Introduction
Chronic hepatitis B virus (HBV) infection is a
worldwide health problem with >400 million people infected
(1,2). Patients with persistent infection of
HBV, including those who are hepatitis B surface antigen
(HBsAg)-positive without diagnosis of hepatitis, may progress to
chronic hepatitis B (CHB), hepatitis B-related acute-on-chronic
liver failure (HB-ACLF), cirrhosis and hepatocellular carcinoma
(HCC). Disease progression results from the struggle between virus
and host (3,4). The existence of different clinical
stages is likely to be due to the various immune states that are
possible with this infection (5,6).
Cytokines are key molecules in the complex signaling network of
humoral and cell-mediated immunity (4). Analyses of the changes in cytokine
expression patterns during progression of the various clinical
stages of chronic HBV infection may facilitate the understanding of
pathogenesis.
Human interleukin (IL)-21 is a member of the type I
cytokine family that is encoded by a gene on chromosome 4 (7). The mature form of human IL-21
contains 131 amino acids. The cytokine is produced by activated
natural killer (NK) T cells and multiple CD4+ T cell subsets,
including effector memory and central memory CD4+ T cells and
differentiated T helper cell subsets polarized towards Th17 cell
and T follicular helper phenotypes (8–10).
IL-21 has important protective roles in the regulation of
hematopoiesis, innate and adaptive immune responses and the
regulation of autoimmunity (11–15).
Similarly to other cytokines that signal through the common γ-chain
subunit, IL-21 activates the Janus kinase (JAK)-family protein
tyrosine kinases, JAK1 and JAK3, with JAK1 binding to the IL-21
receptor (IL-21R) and JAK3 binding to the common γ-chain (16–18).
IL-21R-driven signaling results in the activation of signal
transducer and activator of transcription molecules. IL-21R is
expressed on a variety of immune cells, including T, B, NK and
dendritic cells (DCs), as well as on non-immune cells such as
fibroblasts, epithelial and endothelial cells (19). IL-21 has been shown to overcome
virus-induced CD8+ T cell exhaustion, stimulate memory CD8+ T
cells, stimulate the maturation and lytic ability of NK cells,
suppress T regulatory cells and their production of IL-10 and
stimulate precursor Th17 cells that have the ability to evolve into
Th1 cells (20–22). It is also possible that DCs may
become resistant to the suppressive effects of IL-21. Therefore, as
an important inflammatory factor (23), IL-21 may be involved in liver
injury via regulating the function of innate and adaptive immune
competent cells and/or affecting the expression of other
inflammatory cytokines. Previous studies have identified that IL-21
has an important role in murine lymphocytic choriomeningitis virus
and human immunodeficiency virus infections (24–30).
However, the role of IL-21 in chronic HBV infection remains
unclear.
Therefore, the aim of the present study was to
analyze serum IL-21 levels at various clinical stages of chronic
HBV infection and determine whether IL-21 is associated with the
progression of chronic HBV infection.
Materials and methods
Study subjects
A total of 109 patients with chronic HBV infection,
admitted to the First Affiliated Hospital of Xi’an Jiaotong
University (Xi’an, China) between January 2011 and October 2012,
and 19 healthy controls (HCs) were enrolled in this study. All
patients were HBsAg-positive for >6 months and had not received
any antiviral treatment. The patients were divided into four
groups. Firstly, the CHB group (n=35) included 24 hepatitis B e
antigen (HBeAg)-positive and 11 HBeAg-negative cases. Patients were
included in this group if they had serum alanine aminotransferase
levels of >40 IU/l (upper normal limit, 40 IU/l), total
bilirubin (TB) levels of <171 μM and plasma prothrombin activity
(PTA) of >40%. Secondly, the HB-ACLF group (n=34) included 9
Child-Pugh B and 25 Child-Pugh C cases. The diagnosis of HB-ACLF
was based on the clinical observation of grade ≥2 hepatic
encephalopathy or a rapid increase in ascites that occurred within
4 weeks of the first signs of jaundice or coagulopathy. These
clinical criteria were associated with the recent development of
severe jaundice (TB levels, >171 μM) or rapidly rising levels of
TB (>17.1 μmol/day) and a PTA of <40%. Thirdly, the clinical
cirrhosis group (n=40), included 12 Child-Pugh A, 20 Child-Pugh B
and 8 Child-Pugh C cases. Inclusion criteria consisted of the
presence of long-term cirrhosis-associated complications, including
ascites (with or without spontaneous bacterial peritonitis),
varices and encephalopathy, and/or ultrasonographic observation of
a small-sized liver with or without ascites and splenomegaly.
Patients with the following concomitant conditions were excluded
from the study: Hepatitis C (HCV) and D (HDV) infection, Wilson’s
disease, autoimmune hepatitis, primary biliary cirrhosis and
significant intake of alcohol (females, 20 g per day; males, 30 g
per day). Finally, the HC group was recruited from students and
staff at the First Affiliated Hospital of Xi’an Jiaotong
University. The baseline characteristics of the patients are
summarized in Table I.
 | Table IClinical characteristics of the study
subjects. |
Table I
Clinical characteristics of the study
subjects.
