Introduction
The incidence of pediatric urolithiasis is ∼1–4%,
with ∼40–50% of cases aged <5 years and >20% aged <2 years
(1). It has been reported that
there were 50,000 cases of pediatric urolithiasis, including 12,000
cases that were hospitalized and 4 cases that succumbed, due to
melamine-contaminated milk in China in 2008 (2–7).
These children were ∼1 year old with various clinical
manifestations. Due to multiple calculi in the kidney, obstructive
anuria, oliguria and dysuria appears, threatening the health of the
patients. Understanding such severe acute cases of pediatric
urolithiasis is of great importance for diagnosis and
treatment.
Metabolic diseases, chronic infection and urinary
tract malformations are the major cause of pediatric urolithasis,
particularly with metabolic disease and chronic infection (8). However, a large-scale pediatric
urolithasis outbreak in 2008 resulted from the ingestion of
melamine-contaminated infant formula milk. Melamine is a pure white
monoclinic crystalline substance. It is tasteless, slightly soluble
in cold water and weakly alkaline (pKb 8). It hydrolyzes in strong
acid or alkali solution. When cats were fed with increasing doses
of melamine-cyanuric acid, the cats developed renal failure, with
crystals in the kidneys (9,10).
This was also reported in a rat study by Dobson et
al(11). The melamine-cyanuric
acid compound has low solubility, which leads to the formation of
melamine cyanurate crystals in the kidney. It is considered that
melamine-cyanuric acid is absorbed in the digestive tract and
distributed to the whole body. It precipitates in the renal tubule
for unknown reasons, which leads to progressive obstruction and
degeneration (11).
Twenty-eight severe acute cases of pediatric
urolithiasis were analyzed in the present study. The use of
indwelling ureteral stent placement by cystoscopy, open surgery and
conservative treatments, including catheterization and diuretic,
anti-inflammatory and anti-spasmodic therapy, produced good
effects.
Materials and methods
General information
Twenty-eight cases of severe pediatric urolithiasis,
including 21 males and 7 females, were admitted to the Department
of Urology, Hunan Children’s Hospital. The average age was 13.9
months, ranging from 4 months to 3 years, with 17 infants and 11
toddlers. All patients had received melamine-contaminated infant
milk formula. Prior written informed consent was obtained from
parents of each child and the study was approved by the ethics
review board of the Hunan Children’s Hospital, Hunan, Changsha,
China.
All patients had acute onset of anuria, oliguria or
dysuria. There were another three patients who had multiple
symptoms, including kidney and ureter stones, unilateral ureteral
calculi and bladder calculi (Table
I). They were all in critical condition at admission with renal
dysfunction and electrolyte imbalance. Among them, 21 patients had
anuria (75%), two patients had oliguria (7.14%) and two patients
had dysuria (7.14%). A number of patients also had unexplained
fever, diarrhea, recurrent nausea and vomiting. Upper urinary tract
calculi mainly presented anuria, which accounted for 86.95%. Lower
urinary tract calculi mainly presented oliguria and dysuria, which
accounted for 80% (Table I). One
child had heart failure, severe infection and renal failure and two
patients had a coagulation function disorder, one of which was
disseminated intravascular coagulation (DIC).
 | Table ILocalization of stones and clinical
manifestations. |
Table I
Localization of stones and clinical
manifestations.
| Clinical
manifestations | Kidney and ureter
stones | Simple kidney
stones | Unilateral ureteral
calculi | Simple bilateral
ureteral calculi | Bladder calculi | Urinary tract
stones | Total |
|---|
| Anuria | 13 | 1 | 1 | 5 | 1 | 0 | 21 |
| Oliguria | 1 | 0 | 0 | 0 | 1 | 0 | 2 |
| Dysuria | 0 | 0 | 0 | 0 | 0 | 2 | 2 |
| Others | 1 | 0 | 1 | 0 | 1 | 0 | 3 |
| Total | 15 | 1 | 2 | 5 | 3 | 2 | 28 |
Localization of urolithiasis
There were 23 cases of upper urinary tract calculi,
of which five cases were simple ureteral stones, 15 cases were
ureteral stones and kidney stones, one case was simple kidney
stones and two cases were unilateral ureteral stones and
hydronephrosis. There were three cases with upper urinary tract
stones and bladder stones and two cases with urinary tract stones
(one case with anterior urethral stones and one case with posterior
urethral stones).
