Introduction
Atypical fibroxanthoma (AFX) is a comparably rare
dermal neoplasm with only 3,000 cases reported in the literature so
far (1). This tumor predominantly
develops at sun-exposed areas of the human body with emphasis on
the head and neck region, and typically affects more men than women
with a median age above 60 years (1,2). While AFX
can often show a large extension in the superficial skin layers, an
invasion of deeper structures e.g., blood or lymph vessels,
subcutaneous muscles or peripheral nerves is usually not found
resulting in a classification as benign or semi-malignant tumor
(3,4).
Hence, the prognosis of AFX patients is excellent with a median
20-year disease-specific survival rate of 97.8% (1). After its first description in 1963, much
effort was spent to better understand the tumorigenesis and
molecular biology of this tumor entity including
immunohistochemical analyses, electron microscopy, comparative
genomic hybridization and next generation sequencing (5,6). However,
the pathogenesis of AFX is still unclear with keratinocytes,
fibroblasts and myofibroblasts having been discussed as potential
cells of origin (7,8). Since this tumor shows a highly
heterogeneous histological structure with tumor cells ranging from
spindle and epithelioid to multinucleated cells and a variably
structured extracellular matrix, the histological diagnosis is
challenging with undifferentiated pleomorphic sarcoma, malignant
fibrous histiocytoma, dedifferentiated squamous cell carcinoma,
dermatofibrosarcoma protuberance and leiomyosarcoma as differential
diagnoses (1,9). Immunohistochemical markers that can help
to differentiate AFX from other tumor entities are CD99, S-100,
CD34, cytokeratin, desmin, CD10, vimentin, HMB-45, CD68 and p63
(8–12). However, a disease-specific marker as
well as a prognostic marker indicating a higher risk of recurrence
or distant metastasis is still missing (1,3,4). In 2010 an association to Merkel Cell
Polyomavirus was detected in 17% of all AFXs examined (13). Importance of this finding has to be
further elucidated.
The SEC62 gene located at chromosomal region
3q26.2 encodes for a transmembrane protein of the endoplasmic
reticulum (ER) that forms a heterotrimeric complex with the protein
translocation pore and intracellular calcium channel Sec61 as well
as Sec63 (14,15). Under physiological conditions, Sec62
is involved in the posttranslational transport of short secretory
and transmembrane precursor proteins, possibly through its direct
interaction with Sec61 and the ribosome (16–18). Apart
from protein transport, Sec62 was shown to influence the passive
calcium efflux through the Sec61 channel into the cytosol in an
inhibitory manner (19–22). An amplification of the SEC62
encoding region 3q26.2 as well as an overexpression of the
SEC62 gene was observed in various cancer entities including
head and neck cancer (23,24), prostate cancer (25), esophageal cancer (26), cervical cancer (27,28),
ovarian cancer (29) and non-small
cell lung cancer (30). For NSCLC and
HNSCC, high SEC62 expression level was a predictor of poor
clinical outcome and significantly correlated with a positive lymph
node status (31–33). In hepatocellular cancer, high
SEC62 expression levels were correlated with a higher risk
of recurrence after surgical treatment (34). Beneath its role as a prognostic
biomarker, Sec62 was shown to influence tumor cell biology by
stimulating cancer cell migration, invasion and enabling tumor
cells to recover from ER stress by a mechanism called
‘recovER-phagy’ (21,35–39). These
effects can explain how tumor cells profit from an increased
SEC62 expression level and might be responsible for the poor
prognosis of SEC62 overexpressing tumors. Based on the
finding that the stimulation of cancer cell migration by Sec62 is
probably mediated through its influence on the calcium homeostasis
at the ER, the calmodulin antagonist trifluoperazine (TFP) could be
identified as a potent agent to antagonize the calcium effect of
Sec62 and thereby inhibiting Sec62 mediated cancer cell migration
(21). Hence, TFP represents a
promising agent for an antimetastatic therapy in SEC62
overexpressing tumors.
As for AFX, there exist neither reliable
immunohistochemical markers enabling discrimination from other
related sarcomatoid tumors nor prognostic biomarkers indicating a
higher risk of recurrence or distant metastasis, we investigated in
our study the expression of 3q oncogene SEC62 in 41 AFX
cases and correlated the SEC62 expression level with the
patients' clinical and viral data and the pathological
characteristics of the tumors.
Materials and methods
General
Investigations were performed after approval by a
local Human Investigations Committee, approval no. 281/10
(Ethikkomission der Ärztekammer des Saarlandes).
Patient characteristics and tissue
samples
AFXs were retrieved from the histopathology archives
of the department of dermatology. A period from 2006 to 2016 was
investigated. Inclusion criteria for the study were availability of
slides and blocks as well as tumors treated surgically by excision
with curative intention. A total of 41 AFXs of 40 patients were
investigated in this study. The following clinical and
histopathologic features were evaluated: Sex, age and size, mitotic
count, presence of necrosis, ulceration, vascular invasion as well
as invasion depth and Clark level. Follow-up information was
obtained from hospital medical records of the referring clinicians.
Details of clinicopathological characteristics are summarized in
Table I. Detailed histopathologic
data is given in Table II.
 | Table I.Clinical data of all patients
enrolled in the present study. |
Table I.
