Overview on cutaneous T-cell lymphoma
Molecular biology research has contributed a great
deal to advances in medical research, most notably in hematology
and oncology. Molecular mechanisms governing hematopoietic
differentiation and proliferation, as well as mutations involved in
hematopoietic malignancies, are now better understood (1–3).
The established guidelines for the diagnostic and
clinical management of hematologic malignancies, including
lymphomas, were published in 2008, under WHO coordination, and were
revised in 2017 (4). T-cell lymphomas
are classified into several categories, based on WHO
recommendations, accessible in recent reviews (5–8). CTCLs are
characterized by the recruitment of malignant T-cell clones into
the skin. Mycosis fungoides (MF) represent the most common type of
CTCL and account for ~50% of all primary cutaneous lymphomas,
followed by Sézary syndrome. In 2018, the EORTC cutaneous lymphoma
task force proposed a uniformity in classification and prognostic
of these two entities using flow cytometry (9).
An important player in the pathogeny of most tumors
is the vascular niche (10),
responsible for increased output of growth factors, such as VEGF
(vascular endothelial growth factor) and FGFb, that promote
uncontrolled cell growth. An association between angiogenesis and
prognostics of MF has been well established (11–13) and
repeated attempts have been made to target it therapeutically
(14,15). This review is focusing on molecular
mechanisms and druggable molecular targets, as well as biomarker
progress made in the diagnostics and prognostics of CTCLs.
Molecular mechanisms that drive initiation
and progression of cutaneous T-cell lymphoma
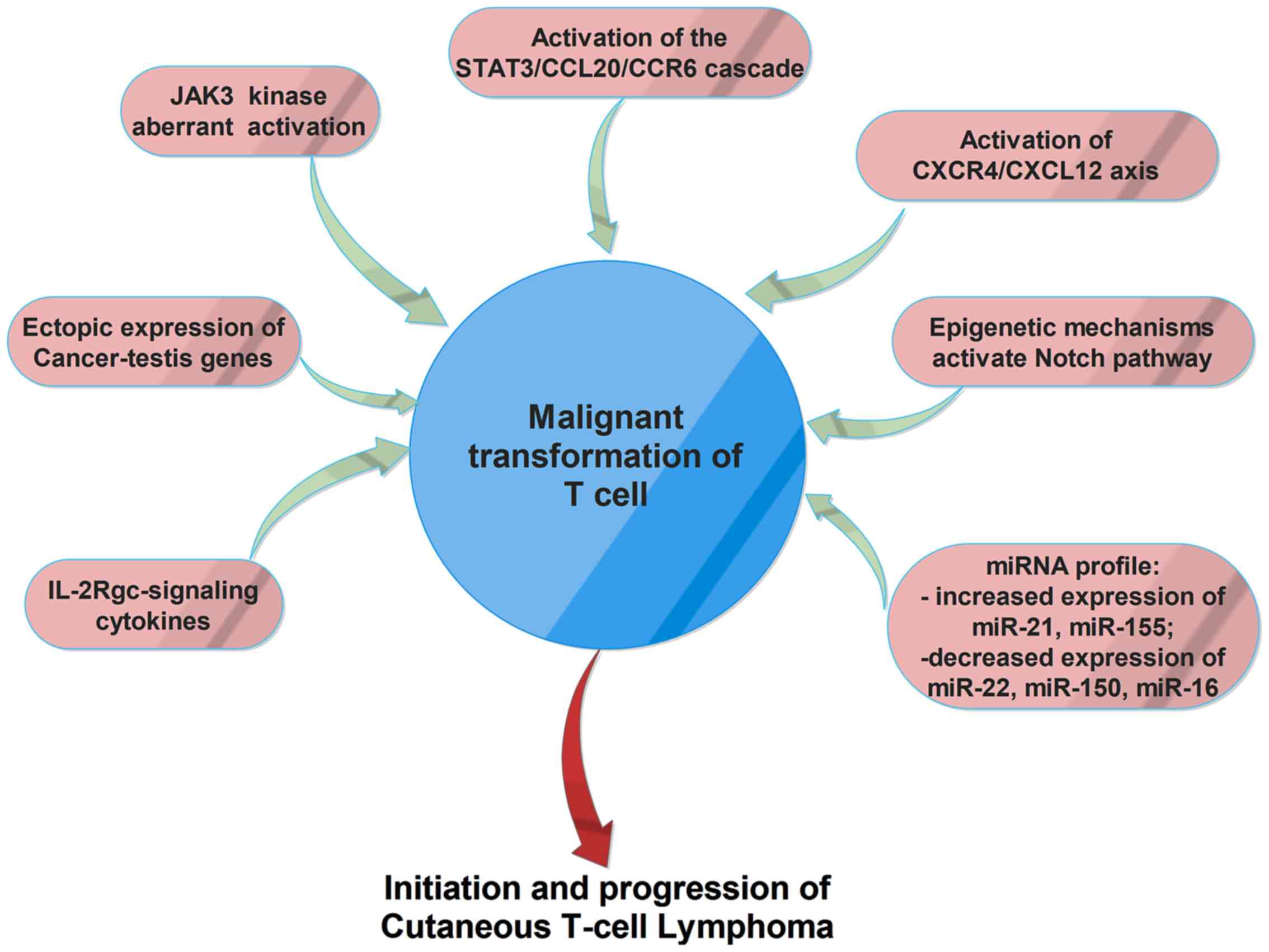
Several dysregulated gene/proteins and signaling
pathways have been associated with CTCLs (Fig. 1), but the exact mechanism of
initiation and progression of this disorder is not yet known.
Recent studies suggested that cancer testis (CT) genes are
ectopically expressed in CTCLs and play an important role in
carcinogenesis. These genes can sustain cell survival by inhibition
of apoptosis, can promote chemo- and radio-therapy resistance and
contribute to oncogenesis by targeting p53 and p21 tumor suppressor
genes. Moreover, these genes can sustain aneuploidy and genomic
instability by producing aberrant chromosomal translocations
(16,17).
Another molecular mechanism involved in malignant
transformation of CTCLs is represented by the aberrant activation
of JAK3 kinase and its key down-stream effectors, STAT3 and STAT5.
Therefore, IL-2, IL-4, IL-7, IL-15, and IL-21 cytokines are
involved in early pathogenesis, whereas constitutive,
interleukin-independent activation of the JAK3/STAT3 pathway seems
to be associated with progressive and advanced disease. Aberrant
activation of the JAK3/STAT signaling pathway and
interleukin-independent proliferation of malignant T-cells are also
related to a decreased expression and/or deregulation of function
of the negative regulators SOCS-3 and SHP1. Aberrant activation of
JAK3/STAT signaling pathway increases the expression of IL-5,
IL-10, IL-17A, IL-17F and angiogenic factors, and sustains the
resistance to treatment with histone deacetylase (HDAC) inhibitors
in malignant T-cells (18).
