Introduction
Turner syndrome is a chromosomal abnormality,
affecting one in 2,000 female live-births (1). X-chromosome monosomy (45XO karyotype)
accounts for >55% of Turner syndrome cases. Mosaicism,
represented mainly by 45XO/46XX or 45XO/47XXX, has been detected in
the remaining cases, with only 1–4% of the reported cases being
45XO/47XXX (2,3).
Patients with Turner syndrome present with a number
of symptoms, including short stature, gonadal failure, broad chest,
low hair-line, low-set ears and a webbed neck. Medical problems
associated with Turner syndrome include congenital heart disease,
hypothyroidism, diabetes, vision and hearing problems, cognitive
deficits and autoimmune diseases. Mosaics with a normal cell line
or an extra X chromosome tend to exhibit a milder phenotype. In
addition, patients with 45XO/47XXX may not develop mental or
behavioral problems and have a higher fertility rate (4). A previous study reported a case of
congenital adrenal hyperplasia associated with Turner syndrome
(5).
Insulinomas are the most common type of functioning
pancreatic neuroendocrine tumor (PNET), with an incidence of two to
four cases per million individuals each year. Insulinomas usually
result in recurrent episodes of fasting hypoglycemia and tend to be
small with no mass effect (6).
Although insulinomas are often sporadic, they account for 10–30% of
functioning PNETs in patients with multiple endocrine neoplasia
type 1. In addition, these tumors have been reported in patients
with neurofibromatosis type 1 (7,8).
However, insulinomas have not been previously reported in patients
with mosaic 45XO/47XXX Turner syndrome or other forms of Turner
syndrome. To the best of our knowledge, the present study reports
the first case of a pathologically confirmed insulinoma in a
patient with mosaic 45XO/47XXX Turner syndrome. Due to the rarity
of the two diseases, the current case may represent a previously
unrecognized association.
Case report
The present case study was approved by the Ethics
Committee of PLA General Hospital (Beijing, China), and informed
consent was obtained from the patient. A 30-year-old female
presented with ‘episodic dizziness, sweating and loss of
consciousness’ in April 2012. The patient was admitted to the
Chinese PLA General Hospital (Beijing, China) with deteriorating
symptoms. The patient was found to suffer from fasting
hyperinsulinemic hypoglycemia (blood glucose, 2.8 mmol/l), which
improved following the ingestion food high in glucose. Within the
13-month period following the initial onset of symptoms, the
patient gained ~5 kg.
Medical history review revealed an allergy to iodine
contrast dye. The patient experienced menarche at the age of 13
years and had regular monthly menses until the age of 23 years.
Despite treatment with progesterone and estrogen, the last
spontaneous menstrual period of the patient was on the
10th of December 2011. The patient had been sexually
active from the age of 23 years, but did not conceive despite
regular unprotected sexual activity. In addition, the female was a
labor worker and did not smoke or drink alcohol. There was no
family history of Turner syndrome or other genetic diseases, with
the exception of a parent having short limbs.
Physical examination revealed a short stature (152
cm), a webbed neck, short limbs, an abnormal upper-to-lower segment
ratio, a low posterior hair line with acanthosis nigricans behind
the neck and a body mass index of 33.3 kg/m2. External
examination of the patient’s genitalia revealed no abnormalities, a
smooth vagina and a small uterus that was positioned forward, but
was movable without tenderness. The female was found to have an IQ
within an average range according to the Wechsler Adult
Intelligence Scale (9).
