Introduction
At present, the main treatments for oral squamous
cell carcinoma (OSCC) are surgery, chemotherapy and radiotherapy
(RT). RT is a particularly effective strategy for OSCC, since it is
employed as both a primary modality and an adjuvant treatment
following surgery. Despite modern radiation techniques, many
studies have highlighted several complications associated with RT,
including bone marrow suppression (1–3).
Disregarding the associated complications, the therapeutic success
of RT is also challenged by the development of tumor-cell
radioresistance, which can be attributed to cell cycle,
differentiation and hypoxia (4–6). Among
these, tumor hypoxia is known to exhibit a significantly strong
association with radioresistance (7,8).
Therefore, resolving tumor hypoxia could be a key strategy in
overcoming radioresistance and improving the antitumor effect of
RT.
The importance of improving tumor oxygenation for
potential clinical use has already been recognized and some
strategies, including the use of radio-sensitizers and hypoxic
cytotoxins, have been developed to overcome hypoxia-mediated tumor
radioresistance (9). However, these
strategies often lead to the development of more severe
side-effects (10,11).
Tumor hypoxia is a characteristic feature of
malignant tumors, including OSCC (12). In hypoxic conditions, hypoxia
inducible factor-1α (HIF-1α), an oxygen-dependent α subunit of HIF,
activates the transcription of specific metastatic genes, thus
playing an important role in the growth and survival of malignant
tumors (13,14). In addition, a recent study has
revealed that HIF-1α plays an important role in hypoxia-related
tumor radioresistance (15).
We previously revealed that transcutaneous
CO2 application caused absorption of CO2 and
an increase in the O2 pressure in treated tissues,
potentially causing an ‘artificial Bohr effect’ (16). We have also reported that
CO2 therapy induced mitochondrial apoptosis and
suppressed tumor growth in OSCC by resolving hypoxia (17). Furthermore, we have revealed that
transcutaneous CO2 decreased the expression of HIF-1α in
OSCC. Considering our previous study, we hypothesized that
transcutaneous CO2 may enhance the antitumor effect of
RT on OSCC by improving intratumoral hypoxia, thereby overcoming
radioresistance.
In the present study, we investigated the antitumor
effects of a combination treatment of transcutaneous CO2
with RT by using human OSCC xenograft models in vivo.
Materials and methods
Cell culture
A human OSCC cell line, HSC-3, was used in our study
(Health Science Research Resources Bank, Osaka, Japan). The HSC-3
cell line was established from a metastatic deposit of poorly
differentiated OSCC of the tongue in a mid-internal jugular lymph
node from a 64-year-old man (18).
The HSC-3 cells were routinely cultured in Eagle's minimum
essential medium (EMEM; Sigma-Aldrich, St. Louis, MO, USA)
supplemented with 10% fetal bovine serum (FBS; Sigma-Aldrich) and
1,000 U/ml penicillin/streptomycin solution (Sigma-Aldrich) in an
incubator with 5% CO2 at 37°C. Trypsin (0.25%) and
ethylenediaminetetraacetic acid (EDTA, 0.02%) (Sigma-Aldrich)
solution were used to isolate the cells for subculture, as
previously described (17,19).
X-ray irradiation
X-ray irradiation was performed at a dose rate of
0.75–0.78 Gy/min using a 150 kV X-ray generator unit operating at 5
mA with an external 0.1 mm aluminum filter (MBR-1505122; Hitachi
Medical Co., Tokyo, Japan).
Colony formation assay
Colony formation assays for the X-ray irradiated
HSC-3 cells were performed to evaluate the response of these cells
to X-ray irradiation. HSC-3 cells in T-25 flasks (Corning Japan,
Tokyo, Japan) were treated by X-ray irradiation at three different
doses (0, 2 or 8 Gy). Immediately after X-ray irradiation, the
cells were trypsinized, seeded at a density of 1,000 cells/well in
6-well plates, and incubated in a humidified atmosphere of 5%
CO2 at 37°C. After 2 weeks of incubation, the cells were
stained by Giemsa (Muto Pure Chemicals Co., Tokyo, Japan) and the
number of colonies was counted.
Animal models
Twenty-four male athymic BALB/c nude mice,
7-week-old, were obtained from CLEA Japan (Tokyo, Japan). The
animals were maintained under pathogen-free conditions, in
accordance with the institutional guidelines. All animal
experiments were performed in accordance with the Guidelines for
Animal Experimentation of Kobe University Animal Experimentation
Regulations (permission no. P120602) and were approved by the
Institutional Animal Care and Use Committee. HSC-3 cells at doses
of 4.0×106 cells in 500 µl phosphate buffered saline (PBS) were
implanted into the back of 24 mice to create the human OSCC
xenograft models.
Transcutaneous CO2
therapy
Transcutaneous CO2 therapy was performed
as previously described (17,19).
Briefly, the area of skin around the implanted tumor was covered
with CO2 hydrogel. This area was then sealed with a
polyethylene bag, and 100% CO2 gas was administered into
the bag. Treatment was performed for 20 min each, twice a week for
2 weeks. Animals in the control group were treated in a similar
manner by replacing CO2 with room air.
In vivo studies
The mice implanted with HSC-3 cells were randomly
divided into four groups: control group (n=6), RT group (n=6),
CO2 group (n=6) or the combination group (n=6). RT was
performed at a dose of 5.0 Gy each and in the RT group, the mice
were treated by RT alone twice a week for 2 weeks (20 Gy in total).
Mice in the CO2 group were treated by transcutaneous
CO2 therapy alone. In the combination group, the mice
were treated by CO2 therapy, immediately followed by RT.
Tumor volume and body weight were monitored and calculated as
previously described (17,19).
Treated tumors were removed 24 h after the final
treatment and the total RNA and cell lysates were immediately
extracted from the half of each tumor. The other half of each tumor
was formalin-fixed and paraffin-embedded for staining. Serial 10-μm
thick transverse sections were prepared from each block. Bone
marrow suppression was investigated by the collection of 10 µl
blood samples by inserting a heparinized capillary tube just below
the eye ball. The obtained samples were diluted with Turk's
solution (190 µl) and the leukocytes (white blood cells) in the
samples were counted using a heamocytometer by a clinical
laboratory technician.
Fluorescence activated cell scanning
(FACS) assay
Flow cytometry was performed using a FACS Calibur™
flow cytometer (BD Pharmingen; BD Biosciences, Franklin Lakes, NJ,
USA) as previously described (17).
The apoptotic activity in treated tumors was evaluated by DNA
fragmentation using the Apo-Direct kit according to the
manufacturer's protocol (BD Pharmingen; BD Biosciences). In
addition, ROS production was evaluated using anti-human ROS
modulator 1 (ROMO-1) antibody (1:1,000; cat. no. ab121379; Abcam,
Cambridge, UK) as an indicator. The data were analyzed using BD
CellQuest software (BD Biosciences), and apoptotic or ROMO-1
expression cells were quantified as a percentage of the total
number of cells.