IL-2Rgc-signaling cytokines, including IL-2, IL-4,
IL-7, IL-15, and IL-21, have been associated with the pathogenesis
of CTCLs (19). Recent studies
suggested that IL-21 could be considered a potent antitumor agent,
which increases the cytotoxicity of both natural killer (NK) and
CD8+ T-cells. Circulating IL-21 levels in patients with
tumor MF were significantly lower than those of healthy controls
and plaque MF and the IL-21 expression level decreased during
tumoral-stage (20). Another study
demonstrated that, in lesional skin, malignant and reactive T-cells
produce IL9, a process regulated by STAT3/5. IL9-depleted mice
showed a reduction of tumor growth, higher frequencies of
regulatory T-cells, and activated CD4 and CD8 T lymphocytes
(21). Upregulation of a chemokine
receptor CCR6 and its ligand CCL20 was found in advanced CTCL
cells; automatic activation of the STAT3/CCL20/CCR6 signaling seems
to have an important role in CTCL lymphomagenesis and could be
responsible for spreading malignant T-cells to sentinel lymph
nodes, the bloodstream, and internal organs (22).
The development of blood and lymphatic vessels was
associated with the progression of CTCL. Therefore, malignant
T-cells produce angiogenic factors, such as podoplanin (PDPN),
lymphatic vessel hyaluronan receptor-1 (LYVE-1), VEGF-C, VEGF-R3,
and lymphotoxin-α (LTα), molecules involved in neoangiogenesis and
neolymphoangiogenesis by promoting endothelial cell development and
tube formation, mainly by stimulation of IL-6 expression (23).
The activation of CXCR4/CXCL12 axis was also
associated with MF development. Moreover, administration of
anti-CXCL12 and CXCR4 agents, including the anti-CXCR4 drug AMD3100
(plerixafor), the CXCL12 analog CTCE-9908, the anti-CXCL12 aptamer
Nox-A12 seems to have promising effects in preclinical and clinical
studies as an adjuvant antitumor therapy (24).
Epigenetic mechanisms that activate Notch signaling
pathway has also been found associated with CTCL. Notch signaling
is involved in cell differentiation, proliferation and stemness.
Genome-wide DNA methylation analysis in MF showed a significant
methylation and downregulation of the Notch-related microRNAs,
especially for miR-200c and miR-124 (25).
Several studies suggested that patients with CTCL
present a distinct miRNA expression profile. For example, increased
expression of miR-21 and miR-155 is able to promote resistance to
apoptosis and malignant proliferation and is associated with poor
prognosis and aggressive behavior (19,26). In
Sézary syndrome, a downregulation of the miR-22 tumor suppressor
was observed, also associated with the activation of JAK3/STAT3
signaling (18). Another study
demonstrated that miR-150 was downregulated only in advanced MF
patients, but its expression can be restored using pan-HDACI
treatment. Same results were obtained in the case of miR-16, whose
expression is decreased in early stages of MF, but can also be
restored by administration of vorinostat, another compound that
inhibits HDACs. These results suggest that dysregulation of miRNAs
by HDACs has an important role in the pathogenesis of CTCL, in both
early and advanced stages, since these miRNAs are able to inhibit
the expression of many oncogenes (27).
Using whole-exome sequencing, da Silva Almeida et
al reported a distinctive pattern of somatic copy number
alterations in tumor samples from patients with Sézary syndrome and
other CTCLs (28). The analyses
identified highly prevalent chromosomal deletions involving the
TP53, RB1, PTEN, DNMT3A and CDKN1B tumor suppressors. Somatic
mutations were found in key genes involved in epigenetic regulation
[TET2, CREBBP, KMT2D (MLL2), KMT2C (MLL3), BRD9, SMARCA4 and CHD3].
Signaling pathways are also affected by mutations in MAPK1, BRAF,
CARD11 and PRKG1 that result in increased MAPK, NF-κB and NFAT
activity upon T-cell receptor stimulation.
Tumor niche of cutaneous T-cell lymphoma -
emphasis on vascular microenvironment
A niche is a microenvironment, both physical and
functional. The physical niche is delineated by several cellular
players, centered on the main resident; in this case, tumor cells.
In addition to the central resident of the niche, other cellular
partners contribute to create a physical or a functional scaffold,
the latter mainly via soluble factors. Presently, Pubmed search
using the terms ‘cutaneous T-cell lymphoma vascular niche’ yielded
no results, although microvascularization has been previously
studied in relationship with this class of tumor (12,29).
Neovascularization of lymphoma can be quantified by microvessel
density (MVD), which is the result of cooperation between tumor
cells, proangiogenic stromal cells and infiltrating benign T
lymphocytes and myeloid cells. It is used as an early marker in MF
(29), but quantification reports
vary among different studies due to the heterogeneity of lymphoma
stroma, the range of cell surface markers used for staining and
differences in scoring methodology (30). In general, MVD scores trend highest in
aggressive subtypes including Burkitt's lymphoma and PTCL, compared
with intermediate in DLBCL and lower in indolent follicular
lymphoma (FL).
Creation of a new vascular niche in CTLCs can be
argued by the emerging role of stromal cell derived factor 1 (SDF1,
CXCL12) and its receptor C-X-C motif chemokine receptor 4 (CXCR4)
axis in progression of MF. Signaling via this axis is known as the
main regulating factor for homing of hematopoietic stem cells to
the bone marrow niche (31). In MF,
neoplastic T-cells express CXCR4, especially in the pretumor stage,
to interact with increased levels of CXCL12, playing a critical
role in MF progression (32). This
axis seems to play an important role in both early and advanced
stages of the disease (24).
Endothelial activation and synthesis of growth
factors can be driven by another couple ligand/receptor;
angiopoietin-1 (Ang1)/Tie2. In bone marrow, activation of this axis
is associated with hematopoietic stem cell quiescence (33). Also, Ang1 and its co-family member
Ang2 have been associated with angiogenesis. The recent study of
Kawaguchi et al showed that circulating levels of Ang2 (not
Ang1), might play a role in Sézary syndrome disease activity. In
addition, expression of Ang2+ cells in lesional skin of
CTCL was higher than in normal skin (34).
The main factor responsible for the angiogenic
switch is the family of VEGF. Members of the VEGF family: VEGF-A,
VEGF-B, VEGF-C, VEGF-D, and placenta growth factor (PlGF), through
interactions with their receptors, regulate vascular angiogenesis
and lymphangiogenesis (13). These
factors create positive feedback loops between endothelium and
tumor cells, as well as autocrine feedback, as it has been
demonstrated that acute lymphocytic leukemia and aggressive
subtypes of lymphoma; peripheral T-cell lymphoma (PTCL), diffuse
large B-cell lymphoma (DLBCL), mantle cell lymphoma (MCL) and
primary effusion lymphoma express both VEGF and VEGFRs (35).
Regarding lymphoid vessels, there are also reports
of increased formation of lymphatic vasculature and secondary
lymphoid structures in CTLC. In addition to the classic factors,
Lauenborg et al studied LTα involvement in the progression
and invasion of tumor T-cells. They showed that CTCL cells express
LTα in situ, which acts as an autocrine factor and is driven
by aberrantly activated JAK3/STAT5 pathway. LTα and LTα-induced
expression of IL-6, and together with VEGF, promoted tumor
angiogenesis (23). Activation of the
same signaling pathway has also been correlated with IL-17A and/or
IL-17F secretion that modulate oncogenic angiogenesis (36).