| Groups |
|---|
|
|
|---|
| Characteristics | CHB | ACLF | Cirrhosis | HC |
|---|
| Patients, n | 35 | 34 | 40 | 19 |
| Age, years | 38.53±15.63 | 37.44±12.40 | 49.88±12.90 | 21.93±0.83 |
| Gender,
male/female, n | 29/6 | 26/8 | 31/9 | 7/12 |
| ALT, IU/l (normal
scale, 0–40) | 106.47±127.50 | 104.27±114.37 | 56.48±53.29 | NA |
| TBIL, μM (normal
scale, 0–17.1) | 46.08±35.12 | 306.38±206.50 | 73.44±71.25 | NA |
| WBC,
×109 | 4.89±2.06 | 4.24±1.57 | 3.83±2.21 | NA |
| Lymphocyte count,
×109 | 1.55±0.65 | 1.29±0.48 | 1.29±0.90 | NA |
| Percentage of
lymphocytes, % | 33.58±10.66 | 32.22±12.24 | 33.90±14.57 | NA |
| HBV DNA,
log10 IU/ml | 5.56±1.38 | 3.79±2.38 | 3.79±2.75 | NA |
Ethical considerations
The study was conducted according to the Declaration
of Helsinki and was approved by the Ethical Committee of the First
Affiliated Hospital of Xi’an Jiaotong University. Written informed
consent was obtained from all participants.
Antibodies and other reagents
IL-21-Alex Fluor 647 and CD4-fluorescein
isothiocyanate (FITC) fluorochrome conjugated antibodies with their
isotype controls were purchased from BD Biosciences (San Jose, CA,
USA).
Serological and routine blood assays
The presence of HBsAg, HBeAg, anti-HBs, anti-HBc,
anti-HBe, anti-HCV and anti-HDV was determined using commercial
kits according to the manufacturer’s instructions (Quantification
kit; Abbott Laboratories, Green Oaks, IL, USA).
Serum cytokine concentration
Serum concentrations of IL-21 were measured in
duplicate using a commercial human IL-21 platinum enzyme-linked
immunosorbent assay kit (eBioscience, Inc., San Diego, CA, USA),
according to the manufacturer’s instructions. The lower detection
limit of the kit was 20 pg/ml.
Intracellular cytokine staining
(ICS)
All cells used in the study were cultured at 37°C in
a humidified atmosphere containing 5% CO2 (31). Heparinized whole blood (200 μl) was
stimulated with 20 ng/ml phorbol-12-myristate-13-acetate (PMA;
Sigma-Aldrich, St. Louis, MO, USA) and 1 μg/ml calcium ionomycin
(Sigma-Aldrich) in the presence of monensin (3 μM; Sigma-Aldrich)
for 5 h. The control consisted of unstimulated cells under
identical conditions. Next, 1 ml 1X BD FACS Lysing Solution (BD
Biosciences; diluted with 10X solution 1:10 with deionized water
prior to use) was added to the activated and unstimulated whole
blood samples, mixed gently and incubated for 10 min at room
temperature. Wash buffer (2 ml) was added to each tube and
centrifuged at 500 × g for 5 min at room temperature. The cells
were harvested and stained with CD4-FITC for 30 min at room
temperature in the dark and then washed and fixed with 100 μl
Medium A (Caltag Fix&Perm™ reagent; Invitrogen Life
Technologies, Carlsbad, CA, USA) for 15 min. Following washing and
permeabilization for 25 min with 100 μl Medium B (Invitrogen Life
Technologies), the cells were incubated at room temperature for 30
min in the dark with IL-21-Alex Fluor 647 or the isotype controls.
Wash buffer (2 ml) was added to each tube and centrifuged at 500 ×
g for 5 min at room temperature. The supernatant was decanted and
200 μl paraformaldehyde (1%) in phosphate-buffered saline was
added. The pellet was resuspended and stored at 4°C in the dark
prior to flow cytometry analysis. Samples were analyzed within 24 h
(32–34).
Statistical analysis
All statistical analyses were performed using SPSS
software version 17.0 (SPSS, Inc., Chicago, IL, USA). Data are
expressed as the mean ± SD. Parametric data were analyzed using
one-way analysis of variance. For the homogeneity test of variance,
Levene’s test was used. Dunnett’s T3 test was used in case of
heterogeneity of variance among multiple groups. A corrected
P-value was calculated by Bonferroni correction for multiple
comparisons when the uncorrected P-value was <0.05. Association
between variables was evaluated using Spearman’s correlation
coefficient. All statistical analyses were based on two-tailed
hypothesis tests where P<0.05 was considered to indicate a
statistically significant difference.
Results
Cross-sectional analysis of serum IL-21
levels
Serum IL-21 concentrations in the CHB, HB-ACLF,
cirrhosis and HC groups are shown in Table II. The mean serum level of IL-21
in the HB-ACLF group was 455.38±412.38 ng/ml, which was
significantly higher than that of the CHB, cirrhosis and HC groups.
The mean serum level of IL-21 in the CHB group was 303.54±152.77
ng/ml, which was higher compared with that of the cirrhosis and HC
groups. The mean level of IL-21 in the cirrhosis group also
increased, but there was no statistically significant difference
when compared with the HC group (Fig.
1).
