Introduction
Diabetic peripheral neuropathy (DPN) is one of the
most common chronic complications of diabetes, inducing disability
and decreased quality of life (1,2).
Although reports of the prevalence of DPN vary substantially,
depending on the diagnostic criteria and investigation depth, the
majority of studies suggest that ~50% of all diabetic patients are
likely to develop DPN (2–4), and that the duration and severity of
the diabetes are the major risk factors (5). Early symptoms include loss of vibratory
perception, altered proprioception and impairment of pain, touch
and temperature perception, ultimately leading to a range of
complications (foot ulcers, foot and joint diseases and amputation)
(6,7). Current treatments for DPN focus on
glycemic control, foot care and the treatment of pain (3,4,8); therefore, these treatments mainly focus
on the symptoms of DPN, rather than on its causes.
DPN is caused by an imbalance between nerve damage
and repair, and is correlated with the apoptosis of peripheral
nerve cells (9,10). This imbalance is mainly fed by the
oxidative stress cycle, which induces important damage to nerve
cells (11–14). Oxidative stress leads to DNA
oxidative damage in these cells, which activates apoptosis
(14–16).
Traditional Chinese Medicine has long recognized
that DPN could be efficiently treated with medicines such as
Jinmaitong (JMT) (17). JMT capsules
can improve DPN symptoms, such as limb pain and numbness, by
increasing the nerve conduction velocity, and by improving glucose
and lipid metabolism (17–19). Studies have shown that JMT can reduce
diabetic damage to the sciatic nerve by reducing the accumulation
of sorbitol, by upregulating the expression of ciliary neurotrophic
factor (CNTF), by reducing the formation of advanced glycosylation
end products (AGEs) and by downregulating the expression of AGE
receptors (18,19). In addition, preliminary studies have
shown that JMT can increase superoxide dismutase activity in
diabetic rats, and reduce lipid peroxidation (18,19).
Despite this, the specific mechanisms underlying the action of JMT
are poorly understood.
The aim of the present study was to investigate the
effects of JMT on specific markers of DNA oxidative damage
[8-hydroxy-deoxyguanosine (8-OHdG) and nicotinamide adenine
dinucleotide phosphate (NADPH) oxidase], as well as on factors
involved in apoptosis, such as B-cell lymphoma 2 (Bcl-2), caspase 3
and cleaved-poly(ADP-ribose) polymerase 1 (PARP-1), in the sciatic
nerve of a diabetic rat model.
Materials and methods
Animals
Male six-week-old Sprague Dawley rats (n=86; body
weight, 231–267 g) were provided by Vital River Laboratory Animal
Technology Co., Ltd. [Beijing, China; certificate no. SCXK
(Beijing) 2007-0001], and were bred in the Experimental Animal
Center (specific pathogen-free level) of the Peking Union Medical
College Hospital (Beijing, China). Rats were acclimated for two
week before the commencement of the experiment. This study was
carried out in strict accordance with the recommendations of the
Guide for the Care and Use of Laboratory Animals of the National
Institutes of Health. The protocol was approved by the
Institutional Animal Care and Use Committee of the Peking Union
Medical College Hospital.
Diabetic rat model and grouping
The diabetic rat model was induced as previously
described (20). After a two-week
adaptation period, rats were randomly divided into the normal and
diabetic model (DM) groups. After a 12-h fast, a 0.45%
streptozotocin (60 mg/kg) solution (Sigma, St. Louis, MO, USA)
prepared in 0.1 mol/l citrate buffer (pH 4.5), was
intraperitoneally injected in rats of the DM group, while rats in
the normal group were injected with the same volume of 0.1 mol/l
citrate buffer. Blood glucose was measured from the tail tip 72 h
later using a blood glucose meter (MediSense® Optium™; Abbott
Laboratories, Chicago, IL, USA). Blood glucose levels ≥16.7 mmol/l
indicated model success, and the success rate was 92.1% (70/76).
