Introduction
Human infections with H7N9 usually occur following
recent exposure to poultry, which causes upper respiratory tract
disease to progress into pneumonia and subsequently multiple organ
failure (1). A diagnosis primarily
depends on virus detection using nasopharyngeal swabs and blood
sampling (2). Early diagnosis may
be achieved through questioning into the epidemic history; an
epidemic of influenza can be easily confounded with seasonal flu,
and requires differentiation with pneumonia through careful
observation of lung disease progression and the general condition
of the patient. Laboratory investigations comprise various methods,
including reverse transcription quantitative polymerase chain
reaction (RT-qPCR), viral isolation and full-genome sequencing, all
of which are able to confirm whether the patient is infected with
the novel H7N9 virus (3).
In the present study, the patient exhibited a rapid
deterioration; however, a diagnosis of H7N9 avian influenza was
only confirmed after five days of continuous fever. Thus, the
treatment process has provided experience for dealing with cases of
H7N9, particularly for community health centers.
Case report
Clinical presentations
A male patient, aged 77 years, was admitted to the
Putuo District People’s Hospital of Shanghai City (Shanghai, China)
after presenting with a fever for four days. On April
3rd 2013, the patient experienced chills and fever,
without evident cause or regularity, with a maximum temperature of
39.4°C. The patient did not suffer from a cough, expectoration,
sore throat, runny nose, chest tightness, chest pain, pant or whole
muscle and joint ache. A chest radiograph, obtained in the initial
hospital, revealed a fuzzy shadow in the left lower lung (Fig. 1). After intravenous (i.v) treatment
with ceftriaxone (2 g/day) and levofloxacin (0.5 g/day) for three
days, the fever improved. The patient was admitted to the Jingnan
District Centre Hospital of Shanghai (Shanghai, China) with a body
temperature of 37.8°C. Emergency blood tests revealed a leukocyte
count of 5×109/l (neutrophils, 83.6%) and a C-reactive
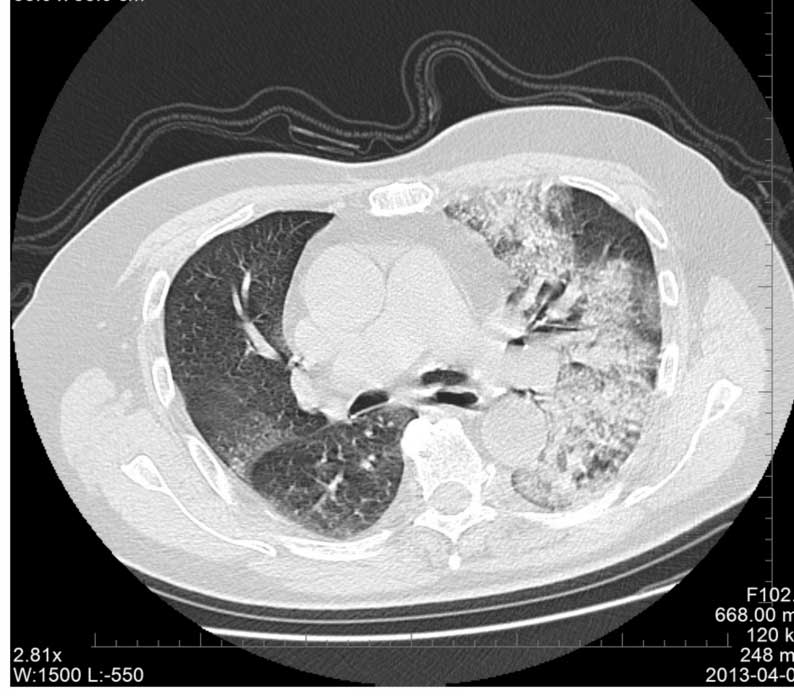
protein level of 192 mg/l. A chest computed tomography scan
(Somatom Definition AS+ 128 Multi-Slice CT Scanner; Siemens,
Munich, Germany) revealed a ‘frosted glass’ appearance in both
lungs, and a high density shadow was observed in the left lower
lobe (Fig. 2). In addition, a
bronchiologram revealed inflammation and left lung consolidation.
