Introduction
Atrial myxomas are the most common primary cardiac
tumors, comprising up to 80% of all primary tumors of the heart
(1). It is widely admitted that these
tumors originate from subendocardial multipotential mesenchymal
cells (2). Anatomically, atrial
myxomas are mostly pedunculated and soft, and which are in
consistency with a smooth, villous, or irregular surface. Atrial
myxomas predominantly occur between the third and the sixth decades
of life and show a 2.05:1 female predominance (3). Over 75% of myxomas originate from the
left atrium, 18% of them from the right atrium, while less than 5%
are found in bilateral atrium (4).
Clinical manifestations of atrial myxoma vary greatly and patients
usually present one of the symptoms in the following tetrad:
Arrhythmias, intracardiac flow obstruction, embolic phenomena and
constitutional symptoms (5). Atrial
myxomas are asymptomatic in ~10% of the affected individuals
(6). In clinic, neurologic signs
occur in 25–45% of myxoma patients, and may appear as the initial
symptom in 12% individuals (7).
Surgical resection is the most effective treatment and preventive
intervention in atrial myxomas.
The neurological signs of atrial myxoma commonly
result from ischemic cerebral infarction complications, which are
found in 30–50% of patients with myxoma (8). Manifestation as haemorrhagic stroke is
uncommon, and this seems to be related to the formation of cerebral
aneurysms (9). The tumor type, size,
location and mobility appear to be closely associated with embolism
in patients with atrial myxomas (10). Cerebral infarction might recur for
non-diagnosed and treated myxomas. The delayed neurological
complications of myxomatous disease include oncotic aneurysms and
myxomatous metastasis. They usually present with manifestations
similar to cerebral vasculitis and infective endocarditis (3). Accordingly, echocardiography, computed
tomography, and magnetic resonance imaging of the heart should be
performed in patients with suspected stroke.
Studies of atrial myxoma and secondary brain
infarction are generally small series and case reports. In this
study, clinical cases of atrial myxoma-associated neurologic
complications were assessed for morphology and clinical data, also
summarizing their imaging characteristics.
Patients and methods
Patients
Patient records of West China Hospital (Chengdu,
China) and Affiliated Hospital of Hainan Medical University
(Haikou, China) were queried for myxoma detection between March 10,
2003 and February 5, 2015, and a total of 130 patients definitely
diagnosed with atrial myxoma were enrolled. After approval by the
institutional review boards, 22 consecutive patients were
identified with neurologic complications resulting from cardiac
myxoma. The medical history of each patient was reviewed in detail,
recording neurological conditions related to atrial myxoma. The
patients were classified into two groups (embolic vs. non-embolic),
and sex, age, cardiovascular risk factors, myxoma location and
size, initial manifestation, neuroimaging assays, and clinical
outcome were recorded for each of them.
Immunohistochemistry
For immunohistochemical analysis of atrium myxoma,
paraffin-embedded samples were sliced and mounted on microscopic
slides. Rabbit monoclonal anti-CD34 and anti-CD68 antibodies (Santa
Cruz Biotechnology Inc., Dallas, TX, USA) were the first antibodies
and were diluted 200 times. Antigens retrieved using citric acid
buffer (10 mmol/l, pH 7.2) and by microwaving slides. The samples
were treated with primary antibody at 4°C overnight followed by
incubation with biotinylated secondary antibody (1:1,000 dilution;
Zhongshan Biology Company, Beijing, China). Finally, freshly
prepared DAB coloring solution was added, and CD34 or CD68 would
stain brown under the microscope.
Statistical analysis
Statistical analysis was performed with SPSS 19.0
(IBM Corp., Armonk, NY, USA). Data were presented as mean ±
standard deviation (SD). Categorical variables were assessed by the
chi-square test or Fisher's exact test. P<0.05 was considered to
indicate a statistically significant difference.