Clinical data of all patients
enrolled in the present study.
| Patient no. | Age at time of
diagnosis | Sex | Localization | Tumor diameter | Relapse | Distant
metastases | Death |
|---|
| 1 | 63 | M | Head | 4.00 | No | No | No |
| 2 | 78 | M | Head | N.A. | No | No | No |
| 3 | 83 | M | Upper
extremity | 1.00 | No | No | Yes |
| 4 | 84 | F | Head | 1.00 | No | No | No |
| 5 | 81 | M | Face | 0.06 | No | No | No |
| 6 | 77 | M | Head | 0.75 | No | No | No |
| 7 | 85 | M | Head | 4.00 | No | No | No |
| 8 | 81 | M | Head | 0.49 | No | No | Yes |
| 9 | 65 | M | Head | N.A. | No | No | No |
| 10 | 81 | M | Head | 1.00 | No | No | No |
| 11 | 83 | F | Head | N.A. | No | No | No |
| 12 | 78 | M | Head | 1.00 | No | No | Yes |
| 13 | 65 | M | Head | 1.65 | No | No | No |
| 14 | 81 | M | Head | N.A. | No | No | No |
| 15 | 81 | F | Head | 3.00 | No | No | No |
| 16 | 78 | M | Upper
extremity | 4.00 | Yes | No | No |
| 17 | 79 | M | Head | 0.25 | No | No | No |
| 18 | 79 | M | Head | 2.50 | No | No | Yes |
| 19 | 84 | M | Head | N.A. | No | No | No |
| 20 | 72 | F | Lower
extremity | 1.00 | No | No | No |
| 21 | 87 | M | Head | N.A. | No | No | No |
| 22 | 90 | F | Head | 4.00 | Yes | No | No |
| 23 | 92 | F | Head | 5.00 | No | No | No |
| 24 | 79 | M | Head | N.A. | No | No | No |
| 25 | 87 | M | Head | 40.00 | No | No | No |
| 26 | 80 | F | Face | 9.00 | No | No | No |
| 27 | 88 | M | Head | 25.00 | Yes | No | Yes |
| 28 | 79 | M | Head | 9.00 | No | No | No |
| 29 | 78 | M | Head | N.A. | No | No | No |
| 30 | 76 | M | Head | 5.75 | No | No | No |
| 31 | 80 | M | Head | 22.00 | No | No | No |
| 32 | 89 | M | Head | 9.00 | No | No | No |
| 33 | 87 | M | Head | 3.00 | No | No | No |
| 34 | 83 | M | Head | 9.00 | No | No | No |
| 35 | 84 | M | Head | N.A. | No | No | Yes |
| 36 | 78 | M | Head | 5.00 | No | No | No |
| 37 | 73 | M | Face | 0.32 | No | No | No |
| 38 | 72 | M | Lower
extremity | 2.70 | No | No | No |
| 39 | 62 | M | Head | 1.00 | No | No | No |
| 40 | 88 | M | Head | N.A. | No | No | No |
| 41 | 89 | F | Face | 1.00 | No | No | No |
| Table II.Histomorphologic data of all atypical
fibroxanthomas of the present study. |
Table II.
Histomorphologic data of all atypical
fibroxanthomas of the present study.
| Patient no. | Vertical tumor
depth, mm | Clark level | Necrosis | Ulceration | Mitotic count | Vascular
invasion | MCPyV DNA | SEC62
Immunoscore |
|---|
| 1 | 8.35 | 5 | Yes | Yes | 8.70 | No | + | 9.0 |
| 2 | 2.68 | 3 | No | Yes | 3.55 | No | – | 2.6 |
| 3 | 2.20 | 3 | No | No | 2.40 | No | + | 6.0 |
| 4 | 2.90 | 4 | No | Yes | 4.40 | No | – | 8.3 |
| 5 | 2.20 | 5 | No | No | 1.50 | No | – | N.A. |
| 6 | 2.40 | 4 | No | No | 2.70 | No | – | N.A |
| 7 | 2.16 | 3 | No | Yes | 4.60 | No | – | 5.6 |
| 8 | 5.70 | 2 | No | Yes | 5.90 | No | – | 4.0 |
| 9 | 2.16 | 3 | No | No | 4.00 | No | – | 4.3 |
| 10 | 7.20 | 5 | Yes | Yes | 4.80 | No | – | 1.0 |
| 11 | 8.00 | 5 | No | Yes | N.A. | No | – | 6.3 |
| 12 | 3.10 | 4 | No | No | 4.20 | No | – | 11.0 |
| 13 | 6.90 | 4 | No | No | 4.80 | No | – | 9.3 |
| 14 | 4.08 | 5 | No | Yes | 5.70 | No | – | 10.0 |
| 15 | 7.50 | 5 | No | Yes | 7.50 | No | – | 8.0 |
| 16 | 5.80 | 5 | No | Yes | 5.70 | No | – | 8.0 |
| 17 | 1.29 | 4 | No | No | 2.40 | No | – | 8.6 |
| 18 | 4.80 | 4 | Yes | Yes | 1.10 | No | – | 12.0 |
| 19 | 14.00 | 2 | No | Yes | 8.90 | No | – | 10.0 |
| 20 | 2.40 | 2 | No | Yes | 3.70 | No | – | 6.6 |
| 21 | 6.52 | 5 | No | Yes | 1.00 | No | – | 3.6 |
| 22 | 5.28 | 5 | No | Yes | 5.70 | No | – | 7.3 |
| 23 | 2.60 | 4 | No | Yes | 3.80 | No | + | 8.0 |
| 24 | 4.08 | 4 | Yes | Yes | 5.60 | No | + | 11.0 |
| 25 | 40.00 | 5 | Yes | Yes | N.A. | No | – | 10.0 |
| 26 | 4.80 | 5 | No | Yes | 50.40 | No | – | 7.0 |
| 27 | 2.90 | 4 | No | Yes | 5.10 | No | – | 9.0 |
| 28 | 4.08 | 4 | No | No | 6.10 | No | – | 6.0 |
| 29 | 2.68 | 3 | No | Yes | 3.50 | No | – | 6.6 |
| 30 | 9.50 | 4 | No | No | 5.60 | No | – | 11.0 |
| 31 | 5.80 | 4 | No | Yes | 3.70 | No | – | 9.0 |
| 32 | 7.20 | 5 | No | Yes | 8.40 | No | – | 6.0 |
| 33 | 7.68 | 5 | No | No | 7.00 | No | – | 11.0 |
| 34 | 4.27 | 3 | Yes | Yes | 10.20 | No | – | 12.0 |
| 35 | 4.17 | 5 | No | Yes | 7.90 | No | – | 6.6 |
| 36 | 6.50 | 5 | No | Yes | 4.90 | No | – | 6.6 |
| 37 | 4.80 | 4 | No | Yes | 3.30 | No | – | N.A. |
| 38 | 1.90 | 3 | No | No | 3.60 | No | – | N.A. |
| 39 | 4.30 | 5 | No | No | 2.50 | No | – | N.A. |
| 40 | 6.40 | 5 | No | Yes | 3.80 | No | – | N.A. |
| 41 | 2.00 | 3 | No | No | 4.80 | No | – | N.A. |
Immunohistochemical analysis
FFPE tissue sections were obtained and used for
immunohistochemical staining of Sec62. After omitting the first
three 10-µm sections, consecutive 4-µm sections were obtained using
a Leica RM 2235 rotary microtome (Leica Microsystems, Wetzlar,
Germany), transferred onto Superfrost Ultra Plus microscope slides
(Menzel-Gläser, Braunschweig, Germany) and dried in an incubator at
