Introduction
Elective lower abdominal surgery is frequently
performed under general anesthesia among gynecological cancer
patient population. Gynecology tumor patients are mostly
middle-aged and old, and they often have internal diseases such as
hypertension, cardiovascular and cerebrovascular disease and other
medical problems. Anesthetization is highly demanding in these
operations due to the long time, wide expansion and large wound.
Thus, it is important to choose the appropriate airway
management.
Developments in anesthesia practice and airway
management have increased safety of pediatric anesthesia (1,2). We
improved airway management efficiency by using endotracheal
intubation (ETI) or laryngeal mask airway (LMA) (3). There has been progress in the
development of the design in the past ten years, changes in
production material, and availability of various types.
Anesthetists widely use ETI because of the advantages of good seal
at the cricoid rings, decreased pressure, and thus a lower risk for
mucosal injury (4). However,
subglottic stenosis caused by a lack of cuff related mucosal
perfusion due to cuff tube use, making their use controversial. In
contrast, LMA has the advantages of a lack of direct contact with
the trachea, no requirement for direct laryngoscopy, and a lower
incidence of coughing (5–7).
We compared hemodynamics and respiratory function
between LMA and ETI in gynecological cancer patients undergoing
elective lower abdominal surgery (8,9).
Patients and methods
Study design
A prospective, double-blind, randomized clinical
trial was performed to evaluate the usefulness of the LMA compared
to ETI by analyzing changes in clinical symptoms before and after
surgery. The Ethics Committee of Jiangsu Cancer Hospital (Nanjing,
China) approved the study.
Patients
After obtaining informed consents, 54 women, aged
32–55 years, with cervical and ovarian cancer were included in the
study. The patients were scheduled for lower abdominal surgery at
Jiangsu Cancer Hospital, between June 2012 and December 2012. The
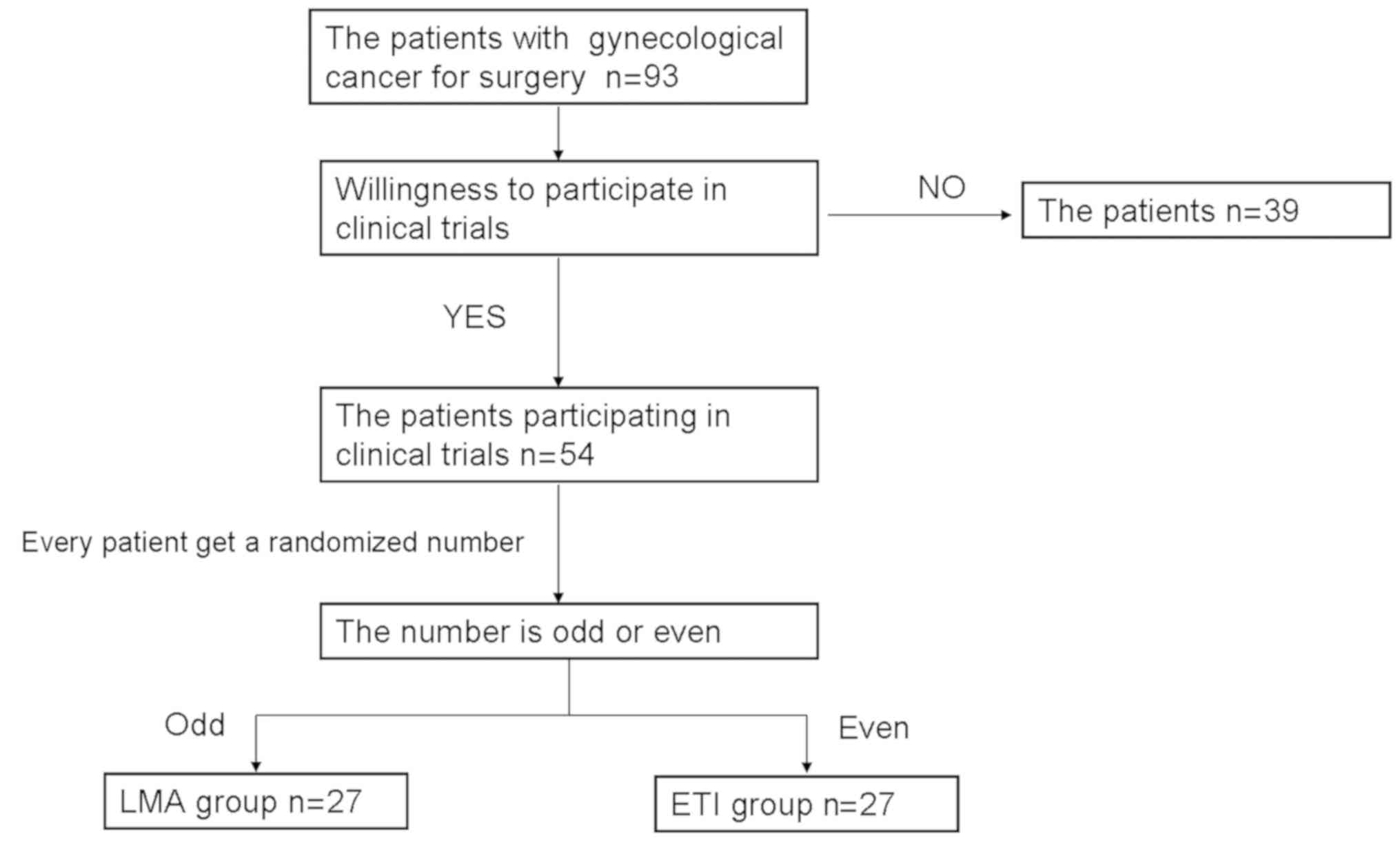
