Introduction
Melanoma is the most lethal form of skin cancer.
Among all malignancies, the incidence of melanoma has exhibited the
most rapid increase in the Caucasian population, apart from lung
cancer in women (1). It is
estimated that 68,130 new cases of cutaneous melanoma will be
diagnosed, and 8,700 patients will die from melanoma in the US in
2010 (2).
Malignant melanoma is associated with very high
mortality rates, particularly in cases of advanced disease.
Patients with metastatic melanoma have an extremely poor prognosis
(3). Therefore, the accurate
prediction of melanoma metastasis and patient outcome is essential
for the selection of the best therapeutic strategy and to improve
patient survival. One way to improve prognostic assessment is the
use of molecular biomarkers. Previously we investigated the
expression of ten biomarkers (Bim, BRG1, BRMS1, CTHRC1, ING4, NQO1,
NF-κB-p50, PUMA, SNF5 and SOX4) in melanomas; most were found to be
important for melanoma prognosis (4–13).
Here, we analyzed the expression of these ten biomarkers in 73
primary melanoma cases and 45 metastatic melanomas. We then
compared the expression of these biomarkers between AJCC I–II
stages (without metastasis) and AJCC III–IV stages (with
metastasis) melanomas. We also compared the capability of each
individual biomarker or combined biomarker system to predict
patient outcome. Our data revealed that the 6-biomarker (Bim,
BRMS1, ING4, NQO1, PUMA and SOX4) system delivers more accurate
prognosis for melanoma patients than any individual biomarker.
Materials and methods
Ethics statement
The use of human skin tissues and the waiver of
patient consent in this study were specifically approved by the
Clinical Research Ethics Board of the University of British
Columbia.
Study population
Formalin-fixed and paraffin-embedded biopsies were
obtained from the 1990–1998 archives of the Department of Pathology
at Vancouver General Hospital. A total of 73 primary melanomas and
45 metastatic melanomas were successfully evaluated for staining of
all of the ten biomarkers. Clinicopathological data were available
for all melanoma cases.
Re-evaluation of expression of each
biomarker
The expression of the ten biomarkers was previously
examined using tissue microarray (TMA) and immunohistochemistry
(IHC). The detailed methodology for the TMA construction and
staining for these biomarkers were previously reported (4–13).
Information concerning the antibodies used in these studies is
listed in Table I. We collected
the raw readings for each individual biomarker and re-grouped the
staining intensity and percentage of positive staining cells
uniformly in this study. Staining intensity was defined as 0
(negative), 1 (weak), 2 (moderate) and 3 (strong), and the
percentage of positive staining was scored according to 3
categories: 1 (0–33%), 2 (34–67%) and 3 (68–100%). The level of
staining of each biomarker was finally evaluated by the
immunoreactive score (IRS; 14), which was calculated by multiplying
the score of the staining intensity by that of the percentage of
positive cells. The IRS was then applied to the statistical
analysis of the expression variation among the various stages of
melanocytic lesions or the various subgroups directly.
 | Table I.Antibodies for the ten biomarkers
studied. |
Table I.
Antibodies for the ten biomarkers
studied.
| Biomarker | Full name | Supplier | Clone |
|---|
| Bim | BCL2-like 11 | NeoMarkers | Polyclonal |
| BRG1 | SWI/SNF related,
matrix-associated, actin dependent regulator of chromatin,
subfamily a, member 4 | Santa Cruz | Polyclonal |
| BRMS1 | Breast cancer
metastasis suppressor 1 | Donationa | Monoclonal |
| CTHRC1 | Collagen triple helix
repeat containing 1 | Immunochem | Polyclonal |
| ING4 | Inhibitor of growth
family, member 4 | ProteinTech | Polyclonal |
| NQO1 | NAD(P)H
dehydrogenase, quinone 1 | Santa Cruz | Monoclonal |
| p50 | Nuclear factor of κ
light polypeptide gene enhancer in B-cells 1 | Santa Cruz | Polyclonal |
| PUMA | BCL2 binding
component 3 | Imgenex | Polyclonal |
| SNF5 | SWI/SNF related,
matrix-associated, actin-dependent regulator of chromatin,
subfamily b, member 1 | Abcam | Monoclonal |
| SOX4 | SRY (sex determining
region Y)-box 4 | Abcam | Polyclonal |
Calculating the index score for multiple
biomarkers
To assess the value of the multiple biomarkers in
melanoma prognosis, the index score was calculated for the multiple
biomarkers. The expression levels of the 6 biomarkers, Bim, BRMS1,
ING4, NQO1, PUMA and SOX4, were all higher in the primary stage
(AJCC I and II) than in the advanced stage (AJCC III and IV)
melanomas. Thus, the final index score was the sum of the IRS of
all six biomarkers. For the survival analysis using the 6-biomarker
system, the final index score was grouped into two categories: the
low score group (0–16) and the high score group (17–48).
