Contents
Introduction
Differential use of needle electrodes depending on
tumor diameter
Differential use of ablation methods with different
needle electrodes
When expandable needle electrodes cannot be used due
to tumor location
Selection of needle electrodes based on the
condition of the surrounding hepatic tissue
Conclusion
Introduction
First reported by Buscarini et al in 1992
(1) and Rossi et al in 1993
(2), radiofrequency ablation (RFA)
is an easy-to-operate and minimally invasive technique that
provides effective local treatment. Subsequently, Shiina et
al reported that, in cases with a small number (<3) of small
(<3 cm in diameter) hepatocellular carcinomas (HCC), RFA was
superior in terms of recurrence, and survival rates compared with
the conventional HCC treatments of percutaneous ethanol injection
therapy and surgical resection (3). As the rate of adverse events was
similar among the three methods, they advocated the use of RFA as a
first-line treatment for HCC (3).
Chen et al also investigated the recurrence and survival
rates of 180 patients with small HCC (<5 cm) who had been
randomly assigned to either RFA treatment or surgical resection
(4). They found no significant
differences in these rates between the two patient groups and thus
recommended RFA due to its minimal invasiveness.
RFA was introduced into our system at Toho
University Medical Center Omori Hospital in 1999, and we treat
nearly 200 HCC cases annually with RFA. Although individual medical
facilities use their own methods of RFA, we would like here to
share our experience of RFA treatment protocols.
Differential use of needle electrodes
depending on tumor diameter
Expandable LeVeen (Boston Scientific Corp., Natick,
MA, USA) and monopolar Cool-tip (Covidien, Boulder, CO, USA) needle
electrodes have been incorporated into our system since 1999 and