37°C overnight. Upon deparaffinization, heat-induced epitope
retrieval was performed by incubation in 10 mM citrate buffer (pH
6.0) at 95°C for 30 min. Unspecific protein binding sites were
blocked with 3% BSA (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany)
in PBS for 30 min at room temperature. Subsequently, primary
antibody incubation was performed using an affinity-purified
polyclonal rabbit anti-peptide antibody directed against the C
terminus of human Sec62 (self-made). For each staining series, a
specimen taken from a subcutaneously grown tumor in mice after
local injection of UM-SCC1 cells (SEC62 overexpressing cell
line) was used as positive control as well as negative controls by
omitting the primary antibody. Visualization was performed using
the REAL™ detection system Alkaline Phosphatase (Dako
Agilent Technologies, Glostrup, Denmark), according to the
manufacturer's instructions, and the slides were counterstained
with hematoxylin (Dako Agilent Technologies).
Sec62-immunoreactivity was evaluated using an immunoreactive score
(IRS) according to Remmele and Stegner (40) with values ranging from 0 to 12. All
immunohistochemical stainings were valued by three experienced
examiners including one dermatopathologist and the mean values of
the three scorings were used for statistical analysis. 34/41 cases
were available for immunohistochemistry with sec62.
Specific detection of mitoses was performed
using phosphohistone H3 (pHH3; polyclonal antibody, Cell
Marque® no. 369A) at a dilution of 1:100 (pre-treatment
for 30 min in a steamer) in accordance with the manufacturer's
protocol. Mitotic figures labeled with pHH3 were twice counted in
10 high-power-fields within the ‘hot spot’ of the tumour and mean
of mitoses was calculated.
MCPyV-DNA PCR
MCPyV-DNA-specific PCR was performed for all FFPE
tissue specimens (n=41). DNA was extracted from the FFPE tissue
samples using a QIAamp DNA FFPE Tissue kit (Qiagen N.V., Hilden,
Germany) according to the manufacturer's instructions.
MCPyV-DNA-PCR was performed with the LightCycler 2.0 instrument
(Roche Diagnostics GmbH, Mannheim, Germany) using MCPyV-specific
primers LT3F (5′-ttg tct cgc cag cat tgt ag-3′) and LT3R (5′-ata
tag ggg cct cgt caa cc-3′) described by Feng et al (41). Cycling conditions were 94°C for 3 min,
followed by 45 PCR cycles with denaturation at 94°C for 45 sec,
annealing at 58°C for 30 sec, elongation at 72°C for 45 sec and
finished by a last elongation at 72°C for 15 min. After
amplification, the PCR products (10 µl) were separated on 2%
agarose gels and visualized by ethidium bromide staining.
Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) PCR served as an
internal control and was performed in parallel for each sample as
described previously by Sperling et al (42).
Statistical analysis
Beside descriptive statistical analyses
(frequencies, mean and standard deviation) the comparison of groups
was performed with the Mann-Whitney U test resp.
Kruskal-Wallis-Test. The analyses were executed with SPSS v. 17.0
(SPSS, Inc., Chicago, IL, USA) and GraphPad Prism 7.0 (GraphPad
Software, Inc., La Jolla, CA, USA). P<0.05 was considered to
indicate a statistically significant difference.
Results
Clinical and pathological
characteristics of patients
Details of clinicopathological characteristics are
summarized in Table I. Detailed
histopathologic data is given in Table
II. 33 male and 8 female patients were included in this study.
Age at time of diagnosis ranged from 62 to 92 years, with a mean of
79.9 years. Clinical information on exact localization of tumors
was available in all tumors. 90.2% (37/41) of tumors were located
in the head and neck area, while 4 where located at the extremities
(9.7%). Tumor diameter ranged from 0,06 to 40 cm2 with a
mean of 5.7 cm2.
One female patient developed 2 separate tumors, when
she was 90 years old and the second when she was 92 of age. Relapse
of AFXs was seen in three patients (7.3%), distant metastases did
not occur in any patient of this cohort. 6/40 (14.6%) patients died
within observation period. Due to low number of cases we did not
differentiate between the several morphologic variants of AFX, that
have been described (spindle-cell nonpleomorphic AFX, clear-cell
AFX, pigmented, myxoid, osteoclast-like giant cell rich AFX
keloidal and granular cell AFX)43. Invasion depth of all
tumors ranged from 1.29 to 40 mm with a mean of 5.6 mm. In analogy
to Clark Level (CL) in malignant melanoma (CL I-melanoma in
situ, CL II-infiltration of the upper part of the papillary
dermis, CL III-expansion of melanoma cells into the papillary
dermis and upper reticular dermis, CL IV-infiltration of the
reticular dermis and CL V-infiltration of subcutis44) we
analyzed invasion of anatomic levels of the skin: CL I is not
applicable per definitionem as AFXs are primary dermal tumors. CL
II was seen in 7% (3/41), CL III was observed in 19% (8/41).