Statistical analysis
Graphpad PRISM version 5.0 and INSTAT 3 software
(Graphpad Software, La Jolla, CA, USA) were used to compare the
change in expression of each individual biomarker or the combined
multiple-biomarker system between various stages or subgroups. The
correlation coefficient (R) was calculated with λ correlation
statistical analysis. SPSS version 11.5 software (SPSS, Chicago,
IL, USA) was used for the statistical analysis for patient
survival. P<0.05 was considered statistically significant, and
all tests of statistical significance were two-sided.
Results
Clinicopathological features of the
melanoma biopsies
The clinicopathological features of all 118 melanoma
biopsies in this study are summarized as follows. Of the 73 primary
melanoma cases, 46 were men and 27 women, with ages ranging from 21
to 93 years (median, 59 years). In 47 cases, the tumors were
≤2.0-mm thick, while 26 tumors were >2.0 mm. Tumor ulceration
was present in 15 cases at diagnosis. Regarding the histological
subtype, there were 30 cases of superficial-spreading melanoma, 16
lentigo maligna melanomas, 10 nodular melanomas and another 17
unspecified cases. Sixteen melanomas were found in sun-exposed
sites, including the head and neck, while the other 57 were located
in sun-protected areas, including the arm, foot, leg and trunk.
Forty-five patients with melanoma metastases were included in this
analysis, 31 of which were men and 14 women, with ages ranging from
27 to 89 years (median, 60 years). AJCC criteria were also applied
