse outcome regarding overall survival or an interval irrelevant
to disease (28–33). Increasing cfDNA levels suggest tumour
progression during therapy, while decreasing levels indicate an
early treatment response (34,35). By
tracking the serum cfDNA concentration at several time-points in 4
NSCLC patients, we found that cfDNA levels decreased in samples
from NSCLC patients with stable disease, and tended to increase
during or before periods of disease progression, with a lead time
of 1–7 months compared with clinical medical imaging. Although the
number of cases was small, and further confirmation is needed,
these findings show that increasing serum cfDNA values in patients
during follow-up may indicate progression earlier than that in
clinical imaging studies.
In conclusion, the present investigation indicates
that serum cfDNA might be a valuable new biomarker for diagnosing
NSCLC and monitoring metastatic progression. Quantification of
cfDNA may therefore contribute to molecular staging, and to
optimizing advanced personalized medicine for NSCLC. Future studies
on a larger number of NSCLC patients with a sufficient follow-up
time are now required to further validate the clinical utility of
serum cfDNA.
Acknowledgements
Not applicable.
Funding
This study was supported by the Seed Fund Program of
Shanghai University of Medicine & Health Sciences (no.
HMSF-16-21-020).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
LW and WW designed the study, carried out the
experiment and wrote the manuscript. LH and WY collected and
analyzed the data. YD conceived the original idea and analyzed the
results. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Shanghai Sixth People's Hospital East Affiliated to Shanghai
University of Medicine & Health Sciences (Shanghai, China).
Patients who participated in this research, signed an informed
consent and had complete clinical data.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ettinger DS, Akerley W, Bepler G, Blum MG,
Chang A, Cheney RT, Chirieac LR, D'Amico TA, Demmy TL, Ganti AK, et
al; NCCN Non-Small Cell Lung Cancer Panel Members, . Non-small cell
lung cancer. J Natl Compr Canc Netw. 8:740–801. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Schiller JH, Harrington D, Belani CP,
Langer C, Sandler A, Krook J, Zhu J and Johnson DH; Eastern
Cooperative Oncology Group, : Comparison of four chemotherapy
regimens for advanced non-small-cell lung cancer. N Engl J Med.
346:92–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Stroun M, Lyautey J, Lederrey C,
Olson-Sand A and Anker P: About the possible origin and mechanism
of circulating DNA apoptosis and active DNA release. Clin Chim
Acta. 313:139–142. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Volik S, Alcaide M, Morin RD and Collins
C: Cell-free DNA (cfDNA): Clinical significance and utility in
cancer shaped by emerging technologies. Mol Cancer Res. 14:898–908.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jung K, Fleischhacker M and Rabien A:
Cell-free DNA in the blood as a solid tumor biomarker—a critical
appraisal of the literature. Clin Chim Acta. 411:1611–1624. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chiappetta C, Anile M, Leopizzi M, Venuta
F and Della Rocca C: Use of a new generation of capillary
electrophoresis to quantify circulating free DNA in non-small cell
lung cancer. Clin Chim Acta. 425:93–96. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ulivi P, Mercatali L, Casoni GL, Scarpi E,
Bucchi L, Silvestrini R, Sanna S, Monteverde M, Amadori D, Poletti
V, et al: Multiple marker detection in peripheral blood for NSCLC
diagnosis. PLoS One. 8:e574012013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cargnin S, Canonico PL, Genazzani AA and
Terrazzino S: Quantitative analysis of circulating cell-free DNA
for correlation with lung cancer survival: A systematic review and
meta-analysis. J Thorac Oncol. 12:43–53. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Jiang T, Zhai C, Su C, Ren S and Zhou C:
The diagnostic value of circulating cell free DNA quantification in
non-small cell lung cancer: A systematic review with meta-analysis.
Lung Cancer. 100:63–70. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sozzi G, Conte D, Leon M, Ciricione R, Roz
L, Ratcliffe C, Roz E, Cirenei N, Bellomi M, Pelosi G, et al:
Quantification of free circulating DNA as a diagnostic marker in
lung cancer. J Clin Oncol. 21:3902–3908. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Devonshire AS, Whale AS, Gutteridge A,
Jones G, Cowen S, Foy CA and Huggett JF: Towards standardisation of
cell-free DNA measurement in plasma: Controls for extraction
efficiency, fragment size bias and quantification. Anal Bioanal
Chem. 406:6499–6512. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jen J, Wu L and Sidransky D: An overview
on the isolation and analysis of circulating tumor DNA in plasma
and serum. Ann NY Acad Sci. 906:8–12. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lui YY, Chik KW and Lo YM: Does
centrifugation cause the ex vivo release of DNA from blood cells?
Clin Chem. 48:2074–2076. 2002.PubMed/NCBI
|
|
15
|
Jung M, Klotzek S, Lewandowski M,
Fleischhacker M and Jung K: Changes in concentration of DNA in
serum and plasma during storage of blood samples. Clin Chem.