Thirteen cases showed CL IV (31%) and 41% (17/41) of the cases
displayed extension to subcutaneous tissue. Tumor necrosis was
observed in 14.3% (6/41), ulceration of the overlying epidermis was
seen in 69% (28/40). Vascular invasion was seen in none of the
cases of this cohort. Merkel Cell Polyomavirus (MCPyV)-DNA was
detected in 4 cases (9.7%). As a trend, three of these cases were
male with ulcerated tumors and one patient was female. One of these
4 patients died within observation period. A mean of 5.9 mitoses
could be detected in 10 hotspot areas of every tumor.
Expression analysis of SEC62
oncogene
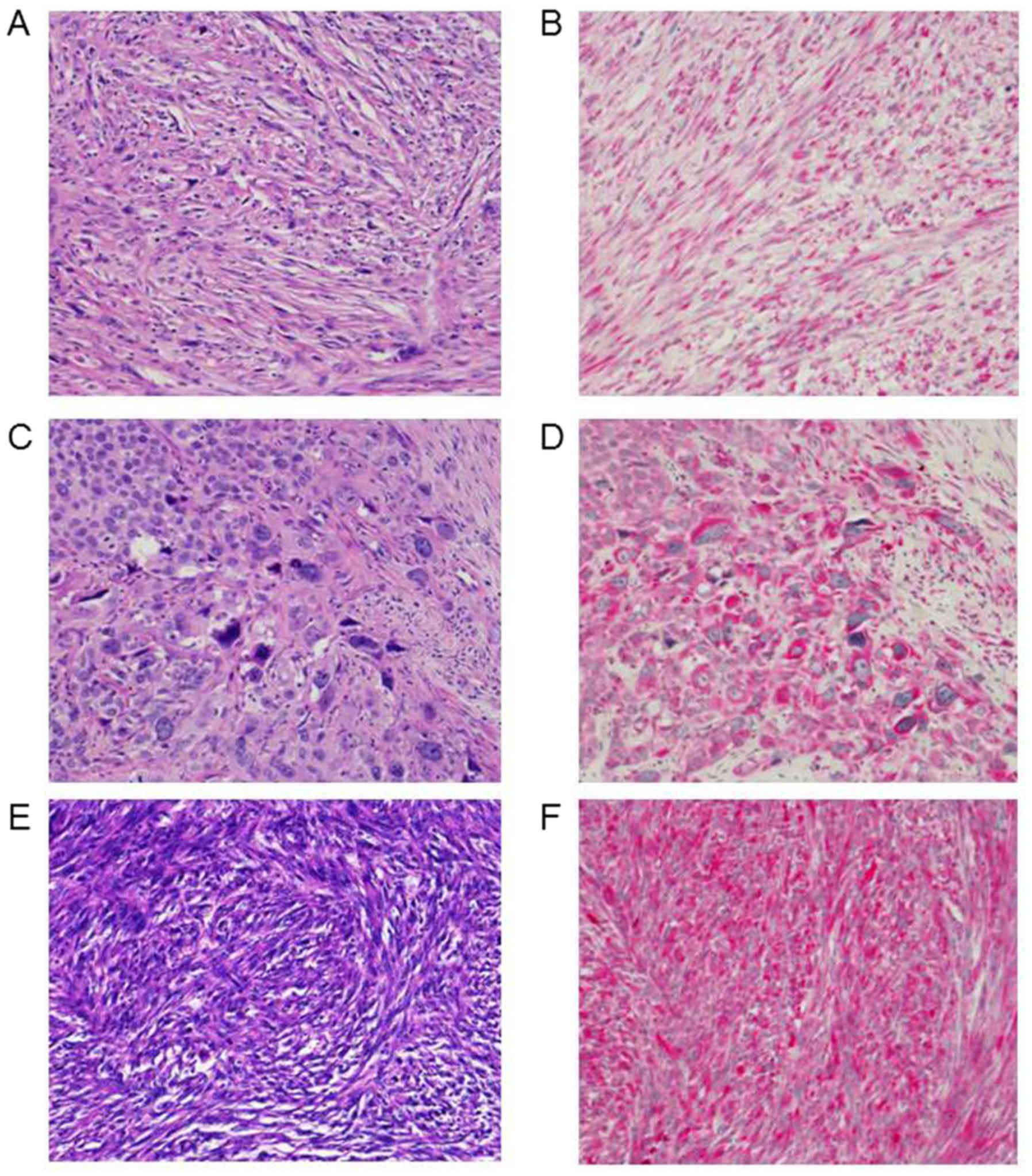
Immunoscore of 3q oncogene SEC62 could be
investigated in 34 cases of all AFXs (Fig. 1). In 100% (34/34) of the samples
cytoplasmatic expression of 3q oncogene SEC62 within the
mesenchymal tumor cells was seen. Mean score was 7.7 with a minimum
of 1 and a maximum score of 12. Exemplary cases of distinct
Sec62-IRS-scores are shown in Fig. 1.