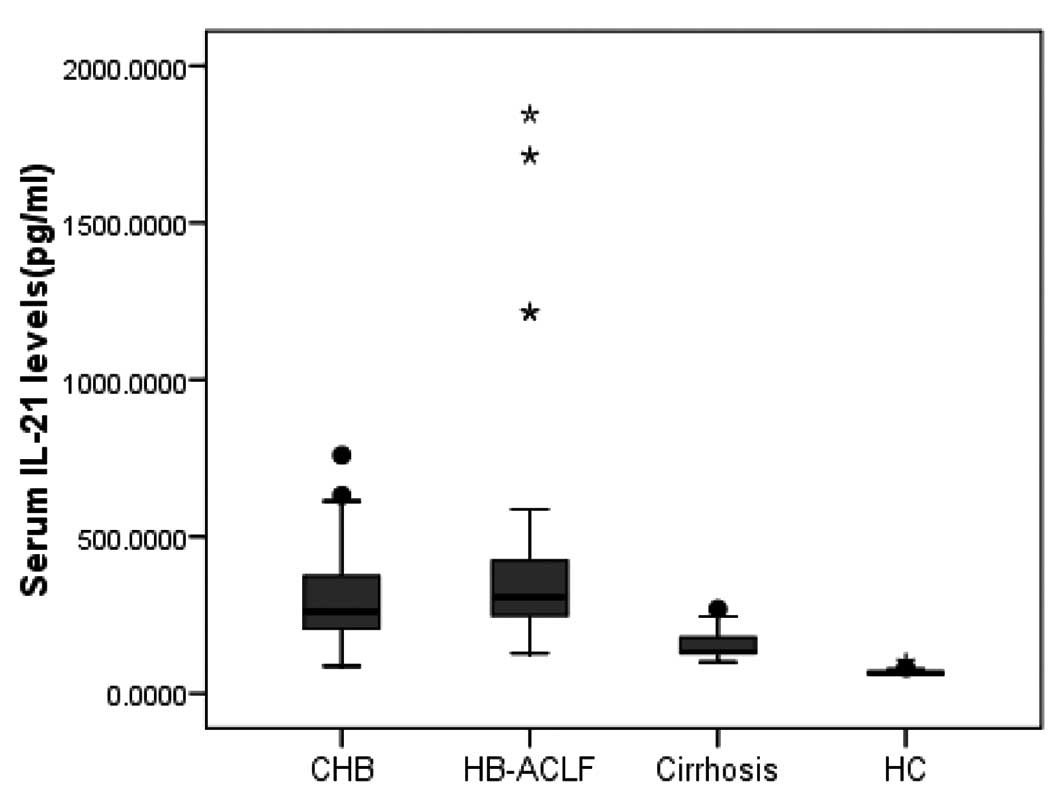 | Figure 1Comparison of serum IL-21
concentrations in the four groups. Horizontal bars indicate the
median values in each group. P-values indicate the significance of
interclass comparisons using one-way analysis of variance.
Corrected P-values were calculated by Bonferroni correction for
multiple comparisons when the uncorrected P-value was <0.05.
P=0.04, CHB vs. HB-ACLF; P=0.033, CHB vs. cirrhosis; P=0.003, CHB
vs. HC; P=0.000, HB-ACLF vs. cirrhosis; P=0.000, HB-ACLF vs. HC ;
P=0.82, cirrhosis vs. HC. CHB, chronic hepatitis B; HB-ACLF,
hepatitis B-related acute-on-chronic liver failure; HC, healthy
controls; IL-21, interleukin-21. |
| Table IIMean serum IL-21 concentrations and
IL-21+CD4+ cell frequencies in the study groups. |
Table II
Mean serum IL-21 concentrations and
IL-21+CD4+ cell frequencies in the study groups.
| Groups | Serum IL-21
concentrations, pg/ml | Frequency of
IL-21+CD4+ cells, % |
|---|
| CHB | 303.54±152.77 | 29.52±9.08 |
| HB-ACLF | 455.38±412.38 | 22.32±10.66 |
| Cirrhosis | 154.38±39.83 | 20.49±8.62 |
| HC | 68.24±9.06 | 13.61±2.87 |
Cross-sectional analysis of
IL-21-secreting CD4+ T cells by ICS
The frequencies of IL-21+CD4+ T cells in
PMA/ionomycin-stimulated lymphocytes in the four groups are shown
in Table II and Figs. 2 and 3. The frequency of IL-21+CD4+ T cells in
the CHB, HB-ACLF and cirrhosis groups was significantly higher
compared with the HC group (P<0.05). The mean percentage of
IL-21+CD4+ T cells in the CHB group was 29.52±9.08%, which was the
highest compared with the remaining groups. However, the percentage
of IL-21+CD4+ T cells in the HB-ACLF group was similar to the
cirrhosis group, but with no statistically significant
difference.