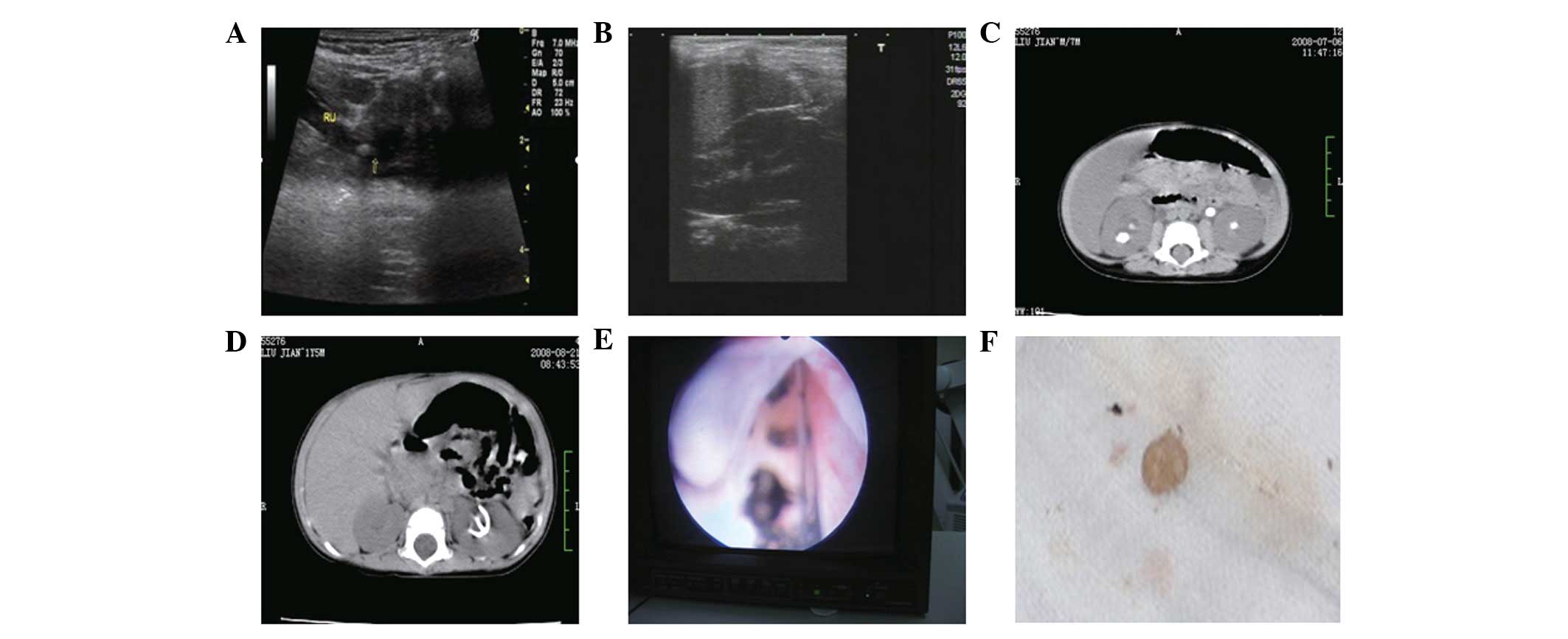
Imaging examination
All cases had calculi, as detected by ultrasound.