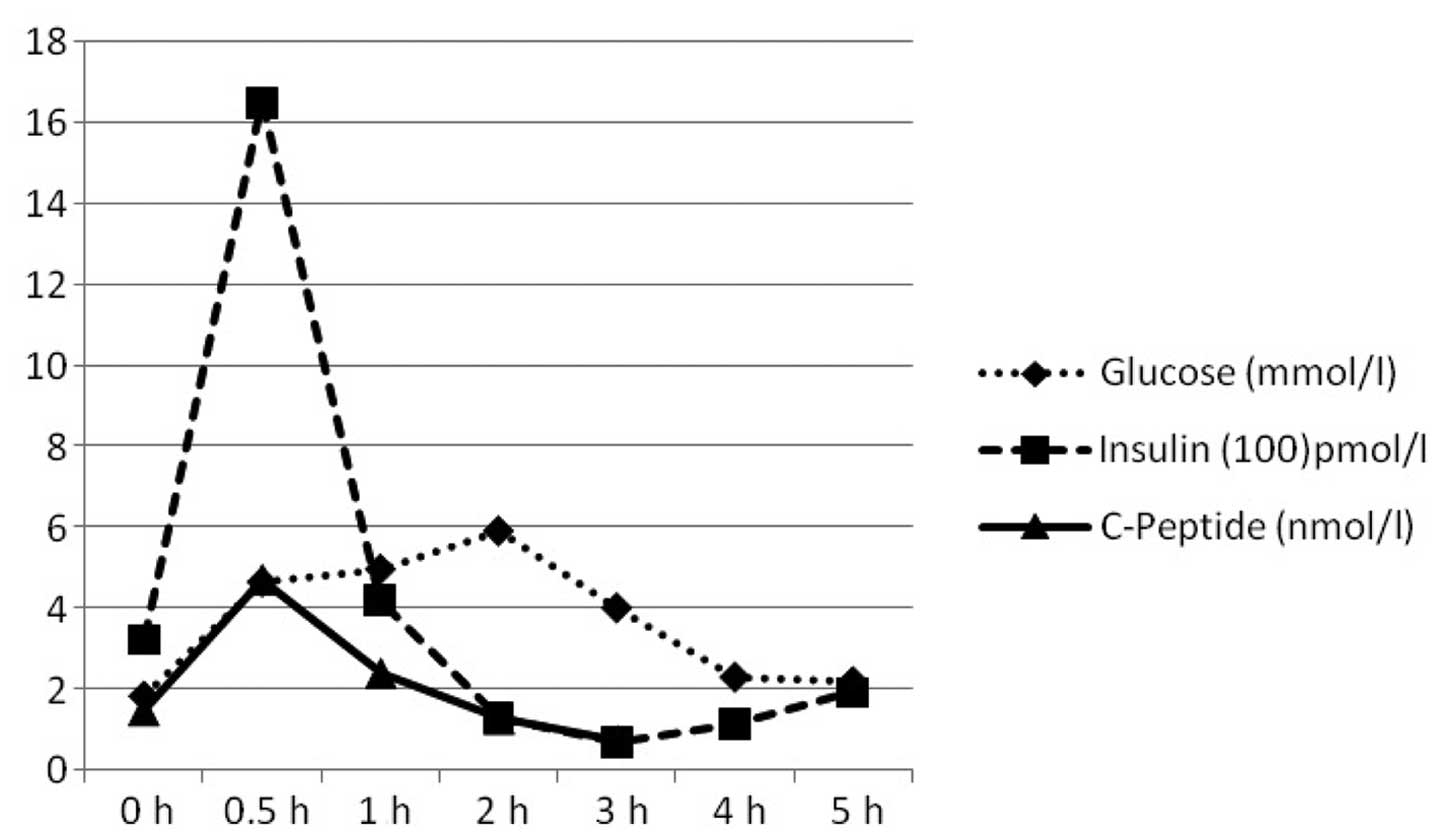
The patient was subjected to an oral glucose
tolerance test, where 75 g glucose was administered and blood
samples were obtained at baseline, 0.5, 1, 2, 3, 4 and 5 h to
detect the serum levels of glucose, insulin and C-peptide. Serum
results revealed that the fasting serum glucose level was low,
while the levels of insulin and C-peptide were high (Fig. 1). The inulin/glucose ratio was
consistently >0.3, indicating the possibility of an
insulinoma.
The estrogen level was found to be slightly
decreased, whereas the follicle-stimulating hormone and luteinizing
hormone levels were slightly elevated. In addition, the levels of
thyroid hormone, thyroid-stimulating hormone and growth hormone in
the patient were found to be normal. Furthermore, the patient’s
cortisol level was slightly reduced at 8 am, while the
adrenocorticotropic hormone level was slightly elevated. Antibodies
for insulin or islet cells were not detected. A magnetic resonance
imaging scan revealed a normal pituitary gland, and the chest X-ray
scan appeared to be normal. An ultrasound scan demonstrated that
the left ovary was 1.4×0.9×0.6 cm3, the right ovary was
1.3×0.5×1.0 cm3 and the two ovaries were streak-like,
without visible follicles.
