Introduction
Breast cancer (BC) is the most common malignancy in
women worldwide, and the majority of BC subtypes are
hormone-associated (1). Estrogen
receptor (ER), progesterone receptor (PR), and human epidermal
growth factor receptor 2 (HER2) status, routinely available in BC
specimens, are reliable and useful tools for therapeutic
decision-making (2). Hormone
receptor (HR)-positive tumors comprise the majority of the cases
and have a relatively better outcome (3). By contrast, triple-negative BC (TNBC)
is a clinically heterogeneous disease with an aggressive clinical
course (4). The lack of targeted
therapies and the relatively poor prognosis of patients with TNBC
have created the need to evaluate novel treatment approaches,
including immunotherapy (5,6). A number of studies have investigated
the efficacy of checkpoint inhibitor immunotherapy against TNBC
(5,7–9). For
example, pembrolizumab and atezolizumab plus nab-paclitaxel have
demonstrated encouraging clinical benefits in patients with
advanced TNBC (5,9).
Cancer immunoediting is the process of eliminating
highly immunogenic tumor cells by somatic evolution and protecting
the host from tumor development through the host immune system
(10). Increased burden of somatic
mutations has been associated with an increased number of
pathogenic germline mutations in high- and moderate-risk BC genes
in patients with BC (11). The
frequency of somatic mutations or tumor mutation burden (TMB) is
associated with the immunogenicity of BC (10). Assessment of TMB is becoming
increasingly important for immunotherapy decisions in patients with
melanoma and lung cancer (12);
however, TMB heterogeneity across BC subtypes has not been well
characterized. The aim of the present study was to examine whether
the TMB of ER (or PR and HER2)-negative BC differs from that of the
corresponding positive subtypes. In addition, the study aimed to
examine what molecular cues are associated with the differences in
TMB between the negative and positive subtypes and whether there is
a difference in immunogenic activity between ER (or PR and
HER2)-negative and -positive BC. The distribution of TMB,
expression of mismatch repair (MMR) genes and immune-associated
genes were comprehensively compared among BC subtypes. HR-negative
BC was found to have a higher TMB and increased expression of major
immune cell types [B cells, CD4+ and CD8+ T
cells, and natural killer (NK) cells] compared with HR-positive BC.
Of note, HER2-positive BC tended to have higher TMB and increased
immune gene expression compared with HER2-negative BC.
Materials and methods
The Cancer Genome Atlas (TCGA)
whole-exome sequencing (WES) and RNA-seq data
Whole-exome somatic variants, gene expression and
clinical data, including ER, PR and HER2 status, of 974 patients
with BC were downloaded from Broad TCGA GDAC (v2016_01_28)
(13). In the TCGA clinical dataset,
ER or PR status is reported as negative or positive. HER2 status is
reported as a score ranging between 0 and 3. A score of 0 or 1 is
considered as HER2-negative, and a score of 3 as HER2-positive.
Calculation of TMB
TMB was defined as the total number of somatic
missense substitutions of the exomes examined. Alternatively, TMB
may be defined as the total number of somatic, coding, base
substitution and indel mutations. In this case, all base
substitutions and indels in the coding region, including silent
alterations, are counted. Both methods were used for calculation of
TMB, and the results were essentially identical. Only the results
based on all base substitutions and indels are presented.
Expression analysis of MMR genes
The normalized expression levels (RNAseqV2, quantile
normalized by RSEM) were downloaded from Broad TCGA GDAC
(v2016_01_28) (13). Five
MMR-associated genes (14),
including MLH1, MLH3, MSH2, MSH6 and PMS2, were
analyzed. Patients that harbored at least two MMR genes with
expression levels in the lower 10% percentile across the cohort
were considered as potentially aberrant (lost expression).
Expression analysis of immune cell
types
To investigate the difference in the expression
levels of immune cell types among different BC subtypes, 4 major
immune cell types were selected for examination, including B cells,
CD4+ T cells, CD8+ T cells and NK cells. Cell
type marker genes were identified based on the previous literature
(15,16). B-cell marker genes include CD79A,
CD79B, BTLA, FCRL1, FCRL3, BANK1, BLK and RALGPS2.