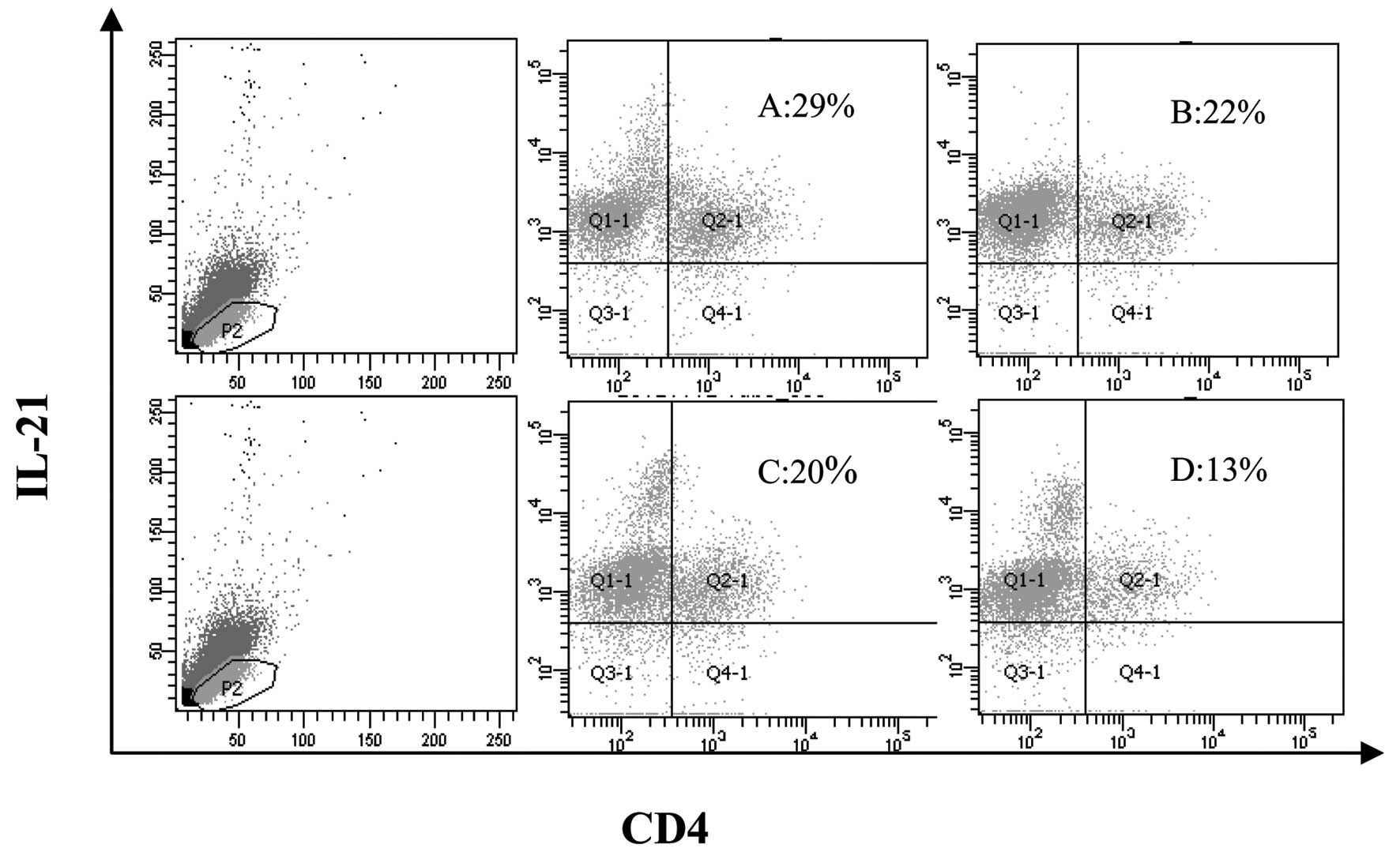 | Figure 2Analysis of IL-21-producing cells by
ICS. The frequencies of IL-21-secreting CD4+ T cells in the CHB,
HB-ACLF and cirrhosis groups are compared with the HC group. Gated
on lymphocytes. A, CHB; B, HB-ACLF; C, cirrhosis; D, HC; ICS,
intracellular cytokine staining; CHB, chronic hepatitis B; HB-ACLF,
hepatitis B-related acute-on-chronic liver failure; HC, healthy
controls; IL-21, interleukin-21. |
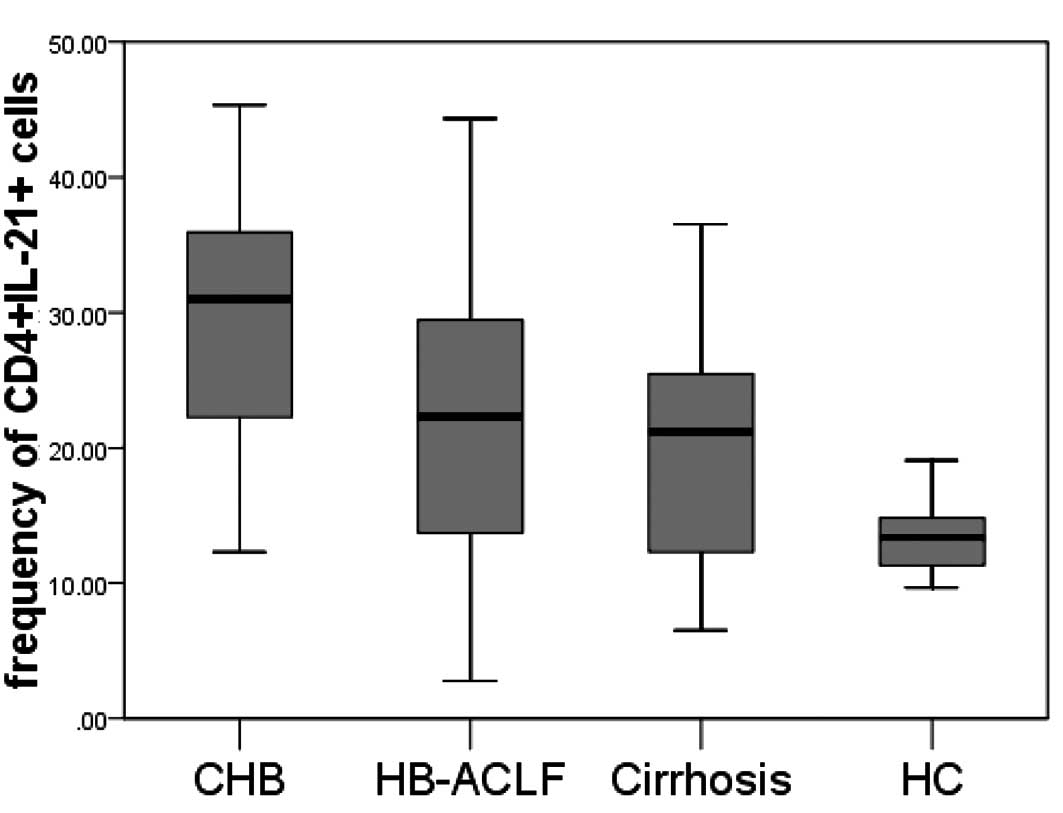 | Figure 3Comparison between the frequencies of
CD4+IL-21+ cells in the CHB, HB-ACLF, cirrhosis and HC groups.