Consequently, 70 successfully modeled diabetic rats were randomly
divided into five groups (n=14/group): DM control, JMT low-dosage
(JMT-L), JMT medium-dosage (JMT-M), JMT high-dosage (JMT-H) and
vitamin C (VC). The normal control group (Con) included 10 rats
with blood glucose levels <7.0 mmol/l. A rat of the JMT-L group
died in the initial stage of modeling. Twelve weeks after modeling,
eight rats died: three in the DM group, one in each of the JMT-L,
-M and -H groups and two in the VC group. Sixteen weeks after
modeling, one rat in the JMT-H group died from unsuccessful gavage
surgery.
Drug administration
JMT [composed of milkvetch root (Radix Astragali),
raw rehmannia root (Radix Rehmanniae), red sage root (Rhizoma
Corydalis), kudzuvine root (Herba Asari), leech (Hirudo), dodder
seed (Semen Cuscutae), grossy privet fruit (Fructus Ligustri
Lucidi), cassia bark tree branchlet (Ramulus Cinnamomi) and
Asarum sieboldi] is a medical preparation that is used at
the Peking Union Medical College Hospital of the Chinese Academy of
Medical Sciences, and is manufactured by Beijing Kowloon
Pharmaceutical Co., Ltd. (Beijing, China) (18). Each capsule contained 0.35 g crude
drug (lot no. 061019). The rationale (18) behind the use of the various herbs in
the JMT formulation according to their use in Chinese medicine is
the following: Dodder seed calms yang and nourishes yin of the
kidney, secures essence (retains jing or the ‘essence’ of the
kidney), improves vision and alleviates diarrhea; glossy privet
fruit nourishes yin of the liver and kidney and clears empty-heat
(too much yang or heat pushed up from the kidney); leech and red
sage root break blood (improve blood flow), expel stasis and
relieve pain; milkvetch root and raw rehmannia root calm qi and
nourish yin; cassia twig and kudzuvine root warm and unblock
channels and vessels, and promote qi and blood circulation.
As an antioxidant, vitamin C can improve oxidative
stress in diabetics (21), and it
was therefore used as a positive control. Vitamin C (0.1 g/tablet)
was purchased from Beijing Double-Crane Pharmaceutical Co., Ltd.
(Beijing, China; lot no. 080213).
Following model success, the JMT-L group received
0.44 g/kg/day JMT, the JMT-M group received 0.88 g/kg/day and the
JMT-H group received 1.75 g/kg/day. These doses were calculated
based on the crude drug content of the capsules. The VC group
received 0.05 g/kg/day vitamin C. These drugs were prepared in
distilled water. The DM and Con groups were orally fed distilled
water (10 ml/kg/day). The rats were treated for 16 weeks. Body
weight and tail tip blood glucose levels were determined prior to
JMT administration, and at weeks 4, 8, 12 and 16.
Mechanical pain threshold
After 16 weeks of treatment, prior to the sacrifice
of the rats, mechanical pain threshold assessment was performed
using the von Frey Pain Measurement Instrument (cat. no. 2391; IITC
Life Science Inc., Woodland Hills, CA, USA). The rats were placed
in an elevated metal net, and covered with transparent organic
glass. After a 15-min adaptation period, the middle of the hind
foot of each rat was vertically stimulated with the electronic Von
Frey probe, making it appear slightly S-shaped, and the paw
withdrawal response was observed. A quick flinching reaction
immediately subsequent to stimulation was considered to be a
positive reaction, and the values (g) were recorded. A paw
withdrawal reaction caused by physical activity was not reported as
positive.
Sciatic nerve tissue specimen
All rats were sacrificed after 16 weeks of
treatment. The rats were intraperitoneally injected with 12%
urethane (10 ml/kg) and were fixed on the operating table in the
prone position. The skin was cut between the biceps femoris and
semimembranosus, along the outside line of the femoral shaft and
entering into the vastus lateralis muscle. Using glass needles,
blunt dissection was performed to expose the sciatic nerve along
the two shafts. A total of 2 cm nerve was fixed using 4%
polyformaldehyde, and the remaining nerve tissue was frozen in
liquid nitrogen for polymerase chain reaction (PCR) and western
blot analyses.