to all the melanoma patients in this study. Among the 118 cases, 41
patients had stage I tumors, while 29 were stage II, 26 stage III
and 22 stage IV.
Six biomarkers are correlated with
melanoma metastasis
Various levels of staining were observed for each
biomarker in the various melanocytic lesions. We compared the
expression profile of all ten biomarkers in the AJCC I–II and AJCC
III–IV stage melanomas. Our data revealed that expression of the
six biomarkers, Bim, BRMS1, ING4, NQO1, PUMA and SOX4, was
significantly higher in the early stage (AJCC I–II) than in the
advanced stage (AJCC III–IV) cases, suggesting that these six
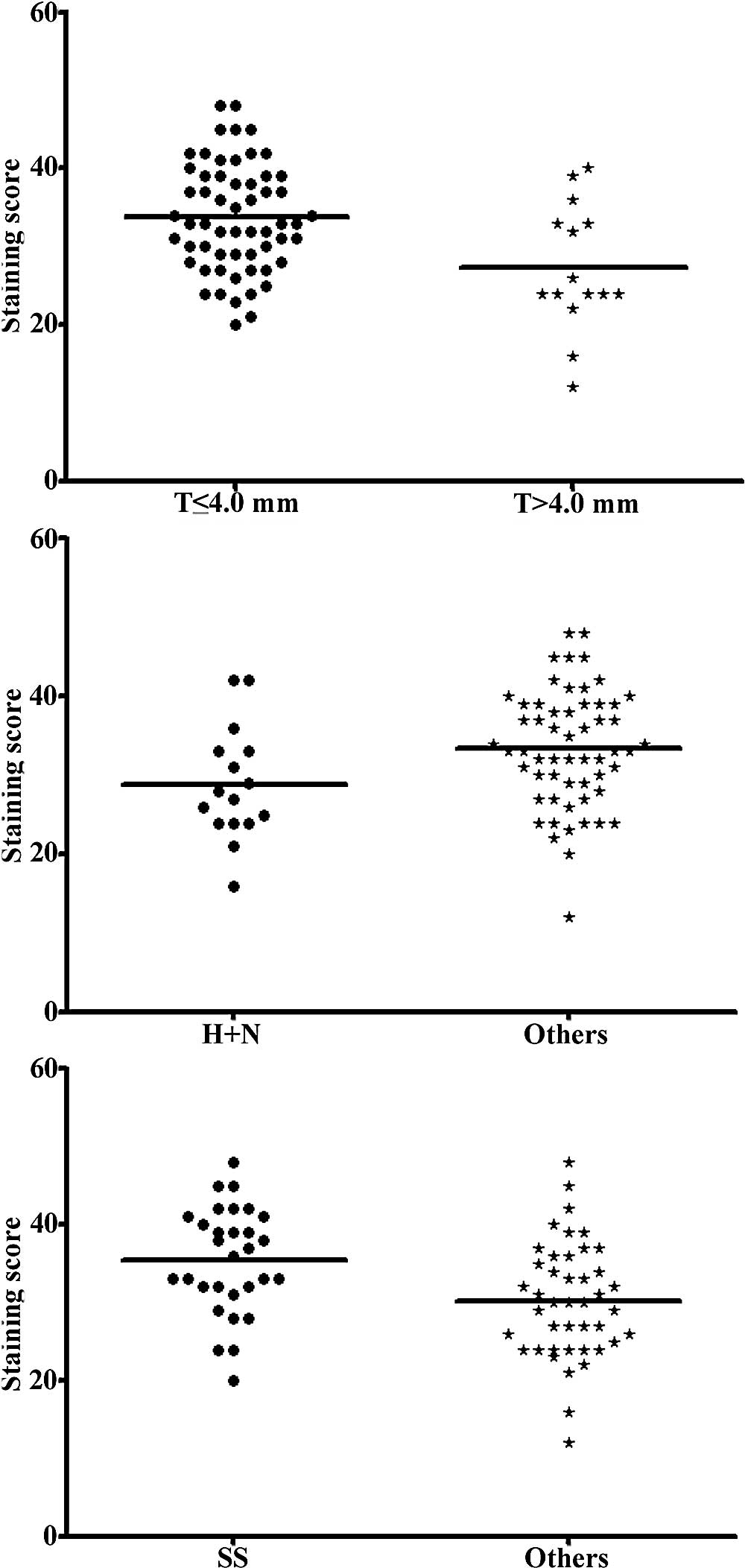
biomarkers are correlated with melanoma metastasis (Table II). We obtained the final index
score for the 6-biomarker system and performed the correlation
analysis. The correlation coefficients for Bim, BRMS1, ING4, NQO1,
PUMA and SOX4 were 0.333, 0.146, 0.188, 0.146, 0.05 and 0.208,
respectively, whereas this value reached 0.5 for the combined
6-biomarker system. Our data also revealed that a higher index
score (17–48) was correlated with tumors ≤4.0 mm thick,
sun-protected sites and superficial spreading melanomas (P=0.008,
0.030 and 0.003, respectively; Mann-Whitney test) (Fig. 1), but was not correlated with
patient age, gender and ulceration.
| Table II.Comparison of the expression of the
ten biomarkers between melanomas with and without metastasis. |
Table II.
Comparison of the expression of the
ten biomarkers between melanomas with and without metastasis.