Since the patient was suspected of having pneumonia, the patient
was admitted to the Central Hospital of Jingan District for further
diagnosis and treatment. This study was conducted in accordance
with the Declaration of Helsinki, and with approval from the Ethics
Committee of the Central Hospital of Shanghai Jingan District.
Written informed consent was obtained from the relatives of the
patient.
Past medical history
The patient had >30 years history of paroxysmal
atrial fibrillation, and had been treated with amiodarone (0.2
g/day, orally). In addition, the patient had >20 years history
of hypertension, up to a maximum of 150/90 mmHg; thus, amlodipine
(5 mg every day) treatment had been used to control the blood
pressure, which was determined to be of proper control. The patient
denied history of diabetes, coronary heart disease, chronic
bronchitis, asthma and chronic kidney disease, viral hepatitis,
tuberculosis, typhoid fever and infectious disease.
Physical examination
Physical examination revealed a body temperature of
39.1°C, a pulse of 98 bpm, a respiratory rate (RR) of 22 and a
blood pressure of 130/70 mmHg. The patient was clear in mentality,
had regular respiration, was cooperative on examination and their
walking was not affected. The skin and mucosa exhibited no rash or
hemorrhagic spots, and the lip mucosa had no cyanosis. Pharyngeal
congestion was mild and the double tonsils were not enlarged.
Breath sounds of the bilateral lung were coarse, and scattered
rales were heard in the left lung, but without wheezing rale and
pleural friction sounds. The heart rate of the patient was 98 bpm.
Cardiac rhythm was regular, and there were no marked pathological
murmurs heard in each valve area. The abdomen was soft, with no
muscle tension, tenderness or rebound tenderness. No organomegaly
or masses were observed, and the liver and spleen were not palpated
under the ribs. There was no edema observed in the lower
extremities, and the four limbs exhibited normal muscle force and
muscle tension.
Auxiliary examination
Hospital emergency blood gas analysis revealed a pH
of 7.49, a PaCO2 of 38.6 mmHg, a PaO2 of 52.6
mmHg and a SaO2 of 87% (without oxygen). An
electrocardiogram (ECG) demonstrated sinus rhythm, atrial premature
beats, poor R wave progression in the anterior wall and T wave
changes.
Initial treatment and diagnosis
Considering the initial diagnosis of severe
pneumonia complicated with type I respiratory failure, the patient
was administered oxygen therapy and methylprednisolone to reduce
the systemic inflammatory response, and biapenem (0.6 g twice
daily, i.v) and azithromycin (0.5 g/day, i.v) were applied as
anti-infective agents. However, the patient continued to suffer
from a fever with a body temperature of up to 39.1°C, experiencing
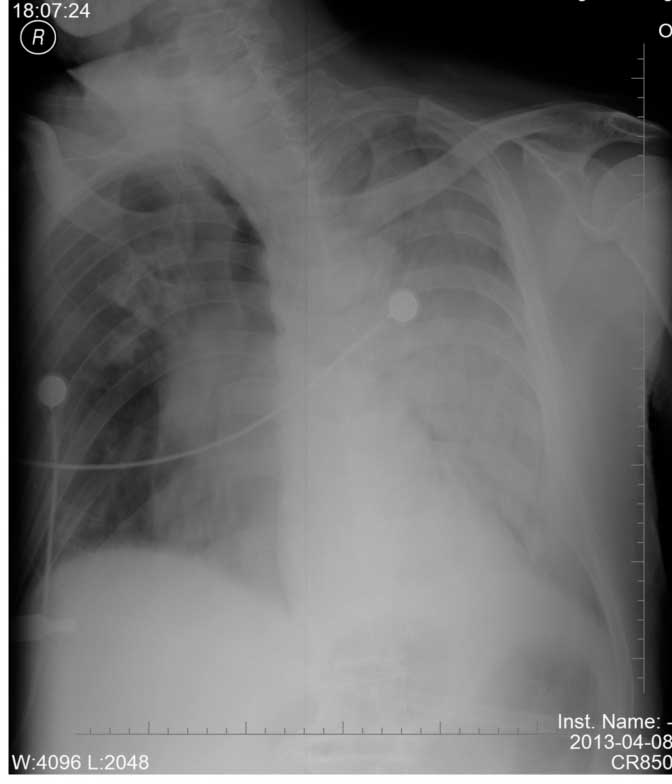
distress on day 2 following admission. With repeated inquiries into
the medical history of the patient, it was found that the patient
had come into contact with chickens two weeks previously. Combining
the epidemiological history and the rapid progression in the
pulmonary lesions of the patient (Fig.