CD4+ T-cell marker genes include CTLA4, IL32, FOXP3,
GPR15 and C15orf53. CD8A is considered as a
CD8+ T-cell marker. NK-cell marker genes include
KLRF1 and KLRC1.
Statistical analysis
Analyses were performed using SPSS (v.20.0, IBM
Corporation, Armonk, NY, USA). Data are presented as mean ± SD. The
non-parametric Wilcoxon's rank-sum test was used to assess the
differences in TMB between patients with negative and positive
hormone receptor status (ER, PR or HER2). Differences in the
proportion of samples with aberrant expression of MMR genes between
ER-, PR- or HER2-negative and -positive status were assessed by the
χ2 test. Similar results were observed when the lower 5%
percentile was considered as the cut-off to define aberrant
expression. P<0.05 was considered to indicate a statistically
significant difference.
Results
TMB differs significantly between
HR-negative and HR-positive BC
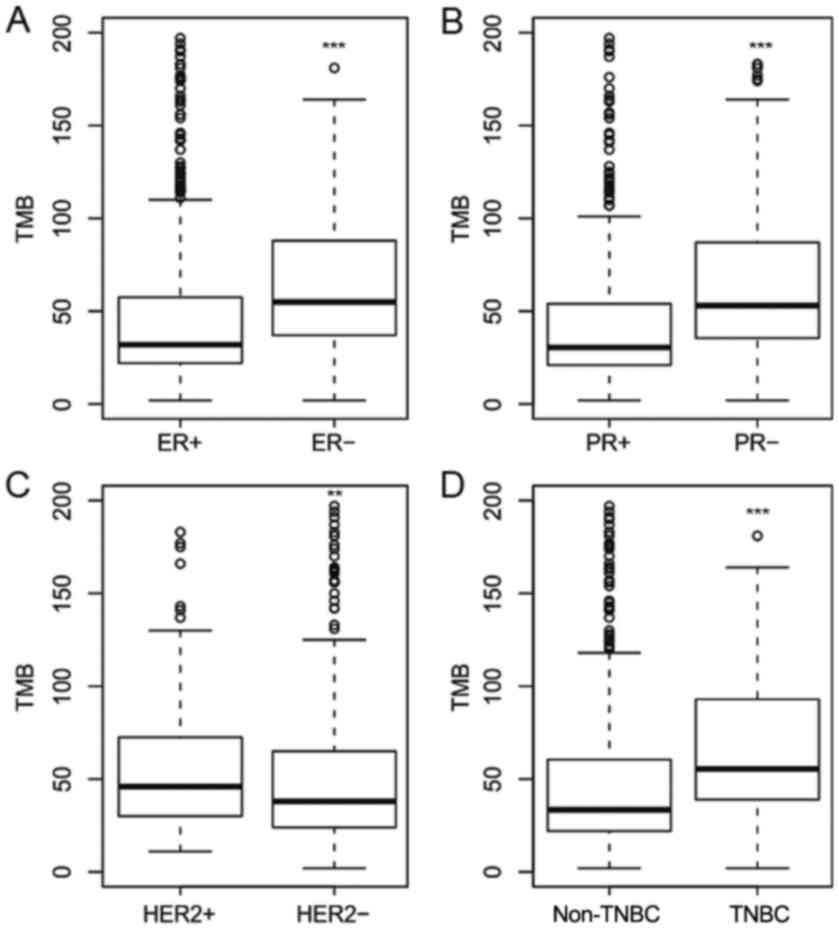
To investigate the mutation burden heterogeneity
across BC subtypes, TMB was compared between patients who were ER
(or PR, HER2)-negative and patients who were ER (or PR,
HER2)-positive. TMB was defined as the total number of coding SNVs6
and indels. Across the TCGA cohort of 974 BC samples, the number of
exome mutations in individual cancers varies widely (range,
2–4,561; median, 38). The TMB and ER/PR/HER2 status were analyzed
(data not shown). Patients who were ER-negative were found to have
a significantly higher TMB (P=4.1×10−13; Wilcoxon's
rank-sum test) compared with patients who were ER-positive
(Fig. 1A). The median TMB was 55 and
32 for patients ER-negative and ER-positive, respectively.