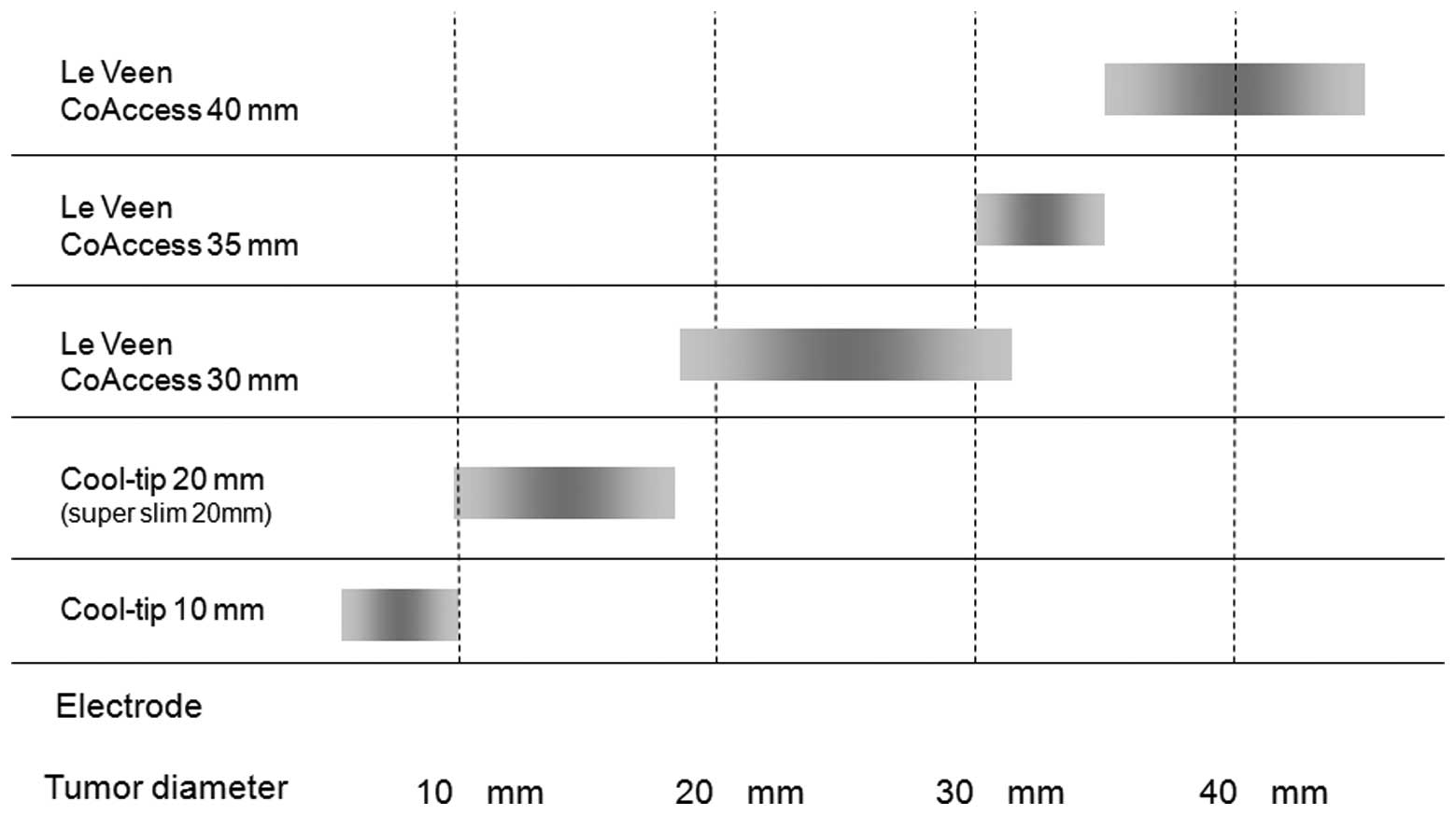
2002, respectively. Depending on tumor diameter, we perform RFA
using either a LeVeen needle with an array diameter of 20, 30, 35,
or 40 mm or a Cool-tip needle with a 10-mm or 20-mm non-insulated
tip. Regardless of tumor size, all patients receive a single RFA
treatment to avoid complications and dispersal of tumor cells due
to repeated needle puncture. This protocol also offers the benefit
of a shorter hospital stay. Bearing in mind the average ablative
diameters afforded by individual needle electrodes and the minimal
ablative margin of 5 mm or larger recommended by many studies
(5), we investigated whether tumor
size could serve as an indication for RFA. Based on the results, we
now select needle electrodes according to tumor size (Fig. 1).
Differential use of ablation methods with
different needle electrodes
Cool-tip needle with a 20-mm tip
We previously used the liver of dead swine to show
that the distance between the distal edge of ablation and the tip
of a Cool-tip needle electrode was ≤2 mm (6). Accordingly, when no vasculature is
present in the vicinity of HCC, we perform the following two-step
ablation method to ensure a sufficient ablative margin from the
needle tip and to avoid dispersal of tumor cells due to needle
puncture.
Two-step ablation method (Fig. 2)
Insert the needle electrode into the tumor, hold the
tip at the distal edge of the tumor, and turn the power on with the
initial output set to 40 W.
Increase the output by 10 W at 1-min intervals until
reaching 60 W. When power roll-off has occurred twice while
maintaining the output at 60 W, turn the power off.
Insert the electrode a further 5 mm, repeat the
above steps starting from 40 W, and end the treatment after
achieving a single roll-off at 60 W.