Malignant stroma (fibroblasts, inflammatory and
infiltrated immune cells, such as monocytes and dendritic cells),
provides additional angiogenic and pro-proliferative cues for tumor
cells. In MF, tumor-associated macrophages were activated by
stroma-produced periostin, to create a tumor niche (37). Stromal cells produce thymic stromal
lymphopoietin and IL-16 that trigger T-cell recruitment to the skin
(38). The stroma of MF can be
highlighted by the presence of (LT)β and CCL21 (39).
Cells from tumor stroma, such as macrophages, can be
targeted for destruction either by treatments aimed primarily at
tumor cells, such as interferons (40), or directly, using cell-targeted
treatments (in this case, macrophage-targeted) (41).
Molecular pathways associated with tumor cells and
modified stroma are further targeted in biomarker research and for
therapeutic purposes, as discussed further.
Proteomic biomarkers for diagnostic and
prognostic of CTLC
An article by Humphrey et al (42) argues the utility of serum ribonuclease
as a biomarker for leukemia diagnosis. In this paper, the authors
refer to an even earlier work from the same decade (43). Since then, as the term entered in
current research language, most notably in protein research,
different definitions have been suggested, trying to harmonize
terms and concepts.
The current widely accepted definition of a
‘biomarker’ was first provided by Biomarkers Definition Working
Group in 2001: ‘A characteristic that is objectively measured and
evaluated as an indicator of normal biological processes,
pathogenic processes, or biological responses to a therapeutic
intervention’ (44,45). This definition was modified in 2016 by
the FDA-NIH Biomarker Working Group to ‘characteristic that is
measured as an indicator of normal biological processes, pathogenic
processes, or responses to an exposure or intervention, including
therapeutic interventions’ (46).
The nature of a biomarker may vary from molecular,
to a histological, imagistic or physiologic characteristic.
Following advances in molecular biology technologies, molecular
biomarkers can now be classified into four main types: i) Genomic
biomarkers, based on the analysis of specific DNA sequences; ii)
transcriptomic biomarkers, based on the analysis of RNA expression
profiles; iii) proteomic biomarkers, based on the analysis of
peptide/protein profiles in a wide range of biological samples from
cell cultures and tissue biopsies to cerebrospinal fluid and tears;
and iv) metabolomic biomarkers, based on the analysis of final- or
by-products of different metabolic pathways.
Various studies emphasize the relevance of
proteomics as a useful tool for biomarker identification, through
minimally invasive procedures, allowing a precise approach by
providing the proteomic signature of the disease. High-throughput
proteomic technologies e.g., ultrasensitive microarray, are
nowadays focused on discovery of specific biomarkers, expanding our
knowledge regarding the mechanisms responsible for disease
development, enabling early diagnostic, prognostic, monitoring and
even tailored therapy of the disease (8,47–54).
Given the indolent nature of CTCLs, with majority of
cases evolving over many years with a very slow progression,
identification of circulating biomarkers for early diagnosis,
differentiation and prognosis would be of great benefit for
patients suffering of CTLC (55).
Serum markers are helpful tools in determining the tumor burden in
cutaneous lymphoma and thus might prove useful for disease
monitoring during treatment. There is also a prognostic value that
they may have for predicting the clinical course.
Circulating endothelial progenitor cells (EPC) and
VEGF levels appear to correlate with tumor volumes. The phenotype
CD133+CD34+VEGFR-2+ EPC present in
peripheral blood and lymph nodes in patients with non-Hodgkin
lymphoma; the blood levels are increased in younger patients and
those with aggressive lymphomas (56). It has been shown that circulating
levels of the soluble interleukin-2 receptor (sIL-2R) of α-chain
and lactate dehydrogenase (LDH) are significantly correlated with
lymph node size, however the correlation with cutaneous clinical
severe symptoms are significant only with regard to sIL-2R in
erythrodermic patients. Furthermore, it has been established that
tissue-based lymphoma cells express low levels of sIL-2R, whilst
large-cell transformation in CTCL contributes to lowering high
levels of sIL-2R in several patients. Besides sIL-2R, other two
molecules-neopterin and β2-microglobulin seem to express
significant high levels in serum samples from patients suffering
from Sézary syndrome. Of these considered biomarkers, only sIL-2R
appears to be the most sensitive; nevertheless, in terms of
prognosis, only neopterin revealed a substantial significance in
nonleukemic CTCL patients (57).
Circulating markers like neopterin,
β2-microglobulin, sIL-2R, IL-6 and −4 have been described to be
elevated in various malignancies. Studies show that increased
cytoplasmic IL-4 is the sole predictor of advanced CTCL disease.
Concerning the outcome of the disease (progression versus
non-progression), only neopterin showed a significant prognostic
value in CTCL patients (58).
The histological and molecular characteristics play
a key-role in establishing the prognosis of CTLC. Various protein
biomarkers useful in CTLC diagnosis have been established,
comprising CD2, CD3, CD4, CD5, CD7, CD8, CD14, CD16/56, CD19, CD25,
CD45, CD45RA, CD45R0. Moshkovskii et al analyzed the
differential cytokine expressions of IL-1Ra, IL-4, G-CSF, IP-10 in
serum samples of MF in the attempt to estimate the probability of
an accurate diagnosis based on serum protein profiling using mass
spectrometry SELDI-TOF. In their study, the authors concluded that
IP-10 may be considered a candidate biomarker for the
differentiation between MF and other skin conditions (59,60).
Moreover, molecules engaged in signaling pathways,
regulation of cellular proliferation, and apoptosis such as Jun,
Myc, c-myb, p53, STATs, Bcl-2, Fas/CD95 and SOCS-3, or involved in
immunopathology such as expression of inhibitory MHC receptors
(ILT2/CD85j), NK receptors (p140/KIR3DL2) and dendritic cell
defects (CD40 abnormal expression) could be of significant
relevance concerning CTLC prognosis (61). There are few studies on the
characterization of DCs in cancer, with implication of their
expression of CD40. It is well recognized that CD40 is a
co-stimulatory molecule, belonging to the tumor necrosis factor
superfamily, essential in DCs activation, and suggested that CD40
expression in DCs is impaired in cancer, particularly in metastatic
disease.
It has been highlighted that aberrant activation of
the JAK/STAT signaling pathway was encountered in almost all T-cell
lymphomas, leading to activation of pathways downstream of the
T-cell receptor (TCR), co-stimulatory proteins, and/or cytokine
receptors (62,63). Considering the high prevalence of
CTCL, it is necessary to determine specific biomarkers in order to
discriminate between more or less aggressive forms CTLC.
In this regard, future studies are needed to
establish the suitable biomarkers for an accurate early diagnostic
of cutaneous lymphoma. The integration of proteomics into clinical
practice needs a high-throughput laboratory infrastructure, leading
to the development of personalized medicine, adapting the specific
biomarkers to application of cancer-type specific drug targets to
individuals.