PR-negative tumors also had a significantly higher TMB
(P<2.2×10−16; Wilcoxon's rank-sum test) compared with
PR-positive tumors (Fig. 1B). The
median TMB was 53 and 30.5 for patients who were PR-negative and
PR-positive, respectively. By contrast, HER2-negative tumors had a
significantly lower TMB (P=0.02; Wilcoxon's rank-sum test) compared
with HER2-positive tumors (Fig. 1C).
The median TMB was 38 and 46 for patients who were HER2-negative
and HER2-positive, respectively. The increased TMB in the
HER2-positive group was more evident in patients who were
HR-positive, however was not observed in the HR-negative group
(data not shown). Patients with TNBC also had a significantly
higher TMB (P=9.4×10−06; Wilcoxon's rank-sum test)
compared with patients with non-TNBC (Fig. 1D). The median TMB was 55.5 and 38 for
patients with TNBC and non-TNBC patients, respectively. These
results suggest that TMB heterogeneity is common among different BC
subtypes based on HR and HER2 status. In general, HR-negative BC
has a higher TMB compared with HR-positive BC, and HER2-negative BC
tends to have a lower TMB compared with HER2-positive BC.
Aberrant expression of MMR genes is
more common in HR-negative BC
In order to investigate the molecular cues of
increased TMB in ER- or PR-negative BC, statistical analysis was
performed to test whether the presence of aberrant MMR expression
was associated with BC subtypes. Five MMR-associated genes,
including MLH1, MLH3, MSH2, MSH6 and PMS2, were
analyzed. Patients that harbored at least two MMR genes with
expression levels in the lower 10% percentile across the TCGA
cohort were considered as potentially aberrant (lost expression).
The expression levels of each MMR gene and ER/PR/HER2 status were
analyzed (data not shown). Aberrant expression of MMR genes was
found to be more common (P<0.001; χ2 test) in
HR-negative BC compared with HR-positive BC (Table I). However, the proportion of
aberrant MMR gene expression did not differ significantly (P=0.1;
χ2 test) between patients who were HER2-positive and
HER2-negative (Table I). This
pattern is consistent with the pattern observed when comparing TMB
among BC subtypes. The results suggest that aberrant expression of
MMR genes is more common in HR-negative patients with BC.
 | Table I.MMR gene expression in patients with
BC with different ER/PR/HER2 status. |
Table I.
MMR gene expression in patients with
BC with different ER/PR/HER2 status.
| Status | Aberrant MMR
expression | Normal MMR
expression | P-valuea |
|---|
| ER- | 46 | 167 | P<0.0001 |
| ER+ | 75 | 641 |
|
| PR- | 62 | 245 | P<0.0001 |
| PR+ | 59 | 560 |
|
| HER2- | 59 | 427 | P=0.091 |
| HER2+ | 4 | 76 |
|
HR-negative BC exhibits increased
expression levels of immune cell marker genes
Previous studies have used genomic data from TCGA to
characterize cytolytic activity estimated using the expression of
two genes (15,17,18).