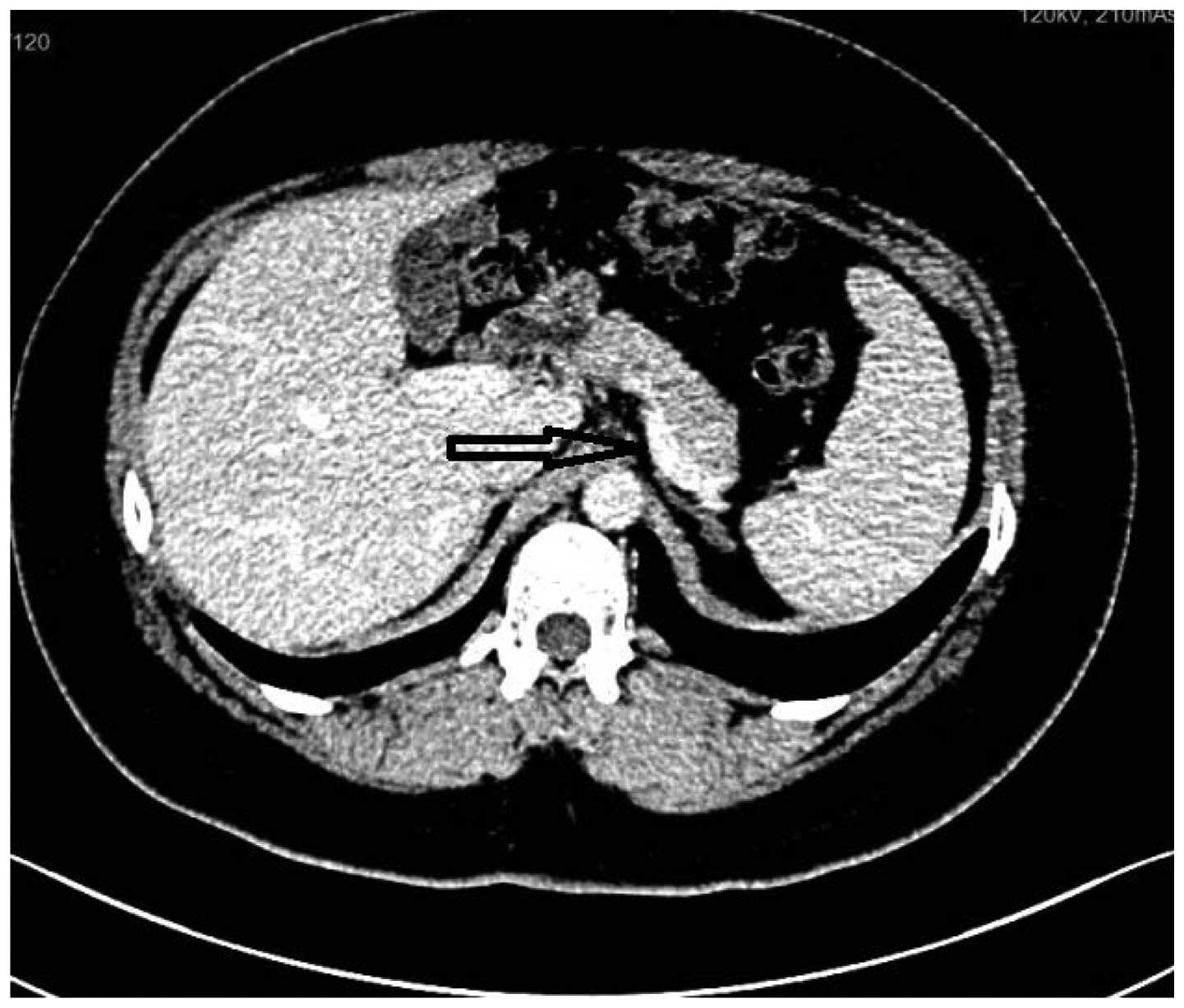
An endoscopic ultrasound revealed a low-echo, dense
lesion at the junction of the pancreas body and tail, with
dimensions of 2.0×1.28 cm2. The observations were
confirmed with ultrasonic angiography and enhanced computed
tomography scanning of the pancreas, indicating the possibility of
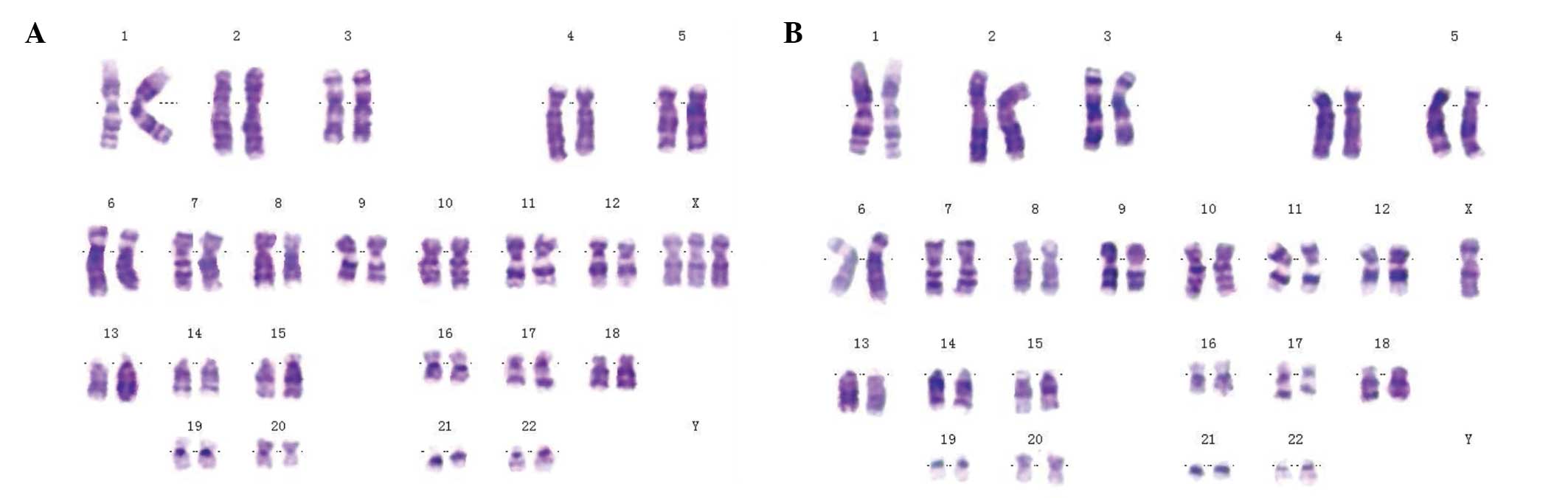
an insulinoma (Fig. 2). The
karyotype of the patient was found to be 45XO/47XXX from a whole
blood sample, with 68% 45XO and 32% 47XXX (Fig. 3).
Subsequently, the patient was transferred to the
Department of Surgery at the Chinese PLA General Hospital and the
lesion was removed under general anesthesia per standard protocol
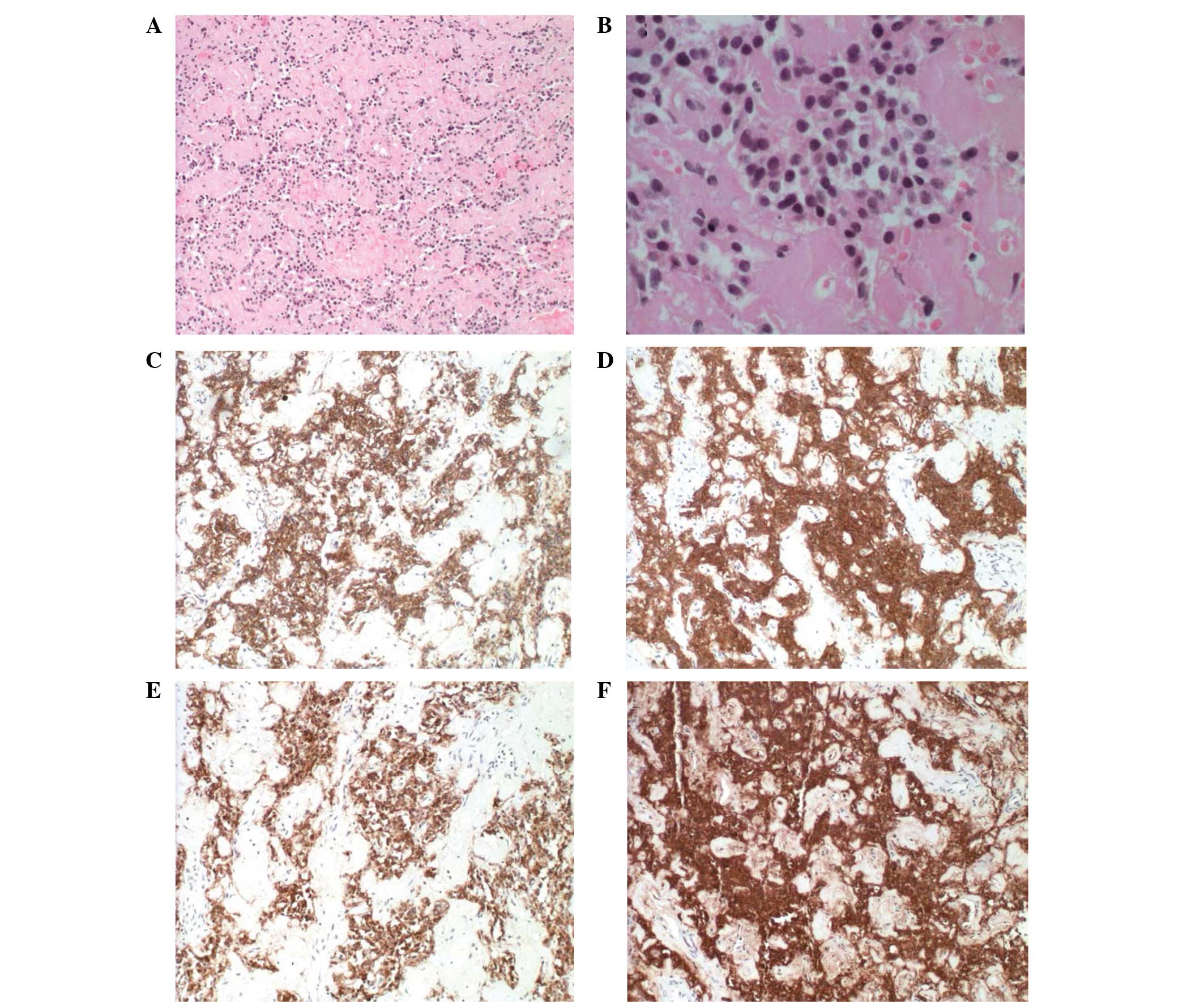
(10). Pathological examination
revealed a grade 1 neuroendocrine lesion that was
well-differentiated. Immunochemical staining revealed that the
tumor was positive for synaptophysin (+++), CD56 (++), insulin
(++), creatine kinase (+) and β-catinin (++), but negative for
glucagon (−), CD10 (−) and Ki-67 (Fig.
4). Immediately following surgical removal of the insulinoma,
the blood glucose level of the patient increased to 9.19 mmol/l,
which was reduced to 6.0 mmol/l within four days of surgery. The