Immunohistochemical analysis
The formalin-fixed and paraffin-embedded tumor
sections were pretreated with citrate buffer for 40 min at 95°C,
quenched with 0.05% H2O2 and incubated
overnight at 4°C with the following primary antibodies in Can Get
Signal immunostain solution A (Toyobo, Osaka, Japan): rabbit
anti-human HIF-1α antibody (1:1,000; cat. no. ab82832; Abcam) and
anti-human ROS modulator 1 (ROMO-1) antibody (1:1,000; cat. no.
ab121379; Abcam). Following the treatment, the sections were
incubated with horseradish peroxidase (HRP)-conjugated goat
anti-rabbit IgG polyclonal antibody (1:1,000; cat. no. 6721;
Nichirei Bioscience, Tokyo, Japan) for 30 min at room temperature.
Signals were developed as a brown reaction product using peroxidase
substrate 3′,3′-diaminobenzidine (Nichirei Bioscience). The
sections were counterstained with hematoxylin and examined with a
BZ-8000 confocal microscope (Keyence, Osaka, Japan).
Immunohistochemical-positive staining was semi-quantified by
densitometric analysis using the ImageJ software, version 1.47
(National Institutes of Health, Bethesda, MD, USA) (http://rsbweb.nih.gov/ij/download.html).
Values were normalized against the control group and were presented
as ratios.
Immunofluorescence staining
To assess the apoptotic activity in treated tumors,
we performed the immunofluorescence staining by using the
Apo-Direct kit following the manufacturer's protocol (BD
Biosciences). The nucleus was stained with DAPI. The images were
captured using a BZ-8000 confocal microscope (Keyence).
Immunoblot analysis
The cell lysates were prepared from treated tumors
by using a whole cell lysis buffer supplemented with Halt protease
and phosphatase inhibitor cocktail (Mammalian Protein Extraction
Reagent; Thermo Fisher Scientific, Rockford, IL, USA). The protein
samples were processed using standard western immunoblot
procedures. The membranes were incubated overnight at 4°C with the
following primary antibodies in Can Get Signal Immunoreaction
Enhancer Solution 1 (Toyobo): anti-human caspase-8 antibody
(1:1,000; cat. no. 9496; Cell Signaling Technology, Danvers, MA,
USA), anti-human caspase-9 antibody (1:1,000; cat. no. 7237; Cell
Signaling Technology), anti-human caspase-3 antibody (1:1,000; cat.
no. 9664; Cell Signaling Technology), anti-human PARP antibody
(1:1,000; cat. no. 5625; Cell Signaling Technology) and anti-human
α-tubulin antibody (1:2,000; cat. no. 6074; Sigma-Aldrich). After
washing, the membranes were incubated with the appropriate
secondary antibody conjugated to horseradish peroxidase (GE
Healthcare Bio-Sciences, Piscataway, NJ, USA) in Can Get Signal
Immunoreaction Enhancer Solution 2 (Toyobo) and exposed with ECL
Prime Plus Western Blotting Detection System Reagent (GE Healthcare
Bio-Sciences, Pittsburgh, PA, USA). The signals were detected using
a Chemilumino analyzer LAS-3000 mini (Fujifilm, Tokyo, Japan).
Positive bands in the immunoblots were semi-quantified by
densitometric analysis using ImageJ software version 1.47. The
values were normalized against α-tubulin and were presented as
ratios.
Statistical analysis
StatView J-4.5 software (Hulinks, Inc., Tokyo,
Japan) was used for statistical analysis performed on all data for
four groups by the Scheffe's test. Data was presented as the mean
value ± standard error. P-value <0.05 was considered to indicate
a statistically significant difference.
Results
RT induces ROS-related apoptosis in
human HSC-3 cells in vitro
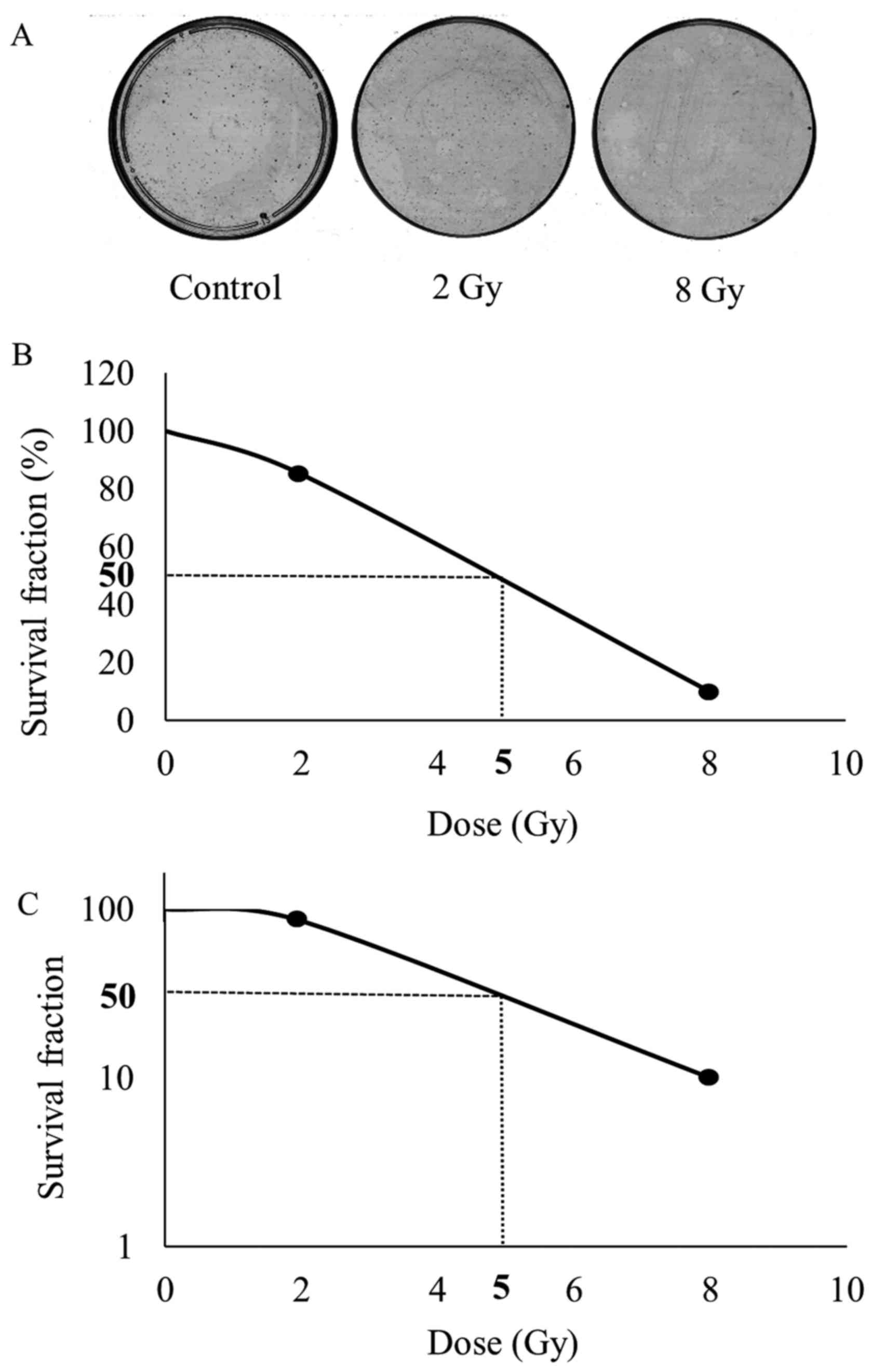
Colony formation assays for HSC-3 cells irradiated
by various doses of X-rays were performed to evaluate the response
of these cells to RT. The number of HSC-3 cell colonies decreased
dose-dependently after RT (Fig.