3), a diagnosis of human infection with H7N9 avian influenza
was considered. Subsequently, the patient was isolated,
administered active anti-infective agents (biapenem and
azithromycin), an antiviral (oseltamivir; 75 mg/day, orally) and
anti-inflammatory drugs (methylprednisolone at 200 mg/day). In
addition, a biphasic positive airway pressure (BiPAP) ventilator
was used for ventilatory support, and the patient received
nasogastric enteral nutrition liquid. The case was reported to the
Jingnan District Center for Disease Control (Shanghai, China) for
nasopharyngeal swabs and blood sampling. In the early morning of
April 9th, a diagnosis of severe human infection with
H7N9 avian influenza was confirmed (1).
Diagnosis confirmation
RNA was extracted from the throat-swab samples using
the QIAamp Viral RNA Mini kit (Qiagen, Hilden, Germany), according
to the manufacturer’s instructions. Specific RT-qPCR assays were
performed to assess the presence of seasonal influenza viruses (H1,
H3, or B), H5N1, severe acute respiratory syndrome coronavirus and
novel coronavirus. RT-qPCR assays with self-designed specific
primer and probe sets were subsequently performed for the detection
of H1 to H16 and N1 to N9 subtypes, in order to verify the viral
subtypes.
Disease progression
Following hospital admission, the body temperature
of the patient fluctuated between 39 and 40°C, with shortness of
breath further aggravating. At 18:00 on April 9th, the
patient presented with cyanosis of the lips and limbs. In addition,
the fingertip pulse oximeter monitor displayed a SPO2 of
45%, and the patient underwent an emergency tracheal intubation for
assisted ventilation (BIPAP mode; set inspiratory pressure, 20 cm
H2O; positive end expiratory pressure, 10 cm
H2O; assisted spontaneous breathing, 10 cm
H2O; inspiratory time, 1.3 sec; respiratory rate, 16
times/min; concentration of oxygen inhalation, 100%), while
improving microcirculation and anti-leakage. On April
10th, the patient exhibited a damaged liver performance,
and was administered nutritional support treatment (human albumin),
intravenous immunoglobulin to strengthen the immunity, drugs for
liver protection [Coenzyme Q10 (20 mg orally, three times daily);
and Compound Glycyrrhihizin (0.2 g i.v. once daily)], daily fluid
therapy [5% glucose solution (500 ml), 5% glucose and sodium
chloride solution (500 ml) and 0.9% sodium chloride solution (500
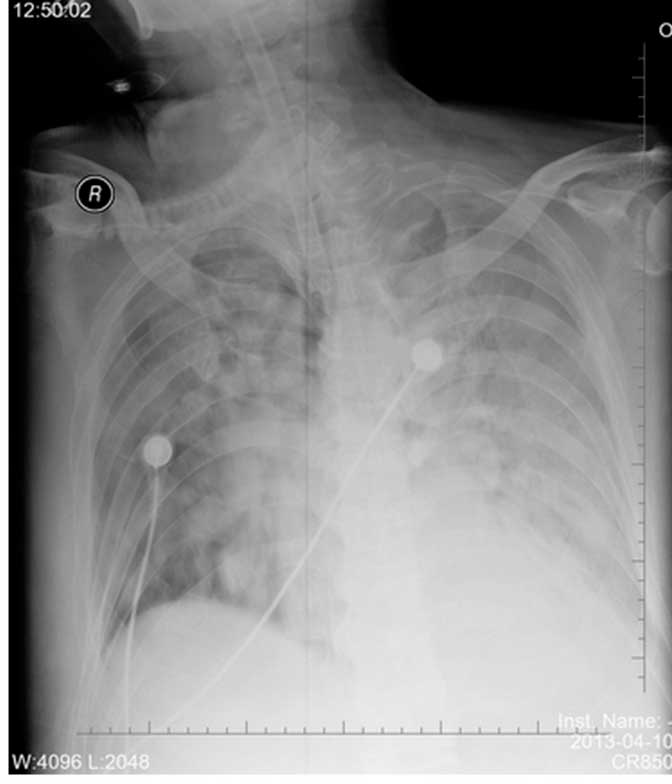
ml)], and psychological treatment. The chest radiograph showed
progression of the lesions in the right lung (Fig. 4). In addition, blood biochemical
analysis revealed glucose levels of 16.8 mmol/l, myoglobin levels
of 1,483 ng/ml, creatine kinase levels of 1,561 U/l, lactate
dehydrogenase levels of 1,007 U/l, albumin levels of 20 g/l,
alanine aminotransferase levels of 82 IU/l, aspartate
aminotransferase levels of 185 IU/l, urea nitrogen levels of 15.85
mmol/l, creatinine levels of 152.50 μmol/l, potassium levels of
4.47 mmol/l, sodium levels of 155 mmol/l and chloride levels of
115.10 mmol/l. Plasma osmotic pressure was 335.74 mmol/l, which was
calculated from the following formula: 2 × (serum sodium
concentration + serum potassium concentration) + blood glucose
