Introduction
Major cardiac surgery patients are a particularly
high-risk population for nosocomial infections (1). Ventilator-associated pneumonia (VAP)
is the primary infectious complication for cardiac surgery patients
(2) and is associated with a
marked increase in morbidity and mortality rates (3). The prevalence of VAP following
cardiac surgery is estimated to be 17.9% in patients who receive
mechanical ventilation for >48 h and 28.8% in patients who
undergo mechanical ventilation for >72 h (4). The median mechanical ventilation time
and duration of hospital stay are significantly prolonged in
patients who develop VAP following cardiac surgery (5). Tamayo et al determined that
cardiac surgery patients who develop VAP have a mortality risk that
is 8.53 times higher than those without VAP (6). In addition, the authors showed that
VAP is the most important independent risk factor for mortality
following major cardiac surgery. Therefore, early prevention,
diagnosis and treatment of VAP is essential.
Procalcitonin (PCT), a protein of 116 amino acids
with a molecular weight of 13 kDa, is the precursor molecule of
calcitonin. PCT is usually produced by parafollicular cells in the
thyroid gland (7). Since PCT
levels were found to be elevated in patients with bacterial
infection, increasing interest has been directed at the possibility
of using PCT as an indicator of infection (7–9). In
addition, PCT has been shown to be useful in discriminating between
septic and nonseptic inflammation and may be a promising biomarker
for the diagnosis of VAP (10).
However, cardiac surgery and the use of cardiopulmonary bypass
(CPB) may activate the immune system and lead to a systemic
inflammatory response, which increases the difficulty of
identifying infectious complications in cardiac surgery patients.
Furthermore, CPB and noninfectious complications, such as organ
dysfunction/failure, contribute to increased PCT levels (11). Therefore, the value of PCT as a
diagnostic marker of infection in cardiac surgery remains
controversial. Adib-Conquy et al (12) showed that PCT is not specifically a
marker for infection, as PCT levels may increase markedly in cases
of acute inflammation with no infection. In addition, Sinning et
al (13) suggested that
systemic inflammatory response syndrome (SIRS) is associated with
PCT in patients with a transcatheter aortic valve implantation.
Therefore, the feasibility of using PCT as a diagnostic marker for
VAP in cardiac surgery patients remains unclear and requires
further study.
The present study examined 92 patients who received
≥48 h of mechanical ventilation following cardiac surgery. The
patient serum levels of PCT, interleukin (IL)-6 and C-reactive
protein (CRP) were analyzed using an electrochemiluminescence
immunoassay (ECLIA). The incidence and type of postoperative
noninfectious complications in the patients were also recorded. In
addition, the diagnostic values of serum levels of PCT, IL-6 and
CRP were analyzed by linear regression.
Materials and methods
Patients
The study was conducted at the intensive care unit
(ICU) of the Department of Cardiothoracic Surgery at the Second
Xiangya Hospital of Central South University (Changsha, China). In
total, 92 consecutive patients (age, ≥18 years) who had received
≥48 h of mechanical ventilation were recruited between January 2012
and June 2013. All the patients had undergone elective cardiac
surgery with CPB. Patients were excluded from the study if they had
been diagnosed with pneumonia prior to the mechanical ventilation,
were pregnant, had received immunosuppressants or long-term
corticosteroid therapy or had a coexisting extrapulmonary infection
that required antibiotic therapy for more than three days prior to
or following the cardiac surgery. The patients were divided into
VAP and non-VAP patient groups.
The study protocol was approved by the Ethics
Committee of the Second Xiangya Hospital of Central South
University, and patients provided written informed consent.
Diagnosis of VAP and classification of
complications
The study focused on patients in the early stages of
VAP that had been diagnosed between 48 h and six days after
initiation of the mechanical ventilation. Diagnosis of VAP
(14) was determined using a novel
criteria, based on chest X-ray results, with at least two of the
following features: Fever with a body temperature of >38°C; a
white blood cell count of >11,000 or <3,000/μl; or the
presence of purulent endotracheal secretions. Microbiological
samples were obtained by fibroscopic bronchoalveolar lavage (BAL),
and the growth of ≥104 colony-forming units/ml
microorganism culture of BAL was considered to be positive.
A number of noninfectious complications were defined
according to specific criteria. Cardiovascular complications were
defined as a low cardiac output with a cardiac index of <2.0
l/min/m2, postoperative myocardial infarction and
malignant ventricular arrhythmia (sustained and requiring further
treatment). Pulmonary dysfunction was diagnosed if the
PaO2/FiO2 ratio was <200 mmHg, unless this
was caused by cardiogenic factors. Acute renal failure was defined
as requiring temporary hemofiltration or hemodialysis, while
neurological complications included stroke and ischemic cerebral
infarction. Finally, rethoracotomy due to bleeding was a potential
noninfectious complication.