1A). The half maximal inhibitory concentration
(IC50) in colony formation was achieved at a dose of 5.0
Gy (Fig. 1B).
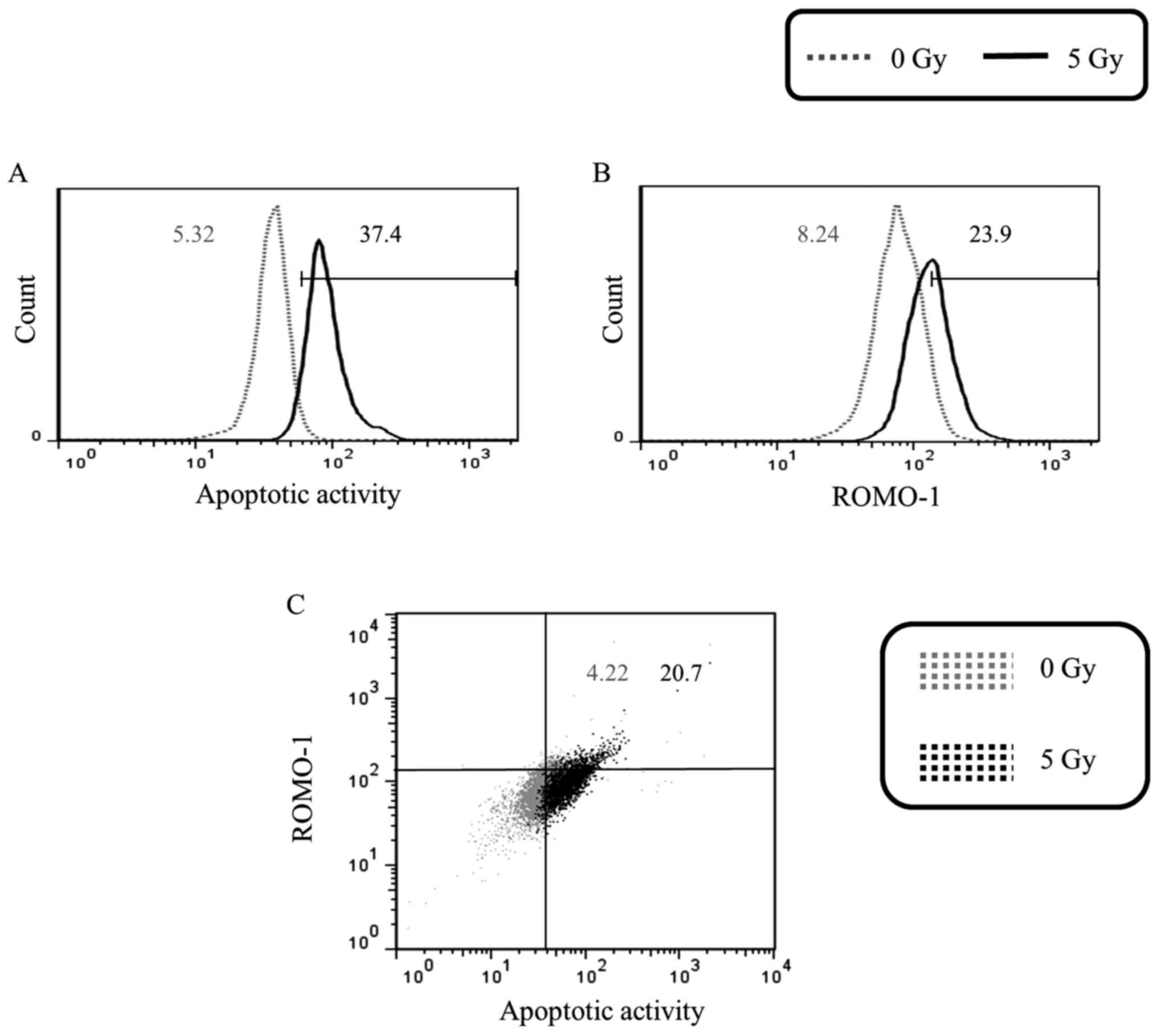
Subsequently, the reliability of ROS-related
apoptosis in X-ray irradiated HSC-3 cells in vitro was
studied. There was a correlation between the apoptotic activity and
the expression of ROMO-1 in the cells irradiated with 5.0 Gy X-rays
(Fig. 2).
Transcutaneous CO2 enhances
the effect of RT on OSCC tumor growth with no observable
side-effects in vivo
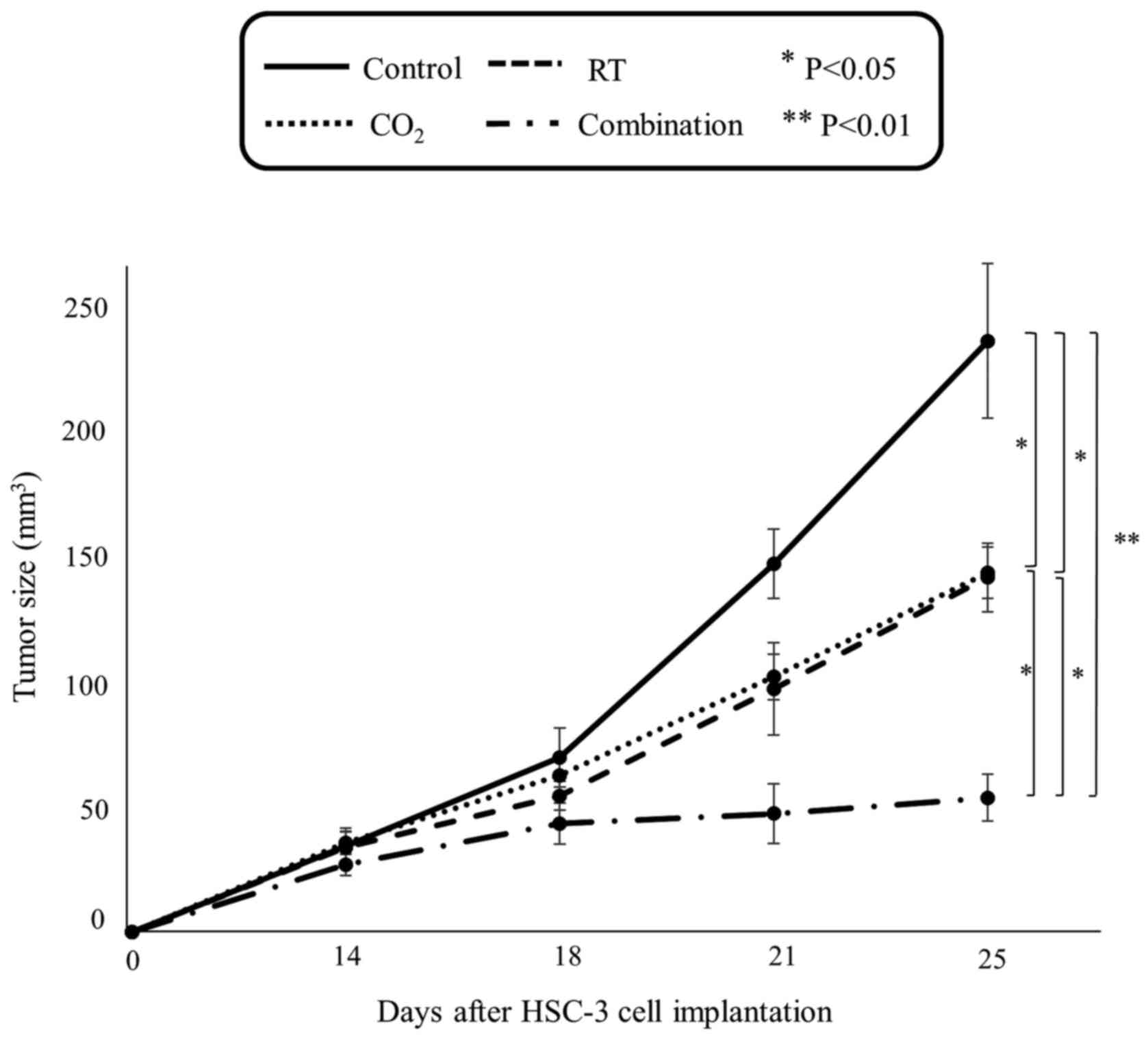
The effect of the transcutaneous CO2
therapy on RT was investigated in vivo. Tumor volume in the
combination group significantly decreased compared with that in the