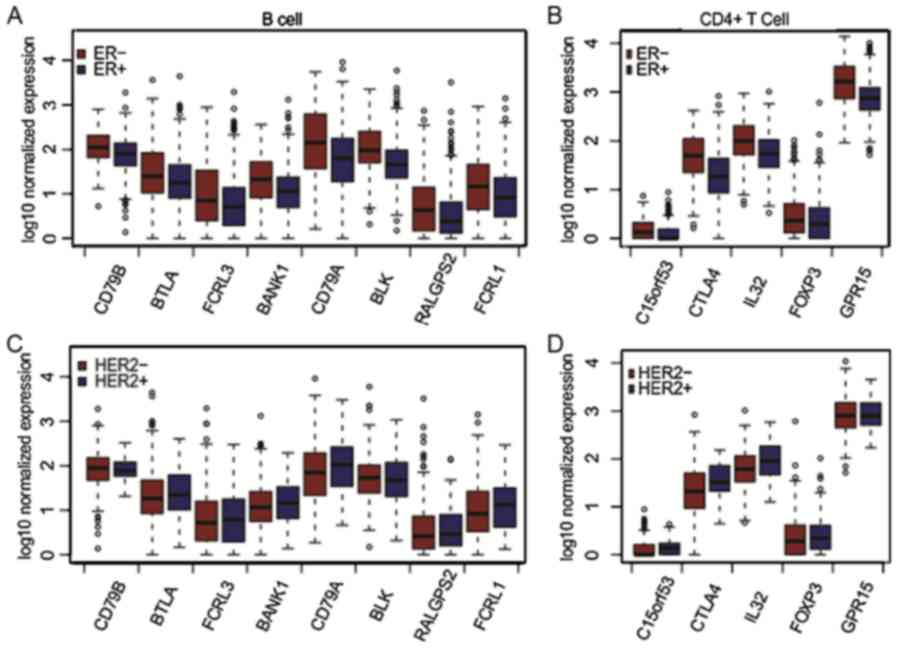
Recently, marker gene expression was used to analyze infiltration
of various immune cell types (16,19–21). In
the present study, 4 major immune cell types, including
CD4+ T cells, CD8+ T cells, B cells and NK
cells, were analyzed. The expression levels of the aforementioned
marker gene sets for each cell type were compared between different
BC subtypes. Significantly higher expression levels of each immune
marker gene were found in patients who were HR-negative compared
with patients who were HR-positive (P<0.001; Fig. 2 and Table
II). By contrast, the HER2-positive group exhibited
significantly increased expression of immune marker genes, such as
CTLA4, FCRL1, C15orf53 and CD79A, compared with the HER2-negative
group (P<0.001; Wilcoxon's rank-sum test). A similar trend was
observed in gene expression between HER2-positive and HER2-negative
groups only in patients who were HR-positive. The median expression
levels for each marker gene in patients with different ER/PR/HER2
status are provided in Table II.
These results suggest that HR-negative BC may exhibit increased
immunogenic activity compared with HR-positive BC. Furthermore,
HER2-positive BC may exhibit increased immunogenic activity
compared with HER2-negative BC.
| Table II.Gene expression from B Cell/T Cell/NK
Cell in patients with BC with different ER/PR/HER2 status. |
Table II.
Gene expression from B Cell/T Cell/NK
Cell in patients with BC with different ER/PR/HER2 status.
