Introduction
The surgical procedure is the mainstay of treatment
for colorectal and other solid cancers. However, it may itself
promote cancer growth and metastasis (1) since tumor cells can disseminate during
surgery. Perioperative immunosuppression may facilitate the spread
and survival of malignant cells in the body (2). Several retrospective studies have
suggested that the use of regional anesthesia in cancer surgery
might improve survival (3–5). The precise mechanisms underlying the
possible effects of regional anesthesia have not been fully
elucidated but an impact on reduction in stress response,
postoperative inflammation and prevention of immunosuppression has
been proposed (6,7). Local anesthetics (LA) act by blocking
voltage-gated sodium channels (VGSC) in all cells and may also have
direct inhibitory effects on cancer cells by inducing apoptosis
(8), demethylating DNA (9), blocking metastatic cancer cell invasion
in vitro (10) and may have
direct cytotoxic (11) and
anti-proliferative effects (12).
While evolving from primary tumor cells to metastatic cells, cancer
cells have to change phenotypes and properties (13). This transformation might also affect
the response of cancer cells to LA.
LA administered by the epidural route are absorbed
into the systemic circulation. Peak plasma concentrations of
ropivacaine during an epidural infusion for 120 h ranged between
2.4 and 6.1 µg/ml, equivalent to approximately 10–22 µM (14). Systemic plasma levels for lidocaine
have been found to lie in the same range (15). After local application of LA by
intraperitoneal injection or tissue infiltration, the LA
concentrations at the injection site are in the millimolar range,
which is 1,000 times greater than that achieved following
intravenous administration (16).
Therefore, it is possible that LA may prevent cancer cell
proliferation and micro-infiltration of cancer cells when injected
locally into tissues as well as potentially inhibit imminent
metastases during the perioperative period when immune modulation
is sub-optimal.
In this study, we hypothesized that commonly used
local anesthetic agents, lidocaine and ropivacaine, decrease cell
viability and inhibit proliferation of colon cancer cells in
vitro in a dose-dependent manner when used in clinically
relevant concentrations. Furthermore, we investigated if there is a
different effect of LA on primary colon cancer cells and cells
derived from metastatic colon cancer.
Materials and methods
Cell culture and LA
Immortalized human colon cancer cells SW480 and
SW620 were purchased from American Type Culture Collection
(ATCC® CCL-228 and CCL-227). SW480 originates from an
adenocarcinoma of the colon in a 50-year-old male and SW620 was
derived from a lymph node metastasis in the same patient one year
later (17). Cells were cultured in
Dulbecco's modified Eagle medium (DMEM) with GlutaMAX, supplemented
with 10% fetal bovine serum (FBS) and 1 µg/ml
penicillin/streptomycin (all from Life technologies, Stockholm,
Sweden) in a humidified incubator at 37°C and 5% CO2.
Cells were cultured following standard microbiological practices
and handled according to recommended seeding procedures. Lidocaine
10 mg/ml (Xylocaine hydrochloride; AstraZeneca, Södertälje, Sweden)
and ropivacaine 2 mg/ml (Fresenius Kabi, Uppsala, Sweden) were
diluted with Dulbecco's PBS (DPBS) to the desired concentrations
used in the experiments (low concentrations = equivalent to
systemic plasma concentration after intravenous or epidural
application, high concentrations = equivalent to local
concentration after tissue infiltration).
Cell viability assay
In 96-well plates, 4,000 cells per well were seeded
in 100 µl supplemented medium and cultured for 24 h. The next day,
10 µl lidocaine or ropivacaine diluted in DPBS were added to the
wells to reach the final concentrations 5, 10, 15, 20, 25, 50, 100
and 500 µM. In addition, a 20 µl solution was added to reach a
final concentration of 1,000 µM of lidocaine and ropivacaine,
respectively. As drug-free control, cells were cultured in
supplemented medium and 10 µl DPBS for 5–500 µM (control 1) and 20
µl DPBS for 1,000 µM (control 2). Each concentration of anesthetics
was run in quadruplicate wells and three independent experiments
were performed. Cell viability was tested after 24, 48 and 72 h
exposure using CellTiter-Blue® Cell Viability Assay
(Promega Biotech AB, Stockholm, Sweden) according to manufacturer's
protocol. Briefly, to estimate cell viability, 20 µl CellTiter-Blue
was added to the 96-well cell culture plate and shaken for 10 sec.
The plates were incubated for 2.5 h before fluorescence was
measured with FLUOstar optima (BMG Labtech GmbH, Ortenberg,
Germany) with a 544Ex/590Em filter set.
Cell proliferation assay
Cell Linker kit PKH67, MINI67 (Sigma-Aldrich,
Stockholm, Sweden) was used to analyze cell proliferation with flow
cytometry. The cells were dyed at time of seeding according to
manufacturer's protocol. The cell linker kit stains lipid regions
of the cell membrane with a green fluorochrome without impairing
cellular functions. The amount of incorporated fluorochrome
decreases as the cells divide during mitosis.