control group (P<0.01), in the RT group (P<0.05) and in the
CO2 group (P<0.05). At the end of the experiment,
tumor volume in the combination group was reduced to 23, 38 and 37%
of that in the control, RT, and CO2 groups, respectively
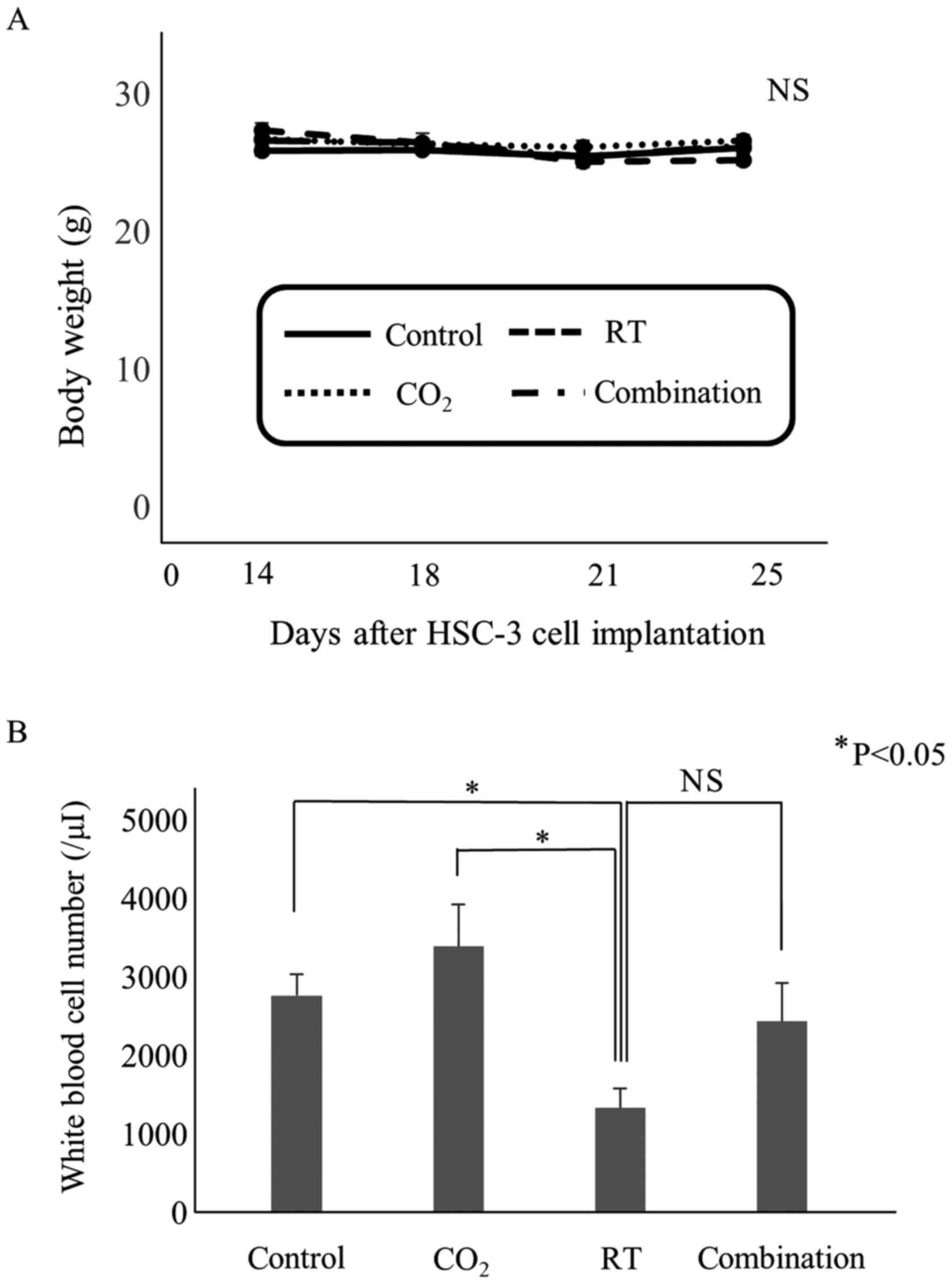
(Fig. 3). In addition, significant
decrease in tumor volume was observed in the CO2 and the
RT groups compared with the control group (P<0.05). No
significant difference in body weight was observed among the four
groups (Fig. 4A), however the white
blood cell number in the RT group was significantly decreased
compared with that in the control and the CO2 group
(Fig. 4B).