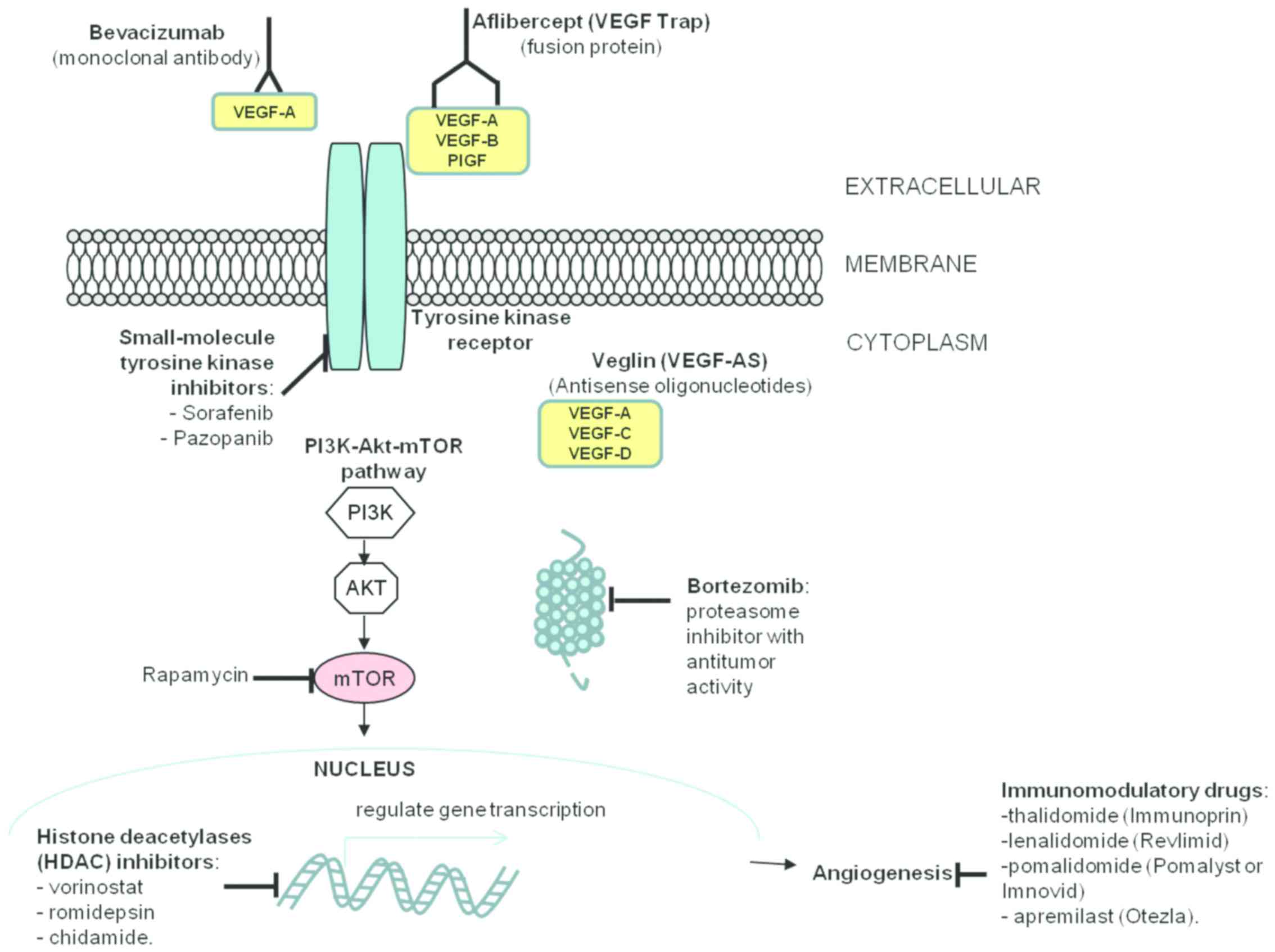
Molecular targets in vascular niche
factors
The growing list of antiangiogenic therapies
available (summarized in Fig. 2)
includes:
i) Direct anti-VEGF (bevacizumab, VEGF-Trap,
VEGF-antisense); due to the importance of the VEGF axis for the
angiogenic process, research efforts focused on direct targeting of
VEGF. The prototypic therapeutic agent is the humanized monoclonal
antibody bevacizumab, which in combination with chemotherapy
improves progression free-survival for patients with metastatic
colorectal, renal, breast and advanced non-small cell lung cancer
(64–66). Other strategies directly targeting
VEGF include the use of antisense oligonucleotides against VEGF,
reported to cause a partial response in one CTCL patient (14) and aflibercept (VEGF Trap), a fusion
protein consisting of the extracellular domains of VEGFR receptors
1 and 2 fused to the Fc portion of human IgG. Aflibercept was
reported to be well tolerated and have antitumoral activity in
patients with advanced solid tumors in a phase I clinical trial
(67).
ii) Immunomodulatory drugs with antiangiogenic
properties; this group includes a number of anticancer agents,
among which the prototype drug thalidomide (Immunoprin) (68), and its more recently developed
analogues: Lenalidomide (Revlimid), pomalidomide (Pomalyst or
Imnovid) and apremilast (Otezla). A phase III clinical study of
lenalidomide maintenance after debulking therapy in patients with
advanced CTCL revealed that lenalidomide maintenance increased
progression free survival. However, these results were not
statistically significant due to the reduced number of patients
enrolled in the study (69,70).
iii) Metronomic chemotherapy refers to the
administration of relatively low doses of medications at close
regular intervals without prolonged drug-free break periods rather
than the conventional ‘maximum tolerated dose’ (71). This approach preferentially damages
endothelial cells in tumor blood vessels presumably due to a
simultaneous blockade of VEGF-A blunting a key survival signal for
endothelial cells, thus selectively amplifying the endothelial cell
targeting effects of chemotherapy, leading to improved subsequent
killing of cancer cells (72).
iv) Other novel antiangiogenic strategies, which
include: a) Mammalian target of rapamycin (mTOR) inhibitors; mTOR
inhibitors have shown antiangiogenic activity by inhibiting VEGF
production through HIF-1α (73,74) and
mTOR has emerged a promising target for cancer therapy in both
solid and hematological tumors. Primary cells from patients with
CTCL or Sézary syndrome were reported to be sensitive to rapamycin
(75) and the inhibition of mTOR was
shown to induce apoptosis in CTCL cells (76); b) HDAC inhibitors; the first clinical
data to support the use of HDAC inhibitors in CTCL came from a 2001
phase-1 trial that looked at the effect of romidepsin on a variety
of cancers. The 3 patients with CTCL enrolled had partial
remission, while a PTCL patient had complete remission (77). Currently, HDAC inhibitors approved for
the treatment of CTCL include vorinostat; c) Proteasome inhibitors;
ubiquitin-proteasome pathway inhibition in tumor cells impedes
tumor growth by inducing cell cycle arrest, apoptosis and
inhibiting tumor metastasis and angiogenesis. Bortezomib is a
proteasome inhibitor with antitumor activity (78,79) that
has several downstream effects, including activation of p53,
inhibition of NF-κB and accumulation of pro-apoptotic proteins
(80). Bortezomib was approved in
2003 by the FDA for the treatment of multiple myeloma and for
relapsed or refractory mantle cell lymphoma (81,82) and
several reports and clinical trials reveal that it can also be used
for the treatment of solid tumors, alone or in combination
(83–85). Bortezomib has shown promising results
in patients with relapsed or refractory CTCL (86–88).