In 6-well plates, 120,000 PKH67 stained cells per
well were seeded in 3 ml supplemented medium 24 h before drug
exposure. Then, 330 µl lidocaine or ropivacaine diluted in DPBS
were added to the cells to achieve the final concentrations: 10,
500 and 1,000 µM. The same volume DPBS was used as drug-free
control. Each concentration of anesthetics was run in duplicate
wells and three independent experiments were performed. After 72 h,
cells were trypsinated and then analysed using a Gallios Flow
Cytometer (Beckman Coulter, Indianapolis, IN, USA) equipped with
blue laser (488 nm), yellow laser (561 nm) red laser (638 nm) and
violet laser (405 nm). Data was collected with Kaluza for Gallios
1.0 and analyzed with Kaluza analysis 1.3 (Beckman Coulter). The
amount of incorporated PKH67 was measured by median fluorescence
intensity (MFI). A MFI ratio between drug-free control and each
concentration was then calculated.
Statistical analysis
Results are presented as median (range) ratio
between respective drug concentration and drug-free control. A
ratio >1 indicates an increased cell viability or cell
proliferation while a ratio <1 indicates decreased cell
viability or inhibition of cell proliferation.
We used Shapiro-Wilks test for normal distribution.
The results showed that the data for some of the experiments were
not normally distributed. Therefore, non-parametric methods were
used for statistical analysis. Cell viability data from three