Reverse transcription-quantitative PCR
(RT-qPCR)
Total mRNA was extracted from sciatic nerve tissue
using TRIzol (Tiangen Biotech Co., Ltd., Beijing, China), according
to the manufacturer's instructions. RNA purity was determined using
absorbance at 260 and 280 nm (A260/280). RNA integrity was verified
by electrophoresis on formaldehyde gels. Total RNA was
reverse-transcribed into cDNAs using oligo (dT) 12–18 primer
(Takara, Dalian, China) and Moloney Murine Leukemia Virus reverse
transcriptase (Takara).
Primer Express® 5.0 software (Applied Biosystems,
Foster City, CA, USA) and Oligo 6.0 biological software (Molecular
Biology Insights, Inc., Colorado Springs, CO, USA) were used to
design the primers shown in Table I.
mRNA quantification was performed via qPCR using the BioEasy SYBR
Green I Real-Time PCR kit (Bioer Technology Co., Ltd., Hangzhou,
China) in a LineGene real-time PCR detection system (Bioer
Technology Co., Ltd.). The qPCR reaction program was as follows:
Pre-incubation at 95°C for 2 min; amplification at 95°C for 20 sec,
59°C for 25 sec and 72°C for 30 sec, for 45 cycles. The melting
curve showed increments of 0.5°C/sec between 65 and 95°C, for a
total of 20 sec. The threshold cycle (Ct) value was defined as the
number of PCR cycles in which the fluorescence signal exceeded the
detection threshold value. ΔCt was initially calculated using the
equation CtGene-Ctβ-actin, and then
2−ΔCt was calculated to represent the relative mRNA
expression of the target genes. β-actin was used as a reference
gene.
 | Table I.Primers for the reverse
transcription-quantitative polymerase chain reaction sequences. |
Table I.
Primers for the reverse
transcription-quantitative polymerase chain reaction sequences.
| Gene | Primer sequence (5′
to 3′) | Product length
(bp) |
|---|
| β-actin | Forward:
CCCATCTATGAGGGTTACGC | 150 |
|
| Reverse:
TTTAATGTCACGCACGATTTC |
|
|
p22phox | Forward:
TATTGTTGCAGGAGTGCTCA | 103 |
|
| Reverse:
CACAGCGGTCAGGTACTTCT |
|
| Bcl-2 | Forward:
TGACTTCTCTCGTCGCTACC | 198 |
|
| Reverse:
GGTGACATCTCCCTGTTGAC |
|
| Caspase 3 | Forward:
GGACCTGTGGACCTGAAAAA | 158 |
|
| Reverse:
CCGGCATGATGAAAGCGAAGA |
|
Immunohistochemistry
Paraffin sections (5-µm) were made from sciatic
nerves. The sections were dewaxed, washed with 0.01 mmol/l
phosphate-buffered saline (PBS) for 5 min and boiled in citric acid
(pH 6.0) for 2 min. Subsequent to cooling, the sections were rinsed
three times for 2 min in 0.01 mmol/l PBS. Endogenous peroxidase was
neutralized with 3% H2O2 for 30 min, and the
sections were rinsed three times for 2 min in 0.01 mmol/l PBS.
Bovine serum albumin (3%) was added and incubated for 20 min at
room temperature. The following primary antibodies were used for
incubation at 4°C, overnight: Rabbit anti-8-OHdG monoclonal
antibody (1:100; Japan Institute for the Control of Aging, Nikken
SEIL Co., Ltd., Shizuoka, Japan; cat.no. MOG-020P), rabbit
anti-NADPH oxidase subunit p22phox polyclonal antibody
(1:400; Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA;
cat.no. SC20781), rabbit anti-Bcl-2 polyclonal antibody (1:200;
Santa Cruz Biotechnology, Inc.; cat.no. SC783) or rabbit
anti-caspase 3 (17 kDa) polyclonal antibody (1:100; Bioworld
Technology Inc., Nanjing, China; cat.no. BS7004). The negative
control was 0.01 mmol/l PBS. The sections were rinsed three times
for 2 min in 0.01 mmol/l PBS prior to the addition of the secondary
antibody (horseradish peroxidase (HRP)-conjugated goat anti-rabbit,
cat.no. PV9001; Zhongshan Goldenbridge Biotechnology Co., Ltd.,
Beijing, China) and incubated at room temperature for 20 min.