patient’s symptoms were markedly resolved following surgery.
Discussion
To the best of our knowledge, the present study is
the first case report of an insulinoma in an individual with
45XO/47XXX mosaic Turner syndrome.
An increased number of X chromosomes has been shown
to reduce the extent of ovarian failure and create a period of
potential fertility (4,11–13).
The patient in the present case study experienced normal menses for
~10 years, between the age of 13 and 23 years. For patients with
mosaic Turner syndrome, during the time in which they have normal
menstruation, they may be fertile (14–16).
Turner syndrome is commonly associated with diabetes
and insulin resistance. Although a previous study supports the
genetic basis for the declined β-cell function, the exact mechanism
of the disease remains unclear (17). Hypoglycemia in Turner syndrome is
rare. A previous case study reported the case of an infant with
Turner syndrome who suffered from hypoglycemia due to a growth
hormone deficiency (18,19). By contrast, the patient in the
present study showed a normal growth hormone level.
Insulinomas and Turner syndrome are relatively rare
conditions. The occurrence of two rare conditions simultaneously
may be due to coincidence. However, since insulinomas and mosaic
Turner syndrome are caused by changes to the same allele on
chromosome 11, a true association may exist that has not been
previously recognized. In the case that a patient presents with
fasting hypoglycemia, the possibility of an insulinoma should be
always considered. However, the convergence of the two rare
conditions should sensitize the consideration that in the context
of mosiac Turner syndrome, an insulinoma may be more common.
References
|
1
|
Improda N, Rezzuto M, Alfano S, Parenti G,
Vajro P, Pignata C and Salerno M: Precocious puberty in Turner
Syndrome: report of a case and review of the literature. Ital J
Pediatr. 38:542012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Abir R, Fisch B, Nahum R, Orvieto R, Nitke
S and Ben Rafael Z: Turner’s syndrome and fertility: current status
and possible putative prospects. Hum Reprod Update. 7:603–610.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bouchlariotou S, Tsikouras P, Dimitraki M,
Athanasiadis A, Papoulidis I, Maroulis G, Liberis A and Liberis V:
Turner’s syndrome and pregnancy: has the 45,X/47,XXX mosaicism a
different prognosis? Own clinical experience and literature review.