Data collection
Follow-up lasted for seven days or until patient
mortality. Patient characteristics and clinical data, including the
age, gender, preoperative diagnosis, left ventricular ejection
fraction, brain natriuretic peptide level, type of surgery, CPB
time, aortic cross-clamp time, mechanical ventilation time, length
of ICU stay and diagnosis of noninfectious complications, were
collected.
Biological measurements and sequential
organ failure assessment (SOFA)
Blood samples were collected prior to cardiac
surgery in order to define the baseline biological measurement
values. Patients were evaluated daily for symptoms of VAP. Once VAP
was diagnosed (defined as day 1), the patients received empirical
antibiotic treatment until the results of the bacterial culture
were available. In the non-VAP group, day 1 was defined as the day
when the tracheal intubation was removed from each patient. The
levels of PCT, IL-6 and CRP were measured using an ECLIA (Roche
Diagnostics GmbH, Mannheim, Germany) for the patients in the VAP
and non-VAP groups on days 1, 3, 5 and 7.
SOFA was conducted on days 1 and 7 for the patients
in the VAP and non-VAP groups (15).
Statistical analysis
Data are presented as the mean ± standard deviation
and statistical analysis was performed using SPSS 16.0 software
(SPSS, Inc., Chicago, IL, USA). Comparisons between the groups were
conducted using the Student’s t-test, the Mann-Whitney test or
Fisher’s exact method. Receiver operating characteristic (ROC)
curves were used to determine the optimum threshold values for
sensitivity and specificity. Correlations were analyzed using
Pearson’s correlation coefficient. Two-tailed P-values of <0.05
were considered to indicate a statistically significant
difference.
Results
Preoperative and postoperative patient
characteristics
A total of 92 patients, including 59 non-VAP
patients and 33 VAP patients, were included in the prospective
cohort study. Detailed preoperative and postoperative
characteristics of the VAP and non-VAP patients are summarized in
Table I. There were no
statistically significant differences in preoperative
characteristics between the VAP and non-VAP group patients. In
addition, no statistically significant difference was observed in
the occurrence of postoperative complications between the VAP and