The majority of the stones affected the collecting system and
ureters. Ureteral stones were mainly in the uretero-pelvic
junction, the cross-iliac artery segment of the ureter and the
ureter-bladder junction. Stones accumulated as powder, involving a
large area. A light sound shadow was at the rear and a trailing
edge was detectable, which is different from calcium oxalate
stones. Stones obstructed the urinary tract (Figs. 1A and B). Computed tomography (CT)
examination further clarified the location of the stones,
hydronephrosis level and assessment of kidney function. There was
mild to moderate hydronephrosis, bilateral ureteral expansion or no
expansion, multiple kidney stones, multiple bilateral ureter with
different locations or stones obstructing the junction of the renal
pelvis and ureter, with no urine in the bladder (Figs. 1C and D).
Treatment
The 28 children were admitted to hospital for
examination of blood, liver, kidney and coagulation function, as
well as ultrasound and CT scan. For children with upper urinary
tract stones and anuria and oliguria, an indwelling ureteral stent
was inserted with the aid of a cystoscope (Fig. 1E). For children with urinary tract
stones, conservative treatment was applied. Stones in the urinary
tract were pushed into the bladder. For children with bladder
stones, conservative treatment or incision lithotripsy was
administered (Table II).
Postoperative examination was also performed.
| Table IILocalization of stones and related
treatment. |
Table II
Localization of stones and related
treatment.
| Related
treatment | Kidney and ureter
stones | Simple kidney
stones | Unilateral ureteral
calculi | Simple bilateral
ureteral calculi | Bladder calculi | Urinary tract
stones | Total |
|---|
| Cystoscopy | 12 | 0 | 1 | 3 | 1 | 0 | 17 |
| Open surgery | 1 | 0 | 1 | 1 | 1 | 1 | 5 |
| Cystoscopy + open
surgery | 1 | 0 | 0 | 1 | 0 | 0 | 2 |
| Conservative
treatment | 1 | 1 | 0 | 0 | 1 | 1 | 4 |
Statistical analysis
Data are expressed as mean ± standard error of the
mean (SEM). The significance was analyzed by SPSS 16.0 statistical
analysis software (SPSS Inc., Chicago, IL, USA) using one-way
analysis of variance (ANOVA), with an inspection level of
α=0.05.
Results
Outcomes of treatment
After the placement of a bilateral ureteral
indwelling epidural catheter or Double-J tube by cystoscopy, urine
was drained successfully in 17 cases (60.71%). Two days after
surgery, renal function was detected to be normal. With infusion
and antispasmodic treatments, stones were discharged in one week.
Five patients received open-surgical lithotomy (17.86%). Four
patients received catheterization and diuretic, anti-inflammatory
and antispasmodic therapy (14.28%). Two patients received
indwelling ureteral stent placement by cystoscopy and a second open
surgery (7.14%). The discharged stones were gray, gray-yellow or
white (Fig. 1F). The stones were
fragile and were easily crushed into a powder.
Renal function and electrolyte
recovery
Renal function and electrolytes were abnormal in 22
children. However, following indwelling ureteral stent placement by
cystoscopy, open surgery and conservative treatment, serum
potassium levels in the majority of cases returned to normal within
1 day. Creatinine and urea nitrogen levels in the majority of cases
returned to normal on the second day (Table III).
| Table IIIRenal function recovery following
treatment. |
Table III
Renal function recovery following
treatment.
| Time | Serum potassium
(mM) | BUN (mM) | Cr (μM) | CO2CP
(mM) |
|---|
| Before treatment | 5.22±0.25 | 18.86±1.95 | 390.2±27.7 | 18.74±0.68 |
| 1 day after
treatment | 4.38±0.23 | 12.00±1.43 | 185.2±23.3 | 19.66±0.93 |
| 2 days after
treatment | 3.79±0.16 | 7.00±1.13 | 107±17.1 | 20.02±0.58 |
| P-value | <0.001 | <0.001 | <0.001 | =0.46 |
Follow-up
When discharged from the hospital, pediatric
urolithiasis was not detectable in 23 cases. In the five cases with
residual stones, three cases had recurrence of urinary tract
obstruction and two cases underwent re-examination by ultrasound
one month after surgery, which identified kidney stones with
hydronephrosis. All patients were followed up for two years.