An ablative margin of 5 mm or larger will be ensured
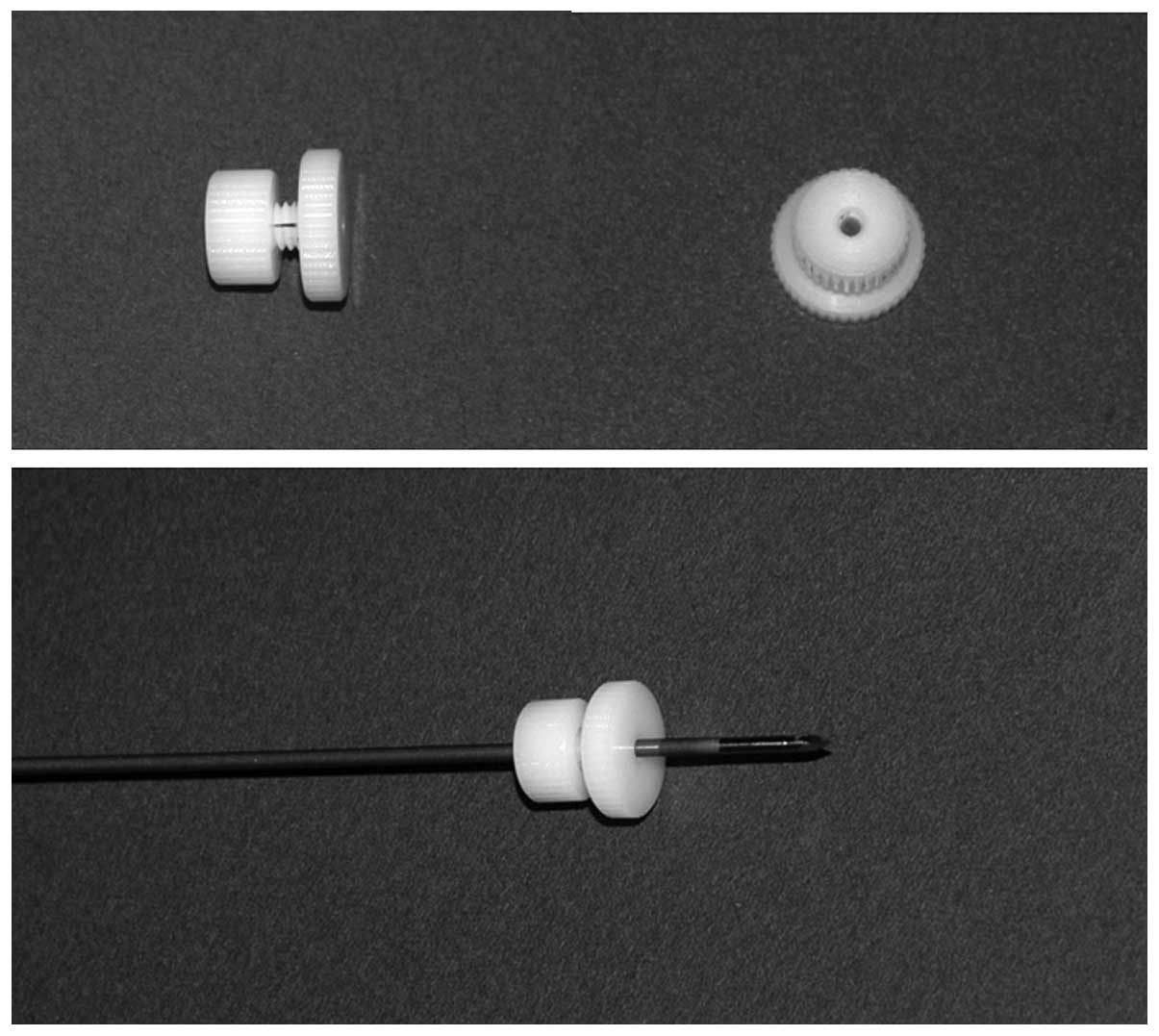
by advancing the tip further. A needle stopper made of Duracon for
percutaneous microwave coagulation therapy is used to ensure
accurate needle advancement (Fig.
3) (7). We perform RFA at low
power, starting from 40 W up to a maximum of 60 W, because, unlike
high-power ablation methods (8),
this method prevents complications and does not affect the rate of
local recurrence.
Fixed ablation method. If vasculature is
present in the vicinity of HCC, inserting a Cool-tip needle down to
the distal edge of tumor may result in vessel perforation. In such
cases we perform a different ablation method as follows:
Hold the tip of a needle electrode at the distal
edge of tumor and turn the power on with the initial output set at
40 W.
Increase the output by 10 W at 1-min intervals until
reaching 60 W. When power roll-off has occurred three times while
maintaining the output at 60 W, end the treatment.
Cool-tip needle with a 10-mm tip
A Cool-tip needle with a 10-mm non-insulated tip is
suitable for treating tumors with a diameter of <10 mm. It is
particularly useful in cases with reduced hepatic functional
reserve (7,9).
Hold the tip of a needle electrode at the distal
edge of the tumor and turn the power on with the initial output at
20 W.
Increase the output by 10 W at 1-min intervals until
reaching 30 W. When roll-off has occurred twice while maintaining
the output at 30 W, turn the power off.
