Introduction
For pancreatic ductal adenocarcinoma (PDAC), one of
the deadliest malignant diseases (1,2), there
has been poor progress in the development of new effective
treatments. Surgical resection is still to date the only
potentially curative treatment. However, only about 20% of patients
present tumors eligible for resection at time of diagnosis
(1). Despite surgery, many patients
relapse or develop metastasizing disease (3,4). Hence,
there is a need for therapy improvement and specific biomarkers
that predict patient outcome or that can guide individualized
treatment after surgery.
Epithelial growth factor receptor (EGFR) has been
extensively studied in PDAC (5).
EGFR protein overexpression has been reported in 40–70% of
pancreatic cancers (6,7), with variable association with survival
(8). Erlotinib, a small molecule
EGFR inhibitor, is in clinical use in combination with gemcitabine
for unresectable locally advanced or metastatic PDAC (9,10). The
effectiveness of erlotinib in resected PDAC is less studied and
remains unclear (11,12). Recent experimental studies by Ardito
et al (13) and Navas et
al (14) showing that knock-out
of Egfr in KRAS-mutated mice completely blocked development
of PDAC, suggest a critical role for EGFR activation in the
pathogenesis of human KRAS-driven PDAC.
Cyclooxygenase-2 (COX-2), far less studied than EGFR
in PDAC, has also been reported to be overexpressed in 60 to 70% of
tumor patients (15,16). The association with survival is
unclear (17–22). Further, no anti-COX-2 treatment has
yet been proven effective in PDAC patients in combination with
chemotherapy (23). Activation of
COX-2 signaling has been reported to promote PDAC tumor growth in
experimental models (24,25).
EGFR and COX-2 signaling pathways have been
suggested to be linked. This has been reported in experimental
studies of colorectal cancer and head and neck cancer, where EGFR
is shown to upregulate COX-2 or vice versa (26,27).
However, whether there is a link in human PDAC is currently
unknown.
The effects of EGFR and COX-2 protein overexpression
on clinical outcomes in PDAC patients remain unclear. Therefore,
the aim of this study was to explore the prognostic and
clinicopathological significance of both EGFR and COX-2 protein
expression in tumor cells in patients with surgically resected PDAC
aimed at cure.
Materials and methods
Patients and tumor tissue samples
Pancreatic tumor tissue sections were obtained from
32 patients with pancreatic ductal adenocarcinoma who underwent
surgical tumor resection in 1998 to 2005 at Sahlgrenska University
Hospital, Gothenburg, Sweden. All patients underwent surgery as
primary treatment and none had received neoadjuvant chemotherapy.
The group of patients consisted of 53% males and 47% females with a
mean age of 64.1 years (range 50 to 80 years) at surgery. Median
overall survival was 22.9 months (range 1.1 to 122.4 months) after
surgery. All the tumors were histologically diagnosed as ductal
adenocarcinoma and classified according to the TNM staging system
by the Pathology department at Sahlgrenska University Hospital. The
present study was approved by the Regional Ethical Review Board in
Gothenburg, Sweden (reference number 002-06) and all participants
gave written informed consent. Data was analyzed anonymously.
Histology and
immunohistochemistry
Pancreatic tumor tissues were fixed in 10%
neutral-buffered formalin and embedded in paraffin. Sections of 4
µm were prepared. Immunohistochemistry (IHC) was performed as
follows: After xylene deparaffinization, ethanol dehydration and
antigen retrieval (water bath for 30 min at 98°C in citrate buffer
pH 6.0), sections were first blocked with 5% non-fat milk in 5 mM
Tris-buffered saline (TBS), pH 7.8 for 30 min and then endogenous
peroxidase activity was quenched in 0.3% H2O2
solution (Dual Endogenous Enzyme Block, Dako Envision K4065,
Agilent Technologies, Santa Clara, CA, USA) for 15 min. Sections
were incubated with primary antibodies diluted in 5% non-fat milk
in TBS overnight at 4°C, followed by incubation with polymer
labelled secondary antibodies conjugated with HRP (Labelled
polymer-HRP, Dako Envision K4065, Agilent Technologies), for 40 min
at room temperature. Bound peroxidase was visualized by 15 min
incubation in a 3,3′-diaminobenzidine (DAB) solution (Dako Envision
K4065, Agilent Technologies). Sections were washed, counterstained
with hematoxylin, dehydrated and mounted. The following antibodies
were used: Monoclonal mouse anti-human wild-type EGFR (detects the
membranous N-terminal part of the extracellular domain, but not the
2–7 truncated EGFR variant (EGFR-vIII), immunizing peptide aa
30–198), clone DAK H1 WT, M7298, Agilent Technologies, dilution
1:50, polyclonal rabbit anti-COX-2 (cytosolic detection), ab15191,
Abcam, Cambridge, UK, dilution 1:200, negative control mouse IgG1
(X0931, Agilent Technologies) and rabbit IgG1 (X0903, Agilent
Technologies) diluted in 5% non-fat milk in TBS. Negative control
antibodies were diluted to the same protein concentration as the
primary antibody. Methodology has been used and described
previously (28,29).
Scoring of immunohistochemical
stainings
Tumor tissue samples were evaluated for membranous
EGFR and cytoplasmic COX-2 staining using a histoscore (H-score)
system. Staining intensity of EGFR and COX-2 protein expression was
scored from negative (score=0), low (score=1), intermediate
(score=2) to high (score=3). The percentage of tumor cells showing
positive staining was assessed separately. For both staining
intensity and percentage of tumor cells, 10 high magnification
(×200) fields per patient and staining were assessed and averaged.