49:1028–1029. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Holdhoff M, Schmidt K, Diehl F, Aggrawal
N, Angenendt P, Romans K, Edelstein DL, Torbenson M, Kinzler KW,
Vogelstein B, et al: Detection of tumor DNA at the margins of
colorectal cancer liver metastasis. Clin Cancer Res. 17:3551–3557.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Q, Zheng H, Hu F, Zhang H, Hu Y, Li
J, Zhang T, Liu Z, Lu B, Hu A, et al: Serum CYFRA21-1 is correlated
with the efficacy of epidermal growth factor receptor-tyrosine
kinase inhibitor in non-small cell lung cancer patients harboring
EGFR mutations. Zhongguo Fei Ai Za Zhi. 19:550–558. 2016.(In
Chinese). PubMed/NCBI
|
|
19
|
Molina-Vila MA, de-Las-Casas CM,
Bertran-Alamillo J, Jordana-Ariza N, González-Cao M and Rosell R:
cfDNA analysis from blood in melanoma. Ann Transl Med.
3:3092015.PubMed/NCBI
|
|
20
|
Chen K, Zhang H, Zhang LN, Ju SQ, Qi J,
Huang DF, Li F, Wei Q and Zhang J: Value of circulating cell-free
DNA in diagnosis of hepatocelluar carcinoma. World J Gastroenterol.
19:3143–3149. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cicchillitti L, Corrado G, De Angeli M,
Mancini E, Baiocco E, Patrizi L, Zampa A, Merola R, Martayan A,
Conti L, et al: Circulating cell-free DNA content as blood based
biomarker in endometrial cancer. Oncotarget. 8:115230–115243. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gormally E, Caboux E, Vineis P and Hainaut
P: Circulating free DNA in plasma or serum as biomarker of
carcinogenesis: Practical aspects and biological significance.
Mutat Res. 635:105–117. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fawzy A, Sweify KM, El-Fayoumy HM and
Nofal N: Quantitative analysis of plasma cell-free DNA and its DNA
integrity in patients with metastatic prostate cancer using ALU
sequence. J Egypt Natl Cancer Inst. 28:235–242. 2016. View Article : Google Scholar
|
|
24
|
Lo YM, Tein MS, Lau TK, Haines CJ, Leung
TN, Poon PM, Wainscoat JS, Johnson PJ, Chang AM and Hjelm NM:
Quantitative analysis of fetal DNA in maternal plasma and serum:
Implications for noninvasive prenatal diagnosis. Am J Hum Genet.
62:768–775. 1998. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lee TH, Montalvo L, Chrebtow V and Busch
MP: Quantitation of genomic DNA in plasma and serum samples: Higher
concentrations of genomic DNA found in serum than in plasma.
Transfusion. 41:276–282. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ma S, Shen L, Qian N and Chen K: The
prognostic values of CA125, CA19.9, NSE, AND SCC for stage I NSCLC
are limited. Cancer Biomark. 10:155–162. 2011-2012. View Article : Google Scholar
|
|
27
|
Rosell R, Carcereny E, Gervais R,
Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, Sanchez JM, et al Spanish Lung Cancer Group in
collaboration with Groupe Français de Pneumo-Cancérologie and
Associazione Italiana Oncologia Toracica, : Erlotinib versus
standard chemotherapy as first-line treatment for European patients
with advanced EGFR mutation-positive non-small-cell lung cancer
(EURTAC): A multicentre, open-label, randomised phase 3 trial.
Lancet Oncol. 13:239–246. 2012-2012. View Article : Google Scholar
|
|
28
|
Schwarzenbach H, Müller V, Stahmann N and
Pantel K: Detection and characterization of circulating
microsatellite-DNA in blood of patients with breast cancer. Ann NY
Acad Sci. 1022:25–32. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ren N, Qin LX, Tu H, Liu YK, Zhang BH and
Tang ZY: The prognostic value of circulating plasma DNA level and
its allelic imbalance on chromosome 8p in patients with
hepatocellular carcinoma. J Cancer Res Clin Oncol. 132:399–407.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yoon KA, Park S, Lee SH, Kim JH and Lee
JS: Comparison of circulating plasma DNA levels between lung cancer
patients and healthy controls. J Mol Diagn. 11:182–185. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ludovini V, Pistola L, Gregorc V, Floriani
I, Rulli E, Piattoni S, Di Carlo L, Semeraro A, Darwish S,
Tofanetti FR, et al: Plasma DNA, microsatellite alterations, and
p53 tumor mutations are associated with disease-free survival in
radically resected non-small cell lung cancer patients: a study of
the perugia multidisciplinary team for thoracic oncology. J Thorac
Oncol. 3:365–373. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kamat AA, Baldwin M, Urbauer D, Dang D,
Han LY, Godwin A, Karlan BY, Simpson JL, Gershenson DM, Coleman RL,
et al: Plasma cell-free DNA in ovarian cancer: An independent
prognostic biomarker. Cancer. 116:1918–1925. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Jung K, Stephan C, Lewandowski M, Klotzek
S, Jung M, Kristiansen G, Lein M, Loening SA and Schnorr D:
Increased cell-free DNA in plasma of patients with metastatic
spread in prostate cancer. Cancer Lett. 205:173–180. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Gautschi O, Bigosch C, Huegli B, Jermann
M, Marx A, Chassé E, Ratschiller D, Weder W, Joerger M, Betticher
DC, et al: Circulating deoxyribonucleic Acid as prognostic marker
in non-small-cell lung cancer patients undergoing chemotherapy. J
Clin Oncol. 22:4157–4164. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kumar S, Guleria R, Singh V, Bharti AC,
Mohan A and Das BC: Efficacy of circulating plasma DNA as a
diagnostic tool for advanced non-small cell lung cancer and its
predictive utility for survival and response to chemotherapy. Lung
Cancer. 70:211–217. 2010. View Article : Google Scholar : PubMed/NCBI
|