Discussion
In the 28 acute severe cases of pediatric
urolithiasis in the present study, all patients had a history of
contaminated milk and had no urinary tract abnormalities. The
contaminated milk feeding time varied from 3 months to 1 year. The
main complaint was anuria (75%) due to bilateral upper urinary
tract calculi obstruction. Other complaints were oliguria and
dysuria (14.28%). The onset of anuric renal dysfunction was acute
and severe. Children were in a critical condition with
hypertension, poor appetite and lack of energy, and internal
environment disturbance, with or without mild edema. However, the
anuria was temporary. Once the obstruction was relieved, urine was
discharged. In this study, 21 children had anuria and they all
discharged urine following indwelling ureteral stent placement by
cystoscopy, open surgery and conservative treatment. Their renal
dysfunction was prerenal and their kidney function recovered once
the urinary tract obstruction was removed. There were 22 children
with electrolyte disorders and their renal function and electrolyte
disorders were all recovered one or two days after urine drainage.
Nineteen of them underwent indwelling ureteral stent placement by
cystoscopy and three underwent open surgery and received
conservative treatment of urine alkalization following urine
drainage.
The clinical diagnosis of infant urolithiasis caused
by melamine relies on appropriate imaging examination. Ultrasound
is the first option (12).
Two-dimensional sonography provides location, size, shape, edge,
number, echo and rear sound shadow, which indicates the hardness
and degree of the loose structure, of the stones. It also shows the
scope, degree of hydronephrosis, renal parenchymal compression and
its internal structural changes. With the application of Doppler
ultrasound (US), renal blood flow and urine flow in the renal hilum
and ureter were observed in order to diagnose the obstruction.
Clinically, US diagnosis of urolithiasis is extremely sensitive. A
CT scan shows radioparentcalculus; however, it also aids the
differential diagnosis. CT and US are the first options for
urolithasis diagnosis. With US and CT scans, the locations of
stones and anatomical deformity are observed for future treatment
(13).
Non-open treatment is increasingly popular for
pediatric urolithiasis, particularly extracorporeal shock wave
lithotripsy (ESWL) and shock wave lithotripsy (SWL) (14,15).
Moreover, with the development of cavity urinary technology,
particularly fiber endoscopy, pneumatic lithotripsy is applied for
treatment of pediatric urolithiasis (16). However, melamine-induced
urolithiasis has its own characteristics: i) it easily causes
bilateral urinary tract obstruction; ii) following indwelling
ureteral stent placement by cystoscopy, urine discharges easily;
and iii) the stones are loose and friable and when urine is
drained, the stones self-discharge. In this study, indwelling
ureteral stent placement by cystoscopy was applied. The amount of
urine was recorded for 24 h and renal function and electrolytes
were examined repeatedly. Antispasmodic anisodamine (654-2), urine
alkalization, anti-infection and rehydration therapy were
administered. When the vital signs were stable, the ureteral stents
were removed. A CT scan was performed again to observe the amount
of urine and to determine if the stones had been expelled. A volume
of fluid and electrolytes was administered according to electrolyte
values. Conservative therapy with a diuretic, antibiotics and
rehydration was applied if the stones were small and the anuric
time was short. If the obstruction remained, open surgery was
performed. When the urine had been drained, the electrolyte levels
of the children returned to normal one day after surgery and renal
function recovered two days after surgery. It is essential that
electrolyte balance disorders and infection are prevented in the
polyuric period; therefore, children with preoperative concurrent
heart failure, severe infection or coagulation disorders, including
DIC, should be admitted to the intensive care unit (ICU) to get
through the postoperative infection, polyuric and coagulation
disorders or DIC periods.