non-VAP patients (33/33 vs. 53/59, P=0.058). There were six
patients in the VAP group and four in the non-VAP group who
suffered from multiple noninfectious postoperative complications.
The SOFA scores on days 1 and 7 were significantly higher in the
VAP group when compared with the non-VAP group (P<0.001).
Furthermore, the durations of ICU stay (P=0.001) and mechanical
ventilation (P<0.001) were longer in the VAP group when compared
with the non-VAP group.
 | Table IPreoperative and postoperative
characteristics of patients in the non-VAP and VAP groups. |
Table I
Preoperative and postoperative
characteristics of patients in the non-VAP and VAP groups.
| Characteristic | Non-VAP group
(n=59) | VAP group (n=33) | P-value |
|---|
| aAge (years) | 47±11 | 50±13 | NS |
| Gender, male/female
(n) | 29/30 | 18/15 | NS |
| Type of surgery
(n) | | | - |
| Valve surgery | 32 | 10 | - |
| Coronary artery
bypass grafting | 13 | 6 | - |
| Ascending aortic
surgery | 8 | 8 | - |
| Combined
surgery | 4 | 7 | - |
| Others | 2 | 2 | - |
| Comorbidities
(n) | | | - |
| Hypertension | 31 | 10 | - |
| Diabetes
mellitus | 10 | 4 | - |
| Pulmonary
diseases | 6 | 4 | - |
| Kidney disease | 0 | 2 | - |
| Others | 6 | 5 | - |
| aLVEF (%) | 61±13 | 63±9 | NS |
| aBaseline biological measurements |
| PCT (ng/ml) | 0.11±0.09 | 0.20±0.21 | NS |
| IL-6 (pg/ml) | 8.44±4.32 | 9.58±5.35 | NS |
| CRP (ng/ml) | 10.18±8.04 | 12.33±0.76 | NS |
| aCPB duration (min) | 118±48 | 156±94 | NS |
| aAortic cross clamping time (min) | 66±23 | 71±41 | NS |
| aMechanical ventilation duration
(days) | 3±2 | 6±3 | 0.000 |
| aLength of stay in the ICU (days) | 8±6 | 12±9 | 0.001 |
| Postoperative
complication (n) | 53 | 33 | NS |
| Cardiovascular
complication (n) | 47 | 26 | - |
| Pulmonary
dysfunction (n) | 3 | 4 | - |
| Neurological
complication (n) | 0 | 2 | - |
| Reoperation due to
bleeding (n) | 6 | 3 | - |
| AKI requiring RRT
(n) | 1 | 3 | - |
| aSOFA on day 1 | 9±3 | 11±2 | <0.001 |
| aSOFA on day 7 | 3±1 | 7±4 | <0.001 |
| Mortality (n) | 3 | 7 | 0.02 |
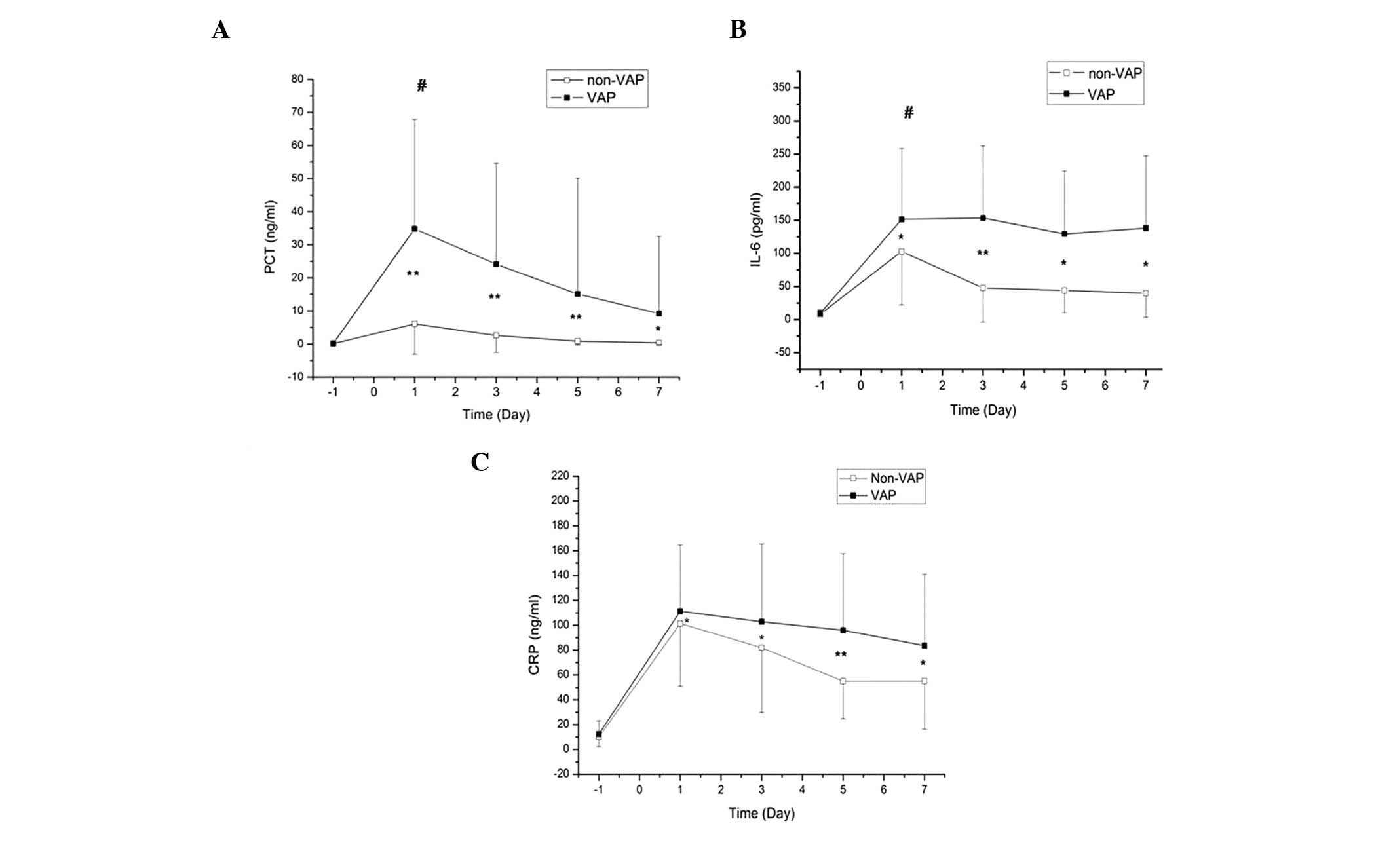
Serum PCT, CRP and IL-6 levels
Preoperative and postoperative (days 1, 3, 5 and 7)
serum PCT, IL-6 and CRP levels were compared between patients in
the VAP and non-VAP groups (Fig.