patient who took part in our research were randomized from 1 to
100. Then they were divided into two groups according the odd/even
numbers (Fig. 1). Then, the 54
patients were randomized into the LMA group (n=27) and ETI group
(n=27). Patients with congenital abnormalities, risk of aspiration,
upper respiratory tract infection, acute or chronic pulmonary
diseases, or risk for difficult intubation were excluded from the
study.
Statistical analysis
Continuous data were expressed as the number of
participants (n), mean ± SD, whereas categorical data were
expressed as frequencies and percentages. Comparisons between the
two groups were done using independent Students t-test. Statistical
analysis was carried out using Statistical Product and Service
Solutions (SPSS) 16.0 (SPSS Inc., Chicago, IL, USA). A P-value
<0.05 was considered statistically significant.
Results
A total of 54 patients were randomized in this
study: 27 in the LMA group and 27 in the ETI group. The sex and age
of the two groups were similar. The demographic and surgical data
are presented in Table I.
 | Table I.Demographic and surgical data. |
Table I.
Demographic and surgical data.
| Items | LMA | ETI |
|---|
| Age (year) |
44.30±8.05 |
46.81±8.41 |
| Sex (F/M, no.) | 28/0 | 28/0 |
| Weight (kg) |
60.22±7.73 |
61.93±8.87 |
| Height (cm) | 160.93±4.75 | 159.19±3.94 |
| Surgery time
(min) |
125.19±17.70 |
110.85±15.40 |
| Total anesthesia time
(min) |
137.56±17.92 |
121.22±16.28 |
Acceleration index (ACI), cardiac index (CI),
cardiac output (CO), left cardiac work (LCW), systemic circulation
resistance (SVR), mean arterial pressure (MAP), heart rate (HR),
systolic blood pressure (SBP) and diastolic blood pressure (DBP)
were recorded at 12 time-points: before surgery (T0), start effect
(T1), lost consciousness (T2), before ETI or LMA (T3), 1 min (T4),
3 min (T5), 5 min (T6) after ETI or LMA, the beginning of surgery
(T7), 30 min (T8), 2 hours (T9) after surgery, the end of surgery
(T10) and extubation (T11) (Table
II).
| Table II.Comparison of clinical indexes between
LMA and ETI (means ± SD). |
Table II.