P=0.003, CHB vs. HB-ACLF; P=0.000, CHB vs. cirrhosis; P=0.000, CHB
vs. HC; P=0.88, HB-ACLF vs. cirrhosis; P=0.003, HB-ACLF vs. HC;
P=0.04, cirrhosis vs. HC. CHB, chronic hepatitis B; HB-ACLF,
hepatitis B-related acute-on-chronic liver failure; HC, healthy
controls; IL-21, interleukin-21. |
Association between IL-21 concentrations
and lymphocytes in the peripheral blood
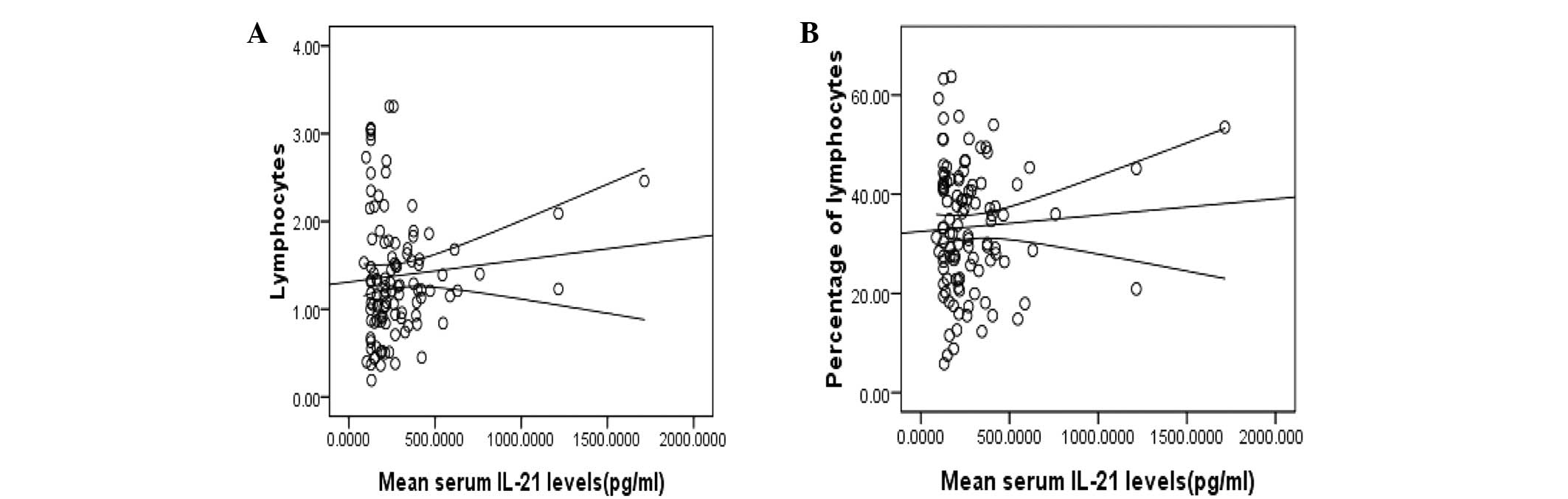
There were no correlations between IL-21
concentrations and the frequency (r=0.081; P=0.402) or percentage
of lymphocytes (r=0.06; P=0.534) in the peripheral blood (Fig. 4).
Association between the frequency of
IL-21+CD4+ cells and lymphocytes in the peripheral blood
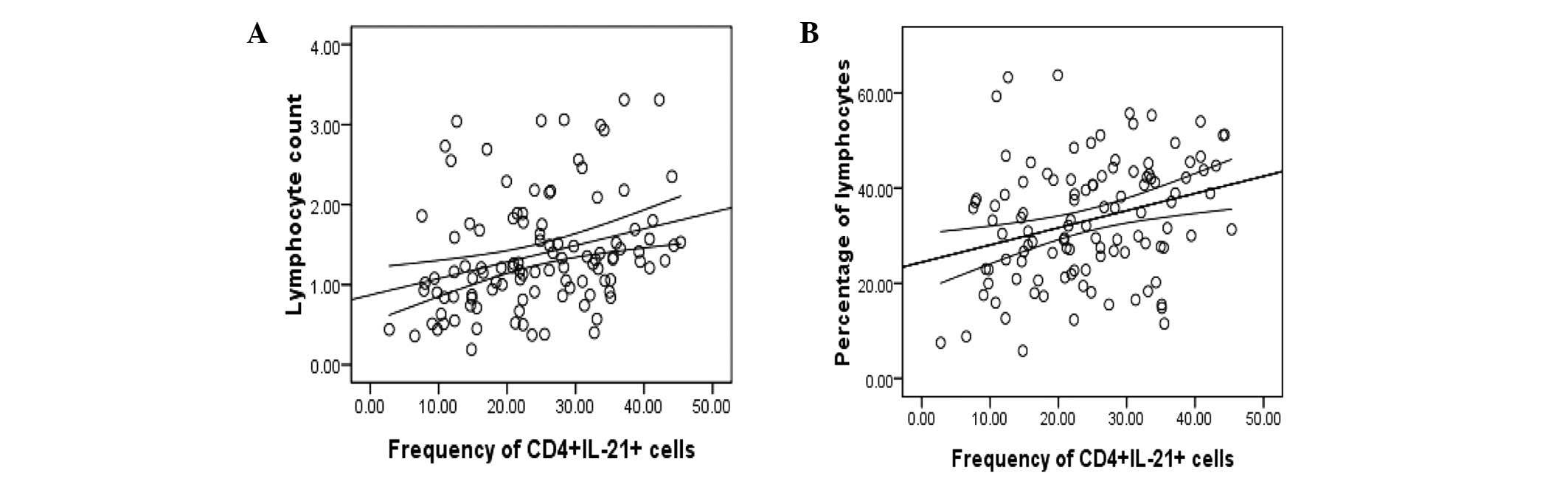
The frequency of IL-21+CD4+ cells positively
correlated with the frequency (r=0.296; P=0.002) and percentage of
lymphocytes (r=0.293; P=0.002) in the peripheral blood (Fig. 5).