| A, B cell |
|---|
|
|---|
| Gene | ER_NEG | ER_POS | PR_NEG | PR_POS | HER2_NEG | HER2_POS | TRIPLE_NEG | NON_TRIPLE |
|---|
| CD79B | 108.6660 | 80.5172 | 94.0301 | 81.7910 | 80.8910 | 75.8138 | 113.5951 | 72.3639 |
| BTLA | 24.1280 | 16.8827 | 21.9850 | 16.9827 | 16.3043 | 20.5051 | 31.5309 | 16.2235 |
| FCRL3 | 6.0477 | 4.1124 | 4.9558 | 4.1163 | 3.8578 | 4.9408 | 6.54325 | 4.1272 |
| BANK1 | 20.2347 | 10.3978 | 15.2576 | 10.5348 | 10.5432 | 13.4445 | 18.9792 | 11.8900 |
| CD79A | 141.0011 | 61.8596 | 106.4768 | 62.0842 | 63.7342 | 102.0126 | 151.2536 | 73.3673 |
| BLK | 94.1826 | 44.5720 | 78.2432 | 44.7591 | 49.9627 | 48.1587 | 108.8669 | 35.4945 |
| RALGPS2 | 3.3266 | 1.4465 | 2.2954 | 1.4508 | 1.4550 | 1.8520 | 3.3051 | 1.7174 |
| FCRL1 | 13.7678 | 7.3211 | 10.6117 | 7.3071 | 7.2333 | 12.0030 | 12.9948 | 11.8360 |
|
| B, CD4+ T
cell |
|
| Gene | ER_NEG | ER_POS | PR_NEG | PR_POS |
HER2_NEG |
HER2_POS |
TRIPLE_NEG |
NON_TRIPLE |
|
| C15orf53 | 0.3477 | 0.0000 | 0.3127 | 0.0000 | 0.0000 | 0.3605 | 0.2955 | 0.3269 |
| CTLA4 | 49.0202 | 17.7471 | 39.7454 | 17.4976 | 20.1526 | 32.0127 | 56.9741 | 32.1545 |
| IL32 | 98.8562 | 54.1037 | 86.7804 | 52.8931 | 56.4775 | 88.3388 | 99.1651 | 79.2368 |
| FOXP3 | 1.3298 | 0.9843 | 1.2318 | 0.9814 | 0.8780 | 1.2063 | 0.9259 | 0.7234 |
| GPR15 | 1657.1686 | 751.7339 | 1184.3091 | 755.4254 | 803.0842 | 786.9443 | 1861.1596 | 848.1356 |
|
| C, CD8+ T
cell |
|
| Gene | ER_NEG | ER_POS | PR_NEG | PR_POS |
HER2_NEG |
HER2_POS |
TRIPLE_NEG |
NON_TRIPLE |
|
| CD8A | 188.2387 | 148.8562 | 163.3699 | 151.1880 | 151.2229 | 152.5424 | 194.0695 | 168.3510 |
|
| D, NK
cell |
|
| Gene | ER_NEG | ER_POS | PR_NEG | PR_POS |
HER2_NEG |
HER2_POS |
TRIPLE_NEG |
NON_TRIPLE |
|
| KLRF1 | 5.4054 | 2.9576 | 4.39585 | 3.01835 | 3.1873 | 3.6188 | 5.0695 | 3.3683 |
| KLRC1 | 3.6041 | 3.0883 | 2.9054 | 3.22965 | 2.9617 | 3.2038 | 3.1361 | 2.5931 |
Discussion
Cancer immunoediting is the process of eliminating
highly immunogenic tumor cells by somatic evolution, and protecting
the host from tumor development through the host immune system
(7). Molecular studies have reported
that mutational heterogeneity in BC was associated with novel
cancer-associated genes, such as breast cancer genes 1 and 2
(BRCA1/2) and ataxia telangiectasia mutated (ATM) serine/threonine
kinase, and antigens (CD8+, PD-L1+) that were produced by mutated
genes, aberrantly expressed normal genes, or genes encoding viral
proteins (7–9,22). The
frequency of somatic mutations or TMB was associated with the
immunogenicity of breast cancer. The present study characterized
and provided extensive data describing TMB differences between ER
(or PR, HER2)-negative and ER (or PR, HER2)-positive patients with
BC. It was observed that the HR-negative group had a higher TMB
compared with the HR-positive group. Shaw et al (23) demonstrated that the level of TMB
calculated by total circulating free DNA and the circulating tumor
cell count (≥5) were both significantly associated with overall
survival in patients with metastatic BC, unlike the
cancer-associated biomarkers, including cancer antigen 15-3 and
alkaline phosphatase (23,24). The similar trend of estrogen receptor
1 and KRAS proto-oncogene, GTPase gene mutations was absent from
primary tumor tissue, and appeared to be acquired with disease
progression (23,25). This TMB marker may reflect the degree
of metastatic burden and may serve as a favorable predictor for
clinical decision-making. The total mutation burden was correlated
with response to chemotherapy and poly (ADP-ribose) polymerase
inhibitors in patients with ovarian cancer with BRCA1/2
mutations (26). Low TMB predicted
resistance to chemotherapy, whereas high TMB predicted a remarkably
favorable clinical outcome in mBRCA-associated ovarian
cancer in the TCGA cohort (26). Our
previous study revealed that the TMB value in patients with breast
cancer can be predicted based on the expression levels of ER, PR,
HER-2 and Ki-67 (27). These
observations suggest that TMB coupled with HR negativity in BC is a
genomic marker of prognosis and a predictor of response to
immunotherapy.