Comparison of clinical indexes between
LMA and ETI (means ± SD).
| Item | T0 | T1 | T2 | T3 | T4 | T5 |
|---|
| ACI |
| LMA | 92.31±37.33 | 90.79±44.29 | 81.62±29.31 | 88.81±34.65 | 87.24±34.84 | 86.21±33.31 |
| ETI | 84.28±32.73 | 76.76±32.60 | 70.40±30.03 | 73.16±27.77 | 65.96±26.86 | 76.44±32.59 |
|
P-value | 0.377 | 0.174 | 0.138 | 0.059 | 0.011 | 0.246 |
| CI |
| LMA | 2.886±0.73 | 2.75±0.79 | 2.66±0.61 | 2.53±0.63 | 2.58±0.58 | 2.50±0.64 |
| ETI | 2.808±0.53 | 2.63±0.65 | 2.38±0.63 | 2.25±0.58 | 2.38±0.56 | 2.44±0.60 |
|
P-value | 0.643 | 0.532 | 0.081 | 0.076 | 0.154 | 0.735 |
| CO |
| LMA | 4.70±1.15 | 4.49±1.30 | 4.24±0.96 | 3.97±1.00 | 4.20±0.94 | 4.07±1.06 |
| ETI | 4.48±1.04 | 4.18±1.26 | 3.74±0.99 | 3.67±1.35 | 3.83±1.31 | 3.92±1.28 |
|
P-value | 0.43 | 0.352 | 0.049 | 0.296 | 0.187 | 0.612 |
| LCW |
| LMA | 5.30±1.31 | 4.60±1.57 | 4.10±1.22 | 3.61±0.95 | 4.08±1.10 | 3.63±1.11 |
| ETI | 5.38±1.53 | 4.40±1.35 | 3.50±1.05 | 3.03±1.06 | 4.45±1.32 | 3.76±1.21 |
|
P-value | 0.812 | 0.571 | 0.047 | 0.024 | 0.228 | 0.663 |
| SVR |
| LMA | 1,623.05±836.75 | 1,625.98±906.83 | 1,440.45±685.12 | 1,489.32±986.32 | 1,509.00±681.90 | 1,470.14±786.71 |
| ETI | 1,814.80±627.03 |
1,849.32±1,024.45 |
1,749.32±1,046.70 | 1,628.00±844.12 | 2,099.04±990.98 |
1,813.28±1,022.65 |
|
P-value | 0.291 | 0.356 | 0.149 | 0.545 | 0.005 | 0.128 |
| MAP |
|
LMA | 90.29±7.86 | 81.98±7.31 | 74.88±8.60 | 69.52±8.43 | 77.40±13.75 | 71.76±12.12 |
|
ETI | 96.00±11.67 | 86.04±11.06 | 75.84±9.40 | 69.96±12.70 | 94.76±16.77 | 79.64±15.43 |
|
P-value | 0.019 | 0.075 | 0.671 | 0.866 | 0 | 0.023 |
| HR |
|
LMA | 85.74±12.43 | 78.41±10.71 | 79.43±12.89 | 76.33±11.25 | 81.76±13.76 | 74.12±13.28 |
|
ETI | 96.56±14.38 | 88.36±13.28 | 89.36±14.27 | 82.80±13.73 | 91.08±12.42 | 86.60±13.39 |
|
P-value | 0.546 | 0.043 | 0.343 | 0.04 | 0.006 | 0.001 |
| SBP |
|
LMA | 119.29±11.35 | 107.64±17.99 | 101.62±9.27 | 98.14±10.21 | 103.79±12.77 | 99.76±11.49 |
|