1). No statistically significant differences were observed in
the preoperative serum levels of PCT, IL-6 and CRP between the VAP
and non-VAP groups (P>0.05). However, the serum levels of PCT,
IL-6 and CRP in the VAP and non-VAP groups were significantly
higher on days 1, 3, 5 and 7 when compared with the preoperative
baseline levels (P<0.05). Levels of PCT and IL-6 on day 1 were
significantly higher in the VAP group when compared with the
non-VAP group (P<0.05), while there was no statistically
significant difference in the CRP levels between the groups on day
1 (P>0.05).
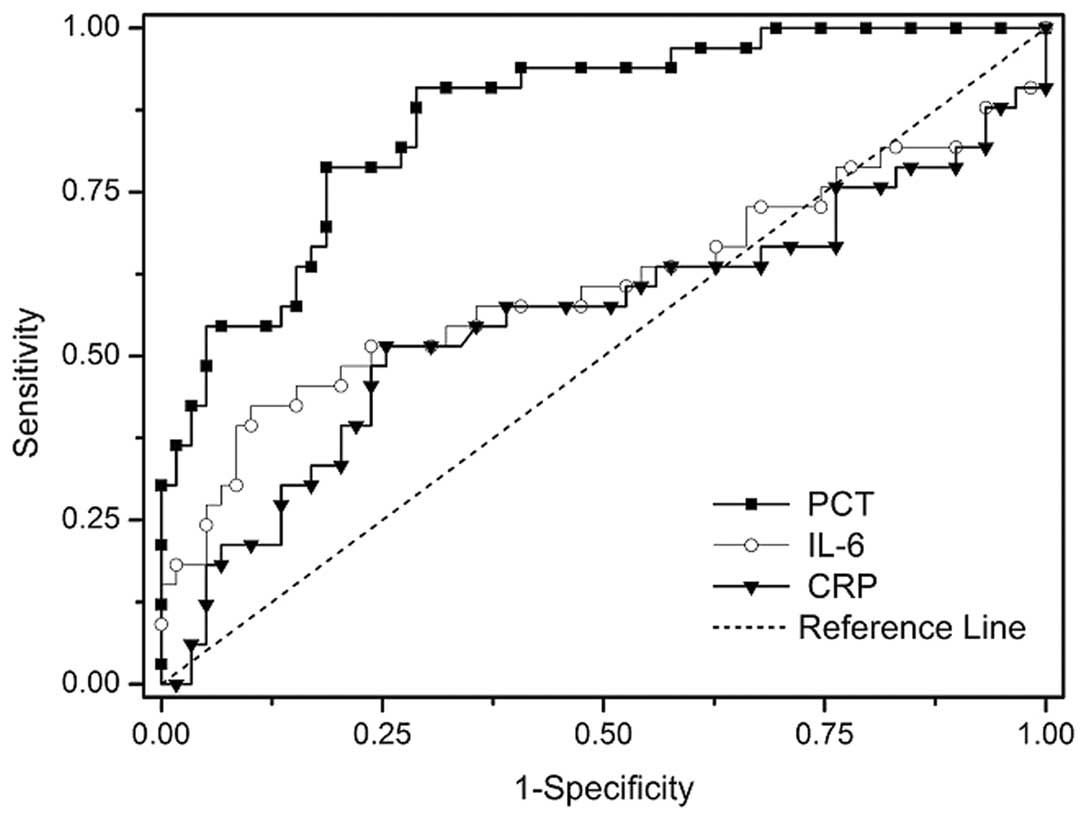
Diagnostic value of serum PCT, IL-6 and
CRP levels
Using the ROC curves, it was concluded that the
optimum PCT cut-off value for VAP diagnosis on day 1 was 5.0 ng/ml,
with a sensitivity of 91% and a specificity of 71%. The areas under
the ROC curve were 0.87, 0.61 and 0.56 for PCT, IL-6 and CRP,
respectively (Table II; Fig. 2).
| Table IIDiagnostic value of serum levels of
PCT, IL-6 and CRP on day 1. |
Table II
Diagnostic value of serum levels of
PCT, IL-6 and CRP on day 1.