Subsequent to rinsing three times for 2 min in 0.01 mmol/l PBS, 50
µl 3,3′-diaminobenzidine solution (Zhongshan Goldenbridge
Biotechnology Co., Ltd.) was added. The sections were then
counterstained with hematoxylin and observed using a Leica DM3000
microscope and the Leica image acquisition system (Leica
Microsystems, Wetzlar, Germany). Image-Pro Plus 6.0 software (Media
Cybernetics, Inc., Rockville, MD, USA) was used for image analysis.
Immunohistochemistry results were measured using the integrated
optical density.
Western blot analysis
Total proteins were extracted from the rat sciatic
nerves using the Pierce Cell Lysis reagents (Thermo Fisher
Scientific, Inc., Waltham, MA, USA) for protein extraction. The
resulting solution was centrifuged at 10,000 xg and 4°C, for 10
min. The bicinchoninic acid (BCA) method (BCA Protein Assay kit;
Thermo Fisher Scientific, Inc.) was used to determine the protein
concentrations. The same quantity of proteins (50 µg) was separated
by 6% SDS-PAGE, and transferred onto polyvinylidene fluoride
membranes (GE Healthcare, Waukesha, WI, USA). Non-specific sites
were blocked with 5% powdered milk diluted in Tris-buffered saline
with 0.05% Tween 20 (TBST) for 30 min at room temperature. Proteins
were detected overnight at 4°C, using the following primary
antibodies: Anti-cleaved-PARP-1 (89 kDa) polyclonal antibody (Cell
Signaling Technology, Inc., Danvers, MA, USA; cat.no. 9542s) and
β-actin (Sigma, St. Louis, MO, USA; cat.no. A3853). Subsequent to
being washed with TBST, the membranes were incubated with
HRP-conjugated immunoglobulin G (Zhongshan Goldenbridge
Biotechnology Co., Ltd.) for 1 h at room temperature. The membranes
were then further washed with TBST, and the proteins were detected
using an enhanced chemiluminescence reagent (Thermo Fisher
Scientific, Inc.), according to the manufacturer's instructions,
using a FluorChem IS-8800 imaging system (Alpha Innotech Corp., San
Leandro, CA, USA). The bands were quantified using the AlphaEaseFC™
software (Alpha Innotech Corp.).
Statistical analysis
SPSS 13.0 software (SPSS Inc., Chicago, IL, USA) was
used for the statistical analysis. The one-sample
Kolmogorov-Smirnov Z-test was used to determine if the variables
were normally distributed. Normally-distributed data are expressed
as the mean ± standard deviation. Multi-group independent samples
were compared using one-way analysis of variance, with the least
significant difference post hoc test. Non-normally-distributed data
were analyzed with non-parametric tests. P<0.05 was considered
to indicate a statistically significant difference.
Results
Effect of JMT on fasting blood glucose
levels and body weight in the diabetic rat model
Fasting blood glucose levels in all the diabetic
rats were higher than those in the control group rats at all
time-points (Table II, all
P<0.01). No significant differences in fasting blood glucose
levels were found among the DM, VC and JMT groups at any
time-points (Table II, all
P>0.05).
| Table II.Effect of JMT on fasting blood
glucose levels in the diabetic rat model. |
Table II.
Effect of JMT on fasting blood
glucose levels in the diabetic rat model.
|
|
|
| Post-treatment
(mmol/l) |
|---|
|
|
|
|
|
|---|
| Group | n | Pre-treatment
(mmol/l) | 4 weeks | 8 weeks | 12 weeks | 16 weeks |
|---|
| Con | 10 |
5.0±0.7 |
5.1±0.3 |
5.4±0.8 |
6.1±0.1 |
5.4±0.4 |
| DM | 11 |
21.1±3.1a |
21.1±1.8a |
23.2±1.0a |
23.9±2.4a |
21.9±0.7a |
| JMT-L | 12 |
20.8±3.2a |
21.2±1.9a |
22.9±0.9a |
22.8±1.6a |
22.3±0.7a |
| JMT-M | 13 |
21.0±3.1a |
22.8±1.7a |
23.5±0.8a |
23.3±2.5a |
21.2±1.8a |
| JMT-H | 12 |
20.8±3.3a |
22.4±2.1a |
21.9±0.7a |
23.4±1.1a |
22.1±0.7a |
| VC | 12 |
21.3±3.1a |
20.7±1.4a |
23.8±0.5a |
23.8±0.5a |
22.9±1.1a |
No significant differences in body weight were
observed at baseline among the different groups (all P>0.05).