The final staining score is the product of the average intensity
score and the average percentage of tumor cells showing positive
staining and ranged from 0 to 270 (30). Scoring of tumor tissue samples was
performed in blinded manner by JBF without knowledge of
pathological and clinical data. For statistical analysis, EGFR and
COX-2 scores were classified into two staining grades according to
the median staining score (the high grade represents ≥ median; the
low grade represents < median).
Statistical analyses
Data are presented as median and range (continuous
data), and as numbers and percentages (categorical data).
Mann-Whitney U and Pearson's Chi-square tests were used to
determine the association between EGFR and COX-2 protein expression
in tumor cells and clinicopathological and molecular parameters.
Overall survival (OS) was evaluated using Kaplan-Meier survival
plots, and differences in survival were tested using log-rank
(Mantel-Cox) tests. Cox proportional hazards regression analyses
were used to estimate hazard ratios (HR) and 95% confidence
intervals (95% CI). Multivariate Cox proportional hazards
regression analysis was performed to assess independent prognostic
factors using covariates found significant in univariate analysis
(regional lymph node metastasis and EGFR score). All P-values
corresponded to two-sided tests and P<0.05 was considered to
indicate a statistically significant difference. All statistical
analyses were conducted using either SPSS version 22 (IBM Corp.,
Armonk, NY, USA) or GraphPad Prism 7 (GraphPad Software, Inc., La
Jolla, CA, USA).
Results
Association between EGFR and COX-2
protein expression in tumor cells and clinicopathological
characteristics