These results revealed that the aberrant expression
of MMR genes may contribute to the increased TMB in HR-negative
patients. BC is a relatively heterogeneous disease, and deficiency
of major BC-susceptibility genes in DNA repair pathways, including
MMR, may be involved in familial BC and implicated in higher TMB
(28,29). An increasing number of studies
suggest that triple-negative, luminal B-like or HER2-positive
tumors harbor a high mutational burden, and these molecular types
are considered as immunogenic (7,27). An
interesting finding of the present study is that patients who were
HER2-positive (particular in the HR-positive group) indicated to
have higher TMB and increased expression levels of immune cell
marker genes compared with patients who were HER2-negative.
Immunotherapeutic strategies may increase the quality or quantity
of immune effector cells, reveal additional protective tumor
antigens, and/or eliminate cancer-induced immunosuppressive
mechanisms (7). Large clinical
trials of multiple immunotherapy approaches in patients with BC are
ongoing, including therapeutic administration of monoclonal
antibodies to target and relieve cancer-induced immunosuppression,
including CTLA-4, PD-1 or Treg cells (7,9).
Previous studies have been focused on immunotherapy for TNBC
instead of other subtypes of BC. In triple-negative breast cancer,
Atezolizumab plus nab-paclitaxel prolonged progression-free
survival among patients with metastatic triple-negative breast
cancer in both the intention-to-treat population and the
PD-L1-positive subgroup; among patients with PD-L1-positive tumors,
the median overall survival was prolonged by ~10 months following
Atezolizumab plus nab-paclitaxel treatment (9). In HER-2 positive breast cancer, six
(15%) of 40 PD-L1-positive patients achieved an objective response
ratio (ORR) with pembrolizumab, a PD-1 inhibitor in the PANACEA
study (30). Similarly, an ORR of
only 12.0% and CBR of 20% with monotherapy of pembrolizumab were
observed in ER-positive/HER2-negative metastatic breast cancer
(31). Based on gene markers in
CD4+ T cells, CD8+ T cells, B cells and NK
cells in the present study, the findings suggested that HER2 status
was correlated to a certain extent with immunogenic activity and,
therefore, HER2 status may also be considered for immune checkpoint
inhibition, particularly in patients who are HR-positive.
In conclusion, in the present study, HR-negative or
HER2-positive BC were found to exhibit increased TMB and
immunogenic activity. The present study presents immunotherapeutic
options recommended for such patients.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Liaoning
Province Doctor Startup Fund Program (grant no. 201501108),
National Nature Science Foundation (grant no. 81502188), National
Natural Science Foundation of Liaoning (grant no. 2015020251),
Central Guidance for Special Funds (grant no. 2016007011) and the
Clinical Capability Construction Project for Liaoning Provincial
Hospitals (grant no. LNCCC-C05-2015).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JX, HB and XW performed the literature search, data
extraction and statistical analysis, and drafted the manuscript.
TS, XNW and YS designed and supervised the study. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Liaoning Cancer Hospital & Institute (Shenyang, China).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
DeSantis CE, Ma J, Goding Sauer A, Newman
LA and Jemal A: Breast cancer statistics, 2017, racial disparity in
mortality by state. CA Cancer J Clin. 67:439–448. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Effi AB, Aman NA, Koui BS, Koffi KD,
Traore ZC and Kouyate M: Breast cancer molecular subtypes defined
by ER/PR and HER2 status: Association with clinicopathologic
parameters in ivorian patients. Asian Pac J Cancer Prev.