| Biomarker | IRS mean value
| P-valuea |
|---|
| AJCC I–II (n=70) | AJCC III–IV
(n=48) |
|---|
| Bim | 5.30 | 2.83 | 0.0001 |
| BRMS1 | 5.99 | 4.45 | 0.0030 |
| BRG1 | 6.09 | 6.08 | 0.9253 |
| CTHRC1 | 6.00 | 6.75 | 0.1342 |
| ING4 | 5.86 | 4.75 | 0.0239 |
| NQO1 | 4.96 | 2.75 | 0.0008 |
| NF-κB-p50 | 4.84 | 5.71 | 0.1424 |
| PUMA | 4.89 | 4.19 | 0.0379 |
| SNF5 | 5.84 | 5.87 | 0.9430 |
| SOX4 | 5.77 | 4.35 | 0.0115 |
| 6-Biomarker
system | 26.99b | 18.98b | <0.0001 |
Six-biomarker system provides better
prognostic accuracy
Univariate Cox regression analysis revealed that
five biomarkers, Bim, BRMS1, ING4, NQO1 and PUMA, were all
significantly correlated with both overall and disease-specific
5-year survival in the 118 melanoma patients, while SOX4 was
correlated with disease-specific 5-year survival only. The relative
risk (RR) and P-value for each individual biomarker in the overall
survival analysis ranged from the lowest RR of 0.461 (P=0.003) for
ING4, to the highest RR of 0.626 (P=0.076) for SOX4. In
disease-specific survival analysis, the RR and P-value for
individual biomarkers ranged from the lowest RR of 0.408 (P=0.002)
for BRMS1, to the highest RR of 0.527 (P=0.029) for SOX 4. However,
when we combined these six biomarkers and performed this analysis,
we found that the RR was decreased to 0.273 and 0.222 for overall
and disease-specific survival (P=0.00001 and 0.000002),
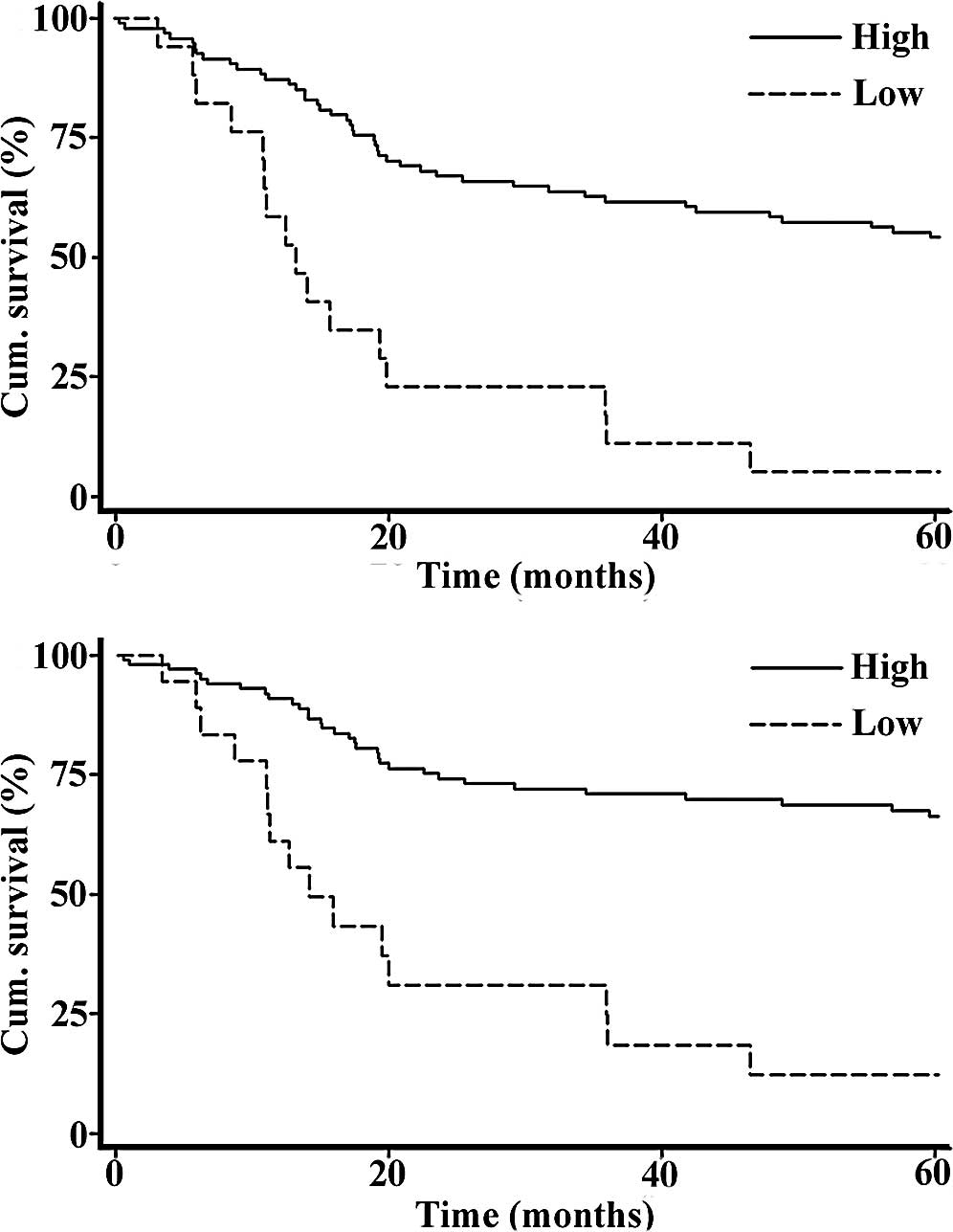
respectively (Table III). We then
constructed the Kaplan-Meier curve for all 118 melanoma patients,
and our data revealed that a high index score of the combined
6-biomarker system was significantly correlated with a more
favorable 5-year patient survival in both overall and
disease-specific survival analyses (P=0.0000 for both, log-rank
test) (Fig. 2). Moreover, a
multivariate Cox regression analysis indicated that a high index
score was an independent prognostic factor for both overall and
disease-specific 5-year survival (RR=0.237 and 0.208; 95% CI,
0.125–0.453 and 0.105–0.414; P=0.00001 and 0.000007, respectively)
(Table IV).