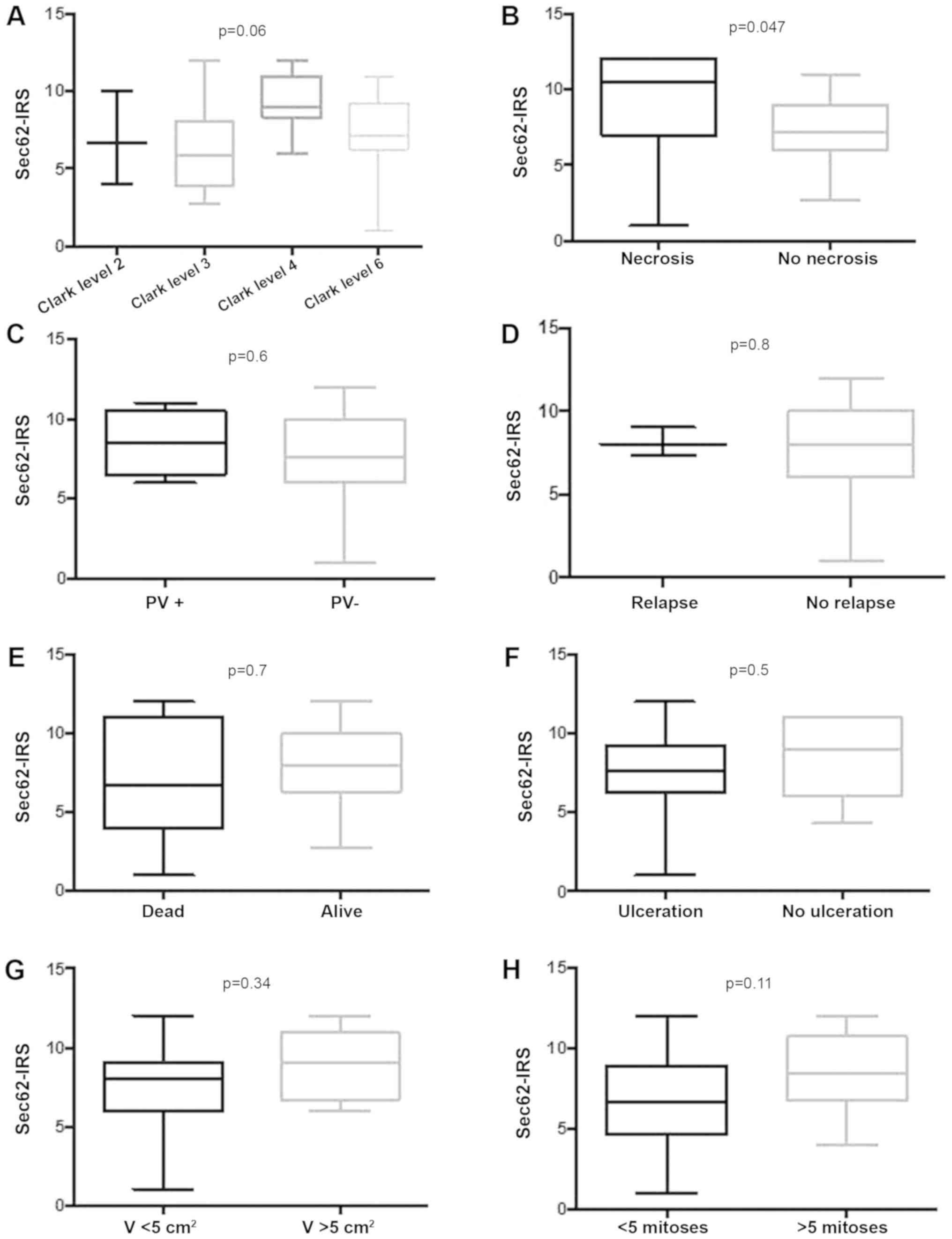
Intriguingly, we found significantly higher expression of
SEC62 in cases of AFX with tumor necrosis (Fig. 2G), while there was no statistically
relevant dependency on invasion depth, ulceration, relapse of
tumor, distant metastases or death due to tumor (Fig. 2). Hence, tendency of higher
SEC62-IRS-scores were found for tumors with higher Clark
levels and a tumor size greater 5 cm2, although reaching
no significance level (Fig. 2G).
Analysis of MCPyV DNA
MCPyV DNA positive cases did not show any
statistically significant differences in 3q oncogene SEC62
expression, probably due to low number of positive cases (Fig. 2C). There was also no dependency
between invasion depth of the tumor in correlation with
virus-positive cases, Clark level, necroses, ulceration, relapse or
death due to disease (data not shown).
Discussion
AFX is a mesenchymal neoplasm, rarely seen in daily
routine, even in dermatology and dermatopathology units.
Relationship of AFX and pleomorphic dermal sarcoma (PDS) is still
not clearly identified (43). As AFX
is a diagnosis of exclusion, it is mandatory to apply strict
diagnostic criteria that include diligent immunohistochemical
workup (8–12).
There is growing evidence that viruses play an
important role in tumorigenesis, mainly in immunosuppressed
patients and an estimated 20% of global cancer burden is related to
viral infections (44). Merkel Cell
Polyomavirus (MCPyV) was recently detected in Merkel cell carcinoma
(MCC) and approximately 91.2% of MCC are MCPyV-positive (41,45).
Intriguingly, 85% of all healthy adults and 58% of children younger
than 10 years are MCPyV-positive displaying a high seroprevalence
of MCPyV (46). In 2010 MCPyV was
initially detected within samples of AFX with an incidence of 17%
in this study (13). The authors
concluded that MCPyV may act as a cofactor in the tumorigenesis of
a subset of AFXs (13). In our cohort
we were able to detect MCPyV-DNA in 9.7% only. Comparable to Andres
et al, virus-positive AFXs were detected predominantly in
older males with ulcerated tumors (13), but with no correlation to invasion
depth or tumor size in our study. At the moment, the role of MCPyV
in AFXs remains unclear. Due to high seroprevalence of MCPyV and
possibility of viral persistence in several compartments of the
body (body fluids, tissue biopsies, several organ specimens) its
role in tumorigenesis of AFX remains to be determined (46). MCPyV is frequently detected on healthy
human skin (46,47). Therefore, it cannot be excluded that
MCPyV detection may only be a bystander phenomenon without clinical
implication (46). Intriguingly, in
2016 Liu and colleagues managed to identify human dermal
fibroblasts as the primary skin cell type supporting MCPyV gene
expression and productive replication after infectious entry
(48). Hence, they showed MCPyV
infection is promoted via induction of matrix metalloproteinase
(MMP) genes by the WNT/β-catenin signaling pathway. It is already
known that UV radiation stimulates the WNT signaling and MMP
expression (48,49). Taken together molecular pathways with
connection to chronic UV exposure and host cell of MCPyV, our
findings indicate towards a pathogenetic relationship between
infection and AFX. Though, number of MCPyV cases actually is too
low to draw clear conclusions.