After 4 weeks of treatment, the body weight of the diabetic rats
was lower than that of the control group rats (all P<0.01). No
significant differences in body weight were found among the DM, VC
and JMT groups at any time-points (Table III, all P>0.05).
| Table III.Effect of JMT on body weight in the
diabetic rat model. |
Table III.
Effect of JMT on body weight in the
diabetic rat model.
|
|
|
| Post-treatment
(g) |
|---|
|
|
|
|
|
|---|
| Group | n | Pre-treatment
(g) | 4 weeks | 8 weeks | 12 weeks | 16 weeks |
|---|
| Con | 10 |
257.2±20.2 |
532.5±10.5 |
578.3±24.4 |
604.1±33.1 |
641.2±15.8 |
| DM | 11 |
256.4±17.3 |
303.6±10.1a |
321.5±9.3a |
431.1±6.8a |
468.1±7.2a |
| JMT-L | 12 |
258.1±22.1 |
284.9±10.1a |
326.5±10.4a |
426.2±8.5a |
459.5±10.7a |
| JMT-M | 13 |
256.2±18.8 |
303.3±10.7a |
324.5±10.9a |
452.6±9.3a |
480.6±12.3a |
| JMT-H | 12 |
257.9±23.9 |
299.9±16.6a |
341.7±14.3a |
442.2±13.6a |
467.8±14.8a |
| VC | 12 |
257.1±33.8 |
301.2±9.6a |
329.7±8.3a |
449.2±10.7a |
477.2±8.9a |
Effect of JMT on mechanical pain
threshold in the diabetic rat model
The mechanical pain threshold values are listed in
Table IV. Compared with the normal
controls, the mechanical pain threshold values were significantly
lower in the DM group (P<0.01). The mechanical pain threshold
values of each treatment group were higher than those of the DM
group (all P<0.01). Among the JMT groups, the mechanical pain
threshold was significantly higher in the JMT-M group compared with
that in the JMT-L, JMT-H and VC groups (all P<0.01).
| Table IV.Effect of JMT on mechanical pain
threshold in the diabetic rat model. |
Table IV.
Effect of JMT on mechanical pain
threshold in the diabetic rat model.
| Group | n | Value (g) |
|---|
| Con | 10 |
78.69±8.13 |
| DM | 11 |
35.32±12.06a |
| JMT-L | 12 |
52.87±6.46a,b,c |
| JMT-M | 13 |
74.69±9.26b,d |
| JMT-H | 12 |
61.71±1.95a,b,c |
| VC | 12 |
59.49±3.42a,b |
Effect of JMT on 8-OHdG and NADPH
p22phox expression in the sciatic nerve of the diabetic
rat model
The DM group exhibited a 2.1-fold increase in 8-OHdG
levels compared with the Con group (P<0.01). Compared with the
DM group, 8-OHdG was decreased in each treatment group (JMT-L,
−11.2%; JMT-M, −30.0%; JMT-H, −22.3% and VC, −20.2%; all P<0.01)
(Fig. 1). The decrease in the JMT-M
group was more notable than that in the JMT-L, JMT-H and VC groups
(all P<0.01).