J Matern Fetal Neonatal Med. 24:668–672. 2011. View Article : Google Scholar
|
|
4
|
Zhong Q and Layman LC: Genetic
considerations in the patient with Turner syndrome - 45,X with or
without mosaicism. Fertil Steril. 98:775–779. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kendirci HN, Aycan Z, Çetinkaya S, Baş VN,
Ağladıoğlu SY and Önder A: A rare combination: congenital adrenal
hyperplasia due to 21 hydroxylase deficiency and Turner syndrome. J
Clin Res Pediatr Endocrinol. 4:213–215. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Batcher E, Madaj P and Gianoukakis AG:
Pancreatic neuroendocrine tumors. Endocr Res. 36:35–43. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lewis RB, Lattin GE Jr and Paal E:
Pancreatic endocrine tumors: radiologic-clinicopathologic
correlation. Radiographics. 30:1445–1464. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jonnakuty C and Gragnoli C: Karyotype of
the human insulinoma CM cell line - beta cell model in vitro? J
Cell Physiol. 213:661–662. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Girard TA, Axelrod BN, Patel R and
Crawford JR: Wechsler adult intelligence scale-IV dyads for
estimating global intelligence. Assessment: Sep 29, 2014 (Epub
ahead of print).
|
|
10
|
Thomson AJ, Morrison G, Thomson E, Beattie
C, Nimmo AF and Glen JB: Induction of general anaesthesia by
effect-site target-controlled infusion of propofol: influence of
pharmacokinetic model and ke0 value. Anaesthesia. 69:429–435. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mauras N, Torres-Santiago L, Taboada M and
Santen R: Estrogen therapy in Turner syndrome: does the type, dose
and mode of delivery matter? Pediatr Endocrinol Rev. 9(Suppl 2):
718–722. 2012.PubMed/NCBI
|
|
12
|
Cho SY, Ki CS, Jang JH, Sohn YB, Park SW,
Kim SH, Kim SJ and Jin DK: Familial Xp22.33-Xp22.12 deletion
delineated by chromosomal microarray analysis causes proportionate
short stature. Am J Med Genet A. 158A:1462–1466. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Burégio-Frota P, Valença L, Leal GF,
Duarte AR, Bispo-Brito AV, Soares-Ventura EM, Marques-Salles TJ,
Nogueira MT, Muniz MT, Silva ML, Hunstig F, Liehr T and Santos N:
Identification of a de novo inv dup(X)(pter--> q22) by
multicolor banding in a girl with Turner syndrome. Genet Mol Res.
9:780–784. 2010. View Article : Google Scholar
|
|
14
|
Karnis MF: Fertility, pregnancy, and
medical management of Turner syndrome in the reproductive years.
Fertil Steril. 98:787–791. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hovatta O: Ovarian function and in vitro
fertilization (IVF) in Turner syndrome. Pediatr Endocrinol Rev.
9(Suppl 2): 713–717. 2012.PubMed/NCBI
|
|
16
|
Chetty SP, Shaffer BL and Norton ME:
Management of pregnancy in women with genetic disorders: Part 2:
Inborn errors of metabolism, cystic fibrosis, neurofibromatosis
type 1, and Turner syndrome in pregnancy. Obstet Gynecol Surv.
66:765–776. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hjerrild BE, Holst JJ, Juhl CB,
Christiansen JS, Schmitz O and Gravholt CH: Delayed β-cell response
and glucose intolerance in young women with Turner syndrome. BMC
Endocr Disord. 11:62011. View Article : Google Scholar
|
|
18
|
Bonfig W, Salem NJ, Heiliger K, Hempel M,
Lederer G, Bornkamm M, Wieland K, Lohse P, Burdach S and Oexle K:
Recurrent hypoglycemia due to growth hormone deficiency in an
infant with Turner syndrome. J Pediatr Endocrinol Metab.
25:991–995. 2012.
|
|
19
|
O’Gorman CS, Syme C, Lang J, Bradley TJ,
Wells GD and Hamilton JK: An evaluation of early cardiometabolic
risk factors in children and adolescents with Turner syndrome. Clin
Endocrinol (Oxf). 78:907–913. 2013. View Article : Google Scholar
|