Results
Patient population
Neurologic complications associated with cardiac
myxoma were found in 22 patients (17%), comprising 9 male and 13
female individuals (Table I). Ages
were 39.9±12.6 (range 13–78) years. Seven patients (32%) had no
remarkable medical history before diagnosis. Meanwhile, 15 subjects
(68%) showed cerebrovascular risk factors such as hyperlipidemia
(n=10), hypertension (n=6), and smoking (n=5). Myxomas were limited
to the left atrium in 20 cases (90.9%). A total of 19 patients
(86.4%) had neurologic signs as initial presentations, while three
patients initially showed cardiac signs, with neurologic symptoms
occurring 2 years after surgical treatment. All patients showing
neurologic complications associated with cardiac myxoma underwent
neuroimaging. Brain computed tomography (CT) was performed in 19
patients (86.4%). Twenty-one individuals (95.5%) had brain magnetic
resonance (MRI) examinations. Twelve patients (54.5%) underwent
cerebrovascular arterial imaging with magnetic resonance
angiography (MRA) and computed tomography angiography (CTA). Five
patients (22.7%) were submitted to digital subtraction angiography
(DSA) examinations.
 | Table I.Baseline clinical characteristics of
patients with atrial myxoma. |
Table I.
Baseline clinical characteristics of
patients with atrial myxoma.
| Patient
characteristic | N (%) |
|---|
| Sex |
|
| Male | 9 (40.9) |
|
Female | 13 (59.1) |
| Age, mean ± SD | 39.9±12.6 |
| Age range, years | 13–78 |
| Medical
conditions |
|
|
Hyperlipidemia | 10 (45.5) |
|
Hypertension | 6 (27.3) |
|
Smoking | 5 (22.7) |
| Myxoma location |
|
| Left
atrium | 20 (90.9) |
| Right
atrium | 1 (4.5) |
|
Multichamber | 1 (4.5) |
| Initial symptoms |
|
|
Dyskinesia | 12 (54.5) |
| Speech
dysfunction | 3 (13.6) |
|
Disturbance of
consciousness | 2 (9.1) |
|
Headache | 1 (4.5) |
| Vision
changes | 1 (4.5) |
|
Palpitations | 2 (9.1) |
|
Dyspnoea | 1 (4.5) |
| Neuroimaging |
|
|
Non-contrast CT | 19 (86.4) |
| CTA | 2 (9.1) |
| MRI | 21 (95.5) |
| MRA | 12 (54.5) |
| DSA | 5 (22.7) |
Characteristics of subjects with
myxoma associated cerebral infarction
The characteristics of 15 individuals developing
cerebral infarction secondary to myxomatous emboli are listed in
Table II. Sudden-onset unilateral
motor deficit was most frequent, occurring in 13 subjects (87%).
Among the 15 cases with cerebral infarctions, 8 (53.3%) and 7
(46.7%), respectively, had infarcts in multiple and single vascular
territories. Cardiac myxomas were surgically resected with success
in all patients. The time period between the onset of neurological
symptoms and resection averaged 20 days, ranging from 1 to 27 days,
excluding patient 5 who suffered a transient ischemic attack (TIA)
2 years before myxoma diagnosis. Three patients (20.0%) showed
persistent neurologic deficits at final follow-up.
| Table II.Characteristics of patients presenting
with cerebral infarction complications of myxoma. |
Table II.
Characteristics of patients presenting
with cerebral infarction complications of myxoma.