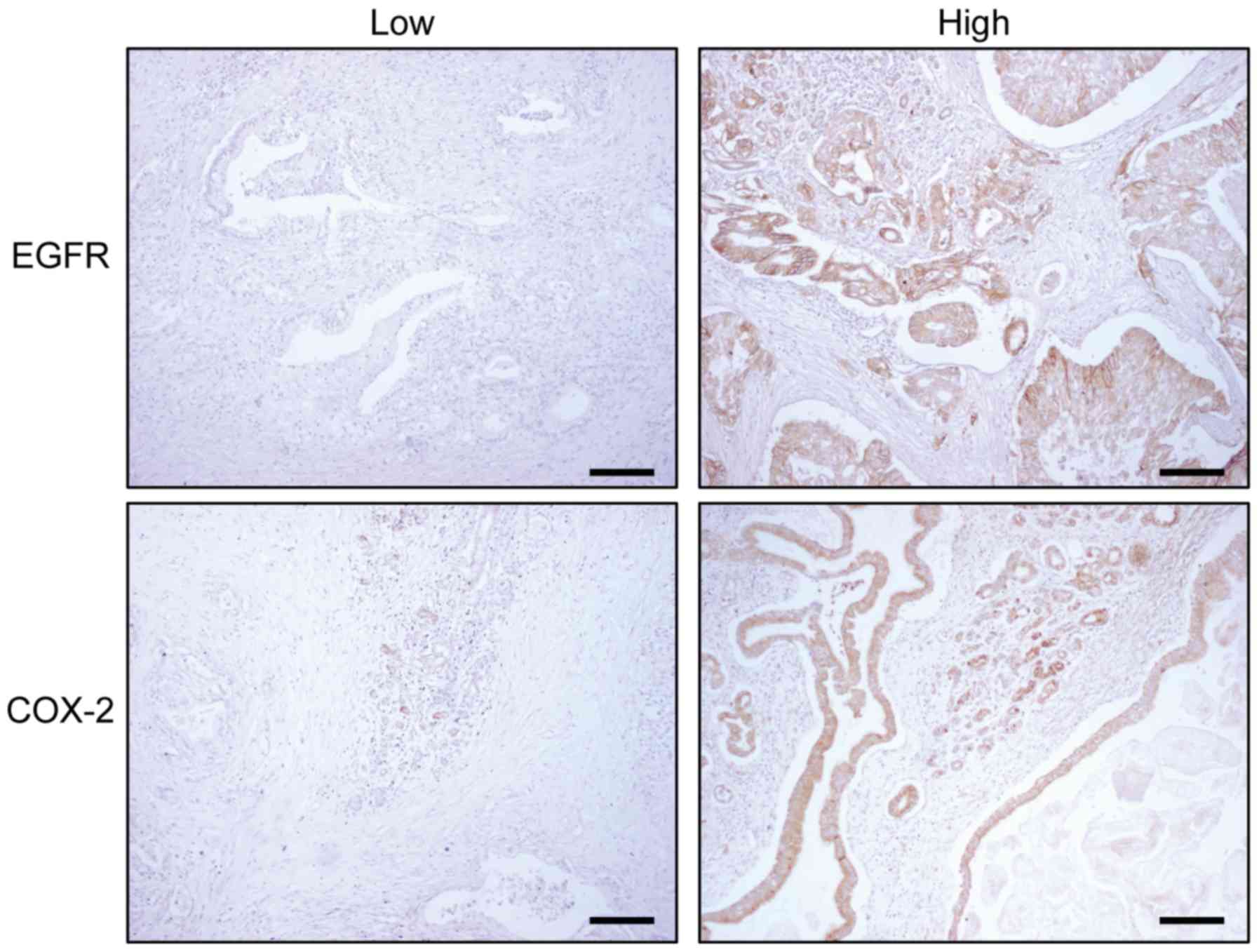
To assess EGFR and COX-2 protein expression in tumor
cells in surgically resected pancreatic ductal adenocarcinoma
(PDAC), protein expression level in PDAC samples was scored and
divided into two subgroups: Low and high grade (Fig. 1) and was then compared to
clinicopathological characteristics. In the study cohort, no
significant associations of either EGFR or COX-2 protein expression
in tumor cells were found with tumor location, tumor stage or
regional lymph node metastasis (Tables
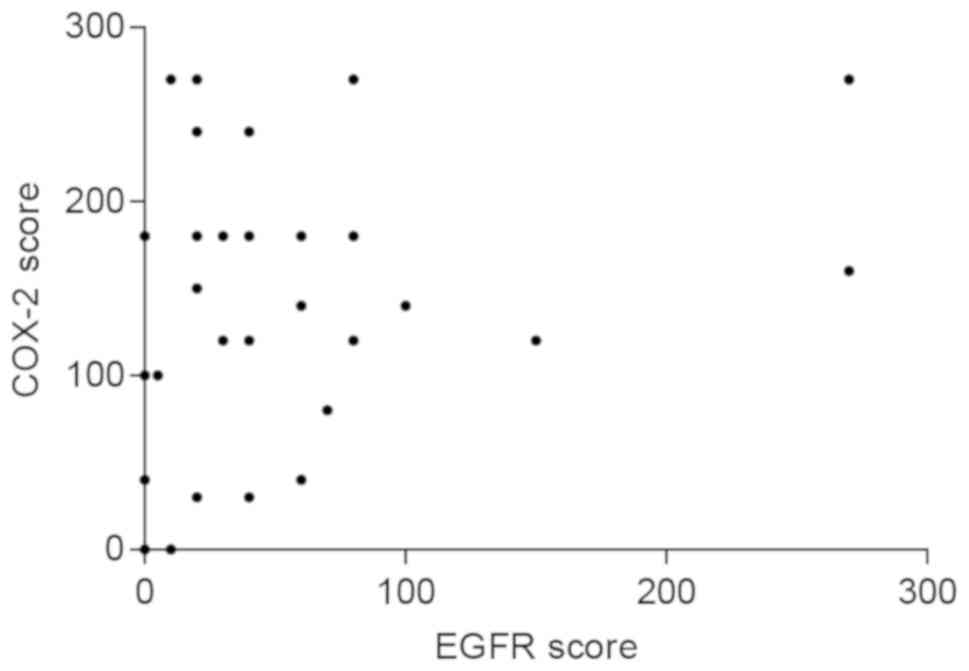
I and II). However, we detected
a weak positive correlation between EGFR and COX-2 protein
expression in tumor cells (Spearman's rank correlation coefficient
of 0.363, P=0.041, Fig. 2).
 | Table I.Clinicopathological characteristics
and EGFR status. |
Table I.
Clinicopathological characteristics
and EGFR status.
|
| EGFR High, | EGFR Low, |
|
|---|
| Characteristic | n (%) | n (%) |
P-valuea |
|---|
| All | 15 (47) | 17
(53) |
|
| Age, years |
|
|
|
|
<65 | 11 (73) | 8
(47) | 0.165b |
|
≥65 | 4
(27) | 9
(53) |
|
| Sex |
|
|
|
|
Female | 7
(47) | 8
(47) | 0.982 |
|
Male | 8
(53) | 9
(53) |
|
| Tumor location |
|
|
|
|
Head | 13 (88) | 16 (94) | 0.471 |
|
Others | 2
(12) | 1 (6) |
|
| Tumor stage |
|
|
|
|
T1 | 3
(20) | 0 (0) | 0.103 |
|
T2 | 6
(40) | 6
(35) |
|
|
T3 | 6
(40) | 8
(47) |
|
|
T4 | 0 (0) | 3
(18) |
|
| Regional lymph node
metastasis |
|
N0 | 10 (67) | 6
(35) | 0.077 |
|
N1 | 5
(33) | 11 (65) |
|
| COX-2 |
|
|
|
|
Low | 9
(60) | 7
(41) | 0.288 |
|
High | 6
(40) | 10 (59) |
|
| Table II.Clinicopathological characteristics
and COX-2 status. |
Table II.
Clinicopathological characteristics
and COX-2 status.