Insert the electrode 5 mm further, repeat the above
steps starting from 20 W, and end the treatment after achieving a
single roll-off at 30 W.
(However, when vasculature is present in the
vicinity of HCC, perform the stationary ablation method described
above with the output starting at 20 W and perform treatment while
maintaining the output at 30 W).
LeVeen needle (Fig. 4)
With LeVeen needles, we perform the following steps
to avoid the dispersal of tumor cells:
Hold the tip of a needle electrode at the distal
edge of the tumor, partially deploy the tines, and apply the power
at the output initially set for the array diameter.
Increase the output by 10 W at 1-min intervals until
the power drops by 2 W, at which time maintain that output until
roll-off occurs.
Depending on the diameter of tumor, deploy the tines
in a stepwise fashion (in 2–4 steps) and apply the power in the
same way until the tines are fully deployed.
Continue to apply 70% of the maximum output at the
distal edge of tumor.
Depending on the diameter of tumor, retract the
electrode by approximately 5–10 mm, perform the same stepwise
ablation with full deployment, and end the treatment.
When expandable needle electrodes cannot be
used due to tumor location
When performing RFA of HCC in contact with a large
blood vessel (hepatic vein, hepatic portal vein) just below the
diaphragm and protruding from the distal surface of the liver, even
for tumor >20 mm in diameter, an expandable LeVeen needle may