| Age/sex | Neurological
syndrome | Infarction location
on imaging | Time elapsed between
cerebral infarction and myxoma diagnosis | Neurological
disability on last follow-up |
|---|
| 44/F | Right-sided
weakness | Left frontoparietal
infarct | Simultaneous | None |
| 58/F | Aphasia and
right-sided hemiparesis | Left temporoparietal
infarct | Simultaneous | Mild persistent
right-sided weakness |
| 22/M | Left-sided
hemiparesis | Right frontal lobe
infarct | Simultaneous | None |
| 71/F | Left-sided
hemiparesis, left arm paraesthesia | Right parietal
infarct | Simultaneous | None |
| 41/M | Left-sided
hemiparesis, facial droop | Right basal ganglia
and corona radiata infarcts | 2 years | None |
| 67/M | Visual changes,
bilateral Frontal headache | Left occipital
ischaemic infarct | Simultaneous | Persistent left sided
weakness |
| 30/F | Left-sided arm and
leg weakness | Right parietal
infarct, posterior putamen and right centrum semiovale | Simultaneous | None |
| 50/F | Right arm and face
weakness | Left thalamus,
midbrain and temporal lobe infarct | Simultaneous | None |
| 69/F | Left-sided arm
weakness | Right parietal
infarct | Simultaneous | None |
| 55/M | Dysarthria, left
hemiparesis | Multiple
infarctions | Simultaneous | Persistent right
sided weakness |
| 23/F | Right-sided
weakness | Left frontoparietal
infarct | Simultaneous | None |
| 49/M | Right facial palsy,
right hemiparesis | Multiple
infarctions | Simultaneous | None |
| 61/F | Left arm
weakness | Left frontal and left
occipital lobe infarcts | Simultaneous | None |
| 62/F | Right-sided
hemiparesis and mixed aphasia | Left temporoparietal
infarct | Simultaneous | None |
| 38/M | Visual changes | Left occipital
ischaemic infarct | Simultaneous | None |
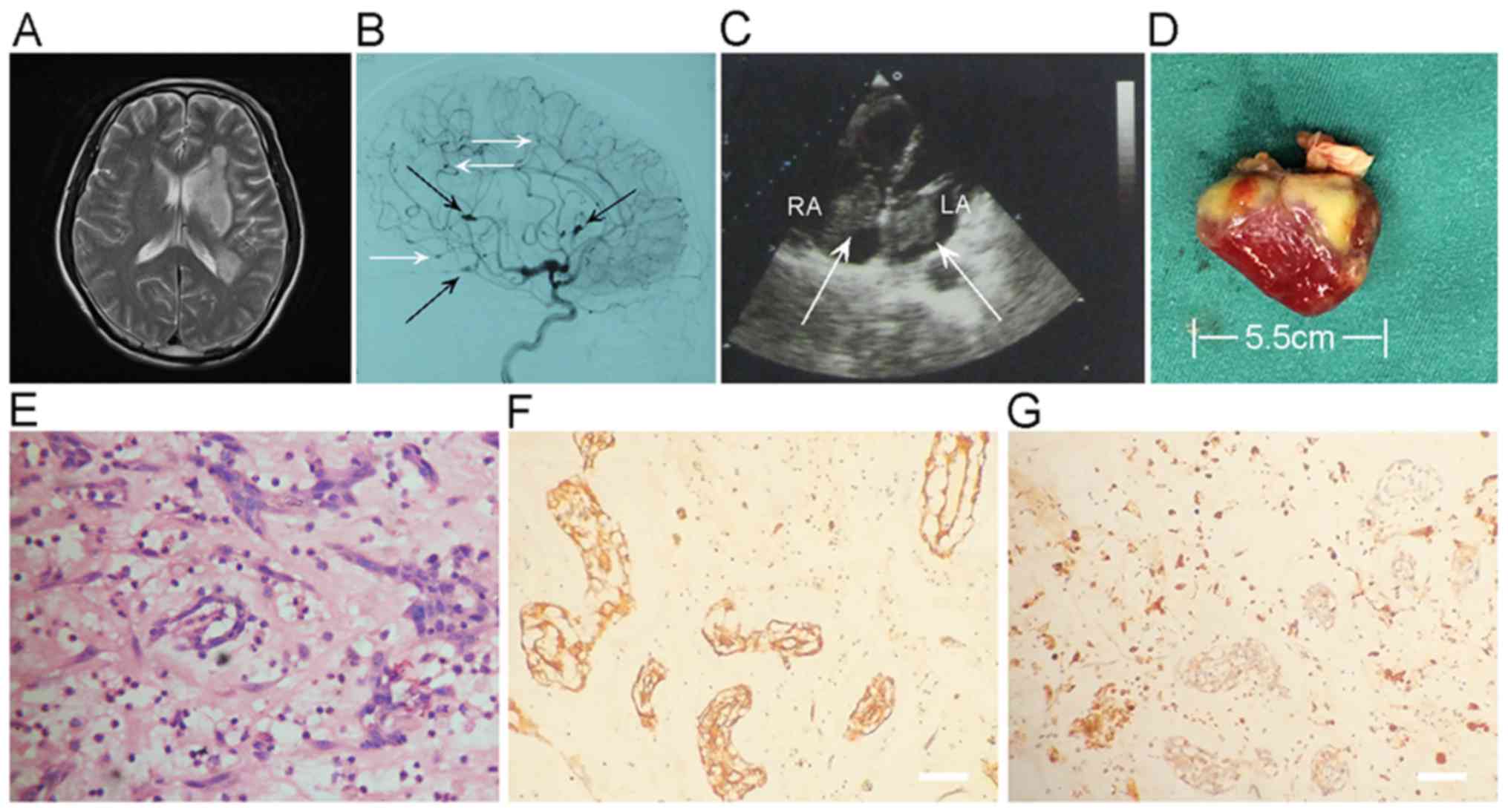
Neuroimaging findings
An example of combined cerebral infarction and
intracranial aneurysm in a myxoma case is shown in Fig. 1. An emergency MRI of the brain
demonstrated multifocal punctate acute infarction throughout the
left temporal, basal ganglia and centrum semiovale (Fig. 1A). Digital subtraction angiography
showed multiple typical distal fusiform and saccular aneurysms in