| Table III.Univariate Cox regression analysis of
individual and multiple biomarkers on 5-year patient survival in
the 118 melanoma cases. |
Table III.
Univariate Cox regression analysis of
individual and multiple biomarkers on 5-year patient survival in
the 118 melanoma cases.
| Biomarker | Overall survival
| Disease-specific
survival
|
|---|
| RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| Bim | 0.465 | 0.258–0.838 | 0.011 | 0.424 | 0.223–0.807 | 0.009 |
| BRMS1 | 0.575 | 0.343–0.965 | 0.036 | 0.408 | 0.230–0.723 | 0.002 |
| ING4 | 0.461 | 0.275–0.772 | 0.003 | 0.416 | 0.234–0.739 | 0.003 |
| NQO1 | 0.473 | 0.279–0.803 | 0.006 | 0.415 | 0.227–0.761 | 0.004 |
| PUMA | 0.514 | 0.304–0.868 | 0.013 | 0.421 | 0.230–0.770 | 0.005 |
| SOX4 | 0.626 | 0.373–1.049 | 0.076 | 0.527 | 0.297–0.935 | 0.029 |
| 6-Biomarkers | 0.273 | 0.152–0.490 |
1×10−5 | 0.222 | 0.119–0.415 |
2×10−6 |
| Table IV.Multivariate Cox regression analysis
of the 6-biomarker index score on 5-year patient survival in the
118 melanoma cases. |
Table IV.
Multivariate Cox regression analysis
of the 6-biomarker index score on 5-year patient survival in the
118 melanoma cases.
| Variablesa | Overall survival
| Disease-specific
survival
|
|---|
| RR | 95% CI | P-value | RR | 95% CI | P-value |
|---|
| Age | 0.574 | 0.337–0.979 | 0.042 | 0.838 | 0.457–1.535 | 0.567 |
| Gender | 1.111 | 0.635–1.943 | 0.713 | 0.976 | 0.523–1.822 | 0.940 |
| 6-Biomarkerb | 0.237 | 0.125–0.453 |
1×10−5 | 0.208 | 0.105–0.414 |
7×10−6 |
Discussion
Previous studies have revealed that numerous
biomarkers are valuable for melanoma prognosis (15). Here, we found that the expression
of six biomarkers, Bim, BRMS1, ING4, NQO1, PUMA and SOX4, differed
significantly between AJCC I–II and AJCC III–IV stage melanomas,
although the effect was limited for the individual biomarkers.
However, the 6-biomarker combination revealed a closer correlation
with melanoma metastasis and provided a better prognostic
accuracy.
The correlation between the expression of the six
biomarkers (Bim, BRMS1, ING4, NQO1, PUMA and SOX4) and melanoma
metastasis observed in this study is consistent with previous
findings. Bim was found to serve as a key factor in the regulation
of apoptosis by interacting with all Bcl-2 members (16), and the loss of Bim was found to be
critical for the pro-survival effect of mitogen-activated protein
kinase (MAPK) in melanoma. BRMS1 was reported to be a suppressor of
metastasis in various types of cancer by inhibiting the expression
of several metastasis-related genes (17–19).