17:1973–1978. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dunnwald LK, Rossing MA and Li CI: Hormone
receptor status, tumor characteristics, and prognosis: A
prospective cohort of breast cancer patients. Breast Cancer Res.
9:R62007. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Davis SL, Eckhardt SG, Tentler JJ and
Diamond JR: Triple-negative breast cancer: Bridging the gap from
cancer genomics to predictive biomarkers. Ther Adv Med Oncol.
6:88–100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nanda R, Chow LQ, Dees EC, Berger R, Gupta
S, Geva R, Pusztai L, Pathiraja K, Aktan G, Cheng JD, et al:
Pembrolizumab in patients with advanced triple-negative breast
cancer: Phase Ib KEYNOTE-012 study. J Clin Oncol. 34:2460–2467.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hartman ZC, Poage GM, den Hollander P,
Tsimelzon A, Hill J, Panupinthu N, Zhang Y, Mazumdar A, Hilsenbeck
SG, Mills GB and Brown PH: Growth of triple-negative breast cancer
cells relies upon coordinate autocrine expression of the
proinflammatory cytokines IL-6 and IL-8. Cancer Res. 73:3470–3480.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Adams S, Schmid P, Rugo HS, Winer EP,
Loirat D, Awada A, Cescon DW, Iwata H, Campone M, Nanda R, et al:
Pembrolizumab monotherapy for previously treated metastatic
triple-negative breast cancer: Cohort A of the phase II KEYNOTE-086
study. Ann Oncol. 30:397–404. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Adams S, Loi S, Toppmeyer D, Cescon DW, De
Laurentiis M, Nanda R, Winer EP, Mukai H, Tamura K, Armstrong A, et
al: Pembrolizumab monotherapy for previously untreated,
PD-L1-positive, metastatic triple-negative breast cancer: Cohort B
of the phase II KEYNOTE-086 study. Ann Oncol. 30:405–411. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schmid P, Adams S, Rugo HS, Schneeweiss A,
Barrios CH, Iwata H, Diéras V, Hegg R, Im SA, Shaw Wright G, et al:
Atezolizumab and nab-paclitaxel in advanced triple-negative breast
cancer. N Engl J Med. 379:2108–2121. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Criscitiello C and Curigliano G:
Immunotherapy of breast cancer. Prog Tumor Res. 42:30–43. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rummel SK, Lovejoy L, Shriver CD and
Ellsworth RE: Contribution of germline mutations in cancer
predisposition genes to tumor etiology in young women diagnosed
with invasive breast cancer. Breast Cancer Res Treat. 164:593–601.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chalmers ZR, Connelly CF, Fabrizio D, Gay
L, Ali SM, Ennis R, Schrock A, Campbell B, Shlien A, Chmielecki J,
et al: Analysis of 100,000 human cancer genomes reveals the
landscape of tumor mutational burden. Genome Med. 9:342017.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tomczak K, Czerwińska P and Wiznerowicz M:
The cancer genome atlas (TCGA): An immeasurable source of
knowledge. Contemp Oncol (Pozn). 19:A68–A77. 2015.PubMed/NCBI
|
|
14
|
Boland CR and Goel A: Microsatellite
instability in colorectal cancer. Gastroenterology. 138:2073–2087,
e2073. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rooney MS, Shukla SA, Wu CJ, Getz G and
Hacohen N: Molecular and genetic properties of tumors associated
with local immune cytolytic activity. Cell. 160:48–61. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Danaher P, Warren S, Dennis L, D'Amico L,
White A, Disis ML, Geller MA, Odunsi K, Beechem J and Fling SP:
Gene expression markers of Tumor Infiltrating Leukocytes. J
Immunother Cancer. 5:182017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Low SK, Zembutsu H and Nakamura Y: Breast
cancer: The translation of big genomic data to cancer precision
medicine. Cancer Sci. 109:497–506. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kraya AA, Maxwell KN, Wubbenhorst B, Wenz
BM, Pluta J, Rech AJ, Dorfman LM, Lunceford N, Barrett A, Mitra N,
et al: Genomic signatures predict the immunogenicity of
BRCA-deficient breast cancer. Clin Cancer Res.