Transcutaneous CO2 with RT
suppresses tumor growth by inducing apoptosis and ROS production in
HSC-3 cells in vivo
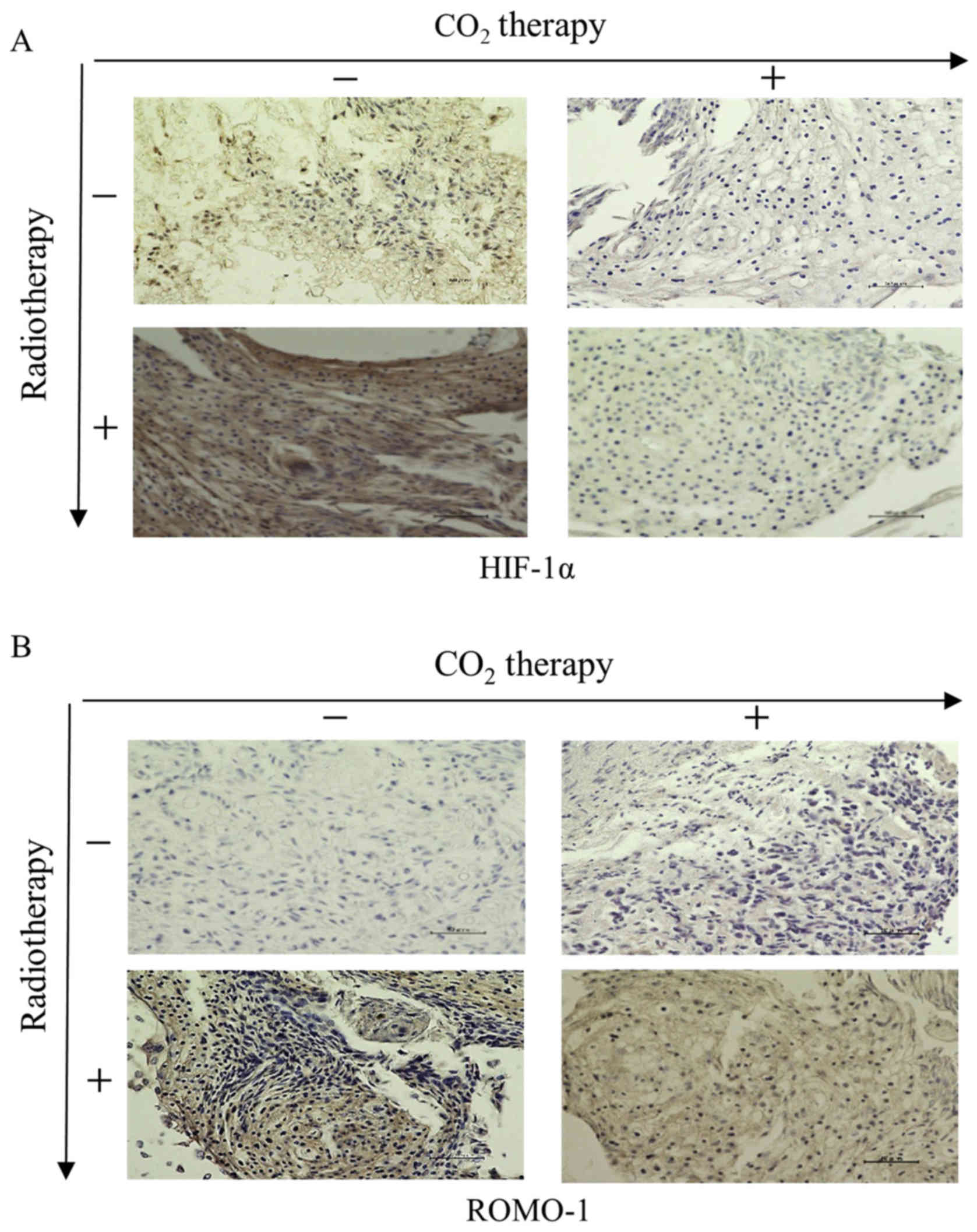
Subsequently, we examined the in vivo effects
of transcutaneous CO2 with RT on the expression of
HIF-1α, the apoptotic activity and the production of ROS in HSC-3
cells. Immunohistochemical positive staining for HIF-1α was hardly
detectable in the CO2 and the combination group compared
with the other two groups (Fig.
5A). In contrast, positive staining for ROMO-1 (indicative of
ROS production) was significantly higher in the combination group
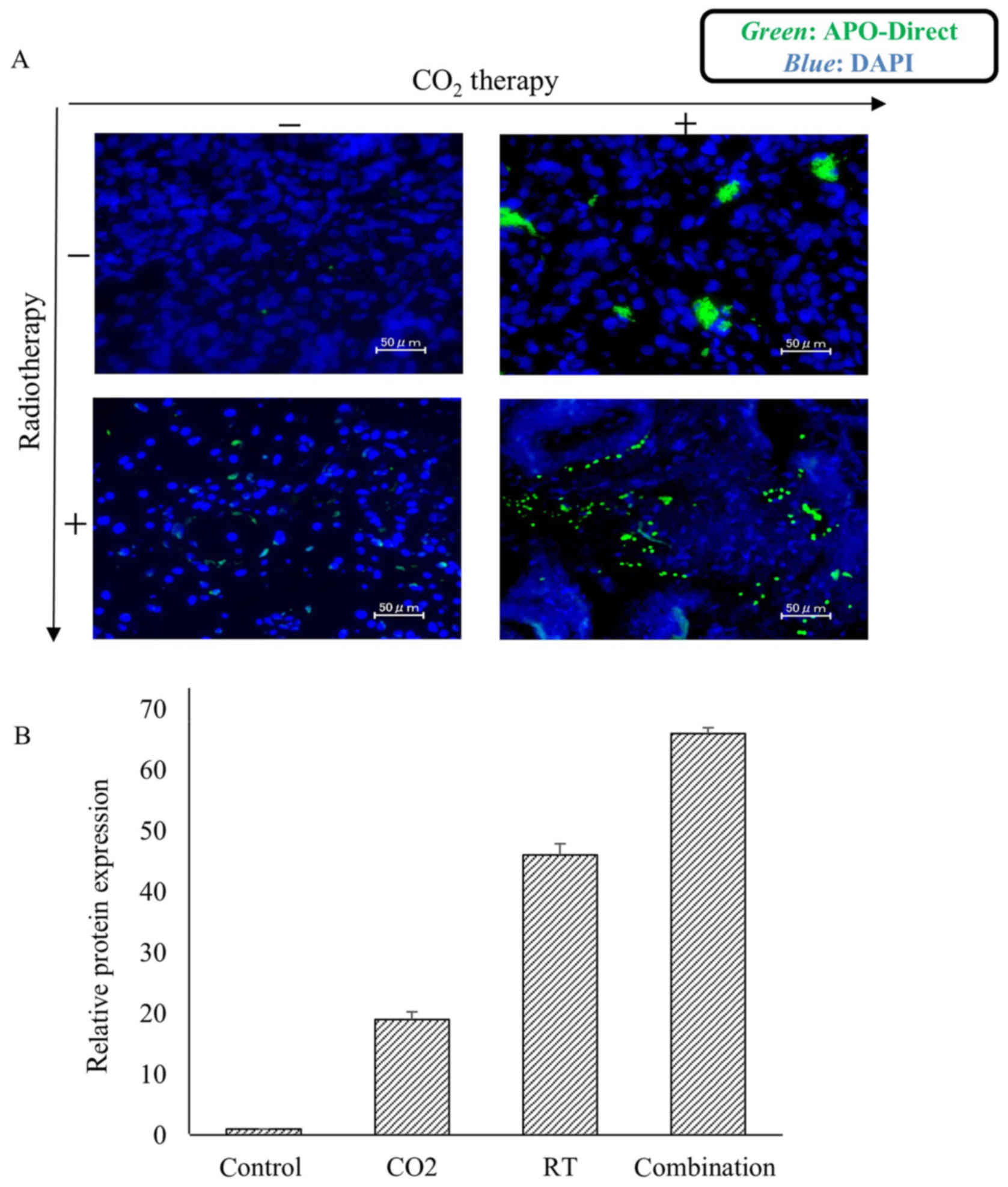
compared with that in the other three groups (Fig. 5B). Furthermore, immunofluorescence
staining revealed that apoptotic activity was increased in both the
CO2 and the combination groups (Fig. 6A). Quantitative analysis of the
immunofluorescence-positive staining revealed that apoptotic cells
were significantly increased. Relative positive staining compared
to the control was increased 19.0-, 46.0-, and 66.0-fold in the
CO2, RT and combination groups, respectively (Fig. 6B).
Immunoblot analysis revealed an
increased protein expression of the cleaved forms of caspase-3 and
PARP in the combination group compared with the other groups
(Fig. 7A)
The protein expression of cleaved caspase-8 was
increased in the RT and the combination group, compared with that
in the other two groups, whereas increased protein expression of
cleaved caspase-9 was observed in the CO2 and the
combination group (Fig. 7A).