|
| COX-2 | COX-2 |
|
|
|---|
| Characteristic | Low, n (%) | High, n (%) |
P-valuea |
|---|
| All | 16 (50) | 16 (50) |
|
| Age, years |
|
|
|
|
<65 | 10 (63) | 9
(56) | 0.468b |
|
≥65 | 6
(37) | 7
(44) |
|
| Sex |
|
|
|
|
Female | 7
(44) | 8
(50) | 0.723 |
|
Male | 9
(56) | 8
(50) |
|
| Tumor location |
|
|
|
|
Head | 14 (88) | 15 (94) | 0.544 |
|
Others | 2
(12) | 1 (6) |
|
| Tumor stage |
|
|
|
| T1 | 1 (6) | 2
(13) | 0.813 |
| T2 | 6
(38) | 6
(38) |
|
| T3 | 8
(50) | 6
(38) |
|
| T4 | 1 (6) | 2
(13) |
|
| Regional lymph node
metastasis |
| N0 | 8
(50) | 8
(50) | 1.000 |
| N1 | 8
(50) | 8
(50) |
|
| EGFR |
|
|
|
|
Low | 9
(56) | 6
(37) | 0.288 |
|
High | 7 (44) | 10 (63) |
|
High EGFR protein expression in tumor
cells associates with shorter overall survival in PDAC
patients
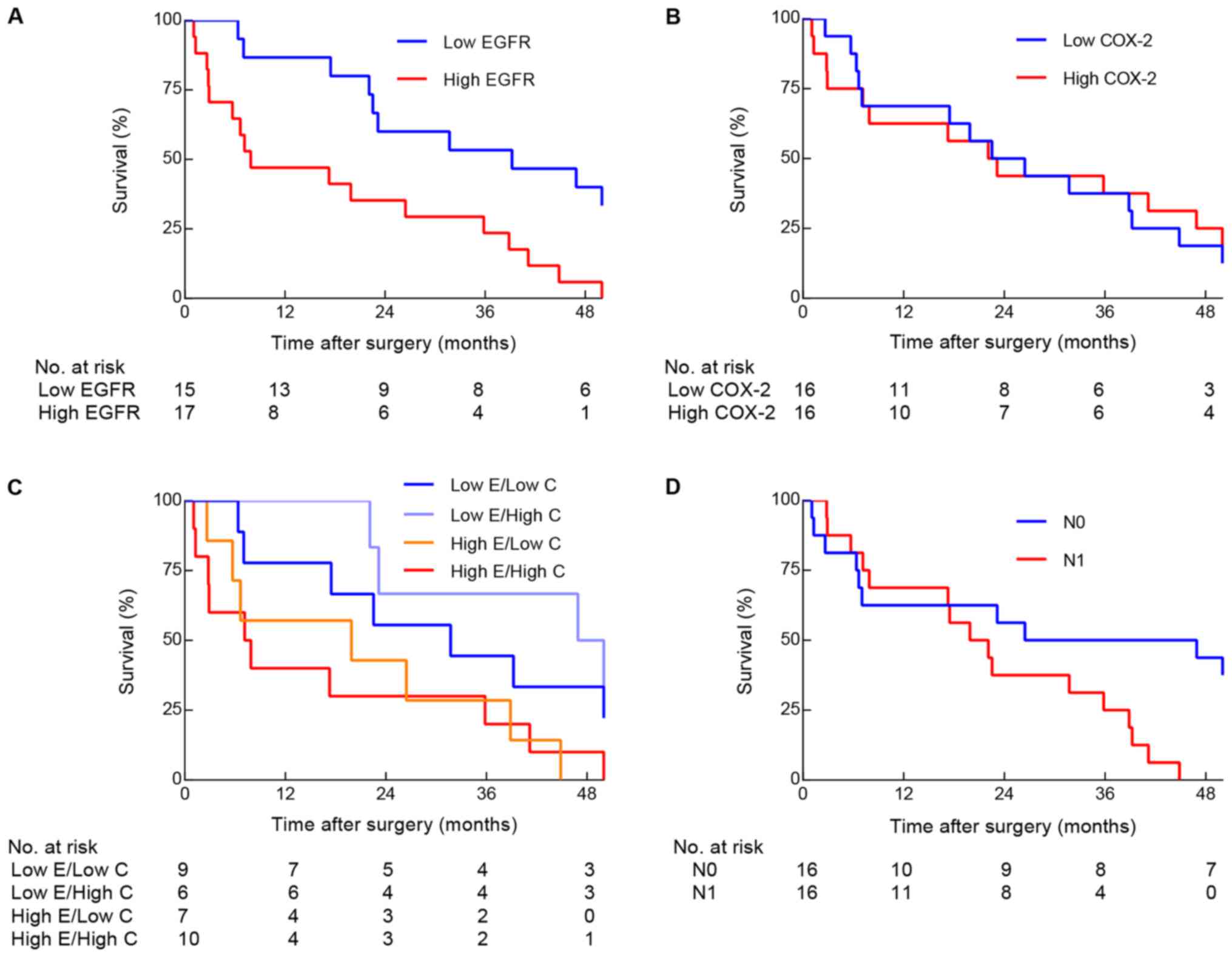
In order to examine the prognostic impact of EGFR
and COX-2 on survival outcome, we analyzed overall survival (OS)
time according to EGFR and COX-2 protein expression in tumor cells.
The median OS for the study cohort was 22.9 months. EGFR protein
expression and regional lymph node metastasis were significantly
associated with survival (Fig. 3).
High EGFR protein expression in tumor cells was significantly
associated with shorter OS (median OS: 7.9 months vs. 39.2 months
P=0.004, Fig. 3A). In contrast, we
did not detect any significant difference in median OS between
patients with high COX-2 and low COX-2 protein expression in tumor
cells (median OS: 22.6 months vs. 24.5 months P=0.596, Fig. 3B). To further evaluate the
association between EGFR and COX-2 protein expression, patients
were divided into four groups: Low EGFR/Low COX-2; Low EGFR/High
COX-2; High EGFR/Low COX-2; High EGFR/High COX-2. Analysis of OS in
these groups showed that patients with high EGFR score have shorter
median OS in both the Low COX-2 and High COX-2 subgroups (median
OS: Low EGFR/Low COX-2=31.7 months vs. High EGFR/Low COX-2=19.9
months and Low EGFR/High COX-2=53.4 months vs. High EGFR/High
COX-2=7.5 months, P=0.038, Fig. 3C).