left internal carotid arterial territories (Fig. 1B). Cardiac ultrasound revealed masses
in the left and right atria that were resected, and identified as
double atrial myxomas. The left atrium tumor and right atrium tumor
measure 60×19 and 43×16 mm, respectively (Fig. 1C). The excised left atrium myxoma
presents as an irregular, and measures 55×19×15 mm (Fig. 1D). Hematoxylin and eosin (H&E)
stain disclosed typical atrial myxoma cells, embedded in a loose
myxoid matrix (Fig. 1E).
Immunohistochemical analysis of resected atrial myxoma showed
positivity for CD34 (Fig. 1F) and
CD68 (Fig. 1G).
Myxoma characteristics
No significant differences were found in the
diameter of myxomas between the embolic and non-embolic groups
(4.26±1.6 vs. 3.18±1.1 cm; P=0.3720). However, significantly more
individuals in the embolic group had large myxomas (>5 cm)
compared with the non-embolic group (47.06 vs. 20.35%, P=0.0230).
Microscopy revealed 10 myxomas with intratumoral hemorrhage
(58.82%) in the embolic group, while 61 myxomas showed intratumoral
hemorrhage (53.98%) in the non-embolic group (P=0.4510). Myxoma
attachment was similar in both groups (1.0±0.2 vs. 1.1±0.4 cm;
P=0.1335; Table III). However,
irregular surface of myxomas was markedly more frequent in the
embolic group compared with patients with no embolism (76.47 vs.
36.28%, P=0.0273).
| Table III.Atrial myxoma characteristics: Embolic
vs. non-embolic groups. |
Table III.
Atrial myxoma characteristics: Embolic
vs. non-embolic groups.
| Myxoma
characteristics | Embolic group, n=17
(%) | Non-embolic group,
n=113 (%) | P-value |
|---|
| Tumor diameter
(cm), mean ± SD | 4.26±1.6 | 3.18±1.1 | 0.3720 |
| >5 cm, n | 8 (47.06) | 23 (20.35) | 0.0230 |
| Intratumoral
haemorrhage | 10 (58.82) | 61 (53.98) | 0.4510 |
| Attachment diameter
(cm), mean ± SD | 1.0±0.2 | 1.1±0.4 | 0.1335 |
| >1 cm, n | 7 (41.18) | 51 (45.13) | 0.4750 |
| Irregular surface,
n | 13 (76.47) | 41 (36.28) | 0.0273 |
Discussion
Atrial myxoma is found in the left atrium in 75% of
patients in the solid or papillary form (2). In this study, ages (age at onset of
30–60 years) and sex distribution (female predominance) of atrial
myxoma cases corroborated previous reports (6,7).