Positive bands in the immunoblots were semi-quantified by
densitometric analysis based on the concentrations of α-tubulin:
caspase-3 (0.22, 0.62, 0.71, 0.89), caspase-8 (0.39, 0.41, 0.83,
0.93), caspase-9 (0.41, 0.79, 0.41, 1.00) and PARP (0.22, 0.53,
0.52, 0.93) in the control, CO2, RT and combination
group, respectively (Fig. 7B).
Discussion
RT is one of the main treatments for OSCC. However,
radioresistance is a recognized obstacle responsible for poor
clinical success and patient prognosis. Radioresistance of tumors
is caused by cell cycle, differentiation and hypoxia of which,
tumor hypoxia is known to demonstrate a strong correlation with
radioresistance (4–8). Hypoxia, characterized by an inadequate
supply of oxygen to the tissues, disturbs the radiolysis of
H2O and reduces the production of reactive and cytotoxic
species, and that radiation-induced DNA damage is fixed under
normoxic conditions (20,21).
Recent studies have revealed that HIF-1α plays a
major role in hypoxia-related tumor radioresistance (15). Under hypoxic conditions, HIF-1α in
tumor cells is activated; this activation promotes tumor growth. In
contrast, normoxic conditions induce the proteolysis of HIF-1α and
the loss of HIF-1α activity, which results in a dramatic decrease
in tumor growth, angiogenesis and cellular energy metabolism
(22).
RT results in tumor reoxygenation, upregulated
production of ROS and activation and stabilization of HIF-1α in
solid tumors, including OSCC (23).
The cytokines induced by HIF-1α activate anti-apoptotic signals to
tumor vessels, thereby imparting radioresistance to tumor cells
(24). Therefore, it stands to
reason that blocking either HIF-1α or these cytokines could
considerably increase the radiosensitivity of tumor vasculature,
thus causing a decreased overall tumor radioresistance (25–28).
Hence, resolving hypoxia via blocking the activation of HIF-1α may
prevent the development of radioresistance and improve the
prognosis of OSCC patients.
In support of this, several studies have revealed
the correlation between the survival rate and the value of hypoxia
in irradiated solid tumors, including OSCC (29–33).
Several strategies to address hypoxia have been explored, including
the use of radio-sensitizers and hypoxic cytotoxins (9). However, when used in combination,
these strategies resulted in a significant increase in the rate of
both severe radiation tissue injury and the chance of seizures
during therapy, presumably due to oxygen (O2) toxicity
(10,11). Strategies for improving hypoxia
employ 100% O2 or carbogen (95% O2 + 5%
CO2), involve direct inhalation and do not inflict any
toxicity (34). Breathing carbogen
in combination with nicotinamide administration was used to improve
the tumor response to accelerated RT in head-and-neck tumors
(35).
We have previously reported that a transcutaneous
CO2 system could combat hypoxia in treated tissues,
potentially resulting in an ‘artificial Bohr effect’ (16). We have also demonstrated that
transcutaneous CO2 induced mitochondrial apoptosis and
suppressed tumor growth in OSCC by resolving hypoxia (17) and decreasing the expression of
HIF-1α in OSCC. In light of these findings, we hypothesized that
transcutaneous CO2 could improve hypoxic conditions and
enhance the antitumor effect of RT on OSCC. CO2 was used
instead of O2 because O2 has an inferior
ability to dissolve in tissues and has no apoptotic action.
Antitumor effects did not arise when O2 was directly
used. Compared to carbogen, CO2 therapy is localized
because the tumor is covered directly with CO2 hydrogel
and the administered 100% CO2 gas.
In the present study, the combination therapy of
transcutaneous CO2 with RT decreased the expression of
HIF-1α and significantly suppressed in vivo OSCC tumor
growth compared with RT alone. The results indicated that
addressing hypoxia by transcutaneous CO2 could mitigate
intratumoral radioresistance.
Apoptosis plays an important role in determining the
cellular fate (36,37) and is mediated by two distinct cell
death pathways: the intrinsic and the extrinsic pathway. The
intrinsic cell death pathway is initiated by mitochondrial outer
membrane damage, followed by the release of cytochrome c
from the mitochondria into the cytoplasm, activation of an
initiator caspase, caspase-9, which activates the downstream
protein, caspase-3. The extrinsic cell death pathway is initiated
when a ligand binds to its receptor causing the activation of an
initiator caspase, caspase-8, which then activates the downstream
protein caspase-3. In both pathways, caspase-3 is responsible for
the cleavage of poly (ADP-ribose) polymerase (PARP) during cell
death (38–40). In the present study, the expression
of cleaved caspase-8 was observed in both the RT and the
combination groups, whereas cleaved caspase-9 was observed in both
the CO2 and the combination groups. These results
indicated that the effect of RT on OSCC results from the activation
of the death receptor-mediated pathway, whereas the effect of
transcutaneous CO2 occurs via the mitochondrial
apoptotic pathway. Furthermore, the combination therapy of
transcutaneous CO2 and RT demonstrated a strong
antitumor effect mediated by both the death receptor and the
mitochondrial apoptotic pathways.
In the present study, CO2 did not induce
significant oxidative stress but did induce obvious apoptosis. We
previously reported that transcutaneous CO2 inhibited
SCC tumor growth in vivo by increasing the number of
mitochondria and activating mitochondrial apoptosis by reducing
intratumoral hypoxia (17).
Mitochondria play important roles in cellular energy metabolism and
apoptosis. Mitochondria proliferate independently from cancer
cells, and the rates of cancer cell division and proliferation are
likely faster than those of mitochondria under hypoxic conditions
(41). Therefore, while cancer
cells exhibit abnormal proliferation, the number of mitochondria
decreases in cancer cells under hypoxic conditions, and
mitochondrial dysfunction (the Warburg effect) prevents apoptosis
in tumor tissue (42).
The antitumor effect of RT is also impacted by the
generation of ROS (43), through a
relationship that still requires further clarification. Radiation
generates ROS when it passes through biological systems. ROS are
very reactive, attack the critical cellular macromolecules such as
DNA, and lead to cell damage and death (44). ROS have an important function in
cell survival and cell death triggered by tumor necrosis factor-α
(TNF-α) signaling, and the main source of these ROS is the
mitochondria (45,46). Specifically, ROMO-1 is a
mitochondrial membrane protein responsible for TNF-α-induced ROS
production (47). ROMO-1 expression
is upregulated in most cancer cells and in senescent cells, and it
is induced by external stimuli (48). TNF-α treatment triggers the
interaction between TNF complex II and the C-terminus of ROMO-1
exposed to the outside of the mitochondrial outer membrane
(49). Simultaneously, ROMO-1
reduces the mitochondrial membrane potential, resulting in ROS
generation and apoptosis. Thus, the ROS level is significantly
increased by ROMO-1 overexpression. In the present study, we
observed a correlation between apoptotic activity and ROMO-1
expression in HSC-3 cells after X-ray irradiation in vitro,
indicating that RT could induce ROS-related apoptosis in human
HSC-3 cells. Additionally, the in vivo overexpression of
ROMO-1 was higher in the combination group than that in the RT
group. In summary, transcutaneous CO2 may not interfere
with ROS-related apoptosis.
In the present study, RT was performed in
vivo at the in vitro IC50 dose of 5.0 Gy.