Prognostic or predictive biomarkers do not exist for
AFXs, neither do any histomorphologic parameters exist, that
predict clinical outcome and metastatic potential. Of greater
importance concerning prognosis than histomorphologic parameters is
surgical margin status, as clear margins are associated with
improved clinical outcome (50).
In contrast, histomorphologic parameters of
prognostic relevance are well defined for malignant melanoma:
Histogenetic subtype, Breslow thickness, Clark level, mitotic
figures, ulceration, regression and others (51). Results of multivariate analysis of
these factors in large melanoma cohorts are reflected in the AJCC
(American Joint Committee on Cancer) for melanoma staging and
classification from 2009 (52).
Hence, in this study we were not able to identify clinical, viral
or histomorphological parameters (displaying worse prognosis for
instance in malignant melanoma) that correlated with clinical
outcome of the patients. Discussion concerning differentiation of
AFX from pleomorphic sarcoma is still ongoing.
For the 3q encoded SEC62 gene, an
overexpression was found in a variety of human cancers (21,25,31,32,36,37,39)
and in non-small cell lung cancer, cervical cancer as well as head
and neck cancer, high SEC62 expression correlated with a
significantly shorter overall survival. These findings indicate a
general role of SEC62 as an oncogene in the pathogenesis of
human cancer and emphasize the role of SEC62 expression
level as a prognostic factor in various cancer entities (53). In our study, we found markedly
increased SEC62 expression levels in the lesional tissue
compared with the adjacent healthy squamous epithelium in the vast
majority of cases pointing towards an oncogenic function of
SEC62 in AFX, as well. While significantly higher
SEC62 expression levels were found in AFX samples that
showed intratumoral necrotic areas, which is known to be an adverse
prognostic factor in this entity (1),
we found no significant correlation of SEC62 expression with
other clinical and histopathological features including the
patients' survival. However, given the comparably low number of
cases and the only marginal portion of cases of death, these data
do not exclude a potential prognostic relevance of Sec62 in AFX
which is further indicated by the association of high SEC62
expression levels with advanced Clark levels and tumor size (see
Fig. 2A and G). As it is recommended
that tumors displaying prognostically unfavorable features
(extension to subcutaneous fat, corresponding to Clark level V,
perineural invasion or necrosis), should be diagnosed as PDS.
Hence, high expression levels of SEC62 could serve as a
diagnostic parameter for distinction between AFX and PDS. This has
to be further investigated with higher number of cases.
Regarding the functional role of Sec62 in tumor cell
biology, it was shown that high Sec62 levels can stimulate the
migration of tumor cells (21,31,39)
as well as their resistance to ER stress (37). If comparable effects can be seen when
SEC62 is overexpressed in AFX cells is a remaining question,
which will be ambitious to answer keeping in mind the extremely
rare metastasis rate of AFX (1,54) and the
fact that there are no established AFX cell lines available.
Acknowledgments
The authors would like to thank Mrs. Anne Kerber,
Mrs. Alexandra Stark, Mrs Monika Hoffmann and Mrs Ulrike Bechtel of
Saarland University Medical Center (Homburg, Germany) for their
technical support.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CSLM and ML were major contributors in writing the
manuscript, made substantial contributions to the conception and
design of the study, and gave final approval of the version to be
published. LK and FB performed the immunohistochemical staining. TP
and SS performed the virological analyzes. SG conducted the
statistical tests. TV and BS critically read the manuscript and
were major contributors in the study design. All authors read and
approve the final manuscript.
Ethics approval and consent to
participate
Investigations were performed after approval by a
local Human Investigations Committee (approval no. 281/10;
Ethikkomission der Ärztekammer des Saarlandes). All participants
gave their informed consent to participate in the study.
Patient consent for publication
Informed consent for publication of the data was
obtained from all patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Koch M, Freundl AJ, Agaimy A, Kiesewetter
F, Künzel J, Cicha I and Alexiou C: Atypical
fibroxanthoma-histological diagnosis, immunohistochemical markers
and concepts of therapy. Anticancer Res. 35:5717–5735.
2015.PubMed/NCBI
|
|
2
|
Kim YS, Lee HM, Kim JP and Lim CR: Unusual
presentation of a type 1 Monteggia equivalent lesion: Simultaneous
medial humeral condyle fracture with ipsilateral anterior
dislocation of the radial head and acute plastic bowing of the
ulna. J Pediatr Orthop B. 23:383–388. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tchernev G, Tronnier M, Ananiev J, Taneva
T, Patterson JW, Gulubova M, Trafeli JP, Gegova A, Harrell M,
Guarneri C, et al: Atypical fibroxanthoma-a diagnosis of exclusion!
Wien Med Wochenschr. 163:380–386. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ziemer M: Atypical fibroxanthoma. J Dtsch
Dermatol Ges. 10:537–550. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Helbig D, Ihle MA, Pütz K, Tantcheva-Poor
I, Mauch C, Büttner R and Quaas A: Oncogene and therapeutic target
analyses in atypical fibroxanthomas and pleomorphic dermal
sarcomas. Oncotarget. 7:21763–21774. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Weiss A, Vanchinathan V and Kwon EJ:
Aberrant tyrosinase expression in an atypical fibroxanthoma: A case
report. J Cutan Pathol. 44:467–469. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lopez L and Velez R: Atypical
fibroxanthoma. Arch Pathol Lab Med. 140:376–379. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Toll A, Gimeno J, Baró T, Hernández-Munoz
MI and Pujol RM: Study of epithelial to mesenchymal transition in
atypical fibroxanthoma and undifferentiated pleomorphic sarcoma to
discern an epithelial origin. Am J Dermatopathol. 38:270–277. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mahalingam S, Shah A and Stewart A:
Atypical Fibroxanthoma: A case series and review of literature.