independent experiments in quadruplicate (n=12) were analyzed using
Kruskal-Wallis test (5–500 µM) with Dunn's correction for multiple
comparisons. Mann-Whitney-U test was used for the highest
concentration (1,000 µM) in comparison with its drug-free control
(control 2). Cell proliferation data from three independent
experiments set in duplicate (n=6) were analyzed using
Kruskal-Wallis test with Dunn's post hoc test. P<0.05 was
considered to indicate a statistically significant difference. The
statistical analysis was performed using GraphPad Prism version
7.03 (GraphPad Software, Inc., La Jolla, CA, USA).
Results
Cell viability
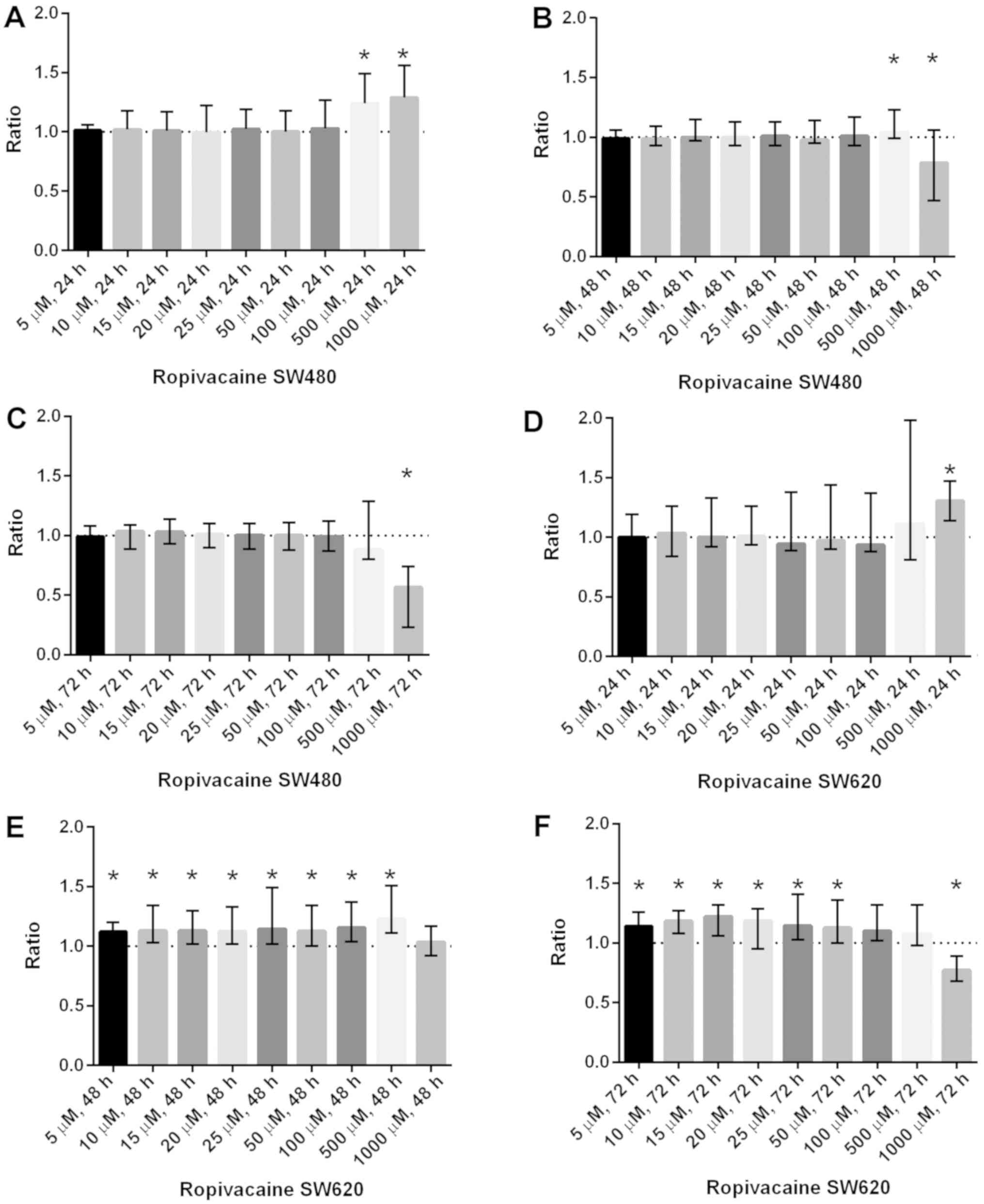
Ropivacaine: Increased cell viability was found at
500 µM [1.24 (1.06–1.49), P<0.0001] and 1,000 µM [1.29
(1.01–1.56), P<0.001] after 24 h in SW480. A significant
increase in cell viability was also shown in SW620 at
concentrations between 5–500 µM after 48 h exposure and at 5–50 µM
after 72 h exposure. Ropivacaine 1,000 µM resulted in significantly
reduced cell viability in SW480 after exposure for 48 h [0.78
(0.44–1.06), P=0.001] and 72 h [0.57 (0.23–0.74), P<0.0001]. In
SW620, cell viability was only reduced by 1,000 µM [0.77
(0.68–0.89), P<0.0001] after 72 h exposure (Fig. 1).
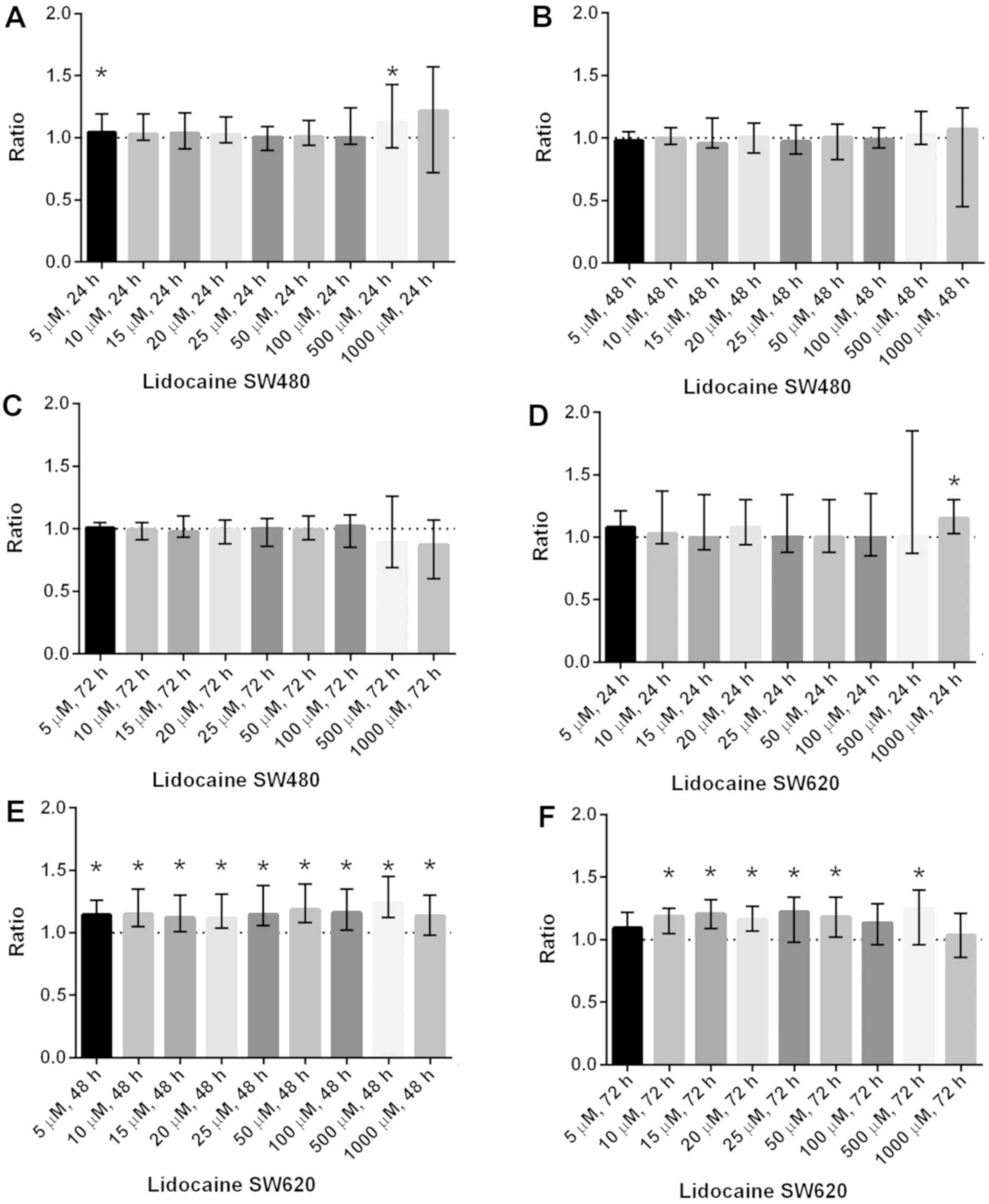
Lidocaine: there was a significant increase in cell
viability after 24 h in SW480 at 500 µM [1.13 (0.92–1.43),
P<0.05] and in SW620 at 1,000 µM [1.15 (1.03–1.30), P<0.001].