Various studies have revealed that mice can be irradiated with
different doses (50–52). In addition, Fujii et al
reported that a single dose of radiation at 5.0 Gy rapidly
increased pO2 in SCC compared to other doses (53). Thus, we hypothesized that a
combination therapy with CO2 and 5.0 Gy
(IC50) would be effective in the present study. However,
it may be more appropriate to use a dose other than 5.0 Gy.
In conclusion, this is the first study to
demonstrate that transcutaneous CO2 enhanced the
antitumor effect of RT on OSCC by improving intratumoral hypoxia,
whilst eliciting no observable side-effects. Although further
studies are required, transcutaneous CO2 may be a novel
adjuvant therapy in combination with RT for OSCC.
Acknowledgements
We would like to thank Ms. Minako Nagata, Ms. Maya
Yasuda and Ms. Kyoko Tanaka for their expert technical
assistance.
Funding
No funding was received.
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
EI, TH, TU, DT, IS and TKa conceived and designed
the study. EI and TU performed the experiments. EI, TH and DT wrote
the paper. TU, TKa and RK reviewed and edited the manuscript. TA,
YS, RS, RK and TKo supervised all aspects of this study. All
authors read and approved the manuscript and agree to be
accountable for all aspects of the research in ensuring that the
accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
All animal experiments were performed in accordance
with the Guidelines for Animal Experimentation of Kobe University
Animal Experimentation Regulations (permission no. P120602) and
were approved by the Institutional Animal Care and Use
Committee.
Consent for publication
Not applicable.
Competing interests
The authors state that they have no competing
interests.
References
|
1
|
Harrison LB, Zelefsky MJ, Pfister DG,
Carper E, Raben A, Kraus DH, Strong EW, Rao A, Thaler H, Polyak T,
et al: Detailed quality of life assessment in patients treated with
primary radiotherapy for squamous cell cancer of the base of the
tongue. Head Neck. 19:169–175. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cooper JS, Fu K, Marks J and Silverman S:
Late effects of radiation therapy in the head and neck region. Int
J Radiat Oncol Biol Phys. 31:1141–1164. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Verastegui EL, Morales RB, Barrera-Franco
JL, Poitevin AC and Hadden J: Long-term immune dysfunction after
radiotherapy to the head and neck area. Int Immunopharmacol.
3:1093–1104. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hockel M, Schlenger K, Aral B, Mitze M,
Schaffer U and Vaupel P: Association between tumor hypoxia and
malignant progression in advanced cancer of the uterine cervix.
Cancer Res. 56:4509–4515. 1996.PubMed/NCBI
|
|
5
|
Chen XY, Wang Z, Li B, Zhang YJ and Li YY:
Pim-3 contributes to radioresistance through regulation of the cell
cycle and DNA damage repair in pancreatic cancer cells. Biochem
Biophys Res Commun. 473:296–302. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang S, Wang Z, Yang YU, Shi MO and Sun Z:
Overexpression of Ku80 correlates with aggressive
clinicopathological features and adverse prognosis in esophageal
squamous cell carcinoma. Oncol Lett. 10:2705–2712. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Koukourakis MI, Giatromanolaki A,
Danielidis V and Sivridis E: Hypoxia inducible factor (HIf1alpha
and HIF2alpha) and carbonic anhydrase 9 (CA9) expression and
response of head-neck cancer to hypofractionated and accelerated
radiotherapy. Int J Radiat Biol. 84:47–52. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Harrison LB, Chadha M, Hill RJ, Hu K and
Shasha D: Impact of tumor hypoxia and anemia on radiation therapy
outcomes. Oncologist. 7:492–508. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Moeller BJ, Richardson RA and Dewhirst MW:
Hypoxia and radiotherapy: Opportunities for improved outcomes in
cancer treatment. Cancer Metastasis Rev. 26:241–248. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bennett M, Feldmeier J, Smee R and Milross
C: Hyperbaric oxygenation for tumour sensitisation to radiotherapy.
Cochrane Database Syst Rev. 19:CD0050072005.
|
|
11
|
Henke M, Laszig R, Rübe C, Schäfer U,
Haase KD, Schilcher B, Mose S, Beer KT, Burger U, Dougherty C, et
al: Erythropoietin to treat head and neck cancer patients with
anaemia undergoing radiotherapy: Randomised, double-blind,
placebo-controlled trial. Lancet. 362:1255–1260. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Teppo S, Sundquist E, Vered M, Holappa H,
Parkkisenniemi J, Rinaldi T, Lehenkari P, Grenman R, Dayan D,
Risteli J, et al: The hypoxic tumor microenvironment regulates
invasion of aggressive oral carcinoma cells. Exp Cell Res.
319:376–389. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Maxwell PH, Dachs GU, Gleadle JM, Nicholls
LG, Harris AL, Stratford IJ, Hankinson O, Pugh CW and Ratcliffe PJ:
Hypoxia-inducible factor-1 modulates gene expression in solid
tumors and influences both angiogenesis and tumor growth. Proc Natl
Acad Sci USA. 94:8104–8109. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jing SW, Wang YD, Chen LQ, Sang MX, Zheng
MM, Sun GG, Liu Q, Cheng YJ and Yang CR: Hypoxia suppresses
E-cadherin and enhances matrix metalloproteinase-2 expression
favoring esophageal carcinoma migration and invasion via hypoxia
inducible factor-1 alpha activation. Dis Esophagus. 26:75–83. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moeller BJ and Dewhirst MW: HIF-1 and
tumour radiosensitivity. Br J Cancer. 95:1–5. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sakai Y, Miwa M, Oe K, Ueha T, Koh A,
Niikura T, Iwakura T, Lee SY, Tanaka M and Kurosaka M: A novel
system for transcutaneous application of carbon dioxide causing an
‘artificial Bohr effect’ in the human body. PLoS One. 6:e241372011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Takeda D, Hasegawa T, Ueha T, Imai Y,
Sakakibara A, Minoda M, Kawamoto T, Minamikawa T, Shibuya Y, Akisue
T, et al: Transcutaneous carbon dioxide induces mitochondrial
apoptosis and suppresses metastasis of oral squamous cell carcinoma
in vivo. PLoS One. 9:e1005302014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Matsui T, Ota T, Ueda Y, Tanino M and
Odashima S: Isolation of a highly metastatic cell line to lymph
node in human oral squamous cell carcinoma by orthotopic
implantation in nude mice. Oral Oncol. 34:253–256. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Iwata E, Hasegawa T, Takeda D, Ueha T,
Kawamoto T, Akisue T, Sakai Y and Komori T: Transcutaneous carbon
dioxide suppresses epithelial-mesenchymal transition in oral
squamous cell carcinoma. Int J Oncol. 48:1493–1498. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Thomlinson RH and Gray LH: The
histological structure of some human lung cancers and the possible
implications for radiotherapy. Br J Cancer. 9:539–549. 1955.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Brown JM and Wilson WR: Exploiting tumour
hypoxia in cancer treatment. Nat Rev Cancer. 4:437–447. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ryan HE, Poloni M, McNulty W, Elson D,
Gassmann M, Arbeit JM and Johnson RS: Hypoxia-inducible factor-1α
is a positive factor in solid tumor growth. Cancer Res.