In conclusion, pediatric urolithiasis caused by
melamine forms quickly and is acute. It mainly presents anuria,
oliguria and dysuria. CT and US are the first choice for diagnosis.
Indwelling ureteral stent placement by cystoscope causes minimal
injury and provides excellent results.
References
|
1.
|
Kamoun A, Daudon M, Abdelmoula J, et al:
Urolithiasis in Tunisian children: a study of 120 cases based on
stone composition. Pediatr Nephrol. 13:920–925. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Shang P, Chang H, Yue ZJ, Shi W, Zhang H,
Tang X, He Q and Wang W: Acute kidney injury caused by consumption
of melamine-contaminated infant formula in 47 children: a
multi-institutional experience in diagnosis, treatment and
follow-up. Urol Res. 40:293–298. 2012. View Article : Google Scholar
|
|
3.
|
Zhang X, Bai J, Ma P, Ma J, Wan J and
Jiang B: Melamine-induced infant urinary calculi: a report on 24
cases and a 1-year follow-up. Urol Res. 38:391–395. 2010.PubMed/NCBI
|
|
4.
|
Yang ZH, Zhang CM, Liu T, Lou XF, Chen ZJ
and Ye S: Continuous renal replacement therapy for patients with
acute kidney injury caused by melamine-related urolithiasis. World
J Pediatr. 6:158–162. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Skinner CG, Thomas JD and Osterloh JD:
Melamine toxicity. J Med Toxicol. 6:50–55. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Sun Q, Shen Y, Sun N, et al: Diagnosis,
treatment and follow-up of 25 patients with melamine-induced kidney
stones complicated by acute obstructive renal failure in Beijing
Children’s Hospital. Eur J Pediatr. 169:483–489. 2010.PubMed/NCBI
|
|
7.
|
Yang VL and Batlle D: Acute renal failure
from adulteration of milk with melamine. ScientificWorldJournal.
8:974–975. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8.
|
Sarkissian A, Babloyan A, Arikyants N,
Hesse A, Blau N and Leumann E: Pediatric urolithiasis in Armenia: a
study of 198 patients observed from 1991 to 1999. Pediatr Nephrol.
16:728–732. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9.
|
Brown CA, Jeong KS, Poppenga RH, et al:
Outbreaks of renal failure associated with melamine and cyanuric
acid in dogs and cats in 2004 and 2007. J Vet Diagn Invest.
19:525–531. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10.
|
Puschner B, Poppenga RH, Lowenstine LJ,
Filigenzi MS and Pesavento PA: Assessment of melamine and cyanuric
acid toxicity in cats. J Vet Diagn Invest. 19:616–624. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
11.
|
Dobson RL, Motlagh S, Quijano M, et al:
Identification and characterization of toxicity of contaminants in
pet food leading to an outbreak of renal toxicity in cats and dogs.
Toxicol Sci. 106:251–262. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Guo YF: Ultrasound diagnosis of urinary
calculi in children. Zhongguo Chao Sheng Yixue Za Zhi.
17:8732001.(In Chinese).
|
|
13.
|
Jayanthi VR, Arnold PM and Koff SA:
Strategies for managing upper tract calculi in young children. J
Urol. 162:1234–1237. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14.
|
Yuan HS, Ren SQ and Wu XM: Extracorporeal
shock wave lithotripsy of bladder stones in children. Journal of
Clinical Urology. 13:1751998.
|
|
15.
|
Chen ZY, Li YP and Zhao HQ: ESWL treatment
of urinary calculi in children. Journal of Harbin Medical
University. 29:591995.
|
|
16.
|
Zou XF, Huang M and Yuan YH: The treatment
of urinary calculi in children with ureteroscopy and the pneumatic
lithotriptor (with reports of 18 cases). Journal of Gannan Medical
College. 3:237–238. 2002.(In Chinese).
|