In the metastatic cell line SW620 (but not in SW480) cell viability
was significantly increased even at lower concentrations after
exposure for 48 and 72 h (Fig. 2).
No significant reduction in cell viability was found after exposure
to lidocaine at any concentration and at any time point for both
cell lines SW480 and SW620.
Cell proliferation
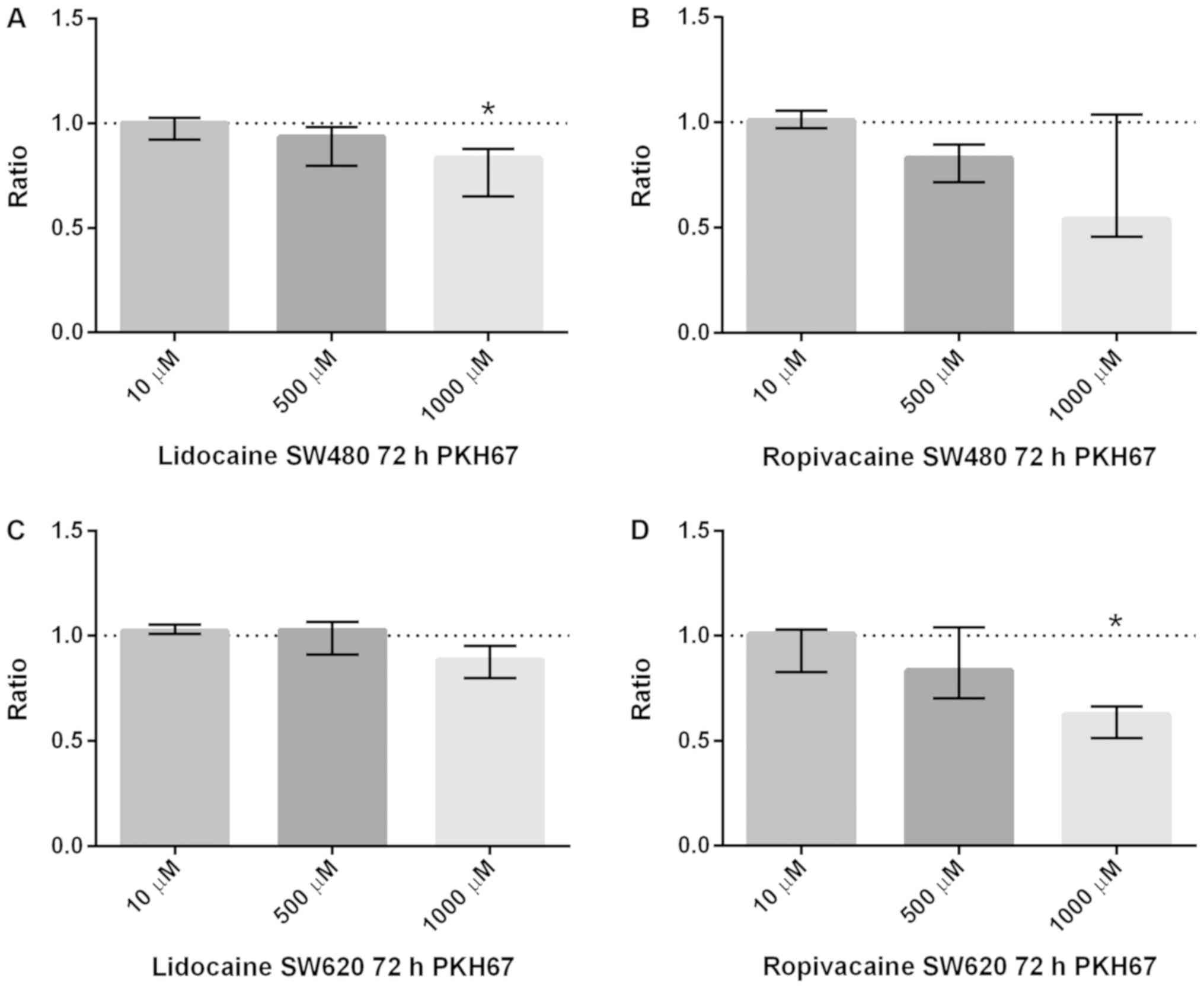
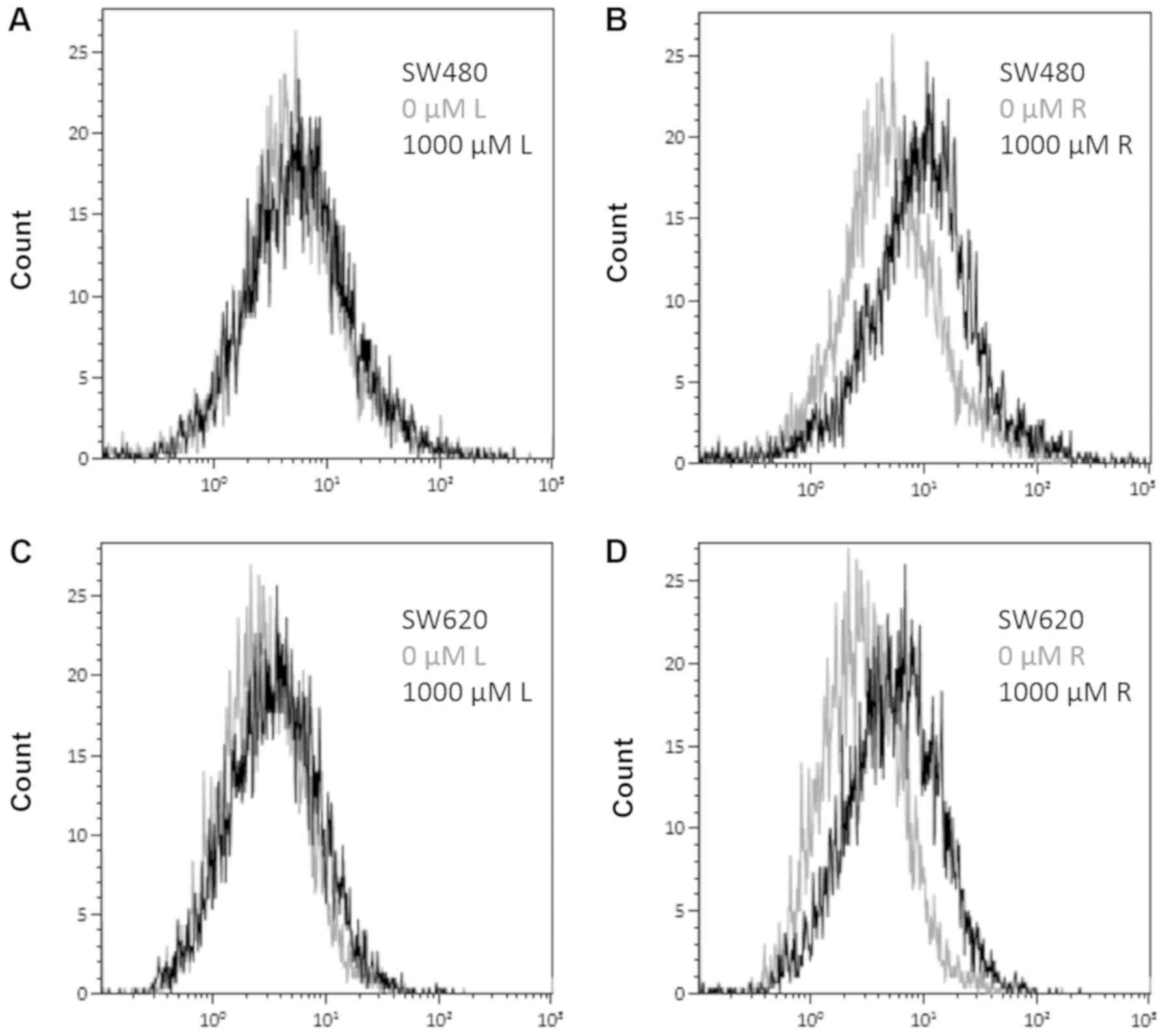
No significant effect on cell proliferation was
found at lower concentrations (10 and 500 µM) of lidocaine or
ropivacaine (Fig. 3). However,
reduction in cell proliferation was found in both cell lines after
exposure to the highest concentration (1,000 µM) of lidocaine and
ropivacaine (Fig. 3). However, after
correction for multiple comparisons, it was only statistically
significant for lidocaine in SW480 and for ropivacaine in SW620.
The anti-proliferative effect seems to be more pronounced for
ropivacaine than for lidocaine (Fig.
4).
Discussion
Our hypothesis of reduced cell viability following
LA exposure was only partially supported by our findings. Cell
viability was not significantly reduced by lidocaine in any
concentration tested or at any time point. However, a significant
decrease in cell viability was observed for ropivacaine at 1,000
µM, when the exposure time was at least 48 h. Our results are based
on estimating cell viability using an assay where a redox dye is
converted into a fluorescent product by metabolically active,
living cells. An increase in fluorescence is regarded to be
proportional to increased cell count, while a reduction in
fluorescence may accordingly be proportional to reduced cell count.