60:4010–4015. 2000.PubMed/NCBI
|
|
23
|
Harada H, Itasaka S, Zhu Y, Zeng L, Xie X,
Morinibu A, Shinomiya K and Hiraoka M: Treatment regimen determines
whether an HIF-1 inhibitor enhances or inhibits the effect of
radiation therapy. Br J Cancer. 100:747–757. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Geng L, Donnelly E, McMahon G, Lin PC,
Sierra-Rivera E, Oshinka H and Hallahan DE: Inhibition of vascular
endothelial growth factor receptor signaling leads to reversal of
tumor resistance to radiotherapy. Cancer Res. 61:2413–2419.
2001.PubMed/NCBI
|
|
25
|
Hess C, Vuong V, Hegyi I, Riesterer O,
Wood J, Fabbro D, Glanzmann C, Bodis S and Pruschy M: Effect of
VEGF receptor inhibitor PTK787/ZK222584 [correction of ZK222548]
combined with ionizing radiation on endothelial cells and tumour
growth. Br J Cancer. 85:2010–2016. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kozin SV, Boucher Y, Hicklin DJ, Bohlen P,
Jain RK and Suit HD: Vascular endothelial growth factor
receptor-2-blocking antibody potentiates radiation-induced
long-term control of human tumor xenografts. Cancer Res. 61:39–44.
2001.PubMed/NCBI
|
|
27
|
Lund EL, Bastholm L and Kristjansen PE:
Therapeutic synergy of TNP-470 and ionizing radiation: Effects on
tumor growth, vessel morphology, and angiogenesis in human
glioblastoma multiforme xenografts. Clin Cancer Res. 6:971–978.
2000.PubMed/NCBI
|
|
28
|
Ning S, Laird D, Cherrington JM and Knox
SJ: The antiangiogenic agents SU5416 and SU6668 increase the
antitumor effects of fractionated irradiation. Radiat Res.
157:45–51. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dunst J, Stadler P, Becker A,
Lautenschläger C, Pelz T, Hänsgen G, Molls M and Kuhnt T: Tumor
volume and tumor hypoxia in head and neck cancers. The amount of
the hypoxic volume is important. Strahlenther Onkol. 179:521–526.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Nordsmark M and Overgaard J: A
confirmatory prognostic study on oxygenation status and
loco-regional control in advanced head and neck squamous cell
carcinoma treated by radiation therapy. Radiother Oncol. 57:39–43.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Stadler P, Becker A, Feldmann HJ, Hänsgen
G, Dunst J, Würschmidt F and Molls M: Influence of the hypoxic
subvolume on the survival of patients with head and neck cancer.
Int J Radiat Oncol Biol Phys. 44:749–754. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nordsmark M, Overgaard M and Overgaard J:
Pretreatment oxygenation predicts radiation response in advanced
squamous cell carcinoma of the head and neck. Radiother Oncol.
41:31–39. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nordsmark M, Bentzen SM, Rudat V, Brizel
D, Lartigau E, Stadler P, Becker A, Adam M, Molls M, Dunst J, et
al: Prognostic value of tumor oxygenation in 397 head and neck
tumors after primary radiation therapy. An international
multi-center study. Radiother Oncol. 77:18–24. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Overgaard J and Horsman MR: Modification
of hypoxia-induced radioresistance in tumors by the use of oxygen
and sensitizers. Semin Radiat Oncol. 6:10–21. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Saunders MI, Hoskin PJ, Pigott K, Powell
ME, Goodchild K, Dische S, Denekamp J, Stratford MR, Dennis MF and
Rojas AM: Accelerated radiotherapy, carbogen and nicotinamide
(ARCON) in locally advanced head and neck cancer: A feasibility
study. Radiother Oncol. 45:159–166. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Fan TJ, Han LH, Cong RS and Liang J:
Caspase family proteases and apoptosis. Acta Biochim Biophys Sin
(Shanghai). 37:719–727. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bosch M, Poulter NS, Vatovec S and
Franklin-Tong VE: Initiation of programmed cell death in
self-incompatibility: Role for cytoskeleton modifications and
several caspase-like activities. Mol Plant. 1:879–887. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kuwana T and Newmeyer DD: Bcl-2-family
proteins and the role of mitochondria in apoptosis. Curr Opin Cell
Biol. 15:691–699. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Sharpe JC, Arnoult D and Youle RJ: Control
of mitochondrial permeability by Bcl-2 family members. Biochim
Biophys Acta. 1644:107–113. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Festjens N, van Gurp M, van Loo G, Saelens
X and Vandenabeele P: Bcl-2 family members as sentinels of cellular
integrity and role of mitochondrial intermembrane space proteins in
apoptotic cell death. Acta Haematol. 111:7–27. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sagan L: On the origin of mitosing cells.
J Theor Biol. 14:255–274. 1967. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Graeber TG, Osmanian C, Jacks T, Housman
DE, Koch CJ, Lowe SW and Giaccia AJ: Hypoxia-mediated selection of
cells with diminished apoptotic potential in solid tumours. Nature.
379:88–91. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Prasad S, Gupta SC and Tyagi AK: Reactive
oxygen species (ROS) and cancer: Role of antioxidative
nutraceuticals. Cancer Lett. 387:95–105. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Jing L, He MT, Chang Y, Mehta SL, He QP,
Zhang JZ and Li PA: Coenzyme Q10 protects astrocytes from
ROS-induced damage through inhibition of mitochondria-mediated cell
death pathway. Int J Biol Sci. 11:59–66. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lo YY and Cruz TF: Involvement of reactive
oxygen species in cytokine and growth factor induction of c-fos
expression in chondrocytes. J Biol Chem. 270:11727–11730. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Locksley RM, Killeen N and Lenardo MJ: The
TNF and TNF receptor superfamilies: Integrating mammalian biology.
Cell. 104:487–501. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Chung YM, Lee SB, Kim HJ, Park SH, Kim JJ,
Chung JS and Yoo YD: Replicative senescence induced by
Romo1-derived reactive oxygen species. J Biol Chem.
283:33763–33771. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Kim JJ, Lee SB, Park JK and Yoo YD:
TNF-alpha-induced ROS production triggering apoptosis is directly
linked to Romo1 and Bcl-X(L). Cell Death Differ. 17:1420–1434.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Lee SB, Kim JJ, Kim TW, Kim BS, Lee MS and
Yoo YD: Serum deprivation-induced reactive oxygen species
production is mediated by Romo1. Apoptosis. 15:204–218. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zheng C, Cotrim AP, Rowzee A, Swaim W,
Sowers A, Mitchell JB and Baum BJ: Prevention of radiation-induced
salivary hypofunction following hKGF gene delivery to murine
submandibular glands. Clin Cancer Res. 17:2842–2851. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Harada K, Ferdous T and Yoshida H:
Investigation of optimal schedule of concurrent radiotherapy with
S-1 for oral squamous cell carcinoma. Oncol Rep. 18:1077–1083.
2007.PubMed/NCBI
|
|
52
|
Chiang IT, Liu YC, Hsu FT, Chien YC, Kao
CH, Lin WJ, Chung JG and Hwang JJ: Curcumin synergistically
enhances the radiosensitivity of human oral squamous cell carcinoma
via suppression of radiation-induced NF-κB activity. Oncol Rep.
31:1729–1737. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Fujii H, Sakata K, Katsumata Y, Sato R,
Kinouchi M, Someya M, Masunaga S, Hareyama M, Swartz HM and Hirata
H: Tissue oxygenation in a murine SCC VII tumor after X-ray
irradiation as determined by EPR spectroscopy. Radiother Oncol.
86:354–360. 2008. View Article : Google Scholar : PubMed/NCBI
|