ETI | 125.60±16.89 | 111.64±14.63 | 100.68±9.39 | 95.20±11.53 | 120.16±21.12 | 104.48±17.75 |
|
P-value | 0.072 | 0.351 | 0.691 | 0.281 | 0 | 0.191 |
| DB |
|
LMA | 72.95±6.14 | 65.71±6.15 | 60.26±7.18 | 54.52±7.39 | 61.95±13.09 | 56.64±10.87 |
|
ETI | 76.80±10.40 | 69.40±9.63 | 60.44±9.39 | 54.72±12.10 | 78.52±16.13 | 63.76±13.83 |
|
P-value | 0.061 | 0.06 | 0.931 | 0.934 | 0 | 0.022 |
| ACI |
|
LMA | 94.31±50.85 | 83.19±30.98 | 82.69±36.48 | 82.12±36.12 | 81.14±32.01 | 80.64±27.92 |
|
ETI | 79.04±42.48 | 68.60±23.01 | 73.20±27.88 | 80.88±30.35 | 80.68±30.37 | 82.00±33.26 |
|
P-value | 0.049 | 0.045 | 0.267 | 0.886 | 0.954 | 0.858 |
| CI |
|
LMA | 2.50±0.63 | 2.35±0.50 | 2.58±0.66 | 2.57±0.76 | 2.53±0.64 | 2.91±0.75 |
|
ETI | 2.33±0.61 | 2.22±0.49 | 2.20±0.33 | 2.46±0.43 | 2.54±0.38 | 2.86±0.60 |
|
P-value | 0.271 | 0.327 | 0.011 | 0.529 | 0.94 | 0.763 |
| CO |
|
LMA | 4.02±1.02 | 3.81±0.94 | 4.23±1.19 | 4.20±1.25 | 4.12±1.07 | 4.78±1.27 |
|
ETI | 3.78±1.45 | 3.40±0.95 | 3.57±0.73 | 3.90±0.75 | 3.88±0.87 | 4.50±0.98 |
|
P-value | 0.443 | 0.093 | 0.014 | 0.288 | 0.331 | 0.335 |
| LCW |
|
LMA | 3.57±1.11 | 3.61±0.86 | 5.06±1.42 | 4.69±1.51 | 4.50±1.32 | 5.96±1.82 |
|
ETI | 3.52±1.23 | 3.43±1.13 | 4.19±0.87 | 4.65±1.18 | 4.33±1.00 | 6.00±1.52 |
|
P-value | 0.884 | 0.482 | 0.007 | 0.899 | 0.596 | 0.929 |
| SVR |
|
LMA |
1,473.17±985.63 |
1,654.62±727.71 |
1,974.33±1,288.26 |
1,848.48±1,279.64 |
1,771.33±1,052.80 |
1,771.69±1,189.15 |
|
ETI |
1,720.08±905.25 |
1,741.44±495.27 |
2,142.88±631.07 |
1,957.08±564.22 |
1,830.48±489.35 |
1,850.28±611.97 |
|
P-value | 0.301 | 0.6 | 0.477 | 0.69 | 0.793 | 0.76 |
| MAP |
|
LMA | 69.43±11.15 | 76.50±11.14 | 93.69±12.05 | 88.33±11.14 | 84.86±10.66 | 96.31±11.89 |
|
ETI | 76.56±14.80 | 75.80±11.19 | 95.16±12.05 | 93.60±9.94 | 87.44±9.62 | 103.08±16.02 |
|
P-value | 0.029 | 0.805 | 0.631 | 0.056 | 0.324 | 0.052 |
| HR |
|
LMA | 72.98±15.23 | 66.17±16.98 | 73.79±11.59 | 72.83±11.84 | 71.21±13.20 | 89.91±17.04 |
|
ETI | 82.44±13.11 | 77.04±16.80 | 76.20±11.37 | 76.32±13.32 | 75.76±13.64 | 102.32±10.47 |