Conclusion
Neoangiogenesis plays potentially important
pathogenic roles in CTLC initiation and prognostic, by stimulating
homing of tumor cells and generation of pro-proliferative soluble
cues. The main signaling pathway involved in autocrine stimulation
of proliferation and survival of lymphoma tumor cells is VEGF-VEGF
receptor axis, although other axes, described in homing studies
(CXCR4/CXCL12) or signaling pathways (JAK3/STAT5) associated with
hematopoietic development were recently associated with clinical
and fundamental studies of CTLC. Proteomic studies are useful to
highlight more members of these signaling pathways that are
modified in the lesions or serum of patients and that may be used
in prognostic or therapy follow-up. These studies can also
highlight novel molecular therapy targets, possibly some with
higher specificity for characterized subsets of patients, in the
framework of personalized medicine.
Acknowledgements
We would like to thank Ms. Irina Radu, certified
translator in Medicine and Pharmacy (certificate credentials:
series E no. 0048), for professional linguistic assistance.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CT, IDP, AME, AAGG, EC, SM, LA, LN and RA
contributed to the gathering of the data, writing the manuscript
and revising it critically for an important intellectual content.
All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
VEGF
|
vascular endothelial growth factor
|
|
VEGFR
|
vascular endothelial growth factor
receptor
|
|
bFGF
|
basic fibroblast growth factor
|
|
PIGF
|
placenta growth factor
|
|
STAT
|
signal transducer and activator of
transcription
|
|
JAK
|
Janus kinase
|
|
CCL20
|
chemokine (C-C motif) ligand 20
|
|
CCR6
|
C-C motif chemokine receptor 6
|
|
PDPN
|
podoplanin
|
|
LYVE-1
|
lymphatic vessel hyaluronan
receptor-1
|
|
LTα
|
lymphotoxin-α
|
|
CXCR4
|
C-X-C chemokine receptor type 4
|
|
CXCL12
|
C-X-C motif chemokine ligand 12
|
|
TP53
|
tumor protein p53
|
|
RB1
|
retinoblastoma protein 1
|
|
PTEN
|
phosphatase and tensin homolog
|
|
DNMT3A
|
DNA methyltransferase 3α
|
|
CDKN1B
|
cyclin-dependent kinase inhibitor
1B
|
|
TET2
|
tet methylcytosine dioxygenase 2
|
|
CREBBP
|
CREB binding protein
|
|
CREB
|
cAMP-response element binding
protein
|
|
KMT2D (MLL2)
|
histone-lysine N-methyltransferase
2D
|
|
KMT2C (MLL3)
|
lysine N-methyltransferase 2C
|
|
BRD9
|
bromodomain-containing protein 9
|
|
SMARCA4
|
transcription activator BRG1
|
|
CHD3
|
chromodomain helicase DNA binding
protein 3
|
|
MAPK1
|
mitogen-activated protein kinase 1
|
|
BRAF
|
v-raf murine sarcoma viral oncogene
homolog B1
|
|
CARD11
|
caspase recruitment domain-containing
protein 11
|
|
PRKG1
|
cGMP-dependent protein kinase 1
|
|
NF-κB
|
nuclear factor-κB
|
|
NFAT
|
nuclear factor of activated
T-cells
|
|
SDF1
|
stromal cell-derived factor 1
|
|
CXCL12
|
C-X-C motif chemokine ligand 12
|
|
Ang1
|
angiopoietin 1
|
|
Tie2
|
angiopoietin receptor
|
|
LDH
|
lactate dehydrogenase
|
|
G-CSF
|
granulocyte colony-stimulating
factor
|
|
IP-10
|
interferon γ-induced protein 10
|
|
Jun
|
AP-1 transcription factor
|
|
Bcl-2
|
B-cell lymphoma 2
|
|
SOCS-3
|
suppressor of cytokine signaling-3
|
References
|
1
|
Patterson-Fortin J and Moliterno AR:
Molecular pathogenesis of myeloproliferative neoplasms: Influence
of age and gender. Curr Hematol Malig Rep. 12:424–431. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kwan W and North TE: Netting novel
regulators of hematopoiesis and hematologic malignancies in
zebrafish. Curr Top Dev Biol. 124:125–160. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Deininger MW, Tyner JW and Solary E:
Turning the tide in myelodysplastic/myeloproliferative neoplasms.
Nat Rev Cancer. 17:425–440. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Swerdlow SH, Harris NL, Campo E, Pileri
SA, Stein H, Jaffe ES and Thiele J: WHO Classification of Tumors of
Haematopoietic and Lymphoid Tissues. 2. 4th. IARC press; Lyon:
2017
|
|
5
|
Jiang M, Bennani NN and Feldman AL:
Lymphoma classification update: T-cell lymphomas, Hodgkin
lymphomas, and histiocytic/dendritic cell neoplasms. Expert Rev
Hematol. 10:239–249. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Swerdlow SH, Campo E, Pileri SA, Harris
NL, Stein H, Siebert R, Advani R, Ghielmini M, Salles GA, Zelenetz
AD, et al: The 2016 revision of the World Health Organization
classification of lymphoid neoplasms. Blood. 127:2375–2390. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Matutes E: The 2017 WHO update on mature
T- and natural killer (NK) cell neoplasms. Int J Lab Hematol.
40:97–103. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lupu M, Caruntu A, Caruntu C, Papagheorghe
LML, Ilie MA, Voiculescu V, Boda D, Constantin C, Tanase C, Sifaki
M, et al: Neuroendocrine factors: The missing link in non melanoma
skin cancer (Review). Oncol Rep. 38:1327–1340. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Scarisbrick JJ, Hodak E, Bagot M,
Stranzenbach R, Stadler R, Ortiz-Romero PL, Papadavid E, Evison F,
Knobler R, Quaglino P, et al: Blood classification and blood
response criteria in mycosis fungoides and Sézary syndrome using
flow cytometry: Recommendations from the EORTC cutaneous lymphoma
task force. Eur J Cancer. 93:47–56. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shahrabi S, Rezaeeyan H, Ahmadzadeh A,
Shahjahani M and Saki N: Bone marrow blood vessels: Normal and
neoplastic niche. Oncol Rev. 10:3062016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vacca A, Moretti S, Ribatti D, Pellegrino
A, Pimpinelli N, Bianchi B, Bonifazi E, Ria R, Serio G and Dammacco
F: Progression of mycosis fungoides is associated with changes in
angiogenesis and expression of the matrix metalloproteinases 2 and
9. Eur J Cancer. 33:1685–1692. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mazur G, Woźniak Z, Wróbel T, Maj J and
Kuliczkowski K: Increased angiogenesis in cutaneous T-cell
lymphomas. Pathol Oncol Res. 10:34–36. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Miyagaki T, Sugaya M, Oka T, Takahashi N,
Kawaguchi M, Suga H, Fujita H, Yoshizaki A, Asano Y and Sato S:
Placental growth factor and vascular endothelial growth factor
together regulate tumour progression via increased vasculature in
cutaneous T-cell lymphoma. Acta Derm Venereol. 97:586–592. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Levine AM, Tulpule A, Quinn DI, Gorospe G
III, Smith DL, Hornor L, Boswell WD, Espina BM, Groshen SG, Masood
R, et al: Phase I study of antisense oligonucleotide against
vascular endothelial growth factor: Decrease in plasma vascular
endothelial growth factor with potential clinical efficacy. J Clin
Oncol. 24:1712–1719. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zain J and O'Connor OA: Targeting histone
deacetylases in the treatment of B- and T-cell malignancies. Invest
New Drugs. 28:S58–S78. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Litvinov IV, Netchiporouk E, Cordeiro B,
Zargham H, Pehr K, Gilbert M, Zhou Y, Moreau L, Woetmann A, Ødum N,
et al: Ectopic expression of embryonic stem cell and other
developmental genes in cutaneous T-cell lymphoma. OncoImmunology.