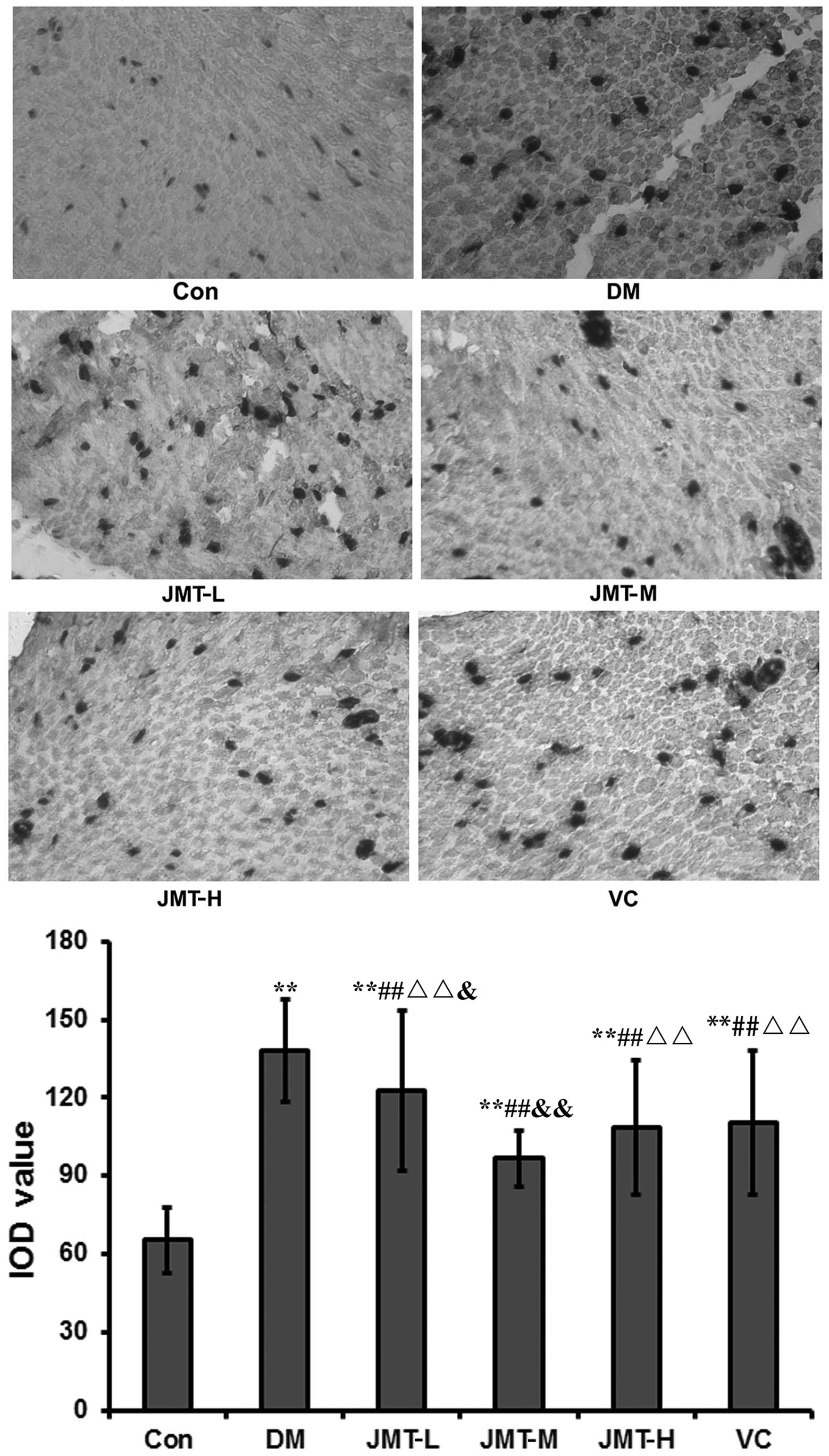 | Figure 1.Effect of JMT on 8-OHdG expression in
the sciatic nerve in a diabetic rat model. 8-OHdG protein
expression was determined by immunohistochemistry (magnification,
x40). IOD values are shown as the mean ± standard deviation
(n=5/group). **P<0.01 vs. Con; ##P<0.01 vs. DM;
ΔΔP<0.01 vs. JMT-M; &P<0.05 and
&&P<0.01 vs. VC. Con, normal control; DM,
diabetic model control; JMT, Jinmaitong; -L, -low-dosage; -M,
medium-dosage; -H, -high-dosage; VC, vitamin C; IOD, integrated
optical density; 8-OHdG, 8-hydroxy-deoxyguanosine. |
A marked increase in NADPH p22phox mRNA
and protein levels was observed in the DM group compared with the
Con group (77.6- and 7.6-fold, respectively, both P<0.01). The
increased NADPH p22phox mRNA and protein levels in the
DM group were then decreased in each treatment group. The results
for the protein levels were as follows: JMT-L, −56.1%; JMT-M,
−83.1%; JMT-H, −67.8% and VC, −41.4% (all P<0.05) (Fig. 2A and B).