Neurological symptoms of atrial myxoma might appear before or at
the time of primary tumor diagnosis. They were found in 16.9% of
patients, a rate lower than previously reported (4,8).
In this study, ischemic cerebral infarction was the
most commonly encountered neurologic complication of atrial myxoma.
Although embolism is a relatively common precursor of cerebral
infarction in the youth, the majority of existing reports merely
describe isolated cases. The present series assessed 22 patients
with neurological manifestations associated with myxoma, including
15 with ischemic cerebral infarction. These data differ from
previous series, which showed TIA as the most frequent neurological
presentation of atrial myxoma (9).
Nevertheless, multiple studies found percentages of ischemic
cerebral infarction similar to the present values (4,5,10). This discrepancy may be associated with
different pathological characteristics of atrial myxomas. This
study showed that myxomas with irregular surface were more prone to
embolism. Fracturing of small myxoma fragments is considered to be
responsible for embolic events. Indeed, the irregular surface
contributes to myxoma fragmentation and increases interactive
areas, resulting in embolism (5,11,12).
Additionally, oncotic aneurysms are late signs of
atrial myxoma. In patients with cardiac myxoma, oncotic aneurysms
are caused by metastatic emboli, which invade and disrupt the
vessel wall (13,14). In the current study, 1 patient
presented with recurrent cerebral infarction caused by a partially
thrombosed 1.7 cm myxomatous oncotic aneurysm. Previous studies
have examined endovascular embolization, chemotherapy, and
radiation in the treatment of such aneurysms, and the findings are
equivocal (15–20). Therefore, the optimal treatment of
myxomatous oncotic aneurysms needs to be established.
Atrial myxoma causes cerebral infarction, but can be
treated. In 22 cases in this series, neurological manifestations
were found as initial sign of atrial myxoma. In 14/15 patients with
cerebral infarction, tumor diagnosis occurred during the hospital
stay, with surgical removal within 1 month. All patients were
diagnosed by echocardiography, which was used routinely after a
stroke of uncertain cause. There was no recurrence of atrial myxoma
in the 22 subjects that underwent surgical treatment during
follow-up (6 months to 12 years). Our findings advocate for early
diagnosis and surgical resection of atrial myxoma before further
embolic or cardiac complications occur.
In summary, atrial myxomas frequently present with
cerebral infarction in individuals without known cardiovascular
risk factors. The middle cerebral artery is more commonly
concerned. Irregular surface of myxomas appears to be related to
embolic events. Echocardiography could improve diagnosis and early
treatment of atrial myxomas.
Acknowledgments
Help and advice from all members of the Clinical
Laboratory Center of the Affiliated Hospital of Hainan Medical
University is acknowledged.
Funding
The present study was funded by the National Natural
Science Foundation of China (grant no. 81460184), the Health and
Family Planning Commission of Hainan Province, China, Scientific
Research Project (2014–07) and the Social Development Project of
Science and Technology in Hainan Province (grant no. 2015SF13).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
XYW, YMC, XPL and QFL conceived and designed the
study. XYW, YMC, LLY and HBZ performed the experiments. XYW, ZBC
and YMC analyzed the data. LM and SRW assisted in the study design
and discussed and interpreted the data. QFL and XYW wrote the
manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the First
Affiliated Hospital of Hainan Medical University's Institutional
Review Board. Individual consent was waived by the committee
because of the retrospective nature of the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gošev I, Paić F, Durić Z, Gošev M, Ivčević
S, Jakuš FB and Biočina B: Cardiac myxoma the great imitators:
Comprehensive histopathological and molecular approach. Int J
Cardiol. 164:7–20. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Liao WH, Ramkalawan D, Liu JL, Shi W, Zee
CS, Yang XS, Li GL, Li J and Wang XY: The imaging features of
neurologic complications of left atrial myxomas. Eur J Radiol.