|
P-value | 0.009 | 0.013 | 0.409 | 0.27 | 0.183 | 0.002 |
| SBP |
|
LMA | 98.26±10.85 | 103.71±10.67 | 116.60±21.00 | 116.69±13.51 | 112.95±11.70 | 126.33±15.41 |
|
ETI | 102.24±15.59 | 99.84±11.67 | 119.76±14.79 | 118.36±11.85 | 113.72±11.64 | 133.72±20.98 |
|
P-value | 0.223 | 0.17 | 0.511 | 0.611 | 0.795 | 0.103 |
| DBP |
|
LMA | 54.57±10.32 | 60.24±10.54 | 76.69±11.33 | 71.21±10.30 | 69.74±9.18 | 79.38±9.67 |
|
ETI | 60.84±13.96 | 61.32±10.68 | 79.12±11.24 | 76.52±9.44 | 70.44±8.72 | 83.72±13.42 |
|
P-value | 0.039 | 0.687 | 0.397 | 0.036 | 0.759 | 0.13 |
We found that in each group these indexes declined
and then increased gently during surgery except for T4 and T12
especially in the ETI group. These indexes reached the highest at
T11 (extubation). This is due to the stimulus on mucosa and muscle
of root of tongue, throat and epiglottis from the windpipe. The
stimulus excites sympathetic nerve and increases the release of
catecholamine. As a result, the heart beats faster and blood
pressure rises. However, the range in the LMA group is smaller
especially at T4 and T11. This is most likely due to LMA not
stimulating the trachea. ACI, CI, CO and LCW were higher in LMA
with statistical significance at certain time-points (P<0.05)
(Fig. 2A-D). Indexes such as SVR,
MAP, HR, SBP and DBP were significantly higher in ETI (Fig. 2E-I).
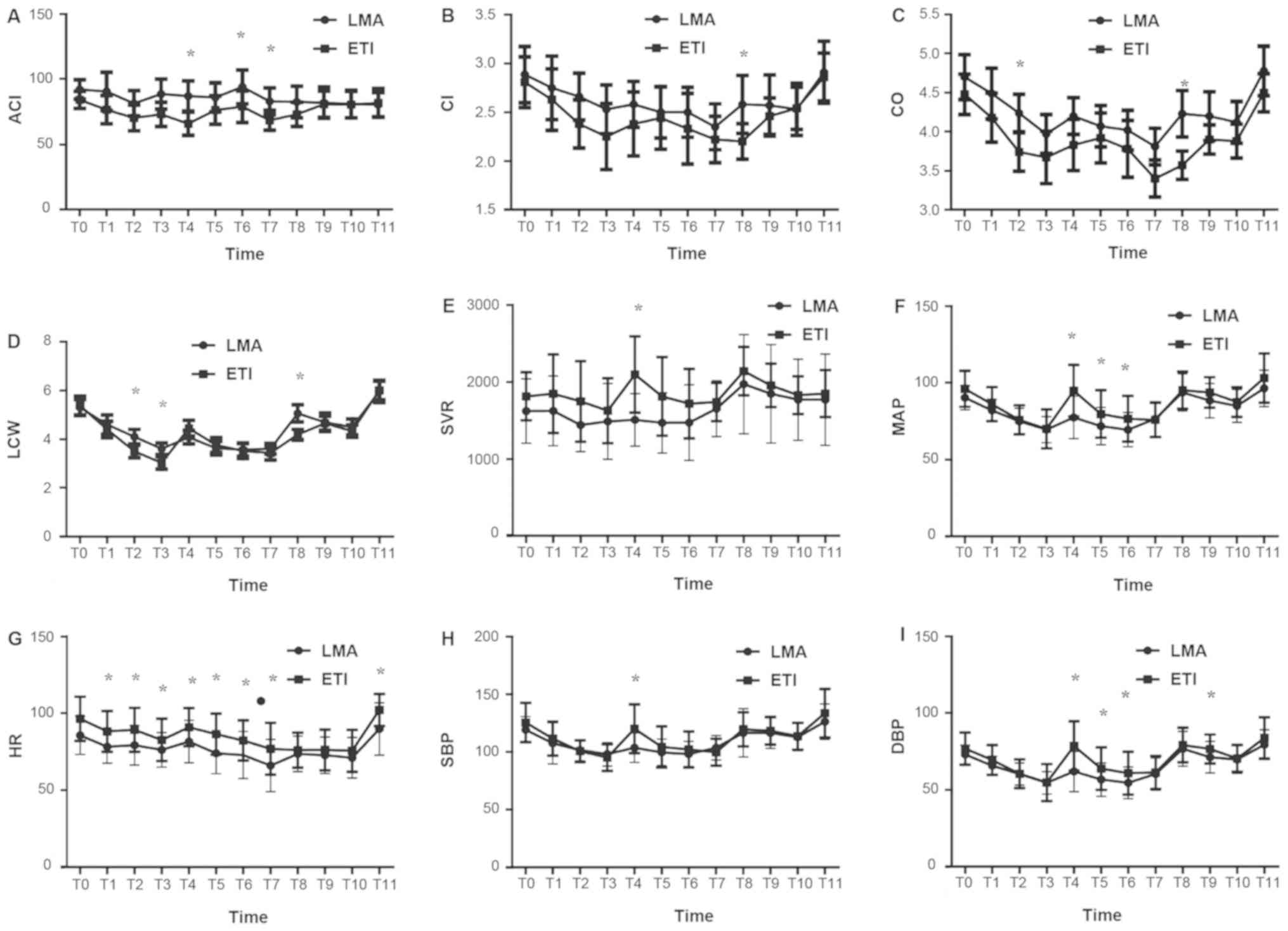 | Figure 2.Comparison of clinical indexes between
the two groups. (A) ACI of the 2 groups at each time-point as
indicated; (B) CI of the 2 groups at the time-points; (C) CO of the
2 groups at the time-points; (D) LCW of the 2 groups at
time-points; (E) SVR of the 2 groups at time-points; (F) MAP of the
2 groups at time-points; (G) HR of the 2 groups at time-points; (H)
SBP of the 2 groups at time-points; (I) DBP of the 2 groups at
time-points. *P<0.05; ACI, acceleration index; CI, cardiac
index; CO, cardiac output; LCW, left cardiac work; SVR, systemic