pii:clincanres.0468.2018. 2019.
|
|
19
|
Stovgaard ES, Nielsen D, Hogdall E and
Balslev E: Triple negative breast cancer-prognostic role of
immune-related factors: A systematic review. Acta Oncol. 57:74–82.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yang J, Xu J, E Y and Sun T: Predictive
and prognostic value of circulating blood lymphocyte subsets in
metastatic breast cancer. Cancer Med. 8:492–500. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Xu J, Jiang L, Cao H, Jia Y, Wu S, Jiang C
and Sun T: Predictive value of CD4+/CD8+
ratio in patients with breast cancer receiving recombinant human
thrombopoietin. J Interferon Cytokine Res. 38:213–220. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
McGrail DJ, Federico L, Li Y, Dai H, Lu Y,
Mills GB, Yi S, Lin SY and Sahni N: Multi-omics analysis reveals
neoantigen-independent immune cell infiltration in copy-number
driven cancers. Nat Commun. 9:13172018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shaw JA, Guttery DS, Hills A,
Fernandez-Garcia D, Page K, Rosales BM, Goddard KS, Hastings RK,
Luo J, Ogle O, et al: Mutation analysis of cell-free DNA and single
circulating tumor cells in metastatic breast cancer patients with
high circulating tumor cell counts. Clin Cancer Res. 23:88–96.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bidard FC, Hajage D, Bachelot T, Delaloge
S, Brain E, Campone M, Cottu P, Beuzeboc P, Rolland E, Mathiot C
and Pierga JY: Assessment of circulating tumor cells and serum
markers for progression-free survival prediction in metastatic
breast cancer: A prospective observational study. Breast Cancer
Res. 14:R292012. View
Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xu J, Sun T, Guo X, Wang Y and Jing M:
Estrogen receptor-α promoter methylation is a biomarker for outcome
prediction of cisplatin resistance in triple-negative breast
cancer. Oncol Lett. 15:2855–2862. 2018.PubMed/NCBI
|
|
26
|
Birkbak NJ, Kochupurakkal B, Izarzugaza
JM, Eklund AC, Li Y, Liu J, Szallasi Z, Matulonis UA, Richardson
AL, Iglehart JD and Wang ZC: Tumor mutation burden forecasts
outcome in ovarian cancer with BRCA1 or BRCA2 mutations. PLoS One.
8:e800232013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Xu J, Guo X, Jing M and Sun T: Prediction
of tumor mutation burden in breast cancer based on the expression
of ER, PR, HER-2, and Ki-67. Onco Targets Ther. 11:2269–2275. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Win AK, Lindor NM and Jenkins MA: Risk of
breast cancer in Lynch syndrome: A systematic review. Breast Cancer
Res. 15:R272013. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kappil M, Terry MB, Delgado-Cruzata L,
Liao Y and Santella RM: Mismatch repair polymorphisms as markers of
breast cancer prevalence in the breast cancer family registry.
Anticancer Res. 36:4437–4441. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Loi S, Giobbie-Hurder A, Gombos A,
Bachelot T, Hui R, Curigliano G, Campone M, Biganzoli L, Bonnefoi
H, Jerusalem G, et al: Pembrolizumab plus trastuzumab in
trastuzumab-resistant, advanced, HER2-positive breast cancer
(PANACEA): A single-arm, multicentre, phase 1b-2 trial. Lancet
Oncol. 20:371–382. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Rugo HS, Delord JP, Im SA, Ott PA,
Piha-Paul SA, Bedard PL, Sachdev J, Tourneau CL, van Brummelen EMJ,
Varga A, et al: Safety and antitumor activity of pembrolizumab in
patients with estrogen receptor-positive/human epidermal growth
factor receptor 2-negative advanced breast cancer. Clin Cancer Res.
24:2804–2811. 2018. View Article : Google Scholar : PubMed/NCBI
|