84:933–939. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thyagarajan B, Kumar MP, Patel S and
Agrawal A: Extracardiac manifestations of atrial myxomas. J Saudi
Heart Assoc. 29:37–43. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Aiello VD and de Campos FP: Cardiac
Myxoma. Autopsy Case Rep. 6:5–7. 2016. View Article : Google Scholar
|
|
5
|
Yin L, Wang J, Li W, Ling X, Xue Q, Zhang
Y and Wang Z: Usefulness of CHA2DS2-VASc scoring systems for
predicting risk of perioperative embolism in patients of cardiac
myxomas underwent surgical treatment. Sci Rep. 6:393232016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rios RE, Burmeister DB and Bean EW:
Complications of atrial myxoma. Am J Emerg Med. 34:2465.e1–2465.e2.
2016. View Article : Google Scholar
|
|
7
|
Andreu Perez J, Parrilla G, Arribas JM,
García-Villalba B, Lucas JJ, Navarro Garcia M, Marín F, Gutierrez F
and Moreno A: Neurological manifestations of cardiac myxoma:
Experience in a referral hospital. Neurologia. 28:529–534.
2013.PubMed/NCBI
|
|
8
|
He DK, Zhang YF, Liang Y, Ye X, Wang C,
Kang B and Wang ZN: Risk factors for embolism in cardiac myxoma: A
retrospective analysis. Med Sci Monit. 21:1146–1154. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wang Z, Chen S, Zhu M, Zhang W, Zhang H,
Li H, Yuan G and Zou C: Risk prediction for emboli and recurrence
of primary cardiac myxomas after resection. J Cardiothorac Surg.
11:222016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Spartalis M, Tzatzaki E, Spartalis E,
Moris D, Athanasiou A, Kyrzopoulos S, Tsiapras D, Kalogris P and
Voudris V: Atrial myxoma mimicking mitral stenosis. Cardiol Res.
8:128–130. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
11
|
Singh S, Tripathy MP, Mohanty BB and
Biswas S: Sporadic multicentric right atrial and right ventricular
myxoma presenting as acute pulmonary thromboembolism. Heart Views.
17:19–22. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sabzi F and Faraji R: Preoperative emboli
in a pregnant woman with myxoma. Iran J Med Sci. 41:345–349.
2016.PubMed/NCBI
|
|
13
|
Ekinci EI and Donnan GA: Neurological
manifestations of cardiac myxoma: A review of the literature and
report of cases. Int Med J. 34:243–249. 2004. View Article : Google Scholar
|
|
14
|
Brinjikji W, Morris JM, Brown RD, Thielen
KR, Wald JT, Giannini C, Cloft HJ and Wood CP: Neuroimaging
findings in cardiac myxoma patients: A single-center case series of
47 patients. Cerebrovasc Dis. 40:35–44. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lee SJ, Kim JH, Na CY and Oh SS: Eleven
years' experience with Korean cardiac myxoma patients: Focus on
embolic complications. Cerebrovasc Dis. 33:471–479. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Alvarez-Sabin J, Lozano M, Sastre-Garriga
J, Montoyo J, Murtra M, Abilleira S and Codina A: Transient
ischaemic attack: A common initial manifestation of cardiac
myxomas. Eur Neurol. 45:165–170. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Isogai T, Yasunaga H, Matsui H, Tanaka H,
Hisagi M and Fushimi K: Factors affecting in-hospital mortality and
likelihood of undergoing surgical resection in patients with
primary cardiac tumors. J Cardiol. 69:287–292. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee TH, Huang SC, Su TM, Yang KY and Rau
CS: Multiple cerebral aneurysms and brain metastasis from primary
cardiac myxosarcoma: A case report and literature review. Chang
Gung Med J. 34:315–319. 2011.PubMed/NCBI
|
|
19
|
Saffie P, Riquelme F, Mura J, Urra A,
Passig C, Castro Á and Illanes S: Multiple myxomatous aneurysms
with bypass and clipping in a 37-year-old man. J Stroke Cerebrovasc
Dis. 24:e69–e71. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Al-Said Y, Al-Rached H, Baeesa S, Kurdi K,
Zabani I and Hassan A: Emergency excision of cardiac myxoma and
endovascular coiling of intracranial aneurysm after cerebral
infarction. Case Rep Neurol Med. 2013:8392702013.PubMed/NCBI
|