3:e9700252014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tanase C, Albulescu R, Codrici E, Calenic
B, Popescu ID, Mihai S, Necula L, Cruceru ML and Hinescu ME:
Decreased expression of APAF-1 and increased expression of
cathepsin B in invasive pituitary adenoma. OncoTargets Ther.
8:81–90. 2014. View Article : Google Scholar
|
|
18
|
Sibbesen NA, Kopp KL, Litvinov IV, Jønson
L, Willerslev-Olsen A, Fredholm S, Petersen DL, Nastasi C,
Krejsgaard T, Lindahl LM, et al: Jak3, STAT3, and STAT5 inhibit
expression of miR-22, a novel tumor suppressor microRNA, in
cutaneous T-Cell lymphoma. Oncotarget. 6:20555–20569. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bagherani N and Smoller BR: An overview of
cutaneous T cell lymphomas. F1000 Res. 5:52016. View Article : Google Scholar
|
|
20
|
Kabasawa M, Sugaya M, Oka T, Takahashi N,
Kawaguchi M, Suga H, Miyagaki T, Takahashi T, Shibata S, Fujita H,
et al: Decreased interleukin-21 expression in skin and blood in
advanced mycosis fungoides. J Dermatol. 43:819–822. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vieyra-Garcia PA, Wei T, Naym DG, Fredholm
S, Fink-Puches R, Cerroni L, Odum N, O'Malley JT, Gniadecki R and
Wolf P: STAT3/5-dependent IL9 overexpression contributes to
neoplastic cell survival in mycosis fungoides. Clin Cancer Res.
22:3328–3339. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ikeda S, Kitadate A, Ito M, Abe F, Nara M,
Watanabe A, Takahashi N, Miyagaki T, Sugaya M and Tagawa H:
Disruption of CCL20-CCR6 interaction inhibits metastasis of
advanced cutaneous T-cell lymphoma. Oncotarget. 7:13563–13574.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lauenborg B, Christensen L, Ralfkiaer U,
Kopp KL, Jønson L, Dabelsteen S, Bonefeld CM, Geisler C, Gjerdrum
LM, Zhang Q, et al: Malignant T-cells express lymphotoxin α and
drive endothelial activation in cutaneous T-cell lymphoma.
Oncotarget. 6:15235–15249. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Maj J, Jankowska-Konsur AM, Hałoń A,
Woźniak Z, Plomer-Niezgoda E and Reich A: Expression of CXCR4 and
CXCL12 and their correlations to the cell proliferation and
angiogenesis in mycosis fungoides. Postepy Dermatol Alergol.
32:437–442. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gallardo F, Sandoval J, Díaz-Lagares A,
Garcia R, D'Altri T, González J, Alegre V, Servitje O, Crujeiras
AB, Stefánsson ÓA, et al: Notch1 pathway activation results from
the epigenetic abrogation of notch-related microRNAs in mycosis
fungoides. J Invest Dermatol. 135:3144–3152. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lindahl LM, Fredholm S, Joseph C, Nielsen
BS, Jønson L, Willerslev-Olsen A, Gluud M, Blümel E, Petersen DL,
Sibbesen N, et al: STAT5 induces miR-21 expression in cutaneous T
cell lymphoma. Oncotarget. 7:45730–45744. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Abe F, Kitadate A, Ikeda S, Yamashita J,
Nakanishi H, Takahashi N, Asaka C, Teshima K, Miyagaki T, Sugaya M,
et al: Histone deacetylase inhibitors inhibit metastasis by
restoring a tumor suppressive microRNA-150 in advanced cutaneous
T-cell lymphoma. Oncotarget. 8:7572–7585. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
da Silva Almeida AC, Abate F, Khiabanian
H, Martinez-Escala E, Guitart J, Tensen CP, Vermeer MH, Rabadan R,
Ferrando A and Palomero T: The mutational landscape of cutaneous
T-cell lymphoma and Sézary syndrome. Nat Genet. 47:1465–1470. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bosseila M, Sayed Sayed K, El-Din Sayed SS
and Abd El Monaem A: Evaluation of angiogenesis in early mycosis
fungoides patients: Dermoscopic and immunohistochemical study.
Dermatology. 231:82–86. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gratzinger D, Zhao S, Tibshirani RJ, Hsi
ED, Hans CP, Pohlman B, Bast M, Avigdor A, Schiby G, Nagler A, et
al: Prognostic significance of VEGF, VEGF receptors, and
microvessel density in diffuse large B cell lymphoma treated with
anthracycline-based chemotherapy. Lab Invest. 88:38–47. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Mendt M and Cardier JE: Stromal-derived
factor-1 and its receptor, CXCR4, are constitutively expressed by
mouse liver sinusoidal endothelial cells: Implications for the
regulation of hematopoietic cell migration to the liver during
extramedullary hematopoiesis. Stem Cells Dev. 21:2142–2151. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Daggett RN, Kurata M, Abe S, Onishi I,
Miura K, Sawada Y, Tanizawa T and Kitagawa M: Expression dynamics
of CXCL12 and CXCR4 during the progression of mycosis fungoides. Br
J Dermatol. 171:722–731. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Arai F, Hirao A, Ohmura M, Sato H,
Matsuoka S, Takubo K, Ito K, Koh GY and Suda T: Tie2/angiopoietin-1
signaling regulates hematopoietic stem cell quiescence in the bone
marrow niche. Cell. 118:149–161. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kawaguchi M, Sugaya M, Suga H, Miyagaki T,
Ohmatsu H, Fujita H, Asano Y, Tada Y, Kadono T and Sato S: Serum
levels of angiopoietin-2, but not angiopoietin-1, are elevated in
patients with erythrodermic cutaneous T-cell lymphoma. Acta Derm
Venereol. 94:9–13. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Alshenawy HA: Prognostic significance of
vascular endothelial growth factor, basic fibroblastic growth
factor, and microvessel density and their relation to cell
proliferation in B-cell non-Hodgkin's lymphoma. Ann Diagn Pathol.