| Protein | Optimal
cut-off | AUC | Sensitivity
(%) | Specificity
(%) | PPV (%) | NPV (%) |
|---|
| PCT | 5.0 ng/ml | 0.87 | 91 | 71 | 64 | 93 |
| IL-6 | 70.8 pg/ml | 0.61 | 58 | 64 | 48 | 73 |
| CRP | 108.3 ng/ml | 0.56 | 52 | 74 | 52 | 73 |
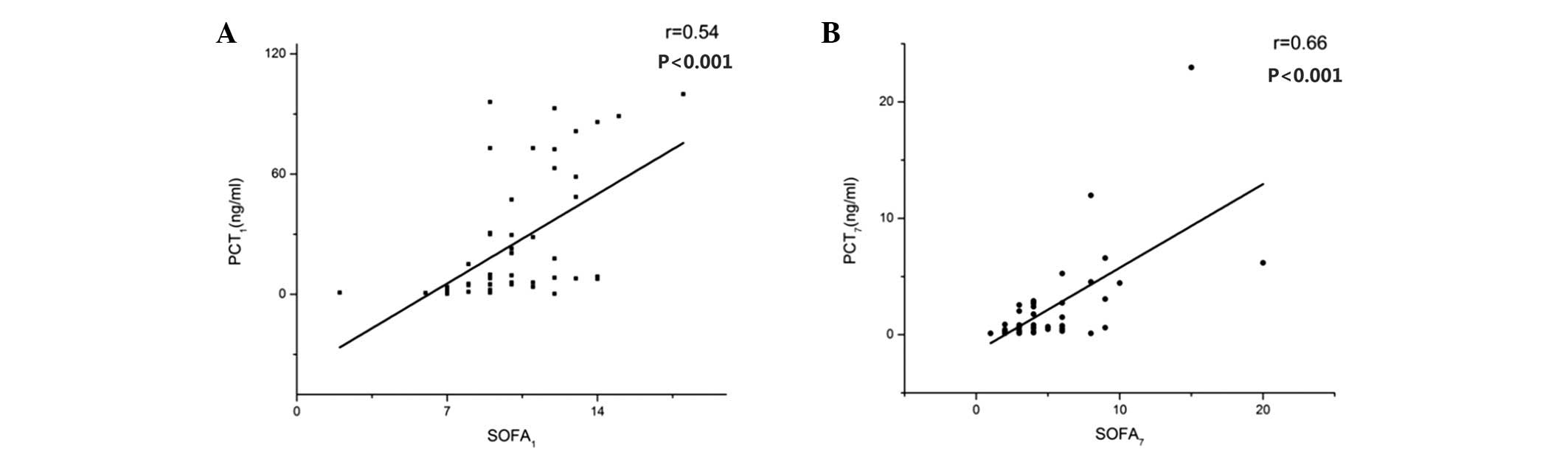
Linear correlation analysis
Associations between the serum levels of PCT, IL-6
and CRP in the VAP patients and the corresponding SOFA scores on
days 1 and 7 were analyzed using linear correlation analysis. The
PCT levels on days 1 and 7 correlated positively with the SOFA
scores (r=0.54, P<0.001 and r=0.66, P<0.001, respectively;
Fig. 3), while the levels of IL-6
and CRP were not found to correlate with the SOFA scores
(P>0.05). There were no statistically significant linear
correlations between the serum levels of PCT, IL-6 and CRP
(P>0.05).
Discussion
Although numerous studies have reported the use of
serum PCT as a marker for VAP (16–18),
the results have been contradictory. In the present study, the
serum levels of PCT, IL-6 and CRP were measured in VAP and non-VAP
cardiac surgery patients. The optimum PCT cut-off value for VAP
diagnosis on day 1 was 5.0 ng/ml, with a sensitivity of 91% and a
specificity of 71%. Furthermore, the serum levels of PCT were shown
to correlate positively with the SOFA scores on days 1 and 7.
Therefore, serum PCT may be used as a diagnostic marker for VAP in
patients following cardiac surgery.
Duflo et al (16) found that serum levels of PCT
increased significantly in VAP patients when compared with non-VAP
patients until day 3. The optimum cut-off value of serum PCT for
the diagnosis of VAP was 3.9 ng/ml, with a low sensitivity of 41%,
but an excellent specificity of 100%. Oppert et al (17) studied 28 patients who exhibited a
spontaneous return in circulation following cardiac arrest and
determined the optimum serum PCT cut-off value to be 1 ng/ml, with
a sensitivity of 100% and a specificity of 75% for VAP diagnosis.
However, a study of 73 suspected VAP patients by Luyt et al
(18) found PCT to be a poor
marker for VAP, with a sensitivity of 72% and a specificity of only
24%, at a cut-off level of 0.5 ng/ml. Mixed ICU, early- or
late-onset of VAP and the use of antibiotics in advance of
diagnosis may lead to decreased sensitivity or specificity. In the
study by Luyt et al, preinfected patients were not excluded,
while in the study by Oppert et al, only 10 cases among 12
patients exhibited early-onset VAP. Furthermore, the population
assessed in the study by Duflo et al consisted of late-onset
VAP patients who had received over two years of ventilation. These
factors may have caused underestimation or overestimation of the
diagnostic value of PCT, which may account for the discrepancies
among previous findings. In the present study, all the patients
exhibited early-onset VAP following cardiac surgery, which ensured
that the subjects were selected from a homogeneous patient
population.