Discussion
The majority of viral infectious diseases are
self-limiting, such as measles, mumps and rhinovirus (35). Only a few result in chronic
infections, including HBV, HCV and HIV (36). The reason that certain viruses only
cause acute infections, while others result in chronic disease has
not been elucidated. The majority of liver damage caused by viral
infections is mediated by the host immune response (6). Acquired and innate immunity are
hypothesized to be involved in the pathogenesis of viral infectious
diseases (3,5).
Patients infected with HBV may develop CHB, ACLF,
cirrhosis and HCC. In the current study, serum IL-21 concentrations
were measured at various clinical stages of chronic HBV infection
and the results demonstrated that serum IL-21 levels were highest
in the HB-ACLF and CHB groups.
At present, CHB pathogenesis remains unclear. HBV
itself has no direct cytotoxic effects. Immune pathological injury
to the liver may be induced by the virus, which maintains in
vivo replication by activating monocyte/macrophage
phagocytosis, processing and triggering an immune response.
Cytokines secreted by immune cells are important in the occurrence,
development and progression of CHB. Chronicity of HBV infection may
be more frequent in T and B cell immunodeficiency (37). IL-21 stimulates T and B cell
responses and is important for the control of chronic viral
infections. Therefore, serum IL-21 levels in patients with CHB may
be involved with the development of chronic HBV infection.
The results of the present study revealed that serum
IL-21 levels were significantly elevated in the CHB group. However,
the elevated levels in the CHB group were lower compared with
previously detected levels in the acute stage of hemorrhagic fever
with renal syndrome (data not shown). A previous study demonstrated
that serum IL-21 levels in CHB patients treated with interferon
(IFN) and nucleoside analogues increased as the viral loads
decreased (38). There are two
antiviral mechanisms of IFN activity. The first is direct antiviral
action and the second is associated with immunoregulation (39). By contrast, nucleoside analogues
interfere directly with the replication of the virus (40). However, a previous study has shown
that certain nucleoside analogues have immunomodulatory effects
(41). There is no general
consensus on whether immune mechanisms are involved in nucleoside
analogue efficacy. However, increased IL-21 levels have been
associated with viral elimination (42). Relatively low serum IL-21 levels in
CHB may play a causal role in the persistence of HBV infection.
Since acute HBV infection commonly begins with no
significant symptoms, the current study did not include cases of
acute HBV infection. Thus, dynamic changes in serum IL-21 levels in
acute HBV infection require further study.
ACLF, an acute hepatic insult that frequently
presents with jaundice and coagulopathy, is complicated within 4
weeks by ascites and/or encephalopathy in patients previously
diagnosed or undiagnosed with chronic liver disease (43). In China, >80% of ACLF cases are
infected with HBV and the relapse of hepatitis occasionally results
in liver failure (44). The
pathogenic mechanisms of HB-ACLF remain largely unknown. Genetic
mutations of the virus and derangements in the hosts themselves can
result in hepatic injury and malfunction of the liver due to
immunological damage, ischemia and anoxia or endotoxemia, which may
occur sequentially or simultaneously with the virological rebound
(45). A number of studies have
focused on immune damage. Monocytes, DCs, NK cells, CD4+CD25+
regulatory T cells, Th17 cells and other immunologically competent
cells have been shown to be involved in the pathogenesis of HB-ACLF
(46–49).
The results of the present study demonstrated that
serum IL-21 levels were elevated in patients with HB-ACLF, which is
consistent with the results of Hu et al (50). Serum IL-21 levels in the HB-ACLF
group were higher than those in the CHB group. Immunological damage
is the main factor of liver injury in HB-ACLF. Higher serum IL-21
levels in HB-ACLF may play a positive or negative role, since IL-21
may activate T and B cells to eliminate the virus or injure the
liver by the release of inflammatory cytokines.
Patients with cirrhosis caused by HBV infection
often have a variety of complications, including chronic liver
failure and HCC. IL-21 levels were measured in patients with CHB,
HB-ACLF and cirrhosis over time. The results showed that serum
IL-21 levels in the CHB and HB-ACLF groups were higher than in
patients with cirrhosis caused by HBV infection. CD4+IL-21+ T cell
frequency in the CHB group was higher compared with the cirrhosis
group and correlated with the peripheral blood lymphocyte counts.
While the mechanism by which these observations occurred has not
yet been determined, one possible contributing factor is the
decrease in the numbers of peripheral blood and lymphocytes due to
the hypersplenism that accompanies portal hypertension in
cirrhosis.
In conclusion, administration of IL-21 is
well-tolerated in humans when compared with other cytokines. IL-21
is currently being evaluated in clinical trials as an immunotherapy
agent against melanoma and renal cell carcinoma (51). The results of the present study
indicate that IL-21 should also be considered as an
immunotherapeutic tool for HBV-infected individuals.