14:321–327. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lauenborg B, Litvinov IV, Zhou Y,
Willerslev-Olsen A, Bonefeld CM, Nastasi C, Fredholm S, Lindahl LM,
Sasseville D, Geisler C, et al: Malignant T-cells activate
endothelial cells via IL-17 F. Blood Cancer J. 7:e5862017.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Furudate S, Fujimura T, Kakizaki A,
Kambayashi Y, Asano M, Watabe A and Aiba S: The possible
interaction between periostin expressed by cancer stroma and
tumor-associated macrophages in developing mycosis fungoides. Exp
Dermatol. 25:107–112. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tuzova M, Richmond J, Wolpowitz D,
Curiel-Lewandrowski C, Chaney K, Kupper T and Cruikshank W:
CCR4+ T-cell recruitment to the skin in mycosis
fungoides: Potential contributions by thymic stromal lymphopoietin
and interleukin-16. Leuk Lymphoma. 56:440–449. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hashikawa K, Yasumoto S, Nakashima K,
Arakawa F, Kiyasu J, Kimura Y, Saruta H, Nakama T, Yasuda K,
Tashiro K, et al: Microarray analysis of gene expression by
microdissected epidermis and dermis in mycosis fungoides and adult
T-cell leukemia/lymphoma. Int J Oncol. 45:1200–1208. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Furudate S, Fujimura T, Kakizaki A, Hidaka
T, Asano M and Aiba S: Tumor-associated M2 macrophages in mycosis
fungoides acquire immunomodulatory function by interferon alpha and
interferon gamma. J Dermatol Sci. 83:182–189. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Fujimura T, Kambayashi Y, Fujisawa Y,
Hidaka T and Aiba S: Tumor-associated macrophages: Therapeutic
targets for skin cancer. Front Oncol. 8:32018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Humphrey RL, Karpetsky TP, Neuwelt EA and
Levy CC: Levels of serum ribonuclease as an indicator of renal
insufficiency in patients with leukemia. Cancer Res. 37:2015–2022.
1977.PubMed/NCBI
|
|
43
|
Serban M, Cucu C, Mihăilescu E and Micu D:
Value of ribonuclease and guanase activity for the diagnosis of
leukemias. Rev Roum Med Intern. 11:319–324. 1974.PubMed/NCBI
|
|
44
|
Biomarkers Definitions Working G;
Biomarkers Definitions Working Group, : Biomarkers and surrogate
endpoints: Preferred definitions and conceptual framework. Clin
Pharmacol Ther. 69:89–95. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Pistol-Tanase C, Raducan E, Dima SO,
Albulescu L, Alina I, Marius P, Cruceru LM, Codorean E, Neagu TM
and Popescu I: Assessment of soluble angiogenic markers in
pancreatic cancer. Biomarkers Med. 2:447–455. 2008. View Article : Google Scholar
|
|
46
|
FDA-NIH Biomarker Working Group, : BEST
(Biomarkers, EndpointS, and other Tools) Resource (Internet).
Silver Spring; MA, USA: 2016
|
|
47
|
Caruntu C, Boda D, Dumitrascu G,
Constantin C and Neagu M: Proteomics focusing on immune markers in
psoriatic arthritis. Biomarkers Med. 9:513–528. 2015. View Article : Google Scholar
|
|
48
|
Neagu M, Caruntu C, Constantin C, Boda D,
Zurac S, Spandidos DA and Tsatsakis AM: Chemically induced skin
carcinogenesis: Updates in experimental models. (Review) Oncol Rep.
35:2516–2528. 2016. View Article : Google Scholar
|
|
49
|
Mihai S, Codrici E, Popescu ID, Enciu AM,
Rusu E, Zilisteanu D, Albulescu R, Anton G and Tanase C: Proteomic
biomarkers panel: New insights in chronic kidney disease. Dis
Markers. 2016:31852322016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Matei C, Tampa M, Caruntu C, Ion RM,
Georgescu SR, Dumitrascu GR, Constantin C and Neagu M: Protein
microarray for complex apoptosis monitoring of dysplastic oral
keratinocytes in experimental photodynamic therapy. Biol Res.
47:332014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Tanase CP, Albulescu R and Neagu M:
Application of 3D hydrogel microarrays in molecular diagnostics:
Advantages and limitations. Expert Rev Mol Diagn. 11:461–464. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Caruntu C: Catecholamines increase in
vitro proliferation of murine B16F10 melanoma cells. Acta
Endocrinol (Bucur). 10:545–558. 2014. View Article : Google Scholar
|
|
53
|
Boda D: Cellomics as integrative omics for
cancer. Curr Proteomics. 10:237–245. 2013. View Article : Google Scholar
|
|
54
|
Zurac S, Neagu M, Constantin C, Cioplea M,
Nedelcu R, Bastian A, Popp C, Nichita L, Andrei R, Tebeica T, et
al: Variations in the expression of TIMP1, TIMP2 and TIMP3 in
cutaneous melanoma with regression and their possible function as
prognostic predictors. Oncol Lett. 11:3354–3360. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Ion A, Popa IM, Papagheorghe LM, Lisievici
C, Lupu M, Voiculescu V, Caruntu C and Boda D: Proteomic approaches
to biomarker discovery in cutaneous T-cell lymphoma. Dis Markers.
2016:96024722016. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Igreja C, Courinha M, Cachaço AS, Pereira
T, Cabeçadas J, Da Silva MG and Dias S: Characterization and
clinical relevance of circulating and biopsy-derived endothelial
progenitor cells in lymphoma patients. Haematologica. 92:469–477.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Schadendorf D, Matharoo-Ball B, Rees R,
Ugurel S and Utikal J: Prognostic biomarkers of cutaneous
malignancies - serological, immunohistochemical and proteomic
approaches. Curr Cancer Ther Rev. 4:96–104. 2008. View Article : Google Scholar
|
|
58
|
Hassel JC, Meier R, Joller-Jemelka H, Burg
G and Dummer R: Serological immunomarkers in cutaneous T-cell
lymphoma. Dermatology. 209:296–300. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Moshkovskii SA, Sokolova EE, Brattseva EV,
Karpova MA, Pyatnitskiy MA, Kubanova AA and Archakov AI: Proteome
and cytokine serum profiling to diagnose a mycosis fungoides.
Proteomics Clin Appl. 5:432–439. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Popescu I, Raducan E, Dinischiotu A and
Tanase C: Applications of SELDI-TOF technology in cancer biomarkers
discovery. Rom Biotechnol Lett. 15:5654–5667. 2010.
|
|
61
|
Wilcox RA: Cutaneous T-cell lymphoma: 2017
update on diagnosis, risk-stratification, and management. Am J
Hematol. 92:1085–1102. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Van Arnam JS, Lim MS and Elenitoba-Johnson
KSJ: Novel insights into the pathogenesis of T-cell lymphomas.