The method has limitations and we cannot be sure that changes in
fluorescence depend on changes in cell metabolism rather than cell
count (18). However, the reduction
in cell viability measured by CellTiter-Blue® for
ropivacaine at 1,000 µM corresponds to a reduction in cell
proliferation measured by PKH67 at the same concentration. Xuan
et al reported similar findings in ovarian and prostate
cancer cell lines (19). In their
study, only bupivacaine at 1 mM decreased cell viability
significantly, but not at lower concentrations. The effect was more
pronounced when these cancer cells were exposed to bupivacaine for
72 h. Similarly, in a study by Le Gac et al, lidocaine and
ropivacaine did not reduce cell viability in human hepatocellular
carcinoma cell lines at low concentrations (1–10 µM). At higher
concentrations (100 µM, 1 and 5 mM), a dose-dependent decrease in
cell viability could be detected, which was more pronounced after
72 h compared to 24 h (20).
Retrospective studies in humans have demonstrated
increased survival in patients having epidural analgesia with LA
compared to intravenous analgesia with morphine in colon and rectal
cancer (3,21). The precise mechanisms for this
protective effect of epidural analgesia remain unclear but one
hypothesis has been that absorption of LA from the epidural space
may inhibit cell proliferation of circulating tumor cells released
during surgery, thereby impeding perioperative cancer metastases
(22). Cell proliferation is an
essential process in the development of malignant tumors and
metastasis (23). Based on our
results and previous studies, we believe that LA do not exert an
anti-proliferative effect on cancer cell lines in the range of
systemic plasma concentrations achieved during epidural
administration of LA. Other anti-metastatic mechanisms of LA in
this low range of concentrations have been proposed. Piegeler et
al have shown that lidocaine and ropivacaine inhibit Src
tyrosine kinase when used in clinically relevant concentrations
(24). Src tyrosine kinase is an
important enzyme in tumor growth and metastasis and controls the
activation of matrix-metalloproteinases (MMP), another important
factor in the pathogenesis of metastasis. Lidocaine and ropivacaine
inhibited MMP9-secretion by NCl-H838 lung adenocarcinoma cells with
an IC50 of 3.3 and 1.5 µM, respectively (25). This effect of LA was independent of
their primary mechanism of action, the blockade of VGSC. VGSC have
been detected on a variety of different cancer cells and are
presumed to play an important role in the process of metastasis
(26). Cancer cell lines SW480 and
SW620 used in our study express mainly the VGSC-isoform
Nav1.5 (27).
Baptista-Hon et al were able to show that metastatic cell
invasion of SW620 is potently inhibited by ropivacaine in
vitro with an IC50 value below 5 µM (10).
The effect of LA varies with different types of
cancer cell lines and their properties. Our findings on inhibition
of cell viability and proliferation are in line with Martinsson
(28). They showed that ropivacaine
reduced cell proliferation in colon cancer cell lines, HT-29 and
Caco-2, in a dose-dependent manner with an IC50>250
and 430 µM, respectively. They also found that lidocaine had a less
potent anti-proliferative effect than ropivacaine. HT-29, Caco-2
and SW480 all originate from human colon adenocarcinoma. There are
many similarities but even distinct differences between these cell
lines (29) justifying further
research.
In contrast to our primary hypothesis, we noted a
significant increase in cell viability especially in the metastatic
cell line SW620 when exposed for at least 48 h to concentrations of
lidocaine or ropivacaine equivalent to those systemically
achievable in vivo. A comparable increase in cell viability
could not be seen in the primary tumor cell line SW480. The cell
lines SW480 and SW620 are unique as they originate from the same
patient reflecting progression from primary to metastatic tumor
cells. It is believed that tumor cells undergo distinctive changes
in both morphologic and functional properties to metastasize to
distant tissues (30). The process
of metastasis is generally inefficient and not all cancer cells
released into the circulation during a surgical procedure are able
to develop into distant metastases (31). Cells that already have passed through
the ‘epithelial-mesenchymal transition’ (EMT) and have acquired the
ability for invasion and dissemination are likely to be able to
form metastases (32). Hewitt et
al showed that SW480 and SW620 have retained significant
histological differences (33).
SW620 cells have a more fibroblast-like appearance, a higher growth
rate and are more invasive than SW480. The fact that SW620 respond
with increased cell viability to LA is thus especially interesting,
as it must be suspected that mainly cells that have undergone
metastatic transformation are able to form distant metastases if
released during the perioperative period. To the best of our
knowledge there is no study published with focus on the effect of
LA on primary and metastatic colon cancer cell lines. The
observation that there is increased cell viability in the
metastatic cell line is remarkable and Bundscherer et al
found similar results in a previous study (34). Bupivacaine also significantly
increased cell growth in PaTu8988t, a cell line originated from a
liver metastasis of a pancreatic adenocarcinoma, in similar
concentrations (0.1–100 µM). However, the increase in cell
viability as measured by CellTiter-Blue® for both
ropivacaine and lidocaine is not accompanied by an increase in cell
proliferation as analyzed by PKH67. The cell viability assay used
in this study cannot exclude that the increase of viability shown
is a result of increased metabolism and not increased cell count.