We previously reported that ING4 inhibited melanoma cell migration
and invasion (7). In addition,
ING4 was found to promote the apoptosis of colorectal cancer cells
(20) and to suppress gliomas
tumor growth and angiogenesis (21), while NQO1 was found to enhance
apoptosis induced by β-lapachone treatment in prostate cancer cells
(22). Moreover, the loss of PUMA
was linked to deficient apoptosis and uncontrolled tumor cell
growth (23), which may finally
contribute to metastasis. SOX4 was reported to inhibit melanoma
cell migration and cell invasion (4) and was also found to be necessary for
the activation of p53 by stabilizing p53 and enhancing p53
acetylation under DNA damage stress (24). The function of these six biomarkers
in inducing apoptosis and inhibiting cell migration and invasion
also explains the correlation between the 6-biomarker index score
and tumor thickness.
We found that a low 6-biomarker index score was
correlated with primary melanomas located at sun-exposed sites.
This can be explained by the functions of these biomarkers in
apoptosis and DNA repair. Decreased expression of Bim, ING4, NQO1
and PUMA was found to result in reduced apoptosis (16,20,22,23,25),
thus leading to the inability to repair severe DNA damage caused by
UV. Furthermore, we previously revealed that NQO1 inhibits the
degradation of p33ING1b, which plays an important role in the
repair of UV-damaged DNA (26,27).
The reason for the correlation between a higher 6-biomarker index
score with superficial spreading melanoma is not known.
Statistical analysis demonstrated that the combined
6-biomarker index provided more accurate prediction of metastasis
than any of the individual biomarkers, which may be attributed to
the fact that these 6 biomarkers function to inhibit metastasis
through different processes, including the induction of apoptosis,
suppression of cell migration, invasion and angiogenesis, as well
as promotion of DNA repair. Thus, the combination of these six
biomarkers demonstrated a significant improvement in the predictive
accuracy for metastasis. Furthermore, this 6-biomarker index score
revealed an enhanced correlation with improved melanoma patient
survival compared to any single biomarker using univariate Cox
regression analysis, as metastasis is a major cause of melanoma
patient death. This 6-biomarker system is of great significance in
predicting melanoma metastasis and outcome, making it valuable in
clinical practice and the development of novel therapeutic targets
for human melanoma.
Acknowledgements
We thank Derek Dai, Hanyang Lin,
Alison Karst, Kai Gao, Yabin Cheng and Seyed Mehdi Jafarnejad for
the technical assistance and Dr Danny R. Welch for providing the
BRMS1 antibody.
References
|
1.
|
Howe HL, Wingo PA, Thun MJ, et al: Annual
report to the nation on the status of cancer (1973 through 1998),
featuring cancers with recent increasing trends. J Natl Cancer
Inst. 93:824–842. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
Statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar
|
|
3.
|
Jemal A, Thomas A, Murray T and Thun M:
Cancer statistics, 2002. CA Cancer J Clin. 52:23–47. 2002.
View Article : Google Scholar
|
|
4.
|
Jafarnejad SM, Wani AA, Martinka M and Li
G: Prognostic significance of Sox4 expression in human cutaneous
melanoma and its role in cell migration and invasion. Am J Pathol.
Oct 15–2010.(E-pub ahead of print).
|
|
5.
|
Dai DL, Wang Y, Liu M, Martinka M and Li
G: Bim expression is reduced in human cutaneous melanomas. J Invest
Dermatol. 128:403–407. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Tang L, Dai DL, Su M, Martinka M, Li G and
Zhou Y: Aberrant expression of collagen triple helix repeat
containing 1 in human solid cancers. Clin Cancer Res. 12:3716–3722.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
7.
|
Li J, Martinka M and Li G: Role of ING4 in
human melanoma cell migration, invasion and patient survival.
Carcinogenesis. 29:1373–1379. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Gao K, Dai DL, Martinka M and Li G:
Prognostic significance of nuclear factor-κB p105/p50 in human
melanoma and its role in cell migration. Cancer Res. 66:8382–8388.