Furthermore, median OS in patients with regional lymph node
metastasis was also significantly shorter than OS in patients
without regional lymph node metastasis (median OS: 21.0 months vs.
36.7 months, P=0.025, Fig. 3D).
However, the established prognostic factor tumor stage (31) was not significantly associated with
survival (data not shown).
The hazard ratio (HR) for death in patients with
high EGFR protein expression in tumor cells (when compared with low
EGFR protein expression in tumor cells) was 3.12 (95% CI:
1.39–7.00, P=0.006, Table III).
The corresponding HR for regional lymph node metastasis was 2.65
(95% CI: 1.10–6.39, P=0.030). In multivariate analysis, where
regional lymph node metastasis and EGFR score were included, only
high EGFR protein expression score remained as significant
independent prognostic factor for overall survival (P=0.043,
Table III).
| Table III.Prognostic factors of overall
survival in 32 patients with pancreatic ductal adenocarcinoma
following resection. |
Table III.
Prognostic factors of overall
survival in 32 patients with pancreatic ductal adenocarcinoma
following resection.
|
| Univariate
analysis | Multivariate
analysisa |
|---|
|
|
|
|
|---|
| Variable | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age, years |
|
|
|
|
|
|
|
<65 | 1 | 0.62–2.71 | 0.487 |
|
|
|
|
≥65 | 1.30 |
|
|
|
|
|
| Sex |
|
|
|
|
|
|
|
Female | 1 | 0.43–1.78 | 0.701 |
|
|
|
|
Male | 0.87 |
|
|
|
|
|
| Tumor location |
|
|
|
|
|
|
|
Head | 1 | 0.46–5.19 | 0.480 |
|
|
|
|
Others | 1.55 |
|
|
|
|
|
| Tumor stage |
|
|
|
|
|
|
|
T1-2 | 1 | 0.38–1.60 | 0.491 |
|
|
|
|
T3-4 | 0.78 |
|
|
|
|
|
| Regional lymph node
metastasis |
|
|
|
|
|
|
| N0 | 1 | 1.10–6.39 | 0.030 | 1 | 0.66–4.48 | 0.267 |
| N1 | 2.65 |
|
| 1.72 |
|
|
| EGFR |
|
|
|
|
|
|
|
Low | 1 | 1.39–7.00 | 0.006 | 1 | 1.03–6.15 | 0.043 |
|
High | 3.12 |
|
| 2.52 |
|
|
| COX-2 |
|
|
|
|
|
|
|
Low | 1 | 0.59–2.51 | 0.596 |
|
|
|
|
High | 1.22 |
|
|
|
|
|
To conclude, these results indicate that high EGFR,
but not COX-2, protein expression in tumor cells is an independent
prognostic factor for poor survival in resected PDAC patients.
Discussion
In this study, we demonstrated that EGFR protein
expression is a prognostic factor for survival in resected PDAC
patients. Patients with high EGFR protein expression in tumor cells
had significantly shorter overall survival. In contrast, COX-2
protein expression was not significantly associated with clinical
outcomes. Thus, EGFR seems to be a more significant predictor than
COX-2 for survival in resected PDAC patients.
In agreement with previous studies, we showed that
high EGFR protein expression is associated with poor survival in
PDAC patients (8,30,32,33). The
study with the largest sample size, by Valsecchi and colleagues
(30) demonstrated similarly to our
study that high membrane EGFR protein expression was significantly
associated with shorter overall survival. Yet, other studies have
not detected any significant association (7,34,35). A
reason for these differences may be the use of different
antibodies. We used an antibody that only detects wild-type EGFR,
whereas many of the studies reporting no association used
antibodies that detect both wild-type and a 2–7 truncated EGFR
variant (EGFR-vIII). This truncated EGFR variant is the most common
form of mutant EGFR and does not require ligand binding to activate
downstream signaling. However, the importance of EGFRvIII
expression in PDAC is unclear (36).
Therefore, conclusions about the prognostic value of EGFR should be
drawn with caution. However, recent studies have given a better
insight into the biology of EGFR-mediated signaling in PDAC and
suggest a critical role for EGFR in development of PDAC. Ardito
et al (13) and Navas et
al (14) knocked out Egfr
in KRAS-mutated mice and found that loss of EGFR completely blocked
pre-malignant lesion development. Together, these studies support
that EGFR is important for KRAS-driven pancreatic tumorigenesis.
Since most PDAC carry KRAS mutations (37), EGFR activation is likely to be
crucial also in the pathogenesis of human PDAC as it increases
aggressiveness of the tumors (32,38) and
causes shorter survival as shown in this and previous studies.
Our results on COX-2, showing no significant
association between high protein expression and overall survival,
confirmed those obtained by others (16,19–22).
However, two more recent studies by Juuti et al (17) and Matsubayashi et al (18) demonstrated significant effects of
COX-2 overexpression and clinical outcomes in PDAC patients. These
studies included more patients than our study (128 and 299
patients), which may be one reason explaining the differing
results. Another reason could be the use of different antibodies
(39). Yet another reason may be
differences in the evaluation of the IHC staining. We used a
histoscore system, where staining intensity and percentage of tumor
cells showing positive staining were assessed separately before
combined into a staining score, in which relatively more weight is
given to higher-intensity staining in a given tumor sample.