perforate nearby vasculature of penetrate through the liver. In the
case of HCC >20 mm in diameter, our conventional method of RFA
using a Cool-tip needle with a 20-mm tip does not ensure a
sufficient ablative margin, and a similar problem has been reported
with the 30-mm tip (10).
Therefore, for HCC >20 mm in diameter, we divide a tumor equally
into three segments parallel to the direction of needle puncture.
We then perform two-step ablation of the segment on the right by
inserting a needle electrode into the distal end of the segment.
The same steps are repeated with the segment on the left. This
ensures an ablation of a wide area (11) and is useful in cases where the use
of a LeVeen needle is not recommended, such as those mentioned
above.
Selection of needle electrodes based on the
condition of the surrounding hepatic tissue
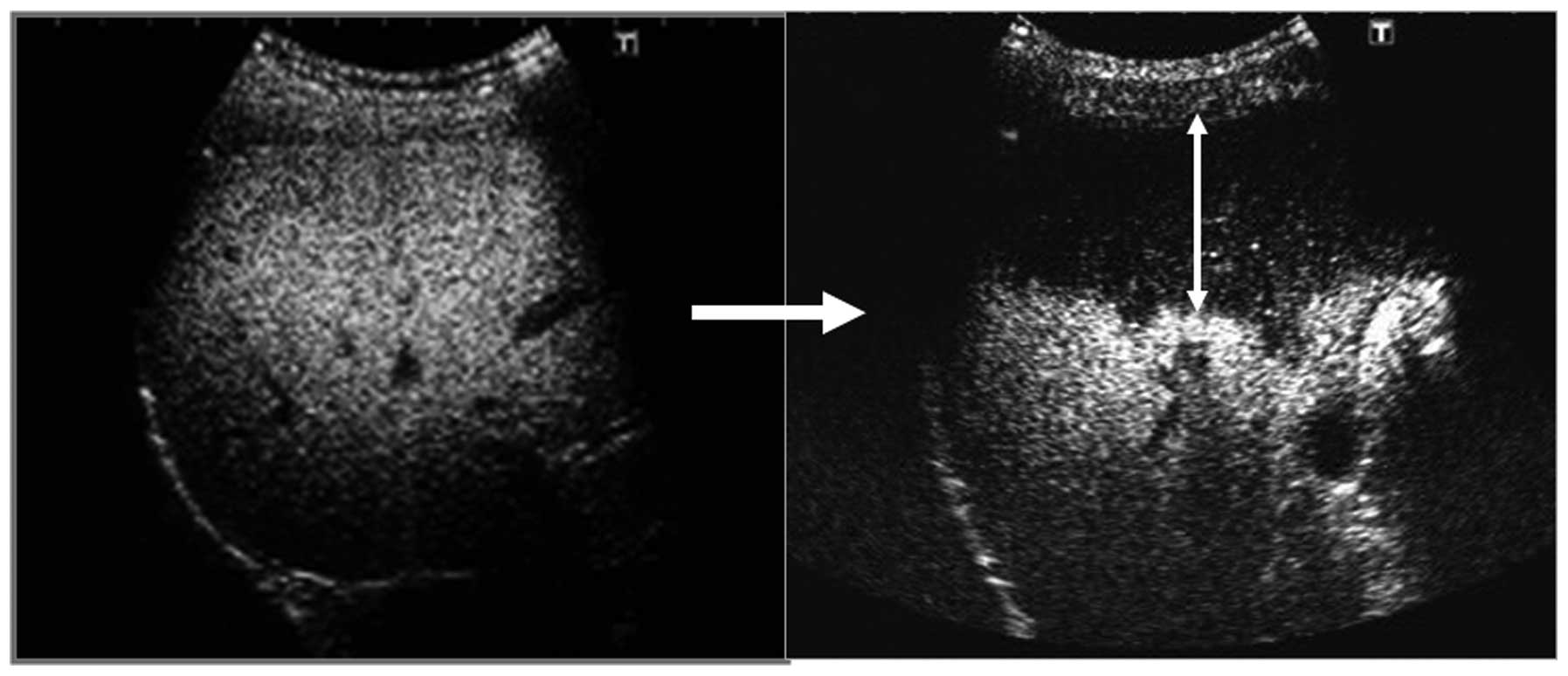
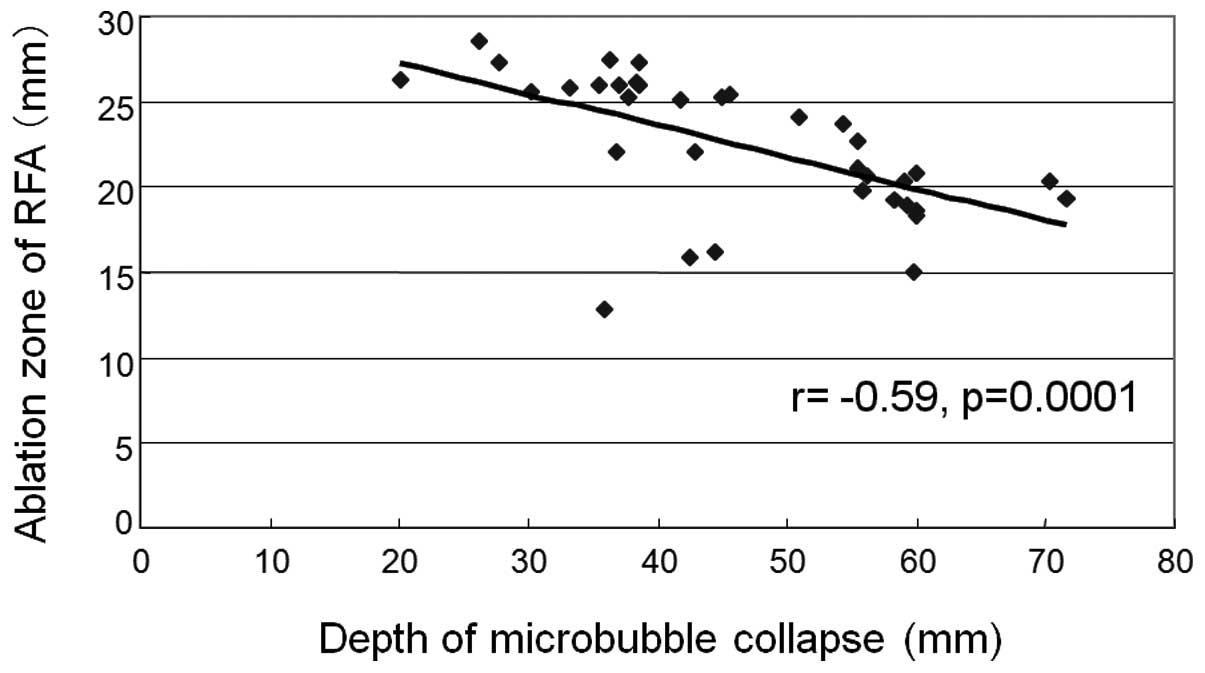
In some cases, RFA produces an unexpectedly small
ablative margin. We previously reported that individual differences
in ablative zone dimensions can be predicted by the depth of
microbubble collapse in the liver parenchyma in the Kupffer phase
of Sonazoid-enhanced ultrasonography (Fig. 5) (12). When an ablative zone is anticipated
to be small because ultrasonography findings show a large area of
microbubble collapse (Fig. 6), we
select an electrode that produces a wider area of ablation than
what we normally require to ensure a sufficient ablative
margin.