Auris Nasus Larynx. 42:469–471. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
de Feraudy S, Mar N and McCalmont TH:
Evaluation of CD10 and procollagen 1 expression in atypical
fibroxanthoma and dermatofibroma. Am J Surg Pathol. 32:1111–1122.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gleason BC, Calder KB, Cibull TL, Thomas
AB, Billings SD, Morgan MB, Hiatt KM and Smoller BR: Utility of p63
in the differential diagnosis of atypical fibroxanthoma and spindle
cell squamous cell carcinoma. J Cutan Pathol. 36:543–547. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tallon B and Beer TW: MITF positivity in
atypical fibroxanthoma. Am J Dermatopathol. 38:165–166. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Andres C, Puchta U and Flaig MJ: Detection
of Merkel cell polyomavirus DNA in atypical fibroxanthoma in
correlation to clinical features. Am J Dermatopathol. 32:799–803.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Conti BJ, Devaraneni PK, Yang Z, David LL
and Skach WR: Cotranslational stabilization of Sec62/63 within the
ER Sec61 translocon is controlled by distinct substrate-driven
translocation events. Mol Cell. 58:269–283. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Meyer HA, Grau H, Kraft R, Kostka S, Prehn
S, Kalies KU and Hartmann E: Mammalian Sec61 is associated with
Sec62 and Sec63. J Biol Chem. 275:14550–14557. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lakkaraju AK, Thankappan R, Mary C,
Garrison JL, Taunton J and Strub K: Efficient secretion of small
proteins in mammalian cells relies on Sec62-dependent
posttranslational translocation. Mol Biol Cell. 23:2712–2722. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lang S, Benedix J, Fedeles SV, Schorr S,
Schirra C, Schäuble N, Jalal C, Greiner M, Hassdenetufel S, Tatzelt
J, et al: Different effects of Sec61α, Sec62 and Sec63 depletion on
transport of polypeptides into the endoplasmic reticulum of
mammalian cells. J Cell Sci. 125:1958–1969. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Müller L, de Escauriaza MD, Lajoie P,
Theis M, Jung M, Müller A, Burgard C, Greiner M, Snapp EL, Dudek J
and Zimmermann R: Evolutionary gain of function for the ER membrane
protein Sec62 from yeast to humans. Mol Biol Cell. 21:691–703.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Erdmann F, Schäuble N, Lang S, Jung M,
Honigmann A, Ahmad M, Dudek J, Benedix J, Harsmann A, Kopp A, et
al: Interaction of calmodulin with Sec61α limits Ca2+ leakage from
the endoplasmic reticulum. EMBO J. 30:17–31. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lang S, Erdmann F, Jung M, Wagner R,
Cavalie A and Zimmermann R: Sec61 complexes form ubiquitous ER Ca2+
leak channels. Channels (Austin). 5:228–235. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Linxweiler M, Schorr S, Schäuble N, Jung
M, Linxweiler J, Langer F, Schäfers HJ, Cavalié A, Zimmermann R and
Greiner M: Targeting cell migration and the endoplasmic reticulum
stress response with calmodulin antagonists: A clinically tested
small molecule phenocopy of SEC62 gene silencing in human tumor
cells. BMC Cancer. 13:5742013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schäuble N, Lang S, Jung M, Cappel S,
Schorr S, Ulucan Ö, Linxweiler J, Dudek J, Blum R, Helms V, et al:
BiP-mediated closing of the Sec61 channel limits Ca2+ leakage from
the ER. EMBO J. 31:3282–3296. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bockmühl U, Schwendel A, Dietel M and
Petersen I: Distinct patterns of chromosomal alterations in high-
and low-grade head and neck squamous cell carcinomas. Cancer Res.
56:5325–5329. 1996.PubMed/NCBI
|
|
24
|
Sheu JJ, Lee CH, Ko JY, Tsao GS, Wu CC,
Fang CY, Tsai FJ, Hua CH, Chen CL and Chen JY: Chromosome
3p12.3-p14.2 and 3q26.2-q26.32 are genomic markers for prognosis of
advanced nasopharyngeal carcinoma. Cancer Epidemiol Biomarkers
Prev. 18:2709–2716. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Jung V, Kindich R, Kamradt J, Jung M,
Müller M, Schulz WA, Engers R, Unteregger G, Stöckle M, Zimmermann
R and Wullich B: Genomic and expression analysis of the 3q25-q26
amplification unit reveals TLOC1/SEC62 as a probable target gene in
prostate cancer. Mol Cancer Res. 4:169–176. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Chang YC, Yeh KT, Liu TC and Chang JG:
Molecular cytogenetic characterization of esophageal cancer
detected by comparative genomic hybridization. J Clin Lab Anal.
24:167–174. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Allen DG, White DJ, Hutchins AM, Scurry
JP, Tabrizi SN, Garland SM and Armes JE: Progressive genetic
aberrations detected by comparative genomic hybridization in
squamous cell cervical cancer. Br J Cancer. 83:1659–1663. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Heselmeyer K, Macville M, Schröck E,
Blegen H, Hellström AC, Shah K, Auer G and Ried T: Advanced-stage
cervical carcinomas are defined by a recurrent pattern of
chromosomal aberrations revealing high genetic instability and a
consistent gain of chromosome arm 3q. Genes Chromosomes Cancer.
19:233–240. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Haverty PM, Hon LS, Kaminker JS, Chant J
and Zhang Z: High-resolution analysis of copy number alterations
and associated expression changes in ovarian tumors. BMC Med
Genomics. 2:212009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dehan E, Ben-Dor A, Liao W, Lipson D,
Frimer H, Rienstein S, Simansky D, Krupsky M, Yaron P, Friedman E,
et al: Chromosomal aberrations and gene expression profiles in
non-small cell lung cancer. Lung Cancer. 56:175–184. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bochen F, Adisurya H, Wemmert S, Lerner C,
Greiner M, Zimmermann R, Hasenfus A, Wagner M, Smola S, Pfuhl T, et
al: Effect of 3q oncogenes SEC62 and SOX2 on lymphatic metastasis
and clinical outcome of head and neck squamous cell carcinomas.