Acknowledgments
The study was supported by grants from the National
Grand Program on Key Infectious Disease of China (no.
2012ZX10002007-002-007) and the Shaanxi Province Natural Foundation
of China (nos. 19100047 and 08140009).
References
|
1
|
Lavanchy D: Worldwide epidemiology of HBV
infection, disease burden, and vaccine prevention. J Clin Virol.
34(Suppl 1): S1–S3. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abdurakhmanov DT: Chronic HBV infection.
Klin Med (Mosk). 80:20–26. 2002.(In Russian).
|
|
3
|
Rapicetta M, Ferrari C and Levrero M:
Viral determinants and host immune responses in the pathogenesis of
HBV infection. J Med Virol. 67:454–457. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nakamura I, Ochiai K and Imawari M:
Persistent infection of HBV - host-related factors and viral
factors. Nihon Rinsho. 62(Suppl 8): S112–S115. 2004.(In
Japanese).
|
|
5
|
Bertoletti A and Ferrari C: Kinetics of
the immune response during HBV and HCV infection. Hepatology.
38:4–13. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Takaki A, Tatsukawa M, Koike K and
Shiratori Y: Mechanism of immune surveillance against HBV
infection. Nihon Rinsho. 62(Suppl 8): S62–S65. 2004.(In
Japanese).
|
|
7
|
Zeng R, Spolski R, Casas E, Zhu W, Levy DE
and Leonard WJ: The molecular basis of IL-21-mediated
proliferation. Blood. 109:4135–4142. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu Z, Yang L, Cui Y, et al: Il-21
enhances NK cell activation and cytolytic activity and induces Th17
cell differentiation in inflammatory bowel disease. Inflamm Bowel
Dis. 15:1133–1144. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Parrish-Novak J, Foster DC, Holly RD and
Clegg CH: Interleukin-21 and the IL-21 receptor: novel effectors of
NK and T cell responses. J Leukoc Biol. 72:856–863. 2002.PubMed/NCBI
|
|
10
|
Wang T, Diaz-Rosales P, Costa MM, et al:
Functional characterization of a nonmammalian IL-21: rainbow trout
Oncorhynchus mykiss IL-21 upregulates the expression of the
Th cell signature cytokines IFN-gamma, IL-10, and IL-22. J Immunol.
186:708–721. 2011.PubMed/NCBI
|
|
11
|
MacDonald TT, Bell I and Monteleone G: The
opposing roles of IL-21 and TGFβ1 in chronic inflammatory bowel
disease. Biochem Soc Trans. 39:1061–1066. 2011.
|
|
12
|
Liu L, Xu Y, Wang J and Li H: Upregulated
IL-21 and IL-21 receptor expression is involved in experimental
autoimmune uveitis (EAU). Mol Vis. 15:2938–2944. 2009.PubMed/NCBI
|
|
13
|
Bubier JA, Sproule TJ, Foreman O, et al: A
critical role for IL-21 receptor signaling in the pathogenesis of
systemic lupus erythematosus in BXSB-Yaa mice. Proc Natl Acad Sci
USA. 106:1518–1523. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Liu R, Wu Q, Su D, et al: A regulatory
effect of IL-21 on T follicular helper-like cell and B cell in
rheumatoid arthritis. Arthritis Res Ther. 14:R2552012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yoshizaki A, Miyagaki T, DiLillo DJ, et
al: Regulatory B cells control T-cell autoimmunity through
IL-21-dependent cognate interactions. Nature. 491:264–268. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Habib T, Senadheera S, Weinberg K and
Kaushansky K: The common gamma chain (gamma c) is a required
signaling component of the IL-21 receptor and supports
IL-21-induced cell proliferation via JAK3. Biochemistry.
41:8725–8731. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
de Totero D, Meazza R, Capaia M, et al:
The opposite effects of IL-15 and IL-21 on CLL B cells correlate
with differential activation of the JAK/STAT and ERK1/2 pathways.
Blood. 111:517–524. 2008.PubMed/NCBI
|
|
18
|
Asao H, Okuyama C, Kumaki S, et al:
Cutting edge: the common gamma-chain is an indispensable subunit of
the IL-21 receptor complex. J Immunol. 167:1–5. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ettinger R, Kuchen S and Lipsky PE: The
role of IL-21 in regulating B-cell function in health and disease.
Immunol Rev. 223:60–86. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Johnson LD and Jameson SC: Immunology. A
chronic need for IL-21. Science. 324:1525–1526. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Deenick EK and Tangye SG: Autoimmunity:
IL-21: a new player in Th17-cell differentiation. Immunol Cell
Biol. 85:503–505. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Barker BR, Gladstone MN, Gillard GO, Panas
MW and Letvin NL: Critical role for IL-21 in both primary and
memory anti-viral CD8+ T-cell responses. Eur J Immunol.
40:3085–3096. 2010.PubMed/NCBI
|
|
23
|
Nurieva R, Yang XO, Martinez G, et al:
Essential autocrine regulation by IL-21 in the generation of
inflammatory T cells. Nature. 448:480–483. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
McGavern DB: A little ‘help’ from IL-21
during persistent viral infection. J Mol Cell Biol. 2:8–10.