Ropivacaine has been shown to affect energy metabolism in cells by
uncoupling of oxidative phosphorylation and a direct inhibitory
effect on mitochondrial enzyme complexes (35,36).
However, this should cause a reduction in cell viability not an
increase. Thus, the mechanisms behind the increase in cell
viability of the metastatic cell line SW620 when exposed to LA are
still unclear, as is its clinical significance. This needs to be
further investigated in future studies.
In conclusion, our findings show that exposure of
colon cancer cell lines to lidocaine and ropivacaine results in
increased cell viability at clinically relevant concentrations,
specifically in the metastatic cancer cell line. Future studies
should explore possible mechanisms for this observation. Reduced
cell viability and proliferation were only seen at the highest
concentration. These high concentrations can be achieved locally by
intraperitoneal administration of LA for several days via a
catheter following intra-abdominal surgery. This opens the window
for in vivo studies investigating the clinical effectiveness
of intraperitoneally administered LA in patients undergoing surgery
for colorectal cancer.
Acknowledgements
An abstract of this study was presented previously
at the 34th SSAI Congress 3017 in Malmö, Sweden. The
authors would like to thank Dr Anna Göthlin Eremo (Örebro
University, Örebro, Sweden) for statistical guidance.
Funding
Financial support was obtained from the Research
Committee of the Örebro County Council.
Availability of data and materials
The datasets analyzed during the study are available
from the corresponding author on reasonable request.
Authors' contributions
AG and ET designed the study. ET and AKVS conducted
the laboratory research with assistance from WS. WS performed the
statistical analysis and wrote the manuscript in close cooperation
with all authors. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ceelen W, Pattyn P and Mareel M: Surgery,
wound healing, and metastasis: Recent insights and clinical
implications. Crit Rev Oncol Hematol. 89:16–26. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Coffey JC, Wang JH, Smith MJ,
Bouchier-Hayes D, Cotter TG and Redmond HP: Excisional surgery for
cancer cure: therapy at a cost. Lancet Oncol. 4:760–768. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gupta A, Björnsson A, Fredriksson M,
Hallböök O and Eintrei C: Reduction in mortality after epidural
anaesthesia and analgesia in patients undergoing rectal but not
colonic cancer surgery: a retrospective analysis of data from 655
patients in central Sweden. Br J Anaesth. 107:164–170. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Christopherson R, James KE, Tableman M,
Marshall P and Johnson FE: Long-term survival after colon cancer
surgery: a variation associated with choice of anesthesia. Anesth
Analg. 107:325–332. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Biki B, Mascha E, Moriarty DC, Fitzpatrick
JM, Sessler DI and Buggy DJ: Anesthetic technique for radical
prostatectomy surgery affects cancer recurrence: a retrospective
analysis. Anesthesiology. 109:180–187. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Beilin B, Shavit Y, Trabekin E, Mordashev
B, Mayburd E, Zeidel A and Bessler H: The effects of postoperative
pain management on immune response to surgery. Anesth Analg.
97:822–827. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kurosawa S: Anesthesia in patients with
cancer disorders. Curr Opin Anaesthesiol. 25:376–384. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chang YC, Liu CL, Chen MJ, Hsu YW, Chen
SN, Lin CH, Chen CM, Yang FM and Hu MC: Local anesthetics induce
apoptosis in human breast tumor cells. Anesth Analg. 118:116–124.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lirk P, Berger R, Hollmann MW and Fiegl H:
Lidocaine time- and dose-dependently demethylates deoxyribonucleic
acid in breast cancer cell lines in vitro. Br J Anaesth.
109:200–207. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Baptista-Hon DT, Robertson FM, Robertson
GB, Owen SJ, Rogers GW, Lydon EL, Lee NH and Hales TG: Potent
inhibition by ropivacaine of metastatic colon cancer SW620 cell
invasion and NaV1.5 channel function. Br J Anaesth. 113 (Suppl
1):i39–i48. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Perez-Castro R, Patel S, Garavito-Aguilar
ZV, Rosenberg A, Recio-Pinto E, Zhang J, Blanck TJ and Xu F:
Cytotoxicity of local anesthetics in human neuronal cells. Anesth
Analg. 108:997–1007. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lucchinetti E, Awad AE, Rahman M, Feng J,
Lou PH, Zhang L, Ionescu L, Lemieux H, Thébaud B and Zaugg M:
Antiproliferative effects of local anesthetics on mesenchymal stem
cells: potential implications for tumor spreading and wound
healing. Anesthesiology. 116:841–856. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Alizadeh AM, Shiri S and Farsinejad S:
Metastasis review: from bench to bedside. Tumour Biol.