Blood. 131:2320–2330. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Kataoka K, Nagata Y, Kitanaka A, Shiraishi
Y, Shimamura T, Yasunaga J, Totoki Y, Chiba K, Sato-Otsubo A, Nagae
G, et al: Integrated molecular analysis of adult T cell
leukemia/lymphoma. Nat Genet. 47:1304–1315. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Hurwitz H, Fehrenbacher L, Novotny W,
Cartwright T, Hainsworth J, Heim W, Berlin J, Baron A, Griffing S,
Holmgren E, et al: Bevacizumab plus irinotecan, fluorouracil, and
leucovorin for metastatic colorectal cancer. N Engl J Med.
350:2335–2342. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Sandler A, Gray R, Perry MC, Brahmer J,
Schiller JH, Dowlati A, Lilenbaum R and Johnson DH:
Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell
lung cancer. N Engl J Med. 355:2542–2550. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Miller KD: E2100: A phase III trial of
paclitaxel versus paclitaxel/bevacizumab for metastatic breast
cancer. Clin Breast Cancer. 3:421–422. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Lockhart AC, Rothenberg ML, Dupont J,
Cooper W, Chevalier P, Sternas L, Buzenet G, Koehler E, Sosman JA,
Schwartz LH, et al: Phase I study of intravenous vascular
endothelial growth factor trap, aflibercept, in patients with
advanced solid tumors. J Clin Oncol. 28:207–214. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
D'Amato RJ, Loughnan MS, Flynn E and
Folkman J: Thalidomide is an inhibitor of angiogenesis. Proc Natl
Acad Sci USA. 91:4082–4085. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Bagot M, Hasan B, Whittaker S,
Beylot-Barry M, Knobler R, Shah E, Marreaud S, Morris S, Dalle S,
Servitje O, et al: A phase III study of lenalidomide maintenance
after debulking therapy in patients with advanced cutaneous T-cell
lymphoma; EORTC 21081 (NCT01098656): Results and lessons learned
for future trial designs. Eur J Dermatol. 27:286–294.
2017.PubMed/NCBI
|
|
70
|
Neagu M, Constantin C and Zurac S: Immune
parameters in the prognosis and therapy monitoring of cutaneous
melanoma patients: Experience, role, and limitations. BioMed Res
Int. 2013:1079402013. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Ferrara N and Kerbel RS: Angiogenesis as a
therapeutic target. Nature. 438:967–974. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Shaked Y, Ciarrocchi A, Franco M, Lee CR,
Man S, Cheung AM, Hicklin DJ, Chaplin D, Foster FS, Benezra R, et
al: Therapy-induced acute recruitment of circulating endothelial
progenitor cells to tumors. Science. 313:1785–1787. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Mayerhofer M, Valent P, Sperr WR, Griffin
JD and Sillaber C: BCR/ABL induces expression of vascular
endothelial growth factor and its transcriptional activator,
hypoxia inducible factor-1alpha, through a pathway involving
phosphoinositide 3-kinase and the mammalian target of rapamycin.
Blood. 100:3767–3775. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Guba M, von Breitenbuch P, Steinbauer M,
Koehl G, Flegel S, Hornung M, Bruns CJ, Zuelke C, Farkas S,
Anthuber M, et al: Rapamycin inhibits primary and metastatic tumor
growth by antiangiogenesis: Involvement of vascular endothelial
growth factor. Nat Med. 8:128–135. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Kremer M, Sliva K, Klemke CD and Schnierle
BS: Cutaneous T-cell lymphoma cells are sensitive to rapamycin. Exp
Dermatol. 19:800–805. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Marzec M, Liu X, Wysocka M, Rook AH, Odum
N and Wasik MA: Simultaneous inhibition of mTOR-containing complex
1 (mTORC1) and MNK induces apoptosis of cutaneous T-cell lymphoma
(CTCL) cells. PLoS One. 6:e248492011. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Piekarz RL, Robey R, Sandor V, Bakke S,
Wilson WH, Dahmoush L, Kingma DM, Turner ML, Altemus R and Bates
SE: Inhibitor of histone deacetylation, depsipeptide, in the
treatment of peripheral and cutaneous T-cell lymphoma: A case
report. Blood. 98:2865–2868. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Hideshima T, Richardson P, Chauhan D,
Palombella VJ, Elliott PJ, Adams J and Anderson KC: The proteasome
inhibitor PS-341 inhibits growth, induces apoptosis, and overcomes
drug resistance in human multiple myeloma cells. Cancer Res.
61:3071–3076. 2001.PubMed/NCBI
|
|
79
|
Shah JJ and Orlowski RZ: Proteasome
inhibitors in the treatment of multiple myeloma. Leukemia.
23:1964–1979. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Jain S, Zain J and O'Connor O: Novel
therapeutic agents for cutaneous T-cell lymphoma. J Hematol Oncol.
5:242012. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Buac D, Shen M, Schmitt S, Kona FR,
Deshmukh R, Zhang Z, Neslund-Dudas C, Mitra B and Dou QP: From
bortezomib to other inhibitors of the proteasome and beyond. Curr
Pharm Des. 19:4025–4038. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Orlowski RZ and Kuhn DJ: Proteasome
inhibitors in cancer therapy: lessons from the first decade. Clin
Cancer Res. 14:1649–1657. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Kozuch PS, Rocha-Lima CM, Dragovich T,
Hochster H, O'Neil BH, Atiq OT, Pipas JM, Ryan DP and Lenz HJ:
Bortezomib with or without irinotecan in relapsed or refractory
colorectal cancer: Results from a randomized phase II study. J Clin
Oncol. 26:2320–2326. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Morris MJ, Kelly WK, Slovin S, Ryan C,
Eicher C, Heller G and Scher HI: A phase II trial of bortezomib and
prednisone for castration resistant metastatic prostate cancer. J
Urol. 178:2378–2383. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Schmid P, Kühnhardt D, Kiewe P,
Lehenbauer-Dehm S, Schippinger W, Greil R, Lange W, Preiss J,
Niederle N, Brossart P, et al: A phase I/II study of bortezomib and
capecitabine in patients with metastatic breast cancer previously
treated with taxanes and/or anthracyclines. Ann Oncol. 19:871–876.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Heider U, Rademacher J, Lamottke B, Mieth
M, Moebs M, von Metzler I, Assaf C and Sezer O: Synergistic
interaction of the histone deacetylase inhibitor SAHA with the
proteasome inhibitor bortezomib in cutaneous T-cell lymphoma. Eur J
Haematol. 82:440–449. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Kim SJ, Yoon DH, Kang HJ, Kim JS, Park SK,
Kim HJ, Lee J, Ryoo BY, Ko YH, Huh J, et al: Consortium for
improving survival of lymphoma (CISL) investigators: Bortezomib in
combination with CHOP as first-line treatment for patients with
stage III/IV peripheral T-cell lymphomas: A multicentre,
single-arm, phase 2 trial. Eur J Cancer. 48:3223–3231. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Zinzani PL, Musuraca G, Tani M, Stefoni V,
Marchi E, Fina M, Pellegrini C, Alinari L, Derenzini E, de Vivo A,
et al: Phase II trial of proteasome inhibitor bortezomib in
patients with relapsed or refractory cutaneous T-cell lymphoma. J
Clin Oncol. 25:4293–4297. 2007. View Article : Google Scholar : PubMed/NCBI
|