2010.
|
|
25
|
Zhao CC, Xue J, Cong Z, et al: Circulating
IL-21 levels increase during early simian-human immunodeficiency
virus infection in macaques. Arch Virol. 158:853–858. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pallikkuth S, Parmigiani A and Pahwa S:
Role of IL-21 and IL-21 receptor on B cells in HIV infection. Crit
Rev Immunol. 32:173–195. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Papatriantafyllou M: Antiviral immunity:
IL-21 comes with age. Nat Rev Immunol. 11:236–237. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Iannello A, Boulassel MR, Samarani S, et
al: Dynamics and consequences of IL-21 production in HIV-infected
individuals: a longitudinal and cross-sectional study. J Immunol.
184:114–126. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Iannello A, Samarani S and Ahmad A:
Comment on ‘HIV-specific IL-21 producing CD4+ T cells are induced
in acute and chronic progressive HIV infection and are associated
with relative viral control’. J Immunol. 185:56752010.
|
|
30
|
Elsaesser H, Sauer K and Brooks DG: IL-21
is required to control chronic viral infection. Science.
324:1569–1572. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Green KJ, Rowbottom DG and Mackinnon LT:
Exercise and T-lymphocyte function: a comparison of proliferation
in PBMC and NK cell-depleted PBMC culture. J Appl Physiol (1985).
92:2390–2395. 2002.PubMed/NCBI
|
|
32
|
Cho SH, Stanciu LA, Begishivili T, Bates
PJ, Holgate ST and Johnston SL: Peripheral blood CD4+ and CD8+ T
cell type 1 and type 2 cytokine production in atopic asthmatic and
normal subjects. Clin Exp Allergy. 32:427–433. 2002.
|
|
33
|
Gauduin MC, Kaur A, Ahmad S, Yilma T,
Lifson JD and Johnson RP: Optimization of intracellular cytokine
staining for the quantitation of antigen-specific CD4+ T cell
responses in rhesus macaques. J Immunol Methods. 288:61–79.
2004.
|
|
34
|
Garba ML and Frelinger JA: Intracellular
cytokine staining for TGF-beta. J Immunol Methods. 258:193–198.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Paunio M, Heinonen OP, Virtanen M,
Leinikki P, Patja A and Peltola H: Measles history and atopic
diseases: a population-based cross-sectional study. JAMA.
283:343–346. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Goeser T and Töx U: Therapy of hepatitis B
and C. Problem situations in chronic HBV and HCV infection. Praxis
(Bern 1994). 91:983–990. 2002.(In German).
|
|
37
|
Kuo A and Gish R: Chronic hepatitis B
infection. Clin Liver Dis. 16:347–369. 2012. View Article : Google Scholar
|
|
38
|
Ma SW, Huang X, Li YY, et al: High serum
IL-21 levels after 12 weeks of antiviral therapy predict HBeAg
seroconversion in chronic hepatitis B. J Hepatol. 56:775–781. 2012.
View Article : Google Scholar
|
|
39
|
Grimm D, Heeg M and Thimme R: Hepatitis B
virus: from immunobiology to immunotherapy. Clin Sci (Lond).
124:77–85. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Michailidis E, Kirby KA, Hachiya A, et al:
Antiviral therapies: focus on hepatitis B reverse transcriptase.
Int J Biochem Cell Biol. 44:1060–1071. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Hann HW: Telbivudine: an effective
anti-HBV drug for chronic hepatitis B patients with early
on-treatment responses. Expert Opin Pharmacother. 11:2243–2249.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Li X, Wang Y, Han D, et al: Correlation of
hepatitis B surface antigen level with response to telbivudine in
naive patients with chronic hepatitis B. Hepatol Res. Mar
4–2013.(Epub ahead of print).
|
|
43
|
Sarin SK, Kumar A, Almeida JA, et al:
Acute-on-chronic liver failure: consensus recommendations of the
Asian Pacific Association for the study of the liver (APASL).
Hepatol Int. 3:269–282. 2009. View Article : Google Scholar
|
|
44
|
Du WB, Li LJ, Huang JR, et al: Effects of
artificial liver support system on patients with acute or chronic
liver failure. Transplant Proc. 37:4359–4364. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ren X, Xu Z, Liu Y, et al: Hepatitis B
virus genotype and basal core promoter/precore mutations are
associated with hepatitis B-related acute-on-chronic liver failure
without pre-existing liver cirrhosis. J Viral Hepat. 17:887–895.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Zhang Z, Zou ZS, Fu JL, et al: Severe
dendritic cell perturbation is actively involved in the
pathogenesis of acute-on-chronic hepatitis B liver failure. J
Hepatol. 49:396–406. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zou Y, Chen T, Han M, et al: Increased
killing of liver NK cells by Fas/Fas ligand and NKG2D/NKG2D ligand
contributes to hepatocyte necrosis in virus-induced liver failure.
J Immunol. 184:466–475. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Xu D, Fu J, Jin L, et al: Circulating and
liver resident CD4+CD25+ regulatory T cells actively influence the
antiviral immune response and disease progression in patients with
hepatitis B. J Immunol. 177:739–747. 2006.
|
|
49
|
Zhang JY, Zhang Z, Lin F, et al:
Interleukin-17-producing CD4(+) T cells increase with severity of
liver damage in patients with chronic hepatitis B. Hepatology.
51:81–91. 2010.
|
|
50
|
Hu X, Ma S, Huang X, et al: Interleukin-21
is upregulated in hepatitis B-related acute-on-chronic liver
failure and associated with severity of liver disease. J Viral
Hepat. 18:458–467. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Hashmi MH and Van Veldhuizen PJ:
Interleukin-21: updated review of Phase I and II clinical trials in
metastatic renal cell carcinoma, metastatic melanoma and
relapsed/refractory indolent non-Hodgkin’s lymphoma. Expert Opin
Biol Ther. 10:807–817. 2010.PubMed/NCBI
|