35:8483–8523. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wiedemann D, Mühlnickel B, Staroske E,
Neumann W and Röse W: Ropivacaine plasma concentrations during
120-hour epidural infusion. Br J Anaesth. 85:830–835. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mayumi T, Dohi S and Takahashi T: Plasma
concentrations of lidocaine associated with cervical, thoracic, and
lumbar epidural anesthesia. Anesth Analg. 62:578–580. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hollmann MW and Durieux ME: Local
anesthetics and the inflammatory response: a new therapeutic
indication? Anesthesiology. 93:858–875. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Leibovitz A, Stinson JC, McCombs WB III,
McCoy CE, Mazur KC and Mabry ND: Classification of human colorectal
adenocarcinoma cell lines. Cancer Res. 36:4562–4569.
1976.PubMed/NCBI
|
|
18
|
Rampersad SN: Multiple applications of
Alamar Blue as an indicator of metabolic function and cellular
health in cell viability bioassays. Sensors (Basel).
12:12347–12360. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xuan W, Zhao H, Hankin J, Chen L, Yao S
and Ma D: Local anesthetic bupivacaine induced ovarian and prostate
cancer apoptotic cell death and underlying mechanisms in vitro. Sci
Rep. 6:262772016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Le Gac G, Angenard G, Clément B, Laviolle
B, Coulouarn C and Beloeil H: Local anesthetics inhibit the growth
of human hepatocellular carcinoma cells. Anesth Analg.
125:1600–1609. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vogelaar FJ, Abegg R, van der Linden JC,
Cornelisse HG, van Dorsten FR, Lemmens VE and Bosscha K: Epidural
analgesia associated with better survival in colon cancer. Int J
Colorectal Dis. 30:1103–1107. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Votta-Velis EG, Piegeler T, Minshall RD,
Aguirre J, Beck-Schimmer B, Schwartz DE and Borgeat A: Regional
anaesthesia and cancer metastases: the implication of local
anaesthetics. Acta Anaesthesiol Scand. 57:1211–1229. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: the next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Piegeler T, Votta-Velis EG, Liu G, Place
AT, Schwartz DE, Beck-Schimmer B, Minshall RD and Borgeat A:
Antimetastatic potential of amide-linked local anesthetics:
inhibition of lung adenocarcinoma cell migration and inflammatory
Src signaling independent of sodium channel blockade.
Anesthesiology. 117:548–559. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Piegeler T, Schläpfer M, Dull RO, Schwartz
DE, Borgeat A, Minshall RD and Beck-Schimmer B: Clinically relevant
concentrations of lidocaine and ropivacaine inhibit TNFα-induced
invasion of lung adenocarcinoma cells in vitro by blocking the
activation of Akt and focal adhesion kinase. Br J Anaesth.
115:784–791. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Brackenbury WJ: Voltage-gated sodium
channels and metastatic disease. Channels (Austin). 6:352–361.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
House CD, Vaske CJ, Schwartz AM, Obias V,
Frank B, Luu T, Sarvazyan N, Irby R, Strausberg RL, Hales TG, et
al: Voltage-gated Na+ channel SCN5A is a key regulator of a gene
transcriptional network that controls colon cancer invasion. Cancer
Res. 70:6957–6967. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Martinsson T: Ropivacaine inhibits
serum-induced proliferation of colon adenocarcinoma cells in vitro.
J Pharmacol Exp Ther. 288:660–664. 1999.PubMed/NCBI
|
|
29
|
Biazik JM, Jahn KA, Su Y, Wu YN and Braet
F: Unlocking the ultrastructure of colorectal cancer cells in vitro
using selective staining. World J Gastroenterol. 16:2743–2753.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Lambert AW, Pattabiraman DR and Weinberg
RA: Emerging biological principles of metastasis. Cell.
168:670–691. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tohme S, Simmons RL and Tsung A: Surgery
for Cancer: a trigger for metastases. Cancer Res. 77:1548–1552.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Talmadge JE and Fidler IJ: AACR centennial
series: the biology of cancer metastasis: historical perspective.
Cancer Res. 70:5649–5669. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hewitt RE, McMarlin A, Kleiner D, Wersto
R, Martin P, Tsokos M, Stamp GW and Stetler-Stevenson WG:
Validation of a model of colon cancer progression. J Pathol.
192:446–454. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bundscherer A, Malsy M, Gebhardt K,
Metterlein T, Plank C, Wiese CH, Gruber M and Graf BM: Effects of
ropivacaine, bupivacaine and sufentanil in colon and pancreatic
cancer cells in vitro. Pharmacol Res 95–96. 126–131. 2015.
View Article : Google Scholar
|
|
35
|
Sztark F, Malgat M, Dabadie P and Mazat
JP: Comparison of the effects of bupivacaine and ropivacaine on
heart cell mitochondrial bioenergetics. Anesthesiology.
88:1340–1349. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Nouette-Gaulain K, Sirvent P, Canal-Raffin
M, Morau D, Malgat M, Molimard M, Mercier J, Lacampagne A, Sztark F
and Capdevila X: Effects of intermittent femoral nerve injections
of bupivacaine, levobupivacaine, and ropivacaine on mitochondrial
energy metabolism and intracellular calcium homeostasis in rat
psoas muscle. Anesthesiology. 106:1026–1034. 2007. View Article : Google Scholar : PubMed/NCBI
|