A link between EGFR and COX-2 signaling pathways has
been suggested in some cancers, mainly in experimental studies of
colorectal cancer and head and neck cancer, where EGFR upregulates
COX-2 or vice versa (26,27). For PDAC, a recent study by Hu et
al (40) using PDAC cell lines
reported that EGFR and COX-2 are linked and that overactive EGFR
signaling leads to overexpression of COX-2 and subsequent secretion
of VEGF, promoting angiogenesis which contribute to PDAC tumor cell
growth. However, there is no support in the literature for such an
association in human PDAC. Although we found a weak positive
correlation between EGFR and COX-2 score, this potential link
between the signaling pathways will require further mechanistic
studies in appropriate experimental models.
The results presented in this study, suggest that
EGFR is a superior predictor of survival than COX-2 since only EGFR
score in tumor cells was shown to be a prognostic factor. To our
knowledge, there is only one previous study that has examined the
relationship between both EGFR and COX-2 tumor expression and
survival among pancreatic cancer patients in the same study.
Lozano-Leon and colleagues (41)
reported no significant associations between EGFR or COX-2
expression and survival. In contrast to our study, where we used
whole tissue sections, they performed IHC on tissue microarrays,
which may have its limitations in survival analysis in small
patient materials and when the number of tumor cores is limited
(42).
A limitation of our study is the small number of
patients. This may explain why we did not find a significant
association between an established prognostic factor such as tumor
stage and survival (31). However,
we could still demonstrate an association between another
established prognostic factor, regional lymph node metastasis, and
overall survival.
As there are no effective treatments, to date, for
pancreatic cancer, it is important to develop molecular biomarkers
that predict clinical outcomes. This may help direct more effective
targeted therapy in high-risk patients such as patients with EGFR
protein overexpression in their tumors. Since the EGFR inhibitor,
erlotinib, is already in clinical use in combination with
gemcitabine for unresectable locally advanced or metastatic PDAC
(9,10), there should be no restrictions as to
consider evaluations of EGFR-targeted therapy for resected PDAC
patients. Our work underscores the importance of biomarkers, such
as wild-type EGFR, for identifying patients for inclusion in large
randomized studies.
In conclusion, our results show that high wild-type
EGFR protein expression, but not COX-2 protein expression, in tumor
cells is a prognostic factor for reduced survival following
pancreatic tumor resection. This supports a role for wild-type EGFR
as a biomarker in identifying resected PDAC patients that may
benefit the most from EGFR-targeted therapy.
Acknowledgements
Not applicable.
Funding
The present research was supported by grants from
the Swedish Cancer Society (grant nos. CAN 2015/400 and 2017/401),
Sahlgrenska Academy (grant no. V 2012/294), Assar Gabrielsson's and
Lundgren's Foundations (grant nos. 2017-1691 and 2018-2314).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
DL and PF performed the experiments. DL, CE and JBF
analyzed the data and performed the statistical analyses. DL, PF,
BMI, KL and JBF conceived the study and designed the experiments.
PN, KL and JBF interpreted data and revised the manuscript
critically for important intellectual content. All authors read,
reviewed and approved the final manuscript.
Ethics approval and consent to
participate
Human pancreatic tumor tissue sections were obtained
from the Pathology Department at Sahlgrenska University Hospital
(Gothenburg, Sweden). The present study was approved by the
Regional Ethical Review Board in Gothenburg, Sweden (reference no.
002-06) and all participants gave written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PDAC
|
pancreatic ductal adenocarcinoma
|
|
EGFR
|
epithelial growth factor receptor
|
|
COX-2
|
cyclooxygenase-2
|
|
HR
|
hazard ratio
|
|
immunohistochemistry
|
IHC
|
|
TBS
|
tris-buffered saline
|
|
DAB
|
3,3′-diaminobenzidine
|
|
H-score
|
histoscore
|
|
CI
|
confidence interval
|
|
OS
|
overall survival
|
References
|
1
|
Hezel AF, Kimmelman AC, Stanger BZ,
Bardeesy N and Depinho RA: Genetics and biology of pancreatic
ductal adenocarcinoma. Genes Dev. 20:1218–1249. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hishinuma S, Ogata Y, Tomikawa M, Ozawa I,
Hirabayashi K and Igarashi S: Patterns of recurrence after curative
resection of pancreatic cancer, based on autopsy findings. J
Gastrointest Surg. 10:511–518. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Iacobuzio-Donahue CA, Fu B, Yachida S, Luo
M, Abe H, Henderson CM, Vilardell F, Wang Z, Keller JW, Banerjee P,
et al: DPC4 gene status of the primary carcinoma correlates with
patterns of failure in patients with pancreatic cancer. J Clin
Oncol. 27:1806–1813. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Philip PA and Lutz MP: Targeting epidermal
growth factor receptor-related signaling pathways in pancreatic
cancer. Pancreas. 44:1046–1052. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tobita K, Kijima H, Dowaki S, Kashiwagi H,
Ohtani Y, Oida Y, Yamazaki H, Nakamura M, Ueyama Y, Tanaka M, et
al: Epidermal growth factor receptor expression in human pancreatic
cancer: Significance for liver metastasis. Int J Mol Med.
11:305–309. 2003.PubMed/NCBI
|
|
7
|
Bloomston M, Bhardwaj A, Ellison EC and
Frankel WL: Epidermal growth factor receptor expression in
pancreatic carcinoma using tissue microarray technique. Dig Surg.