Numerous studies have shown that cardiac surgery and
CPB may affect the serum levels of various biomarkers, including
PCT, CRP, IL-6 and IL-8 (19,20).
Among these proteins, PCT in particular is considered to be closely
associated with infection conditions. In the absence of a bacterial
infection, SIRS caused by surgery or CPB is an important factor in
the stimulation of PCT expression (13). Cardiac surgery and CPB result in
the exposure of blood vessels to nonphysiological surfaces, the
translocation of endotoxin and the release of cytokines, such as
IL-6, all of which have been shown to induce PCT (13). However, numerous studies (20–22)
have indicated that the CPB procedure itself causes only a
moderate, transient postoperative increase in PCT levels. PCT
levels peaked on days 1 or 2 following surgery and decreased
continuously to a normal value, with the peak value not generally
exceeding 2 ng/ml (22).
Therefore, Jebali et al suggested that the diagnostic
properties of PCT may not be evident during the first two days
following surgery (23). Diagnosis
of VAP using PCT as a biomarker requires the patient to undergo
mechanical ventilation for >48 h. However, all the subjects in
the present study were postoperative patients who had been using a
tracheal intubation for over two days; thus, the CPB-induced
postoperative peak in PCT levels was avoided. Therefore, this
experiment did not consider the impact of mechanical ventilation
time.
Markedly increased levels of PCT are primarily
associated with postoperative complications, including low cardiac
output syndrome, perioperative myocardial infarction, pulmonary
dysfunction, renal failure and infection (23). Prat et al (24) found that PCT levels were
significantly higher in 15 patients with infectious or
noninfectious complications compared with patients who recovered
without complications. The optimum cut-off value of PCT on the
first postoperative day was 2 ng/ml, with a sensitivity of 92.3%
and a specificity of 93.8%. Sponholz et al (11) suggested that PCT levels were
significantly higher in patients with postoperative infection when
compared with those in noninfected patients. Therefore, continuous
monitoring of the serum PCT levels was the most effective approach
for diagnosing postoperative infection.
Although the observation period began after >48 h
of postoperative intubation in the present study, there remained
44/59 patients with PCT levels of >2 ng/ml in the non-VAP group,
and all the patients in the VAP group had PCT levels of >2 ng/ml
(33/33). According to the aforementioned criteria, all the patients
in the VAP group exhibited noninfectious complications and there
were no statistically significant differences when compared with
the non-VAP group (53/59). However, the SOFA scores of the patients
in the VAP group were notably higher when compared with the non-VAP
group. A previous study demonstrated that higher SOFA scores were
associated with significantly higher serum PCT concentrations
during the course of multiple organ dysfunction syndrome (MODS) and
sepsis (25). In addition, Haasper
et al (26) showed that the
presence of significantly higher levels of PCT in patients resulted
in the development of MODS. Differences in SOFA scores may increase
the levels of PCT in the VAP group to a greater extent compared
with the non-VAP group, which may indirectly increase the
diagnostic accuracy of VAP. In the present study, the postoperative
PCT levels in the VAP group were significantly higher when compared
with the non-VAP group during the observation period. PCT levels of
>5 ng/ml had a sensitivity of 91.2% and a specificity of 82.4%,
respectively. A study by Ramirez et al (27) examined 44 patients who received
mechanical ventilation for >48 h in a medical ICU, of which 20
patients were suspected of having VAP. Based on a pathological
examination, nine individuals were diagnosed with VAP, while 11
patients were assigned to the non-VAP group. On the day of VAP
diagnosis confirmation, serum PCT levels and SOFA scores in the VAP
group were significantly higher compared with those in the non-VAP
group. The optimum cut-off value of PCT was 2.99 ng/ml, with a
sensitivity of 78% and a specificity of 97%. The optimum serum PCT
cut-off value in the present study was higher (5 ng/ml) when
compared with the results of Oppert et al (17) and Ramirez et al (27), which may be due to the recruitment
of patients from the cardiac surgery ICU, exhibiting more serious
conditions and postoperative complications and higher SOFA
scores.