concentration; the normal reference value is between 280 and 310
mmol/l. Considering the hypertonicity of the plasma, the patient
was administered cold boiled water, an aggressive diuretic and a
small dose of dopamine treatment (5 μg/kg/min, i.v). If the serum
creatinine level had continued to increase and the urine volume
decrease, continual renal replacement therapy at the bedside was
considered. On April 10th at 15:00, a small amount of
coffee colored material emerged from the corner of the lips, and a
50-ml volume of the coffee colored substance was drained. Following
application of gastrointestinal decompression, an occult blood test
of the vomit showed occult blood++, indicating a moderate degree of
microscopic hematuria. The patient was fasted, gastrointestinal
decompression was continued and proton pump inhibitor treatment was
applied. By 23:00, the patient had a rapid heartbeat and shortness
of breath. The monitor displayed the heart rate at 150 bpm, the RR
at 35 and an SPO2 of 87%. In addition, the ECG revealed
atrial fibrillation at a rapid ventricular rate. The patient was
immediately administered 200 mg Cordarone, 20 mg furosemide, 40 mg
Xinkang, 50 mg morphine and 0.4 mg cedilanid intravenously. After 1
h, the heart rate and breathing of the patient improved. On April
13th, the patient exhibited a persistent fever,
circulation failure with renal failure. Furthermore, the blood
pressure was unable to be maintained and the levels of urine were
very low. On April 14th at 00:55, the patient succumbed
to multiple organ failure, which caused cardiac arrest, and
subsequently the loss of ventilator breathing, an arterial pulse
and a pupillary light reflex. The ECG was shown to be asystole, and
clinical death was confirmed.
Discussion
Severe human infection with H7N9 avian influenza
progresses very rapidly. Since no specific and effective therapy
has been developed, treatment is difficult. Early detection and
diagnosis, which may slow the disease progression to prevent severe
pneumonia, are essential for improving patient outcome. However, it
also should be considered that the most effective approach to
managing the problem of H7N9 viral infection is to educate the
general public on aspects of healthcare, such as self-prevention
and the promotion of basic sanitation, which are associated with
the transmission of respiratory infections (4).
Epidemiological history is one of the main clues to
the diagnosis of infectious disease; however, a latency that is
longer than the conventional report or no clear epidemiological
contact history should not be considered as exclusion criteria for
diagnosis. Detection of the H7N9 virus in samples collected from a
pigeon and chickens at a market in Shanghai was confirmed by the
China Animal Disease Control Center (Beijing, China) (5). Severe infection with H7N9 avian
influenza usually has the initial symptoms of fever and respiratory
system infection, and monitoring of the sustained clinical symptoms
and dynamic radio-imaging should be performed. In addition, samples
should be collected immediately following admission for virus
nucleic acid detection to confirm the diagnosis, which may promptly
improve the medication time (6).