2006.
|
|
9.
|
Karst AM, Dai DL, Martinka M and Li G:
PUMA expression is significantly reduced in human cutaneous
melanomas. Oncogene. 24:1111–1116. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Lin H, Wong RP, Martinka M and Li G: Loss
of SNF5 expression correlates with poor patient survival in
melanoma. Clin Cancer Res. 15:6404–6411. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Lin H, Wong RP, Martinka M and Li G: BRG1
expression is increased in human cutaneous melanoma. Br J Dermatol.
163:502–510. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Cheng Y, Li J, Martinka M and Li G: The
expression of NAD(P) H: quinone oxidoreductase 1 is increased along
with NF-κB p105/p50 in human cutaneous melanomas. Oncol Rep.
23:973–979. 2010.
|
|
13.
|
Li J, Cheng Y, Tai D, Martinka M, Welch DR
and Li G: Prognostic significance of BRMS1 expression in human
melanoma and its role in tumor angiogenesis. Oncogene. Oct
11–2010.(E–pub ahead of print).
|
|
14.
|
Remmele W and Stegner HE: Recommendation
for uniform definition of an immunoreactive score (IRS) for
immunohistochemical estrogen receptor detection (ER-ICA) in breast
cancer tissue. Pathologe. 8:138–140. 1987.PubMed/NCBI
|
|
15.
|
Torabian S and Kashani-Sabet M: Biomarkers
for melanoma. Curr Opin Oncol. 17:167–171. 2005. View Article : Google Scholar
|
|
16.
|
Chen L, Willis SN, Wei A, et al:
Differential targeting of prosurvival Bcl-2 proteins by their
BH3-only ligands allows complementary apoptotic function. Mol Cell.
17:393–403. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
17.
|
Vaidya KS, Harihar S, Phadke PA, et al:
Breast cancer metastasis suppressor-1 differentially modulates
growth factor signaling. J Biol Chem. 283:28354–28360. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18.
|
Hedley BD, Welch DR, Allan AL, et al:
Down-regulation of osteopontin contributes to metastasis
suppression by breast cancer metastasis suppressor 1. Int J Cancer.
123:526–534. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19.
|
Yang J, Zhang B, Lin Y, Yang Y, Liu X and
Lu F: Breast cancer metastasis suppressor 1 inhibits
SDF-1alpha-induced migration of non-small cell lung cancer by
decreasing CXCR4 expression. Cancer Lett. 269:46–56. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20.
|
Shiseki M, Nagashima M, Pedeux RM, et al:
p29ING4 and p28ING5 bind to p53 and p300, and enhance p53 activity.
Cancer Res. 63:2373–2378. 2003.PubMed/NCBI
|
|
21.
|
Garkavtsev I, Kozin SV, Chernova O, et al:
The candidate tumour suppressor protein ING4 regulates brain tumour
growth and angiogenesis. Nature. 428:328–332. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22.
|
Planchon SM, Pink JJ, Tagliarino C,
Bornmann WG, Varnes ME and Boothman DA: β-Lapachone-induced
apoptosis in human prostate cancer cells: involvement of NQO1/xip3.
Exp Cell Res. 267:95–106. 2001.
|
|
23.
|
Yu J and Zhang L: PUMA, a potent killer
with or without p53. Oncogene. 27(Suppl 1): S71–S83. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
24.
|
Pan X, Zhao J, Zhang WN, et al: Induction
of SOX4 by DNA damage is critical for p53 stabilization and
function. Proc Natl Acad Sci USA. 106:3788–3793. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25.
|
Li X, Zhang Q, Cai L, et al: Inhibitor of
growth 4 induces apoptosis in human lung adenocarcinoma cell line
A549 via Bcl-2 family proteins and mitochondria apoptosis pathway.
J Cancer Res Clin Oncol. 135:829–835. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26.
|
Garate M, Wong RP, Campos EI, Wang Y and
Li G: NAD(P)H quinone oxidoreductase 1 inhibits the proteasomal
degradation of the tumour suppressor p33(ING1b). EMBO Rep.
9:576–581. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27.
|
Li J, Wang Y, Wong RP and Li G: The role
of ING tumor suppressors in UV stress response and melanoma
progression. Curr Drug Targets. 10:455–464. 2009. View Article : Google Scholar : PubMed/NCBI
|