Conclusion
We described the ‘tips and tricks’ of RFA treatment
that we currently practice. It is our sincere hope that reporting
our experience with RFA protocols will promote safe and highly
effective performance of RFA treatment at all medical
facilities.
References
|
1
|
Buscarini L, Fornari F and Rossi S:
Interstitial radio-frequency hyperthermia in the treatment of small
hepatocellular carcinoma: percutaneous US guidance of electrode
needle. Ultraschall diagnostik 91. Anderegg A, Despland PA, Henner
H and Otto R: Springer-Verlag; Heidelberg: pp. 218–222. 1992
|
|
2
|
Rossi S, Di Stasi M and Buscarini E:
Percutaneous ultrasound-guided radiofrequency electrocautery for
the treatment of small hepatocellular carcinoma. J Interv Radiol.
8:97–103. 1993.
|
|
3
|
Shiina S, Teratani T, Obi S, et al: A
randomized controlled trial of radiofrequency ablation with ethanol
injection for small hepatocellular carcinoma. Gastroenterology.
129:122–130. 2005.
|
|
4
|
Chen MS, Li JQ, Zheng Y, et al: A
prospective randomized trial comparing percutaneous local ablative
therapy and partial hepatectomy for small hepatocellular carcinoma.
Ann Surg. 243:321–328. 2006.
|
|
5
|
Nakazawa T, Kokubu S, Shibuya A, et al:
Radiofrequency ablation of hepatocellular carcinoma: Correlation
between local tumor progression after ablation and ablative margin.
AJR Am J Roentgenol. 188:480–488. 2007.
|
|
6
|
Hagisawa Y, Shiozawa K, Takahashi M, et
al: Two-step radiofrequency ablation system by cool-tip electrode.
Jpn J Med Pharm Sci. 54:163–165. 2005.(In Japanese).
|
|
7
|
Wakui N, Iida K, Takayama R, et al:
Cool-tip 10-mm electrode useful for radiofrequency ablation of
hepatocellular carcinoma. Hepatogastroenterology. 56:1585–1591.
2009.
|
|
8
|
Ikehara T, Iida K, Wakui N, Watanabe M and
Sumino Y: Complications from radiofrequency ablation therapy for
hepatocellular carcinoma: be reduced by output adjustment of the
Cool-tip type RF ablation system? J Med Soc Toho. 55:298–305.
2008.(In Japanese).
|
|
9
|
Wakui N, Iida K, Ikehara T, et al:
Recurrence incidence of small HCC in cirrhosis patients by ablation
versus injection. Hepatogastroenterology. 57:195–201. 2010.
|
|
10
|
Yamasaki T, Kimura T, Kurokawa F, et al:
Percutaneous radiofrequency ablation with cooled electrodes
combined with hepatic arterial balloon occlusion in hepatocellular
carcinoma. J Gastroenterol. 40:171–178. 2005.
|
|
11
|
Takayama R, Iida K and Wakui N: Device
therapy for metastatic liver cancer of the radiofrequency ablation
treatment resistance. Jpn J Med Pharm Sci. 63:228–231. 2010.(In
Japanese).
|
|
12
|
Takahashi M, Iida K, Wakui N, Takayama R,
Shiozawa K and Sumino Y: Relationship between ablation zone of
radiofrequency ablation and length of microbubble collapse in the
post-vascular phase (Kupffer phase) of Sonazoid-enhanced
ultrasonography in patients with hepatocellular carcinoma. Jpn J
Med Ultrasonics. 38:637–646. 2011.(In Japanese with English
abstract).
|