23:74–79. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mahipal A, Mcdonald MJ, Witkiewicz A and
Carr BI: Cell membrane and cytoplasmic epidermal growth factor
receptor expression in pancreatic ductal adenocarcinoma. Med Oncol.
29:134–139. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Moore MJ, Goldstein D, Hamm J, Figer A,
Hecht JR, Gallinger S, Au HJ, Murawa P, Walde D, Wolff RA, et al:
Erlotinib plus gemcitabine compared with gemcitabine alone in
patients with advanced pancreatic cancer: A phase III trial of the
National Cancer Institute of Canada Clinical Trials Group. J Clin
Oncol. 25:1960–1966. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang JP, Wu CY, Yeh YC, Shyr YM, Wu YY,
Kuo CY, Hung YP, Chen MH, Lee WP, Luo JC, et al: Erlotinib is
effective in pancreatic cancer with epidermal growth factor
receptor mutations: A randomized, open-label, prospective trial.
Oncotarget. 6:18162–18173. 2015.PubMed/NCBI
|
|
11
|
Herman JM, Fan KY, Wild AT, Hacker-Prietz
A, Wood LD, Blackford AL, Ellsworth S, Zheng L, Le DT, De
Jesus-Acosta A, et al: Phase 2 study of erlotinib combined with
adjuvant chemoradiation and chemotherapy in patients with
resectable pancreatic cancer. Int J Radiat Oncol Biol Phys.
86:678–685. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sinn M, Bahra M, Liersch T, Gellert K,
Messmann H, Bechstein W, Waldschmidt D, Jacobasch L, Wilhelm M, Rau
BM, et al: CONKO-005: Adjuvant chemotherapy with gemcitabine plus
erlotinib versus gemcitabine alone in patients after R0 resection
of pancreatic cancer: A multicenter randomized phase III trial. J
Clin Oncol. 35:3330–3337. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ardito CM, Grüner BM, Takeuchi KK,
Lubeseder-Martellato C, Teichmann N, Mazur PK, Delgiorno KE,
Carpenter ES, Halbrook CJ, Hall JC, et al: EGF receptor is required
for KRAS-induced pancreatic tumorigenesis. Cancer Cell. 22:304–317.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Navas C, Hernández-Porras I, Schuhmacher
AJ, Sibilia M, Guerra C and Barbacid M: EGF receptor signaling is
essential for k-ras oncogene-driven pancreatic ductal
adenocarcinoma. Cancer Cell. 22:318–330. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Molina MA, Sitja-Arnau M, Lemoine MG,
Frazier ML and Sinicrope FA: Increased cyclooxygenase-2 expression
in human pancreatic carcinomas and cell lines: growth inhibition by
nonsteroidal anti-inflammatory drugs. Cancer Res. 59:4356–4362.
1999.PubMed/NCBI
|
|
16
|
Kokawa A, Kondo H, Gotoda T, Ono H, Saito
D, Nakadaira S, Kosuge T and Yoshida S: Increased expression of
cyclooxygenase-2 in human pancreatic neoplasms and potential for
chemoprevention by cyclooxygenase inhibitors. Cancer. 91:333–338.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Juuti A, Louhimo J, Nordling S, Ristimäki
A and Haglund C: Cyclooxygenase-2 expression correlates with poor
prognosis in pancreatic cancer. J Clin Pathol. 59:382–386. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matsubayashi H, Infante JR, Winter J,
Klein AP, Schulick R, Hruban R, Visvanathan K and Goggins M: Tumor
COX-2 expression and prognosis of patients with resectable
pancreatic cancer. Cancer Biol Ther. 6:1569–1575. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Richards NG, Rittenhouse DW, Freydin B,
Cozzitorto JA, Grenda D, Rui H, Gonye G, Kennedy EP, Yeo CJ, Brody
JR and Witkiewicz AK: HuR status is a powerful marker for prognosis
and response to gemcitabine-based chemotherapy for resected
pancreatic ductal adenocarcinoma patients. Ann Surg. 252:499–506.
2010.PubMed/NCBI
|
|
20
|
Koshiba T, Hosotani R, Miyamoto Y, Wada M,
Lee JU, Fujimoto K, Tsuji S, Nakajima S, Doi R and Imamura M:
Immunohistochemical analysis of cyclooxygenase-2 expression in
pancreatic tumors. Int J Pancreatol. 26:69–76. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Okami J, Yamamoto H, Fujiwara Y, Tsujie M,
Kondo M, Noura S, Oshima S, Nagano H, Dono K, Umeshita K, et al:
Overexpression of cyclooxygenase-2 in carcinoma of the pancreas.