According to a previous study, IL-6 is a cytokine
secreted by giant eosinophilic cells that participates in the acute
inflammatory process (28). IL-6
levels are known to increase in cardiac surgery and may be involved
in the postoperative cytokine cascade (29). CRP synthesized in the liver is a
nonspecific biological marker for inflammation (30). Jebali et al showed that
serum IL-6 was not a marker for postoperative complications
following cardiac surgery (23).
However, the use of CRP for the diagnosis of VAP remains
controversial. Póvoa et al (30) showed that a CRP level of >960
mg/l provided a good accuracy for VAP diagnosis, with a sensitivity
of 87% and a specificity of 88%. In the present study, serum levels
of CRP in the VAP and non-VAP groups did not show a statistically
significant difference until three days following the diagnosis of
VAP, and CRP exhibited no diagnostic value on day 1. The optimum
cut-off value of IL-6 for VAP diagnosis was 70.8 pg/ml; however,
the diagnostic accuracy was relatively low, with a sensitivity of
58% and a specificity of 64%. These results indicated that IL-6 and
CRP were not effective for the diagnosis of VAP following cardiac
surgery with CPB. Although IL-6 has been demonstrated to induce the
production of PCT in vitro (26), no correlation was found between the
levels of IL-6 and PCT.
There were a number of limitations to the present
study. Firstly, the sample size was relatively small, which may
have affected the diagnostic capability of PCT. Thus, further
studies with a larger sample size are required to verify the
results. Secondly, the present study examined only patients with
early-onset VAP who had undergone elective cardiac surgery.
Therefore, the results may differ from other studies that included
early-onset VAP patients who were recruited from a noncardiac
surgical ICU or cardiac surgery patients with late-onset VAP.
Finally, the effects of surgery and CPB on serum levels of PCT
remain unknown, as it was not possible to obtain the premorbid
serum PCT concentrations of the patients.
In conclusion, PCT may play an important role as a
biomarker in the diagnosis of early-onset VAP following cardiac
surgery in clinical practice. Furthermore, serum PCT levels and
SOFA scores were shown to positively correlate. However, these
results require validation by further studies.
References
|
1
|
Hortal J, Giannella M, Pérez MJ, et al:
Incidence and risk factors for ventilator-associated pneumonia
after major heart surgery. Intensive Care Med. 35:1518–1525. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vijarnsorn C, Winijkul G, Laohaprasitiporn
D, et al: Postoperative fever and major infections after pediatric
cardiac surgery. J Med Assoc Thai. 95:761–770. 2012.PubMed/NCBI
|
|
3
|
Melsen WG, Rovers MM, Groenwold RH, et al:
Attributable mortality of ventilator-associated pneumonia: a
meta-analysis of individual patient data from randomised prevention
studies. Lancet Infect Dis. 13:665–671. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hortal J, Muñoz P, Cuerpo G, Litvan H,
Rosseel PM and Bouza E; European Study Group on Nosocomial
Infections; European Workgroup of Cardiothoracic Intensivists.
Ventilator-associated pneumonia in patients undergoing major heart
surgery: an incidence study in Europe. Crit Care. 13:R802009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Roeleveld PP, Guijt D, Kuijper EJ,
Hazekamp MG, de Wilde RB and de Jonge E: Ventilator-associated
pneumonia in children after cardiac surgery in The Netherlands.
Intensive Care Med. 37:1656–1663. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tamayo E, Álvarez FJ, Martínez-Rafael B,
et al: Valladolid Sepsis Study Group: Ventilator-associated
pneumonia is an important risk factor for mortality after major
cardiac surgery. J Crit Care. 27:18–25. 2012. View Article : Google Scholar
|
|
7
|
Becker KL, Snider R and Nylen ES:
Procalcitonin assay in systemic inflammation, infection, and
sepsis: clinical utility and limitations. Crit Care Med.
36:941–952. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Assicot M, Gendrel D, Carsin H, Raymond J,
Guilbaud J and Bohuon C: High serum procalcitonin concentrations in
patients with sepsis and infection. Lancet. 341:515–518. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Riedel S: Procalcitonin and the role of
biomarkers in the diagnosis and management of sepsis. Diagn
Microbiol Infect Dis. 73:221–227. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rea-Neto A, Youssef NC, Tuche F, et al:
Diagnosis of ventilator-associated pneumonia: a systematic review
of the literature. Crit Care. 12:R562008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sponholz C, Sakr Y, Reinhart K and
Brunkhorst F: Diagnostic value and prognostic implications of serum
procalcitonin after cardiac surgery: a systematic review of the
literature. Crit Care. 10:R1452006. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Adib-Conquy M, Monchi M, Goulenok C, et
al: Increased plasma levels of soluble triggering receptor
expressed on myeloid cells 1 and procalcitonin after cardiac
surgery and cardiac arrest without infection. Shock. 28:406–410.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sinning JM, Scheer AC, Adenauer V, et al:
Systemic inflammatory response syndrome predicts increased
mortality in patients after transcatheter aortic valve
implantation. Eur Heart J. 33:1459–1468. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
American Thoracic Society; Infectious
Diseases Society of America. Guidelines for the management of
adults with hospital-acquired, ventilator-associated, and
healthcare-associated pneumonia. Am J Respir Crit Care Med.