circulation resistance; MAP, mean arterial pressure; HR, heart
rate; SBP, systolic blood pressure; DBP, diastolic blood pressure;
ETI, endotracheal intubation; LMA, laryngeal mask airway. |
Discussion
LMA was developed by A. Brain in 1981, and since
then, it has flourished in practice and has been used to treat
millions of patients worldwide (10,11). The
LMA provides more hands-free anesthesia than a facemask does,
avoids many morbidities associated with tracheal intubation because
there is no stress from the laryngoscope, and allows a faster
recovery that does not require muscle relaxation (12,13). The
LMA has become an important choice for routine use, particularly in
outpatient surgeries (14–16).
In our investigation, we assessed the eligibility of
LMA by comparing hemodynamics and respiratory function between LMA
and ETI in gynecological cancer operation. The results showed that
LMA can be used safely and induces less stress reaction in
gynecological cancer patients undergoing lower abdominal surgery.
The correlated clinical indexes recorded in 12 time-points declined
and then increased gently during surgery except for the time-point
of intubation (T4) and extubation (T11) especially in the ETI
group. These indexes reached the highest at extubation (T11). This
is due to the stimulus on mucosa and muscle of root of tongue,
throat and epiglottis, from the windpipe. The stimulus excites
sympathetic nerve and increases the release of catecholamine
(17–21). As a result, hearts beat faster and
blood pressure rises. However, the range in the LMA group is
smaller especially at T4 and T11. This is possibly due to LMA not
stimulating the trachea (22–25). One weakness of our design is that we
could not get meaningful results using a multivariate logistic
regression analysis. This may have been caused by the small number
of samples. We will use a multivariate logistic regression analysis
in future studies when a larger number of samples is available.