Oncotarget. 8:4922–4934. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Linxweiler M, Linxweiler J, Barth M,
Benedix J, Jung V, Kim YJ, Bohle RM, Zimmermann R and Greiner M:
Sec62 bridges the gap from 3q amplification to molecular cell
biology in non-small cell lung cancer. Am J Pathol. 180:473–483.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wemmert S, Lindner Y, Linxweiler J,
Wagenpfeil S, Bohle R, Niewald M and Schick B: Initial evidence for
Sec62 as a prognostic marker in advanced head and neck squamous
cell carcinoma. Oncol Lett. 11:1661–1670. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Weng L, Du J, Zhou Q, Cheng B, Li J, Zhang
D and Ling C: Identification of cyclin B1 and Sec62 as biomarkers
for recurrence in patients with HBV-related hepatocellular
carcinoma after surgical resection. Mol Cancer. 11:392012.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Fumagalli F, Noack J, Bergmann TJ,
Cebollero E, Pisoni GB, Fasana E, Fregno I, Galli C, Loi M, Soldà
T, et al: Translocon component Sec62 acts in endoplasmic reticulum
turnover during stress recovery. Nat Cell Biol. 18:1173–1184. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Greiner M, Kreutzer B, Jung V, Grobholz R,
Hasenfus A, Stöhr RF, Tornillo L..Dudek J, Stöckle M, Unteregger G,
et al: Silencing of the SEC62 gene inhibits migratory and invasive
potential of various tumor cells. Int J Cancer. 128:2284–2295.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Greiner M, Kreutzer B, Lang S, Jung V,
Cavalié A, Unteregger G, Zimmermann R and Wullich B: Sec62 protein
level is crucial for the ER stress tolerance of prostate cancer.
Prostate. 71:1074–1083. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Hagerstrand D, Tong A, Schumacher SE, Ilic
N, Shen RR, Cheung HW, Vazquez F, Shresta Y, Kim SY, Giacomelli AO,
et al: Systematic interrogation of 3q26 identifies TLOC1 and SKIL
as cancer drivers. Cancer Discov. 3:1044–1057. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Linxweiler M, Bochen F, Schick B, Wemmert
S, Al Kadah B, Greiner M, Hasenfus A, Bohle RM, Juhasz-Böss I,
Solomayer EF and Takacs ZF: Identification of SEC62 as a potential
marker for 3q amplification and cellular migration in dysplastic
cervical lesions. BMC Cancer. 16:6762016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Remmele W and Stegner HE: Recommendation
for uniform definition of an immunoreactive score (IRS) for
immunohistochemical estrogen receptor detection (ER-ICA) in breast
cancer tissue. Pathologe. 8:138–140. 1987.PubMed/NCBI
|
|
41
|
Feng H, Shuda M, Chang Y and Moore PS:
Clonal integration of a polyomavirus in human Merkel cell
carcinoma. Science. 319:1096–1100. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sperling T, Oldak M, Walch-Rückheim B,
Wickenhauser C, Doorbar J, Pfister H, Malejczyk M, Majewski S,
Keates AC and Smola S: Human papillomavirus type 8 interferes with
a novel C/EBPβ-mediated mechanism of keratinocyte CCL20 chemokine
expression and Langerhans cell migration. PLoS Pathog.
8:e10028332012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Mentzel T, Requena L and Brenn T: Atypical
Fibroxanthoma revisited. Surg Pathol Clin. 10:319–335. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Luo GG and Ou JH: Oncogenic viruses and
cancer. Virol Sin. 30:83–84. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Álvarez-Argüelles ME, Melón S, Rojo S,
Fernandez-Blázquez A, Boga JA, Palacio A, Vivanco B and de Oña M:
Detection and quantification of Merkel cell polyomavirus. Analysis
of Merkel cell carcinoma cases from 1977 to 2015. J Med Virol.
89:2224–2229. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Mancuso G, Antona J, Sirini C, Salvo M,
Giacometti L, Olivero C, Trisolini E, Indellicato R and Boldorini
R: Frequent detection of Merkel cell polyomavirus DNA in tissues
from 10 consecutive autopsies. J Gen Virol. 98:1372–1376. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Foulongne V, Sauvage V, Hebert C, Dereure
O, Cheval J, Gouilh MA, Pariente K, Segondy M, Burguière A,
Manuguerra JC, et al: Human skin microbiota: High diversity of DNA
viruses identified on the human skin by high throughput sequencing.
PLoS One. 7:e384992012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Liu W, Yang R, Payne AS, Schowalter RM,
Spurgeon ME, Lambert PF, Xu X, Buck CB and You J: Identifying the
target cells and mechanisms of merkel cell polyomavirus infection.
Cell Host Microbe. 19:775–787. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Liu W, MacDonald M and You J: Merkel cell
polyomavirus infection and Merkel cell carcinoma. Curr Opin Virol.
20:20–27. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Nonaka D and Bishop PW: Sarcoma-like tumor
of head and neck skin. Am J Surg Pathol. 38:956–965. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ivan D and Prieto VG: An update on
reporting histopathologic prognostic factors in melanoma. Arch
Pathol Lab Med. 135:825–829. 2011.PubMed/NCBI
|
|
52
|
Balch CM, Gershenwald JE, Soong SJ,
Thimpson JF, Atkins MB, Byrd DR, Buzaid AC, Cochran AJ, Coit DG,
Ding S, et al: Final version of 2009 AJCC melanoma staging and
classification. J Clin Oncol. 27:6199–1206. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Linxweiler M, Schick B and Zimmermann R:
Let's talk about Sec62: Sec61, Sec62 and Sec63 in signal
transduction, oncology and personalized medicine. Signal Transduct
Target Ther. 2:170022017. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Helwig EB and May D: Atypical
fibroxanthoma of the skin with metastasis. Cancer. 57:368–376.
1986. View Article : Google Scholar : PubMed/NCBI
|