Clin Cancer Res. 5:2018–2024. 1999.PubMed/NCBI
|
|
22
|
Merati K, said Siadaty M, Andea A, Sarkar
F, Ben-Josef E, Mohammad R, Philip P, Shields AF, Vaitkevicius V,
Grignon DJ and Adsay NV: Expression of inflammatory modulator COX-2
in pancreatic ductal adenocarcinoma and its relationship to
pathologic and clinical parameters. Am J Clin Oncol. 24:447–452.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lipton A, Campbell-Baird C, Witters L,
Harvey H and Ali S: Phase II trial of gemcitabine, irinotecan, and
celecoxib in patients with advanced pancreatic cancer. J Clin
Gastroenterol. 44:286–288. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kirane A, Toombs JE, Ostapoff K, Carbon
JG, Zaknoen S, Braunfeld J, Schwarz RE, Burrows FJ and Brekken RA:
Apricoxib, a novel inhibitor of COX-2, markedly improves standard
therapy response in molecularly defined models of pancreatic
cancer. Clin Cancer Res. 18:5031–5042. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hill R, Li Y, Tran LM, Dry S, Calvopina
JH, Garcia A, Kim C, Wang Y, Donahue TR, Herschman HR and Wu H:
Cell intrinsic role of COX-2 in pancreatic cancer development. Mol
Cancer Ther. 11:2127–2137. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yang CC and Chang KW: Eicosanoids and
HB-EGF/EGFR in cancer. Cancer Metastasis Rev. 23–Jun;2018.(Epub
ahead of print). View Article : Google Scholar
|
|
27
|
Wang D, Xia D and Dubois RN: The crosstalk
of PTGS2 and EGF signaling pathways in colorectal cancer. Cancers
(Basel). 3:3894–3908. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Axelsson H, Lönnroth C, Andersson M and
Lundholm K: Mechanisms behind COX-1 and COX-2 inhibition of tumor
growth in vivo. Int J Oncol. 37:1143–1152. 2010.PubMed/NCBI
|
|
29
|
Lönnroth C, Andersson M, Asting AG,
Nordgren S and Lundholm K: Preoperative low dose NSAID treatment
influences the genes for stemness, growth, invasion and metastasis
in colorectal cancer. Int J Oncol. 45:2208–2220. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Valsecchi ME, McDonald M, Brody JR, Hyslop
T, Freydin B, Yeo CJ, Solomides C, Peiper SC and Witkiewicz AK:
Epidermal growth factor receptor and insulinlike growth factor 1
receptor expression predict poor survival in pancreatic ductal
adenocarcinoma. Cancer. 118:3484–3493. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lim JE, Chien MW and Earle CC: Prognostic
factors following curative resection for pancreatic adenocarcinoma:
A population-based, linked database analysis of 396 patients. Ann
Surg. 237:74–85. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ueda S, Ogata S, Tsuda H, Kawarabayashi N,
Kimura M, Sugiura Y, Tamai S, Matsubara O, Hatsuse K and Mochizuki
H: The correlation between cytoplasmic overexpression of epidermal
growth factor receptor and tumor aggressiveness: Poor prognosis in
patients with pancreatic ductal adenocarcinoma. Pancreas. 29:e1–e8.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Perini MV, Montagnini AL, Coudry R,
Patzina R, Penteado S, Abdo EE, Diniz A, Jukemura J and da Cunha
JE: Prognostic significance of epidermal growth factor receptor
overexpression in pancreas cancer and nodal metastasis. ANZ J Surg.
85:174–178. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Smeenk HG, Erdmann J, van Dekken H, van
Marion R, Hop WC, Jeekel J and van Eijck CH: Long-term survival
after radical resection for pancreatic head and ampullary cancer: A
potential role for the EGF-R. Dig Surg. 24:38–45. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Park SJ, Gu MJ, Lee DS, Yun SS, Kim HJ and
Choi JH: EGFR expression in pancreatic intraepithelial neoplasia
and ductal adenocarcinoma. Int J Clin Exp Pathol. 8:8298–8304.
2015.PubMed/NCBI
|
|
36
|
Wang L, Wu H, Wang L, Lu J, Duan H, Liu X
and Liang Z: Expression of amphiregulin predicts poor outcome in
patients with pancreatic ductal adenocarcinoma. Diagn Pathol.
11:602016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Almoguera C, Shibata D, Forrester K,
Martin J, Arnheim N and Perucho M: Most human carcinomas of the
exocrine pancreas contain mutant c-K-ras genes. Cell. 53:549–554.
1988. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yamanaka Y, Friess H, Kobrin MS, Buchler
M, Beger HG and Korc M: Coexpression of epidermal growth factor
receptor and ligands in human pancreatic cancer is associated with
enhanced tumor aggressiveness. Anticancer Res. 13:565–569.
1993.PubMed/NCBI
|
|
39
|
Asting AG, Farivar A, Iresjö BM, Svensson
H, Gustavsson B and Lundholm K: EGF receptor and COX-1/COX-2 enzyme
proteins as related to corresponding mRNAs in human per-operative
biopsies of colorectal cancer. BMC Cancer. 13:5112013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hu H, Han T, Zhuo M, Wu LL, Yuan C, Wu L,
Lei W, Jiao F and Wang LW: Elevated COX-2 expression promotes
angiogenesis through EGFR/p38-MAPK/Sp1-dependent signalling in
pancreatic cancer. Sci Rep. 7:4702017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lozano-Leon A, Perez-Quintela BV,
Iglesias-García J, Lariño-Noia J, Varo E, Forteza J and
Domínguez-Muñoz JE: Ductal adenocarcinoma of the pancreas:
Expression of growth factor receptors, oncogenes and suppressor
genes, and their relationship to pathological features, staging and
survival. Oncol Lett. 2:161–166. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Khouja MH, Baekelandt M, Sarab A, Nesland
JM and Holm R: Limitations of tissue microarrays compared with
whole tissue sections in survival analysis. Oncol Lett. 1:827–831.
2010. View Article : Google Scholar : PubMed/NCBI
|