171:388–416. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Vincent JL, Moreno R, Takala J, et al: The
SOFA (Sepsis-related Organ Failure Assessment) score to describe
organ dysfunction/failure. On behalf of the Working Group on
Sepsis-Related Problems of the European Society of Intensive Care
Medicine. Intensive Care Med. 22:707–710. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Duflo F, Debon R, Monneret G, Bienvenu J,
Chassard D and Allaouchiche B: Alveolar and serum procalcitonin:
diagnostic and prognostic value in ventilator-associated pneumonia.
Anesthesiology. 96:74–79. 2002. View Article : Google Scholar
|
|
17
|
Oppert M, Reinicke A, Müller C, Barckow D,
Freix U and Eckardt KU: Elevations in procalcitonin but not
C-reactive protein are associated with pneumonia after
cardiopulmonary resuscitation. Resuscitation. 53:167–170. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Luyt CE, Combes A, Reynaud C, et al:
Usefulness of procalcitonin for the diagnosis of
ventilator-associated pneumonia. Intensive Care Med. 34:1434–1440.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hensel M, Volk T, Döcke WD, et al:
Hyperprocalcitonemia in patients with noninfectious SIRS and
pulmonary dysfunction associated with cardiopulmonary bypass.
Anesthesiology. 89:93–104. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Amin DN, Pruitt JC and Schuetz P:
Influence of major cardiopulmonary surgery on serum levels of
procalcitonin and other inflammatory markers. Anaesth Intensive
Care. 40:760–766. 2012.PubMed/NCBI
|
|
21
|
Beghetti M, Rimensberger PC, Kalangos A,
Habre W and Gervaix A: Kinetics of procalcitonin, interleukin 6 and
C-reactive protein after cardiopulmonary-bypass in children.
Cardiol Young. 13:161–167. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Meisner M, Rauschmayer C, Schmidt J, et
al: Early increase of procalcitonin after cardiovascular surgery in
patients with postoperative complications. Intensive Care Med.
28:1094–1102. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jebali MA, Hausfater P, Abbes Z, Aouni Z,
Riou B and Ferjani M: Assessment of the accuracy of procalcitonin
to diagnose postoperative infection after cardiac surgery.
Anesthesiology. 107:232–238. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Prat C, Ricart P, Ruyra X, et al: Serum
concentrations of procalcitonin after cardiac surgery. J Card Surg.
23:627–632. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Meisner M, Tschaikowsky K, Palmaers T and
Schmidt J: Comparison of procalcitonin (PCT) and C-reactive protein
(CRP) plasma concentrations at different SOFA scores during the
course of sepsis and MODS. Crit Care. 3:45–50. 1999. View Article : Google Scholar
|
|
26
|
Haasper C, Kalmbach M, Dikos GD, et al:
Prognostic value of procalcitonin (PCT) and/or interleukin-6 (IL-6)
plasma levels after multiple trauma for the development of multi
organ dysfunction syndrome (MODS) or sepsis. Technol Health Care.
18:89–100. 2010.PubMed/NCBI
|
|
27
|
Ramirez P, Garcia MA, Ferrer M, et al:
Sequential measurements of procalcitonin levels in diagnosing
ventilator-associated pneumonia. Eur Respir J. 31:356–362. 2008.
View Article : Google Scholar
|
|
28
|
Hammer S, Fuchs AT, Rinker C, et al:
Interleukin-6 and procalcitonin in serum of children undergoing
cardiac surgery with cardiopulmonary bypass. Acta Cardiol.
59:624–629. 2004. View Article : Google Scholar
|
|
29
|
Denizot Y, Lorgeot V, Cornu E and Nathan
N: Plasma leukaemia inhibitory factor, interleukin 6 and soluble
interleukin 6 receptor levels during cardiopulmonary bypass with
extracorporeal circulation. Cytokine. 10:303–306. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Póvoa P: C-reactive protein: a valuable
marker of sepsis. Intensive Care Med. 28:235–243. 2002. View Article : Google Scholar : PubMed/NCBI
|