The influenza virus not only invades the respiratory system, but
also affects multiple organs. With the added complications of the
different baseline statuses of patients and the atypical clinical
manifestations, dynamic monitoring of pulmonary imaging is
particularly important for the early identification of lung
infections and diseases, since viral pneumonia characteristic
changes can be detected. In addition, close monitoring of blood gas
analysis, liver and kidney function, myocardial enzymes and immune
indexes should be performed, as this may lead to early detection of
the disease and subsequent prevention of complications. For cases
that cannot be clinically confirmed, if there are underlying
diseases and risk factors, timely administration of oseltamivir
should be provided to inhibit viral replication, as well as
treatments aimed at the causes. The emergence of the novel H7N9
influenza has caused global concern with regard to the ability of
this virus to spread between humans (7); however, until now, there is no
sufficient evidence of that which requires further study.
In addition, attention should be paid to the control
of complications, nutritional support, reconstruction and
stabilization of the internal environment and immune homeostasis.
Early administration of glucocorticoids can inhibit the
inflammatory reaction, reduce the release of cytokines and
inflammatory mediators, and reduce alveolar exudation. Furthermore,
timely trachea intubation and application of respiratory support
technology can correct hypoxia, protect major organ functions and
prevent multiple organ dysfunction (8). For patients with renal insufficiency,
continuous hemofiltration applied at the bedside may be the primary
method for improving the prognosis.
In conclusion, severe human infection of H7N9 avian
influenza often involves multiple systems, with rapid progression
and poor prognosis, emphasizing the requirement for
multidisciplinary, comprehensive management. Airway management,
prevention of infection, mechanical ventilation, water balance
support, electrolyte and acid-base balance, nutritional support and
the maintenance of important organ function are key to a successful
outcome for critically ill patients (9). In addition, in elderly patients, the
pre-existence of a disease may be a risk factor, and may directly
affect the prognosis of the patients (10).
References
|
1
|
Gao R, Cao B, Hu Y, et al: Human infection
with a novel avian-origin influenza A (H7N9) virus. N Engl J Med.
368:1888–1897. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hackett H, Bialasiewicz S, Jacob K, et al:
Screening for H7N9 influenza A by matrix gene-based real-time
reverse-transcription PCR. J Virol Methods. 195:123–125. 2014.
View Article : Google Scholar
|
|
3
|
Bao CJ, Cui LB, Zhou MH, Hong L, Gao GF
and Wang H: Live-animal markets and influenza A (H7N9) virus
infection. N Engl J Med. 368:2337–2339. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wiwanitkit S and Wiwanitkit V: Effective
strategy for managing H7N9 virus infection. Infection. 42:2292014.
View Article : Google Scholar
|
|
5
|
Chen Y, Liang W, Yang S, et al: Human
infections with the emerging avian influenza A H7N9 virus from wet
market poultry: clinical analysis and characterisation of viral
genome. Lancet. 381:1916–1925. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shi J, Xie J, He Z, et al: A detailed
epidemiological and clinical description of 6 human cases of
avian-origin influenza A (H7N9) virus infection in Shanghai. PLoS
One. 8:e776512013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dortmans JC, Dekkers J, Wickramasinghe IN,
et al: Adaptation of novel H7N9 influenza A virus to human
receptors. Sci Rep. 3:30582013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Qiao JG, Zhang L, Tong YH, Xie W, Shi JD
and Yang QM: Management of the first confirmed case of avian
influenza A H7N9. Respir Care. 59:e43–e46. 2014. View Article : Google Scholar
|
|
9
|
Cao B and Hayden FG: Therapy of H7N9
pneumonia: current perspectives. Expert Rev Anti Infect Ther.
11:1123–1126. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dudley JP and Mackay IM: Age-specific and
sex-specific morbidity and mortality from avian influenza A (H7N9).
J Clin Virol. 58:568–570. 2013. View Article : Google Scholar : PubMed/NCBI
|