There were higher incidences of bucking in the ETI
group in similar anesthesia in extubation. In addition, there were
more postoperative complications in the ETI group such as
pharyngalgia compared with LMA. This may be relevant to improper
operation or excessive inflation of the catheter sleeve. This
indicates that the stimulation of ETI is stronger than LMA. Most
patients with ETI experience varying degrees of pharyngeal pain and
have significant change in HR. However, patients with LMA do not
have this complication. This is because LMA does not need to use
laryngoscope and there is no need to enter trachea, thus avoid
damaging tracheal mucosa and influencing circulation system. LMA
has become complementary technology of ETI to offer a safe,
effective, and simple ventilation method especially to the patient
with microstomia. LMA is simpler to operate than ETI for medical
workers and gains more time during emergency treatment. In
addition, LMA is specifically suitable for the patient with
microstomia (26).
In conclusion, the LMA may be a suitable method for
airway management of patients with gynecological cancer under-going
lower abdominal surgery (27,28). Furthermore, LMA is a good alternative
to ETI with easier insertion, and lower incidence of cardiovascular
response.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JT and LG designed the study and performed the
experiments, ZS, JF and QB collected the data, JT and ZS analyzed
the data, JT and LG prepared the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Jiangsu Cancer Hospital (Nanjing, China). Signed informed consents
were obtained from the patients or their guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Badr A, Tobias JD, Rasmussen GE, Stokes
DC, Neblett WW III and Campbell P: Bronchoscopic airway evaluation
facilitated by the laryngeal mask airway in pediatric patients.
Pediatr Pulmonol. 21:57–61. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Khine HH, Corddry DH, Kettrick RG, Martin
TM, McCloskey JJ, Rose JB, Theroux MC and Zagnoev M: Comparison of
cuffed and uncuffed endotracheal tubes in young children during
general anesthesia. Anesthesiology. 86:627–631; discussion 27A.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Junger A, Klasen J, Hartmann B, Benson M,
Röhrig R, Kuhn D and Hempelmann G: Shorter discharge time after
regional or intravenous anaesthesia in combination with laryngeal
mask airway compared with balanced anaesthesia with endotracheal
intubation. Eur J Anaesthesiol. 19:119–124. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kihara S, Brimacombe J, Yaguchi Y,
Watanabe S, Taguchi N and Komatsuzaki T: Hemodynamic responses
among three tracheal intubation devices in normotensive and
hypertensive patients. Anesth Analg. 96:890–895. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pinosky M: Laryngeal mask airway: Uses in
anesthesiology. South Med J. 89:551–555. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Landsman IS: The laryngeal mask airway.
Int Anesthesiol Clin. 35:49–65. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pennant JH and White PF: The laryngeal
mask airway. Its uses in anesthesiology. Anesthesiology.
79:144–163. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Doksrød S, Løfgren B, Nordhammer A,
Svendsen MV, Gisselsson L and Raeder J: Reinforced laryngeal mask
airway compared with endotracheal tube for adenotonsillectomies.
Eur J Anaesthesiol. 27:941–946. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Webster AC, Morley-Forster PK, Janzen V,
Watson J, Dain SL, Taves D and Dantzer D: Anesthesia for intranasal
surgery: A comparison between tracheal intubation and the flexible
reinforced laryngeal mask airway. Anesth Analg. 88:421–425. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
van Zundert TC, Brimacombe JR, Ferson DZ,
Bacon DR and Wilkinson DJ: Archie Brain: Celebrating 30 years of
development in laryngeal mask airways. Anaesthesia. 67:1375–1385.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hernandez MR, Klock PA Jr and Ovassapian
A: Evolution of the extraglottic airway: A review of its history,
applications, and practical tips for success. Anesth Analg.
114:349–368. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Alexander CA: A modified intavent
laryngeal mask for ENT and dental anaesthesia. Anaesthesia.
45:892–893. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Jakobsson J: The airway in day surgery.
Minerva Anestesiol. 76:38–44. 2010.PubMed/NCBI
|
|
14
|
Shavit I, Aviram E, Hoffmann Y, Biton O
and Glassberg E: Laryngeal mask airway as a rescue device for
failed endotracheal intubation during scene-to-hospital air
transport of combat casualties. Eur J Emerg Med. 25:368–371. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yang C, Zhu X, Lin W, Zhang Q, Su J, Lin
B, Ye H and Yu R: Randomized, controlled trial comparing laryngeal
mask versus endotracheal intubation during neonatal resuscitation -
a secondary publication. BMC Pediatr. 16:172016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Benger JR, Voss S, Coates D, Greenwood R,
Nolan J, Rawstorne S, Rhys M and Thomas M: Randomised comparison of
the effectiveness of the laryngeal mask airway supreme, i-gel and
current practice in the initial airway management of prehospital
cardiac arrest (REVIVE-Airways): a feasibility study research
protocol. BMJ Open. 3(pii): e0024672013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Leventis C, Chalkias A, Sampanis MA,
Foulidou X and Xanthos T: Emergency airway management by
paramedics: Comparison between standard endotracheal intubation,
laryngeal mask airway, and I-gel. Eur J Emerg Med. 21:371–373.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Xu R, Lian Y and Li WX: Airway
complications during and after general anesthesia: a comparison,
systematic review and Meta-Analysis of using flexible laryngeal
mask airways and endotracheal tubes. PLoS One. 11:e01581372016.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gasteiger L, Ofner S, Stögermüller B,
Ziegler B, Brimacombe J and Keller C: Randomized crossover study
assessing oropharyngeal leak pressure and fiber optic positioning:
Laryngeal Mask Airway Supreme™ versus Laryngeal Tube LTS II™ size 2
in non-paralyzed anesthetized children. Anaesthesist. 65:585–589.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ozden ES, Meco BC, Alanoglu Z and Alkıs N:
Comparison of ProSeal laryngeal mask airway (PLMA) with cuffed and
uncuffed endotracheal tubes in infants. Bosn J Basic Med Sci.
16:286–291. 2016.PubMed/NCBI
|
|
21
|
Chun BJ, Bae JS, Lee SH, Joo J, Kim ES and
Sun DI: A prospective randomized controlled trial of the laryngeal
mask airway versus the endotracheal intubation in the thyroid
surgery: evaluation of postoperative voice, and laryngopharyngeal
symptom. World J Surg. 39:1713–1720. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wheeler M: ProSeal laryngeal mask airway
in 120 pediatric surgical patients: a prospective evaluation of
characteristics and performance. Paediatr Anaesth. 16:297–301.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sinha A, Sharma B and Sood J: ProSeal as
an alternative to endotracheal intubation in pediatric laparoscopy.
Paediatr Anaesth. 17:327–332. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Goldmann K, Roettger C and Wulf H: Use of
the ProSeal laryngeal mask airway for pressure-controlled
ventilation with and without positive end-expiratory pressure in
paediatric patients: a randomized, controlled study. Br J Anaesth.
95:831–834. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hanna SF, Mikat-Stevens M, Loo J, Uppal R,
Jellish WS and Adams M: Awake tracheal intubation in anticipated
difficult airways: LMA Fastrach vs flexible bronchoscope: a pilot
study. J Clin Anesth. 37:31–37. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
van Esch BF, Stegeman I and Smit AL:
Comparison of laryngeal mask airway vs tracheal intubation: A
systematic review on airway complications. J Clin Anesth.
36:142–150. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Al-Mazrou KA, Abdullah KM, ElGammal MS,
Ansari RA, Turkistani A and Abdelmeguid ME: Laryngeal mask airway
vs. uncuffed endotracheal tube for nasal and paranasal sinus
surgery: Paediatric airway protection. Eur J Anaesthesiol.
27:16–19. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ong M, Chambers NA, Hullet B, Erb TO and
von Ungern-Sternberg BS: Laryngeal mask airway and tracheal tube
cuff pressures in children: Are clinical endpoints valuable for
guiding inflation? Anaesthesia. 63:738–744. 2008. View Article : Google Scholar : PubMed/NCBI
|