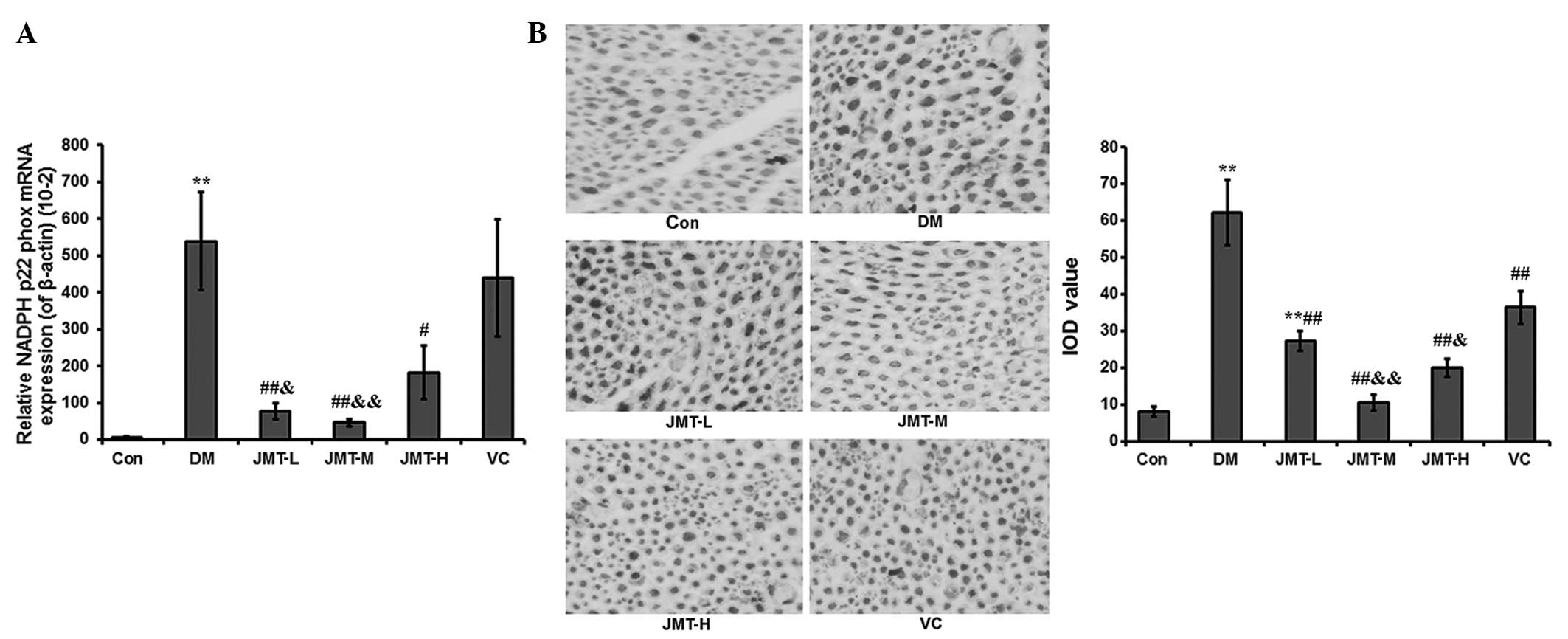 | Figure 2.Effect of JMT on NADPH
p22phox mRNA and protein expression in the sciatic nerve
in a diabetic rat model. (A) NADPH p22phox mRNA
expression was determined by reverse transcription-quantitative
polymerase chain reaction analysis; β-actin was used as a reference
gene; (B) NADPH p22phox protein expression was
determined by immunohistochemistry (magnification, x200). The data
are shown as the mean ± standard deviation (n=5/group). **P<0.01
vs. Con; #P<0.05 and ##P<0.01 vs. DM;
&P<0.05 and &&P<0.01 vs.
VC. Con, normal control; DM, diabetic model control; JMT,
Jinmaitong; -L, -low-dosage; -M, medium-dosage; -H, -high-dosage;
VC, vitamin C; IOD, integrated optical density; NADPH, nicotinamide
adenine dinucleotide phosphate. |
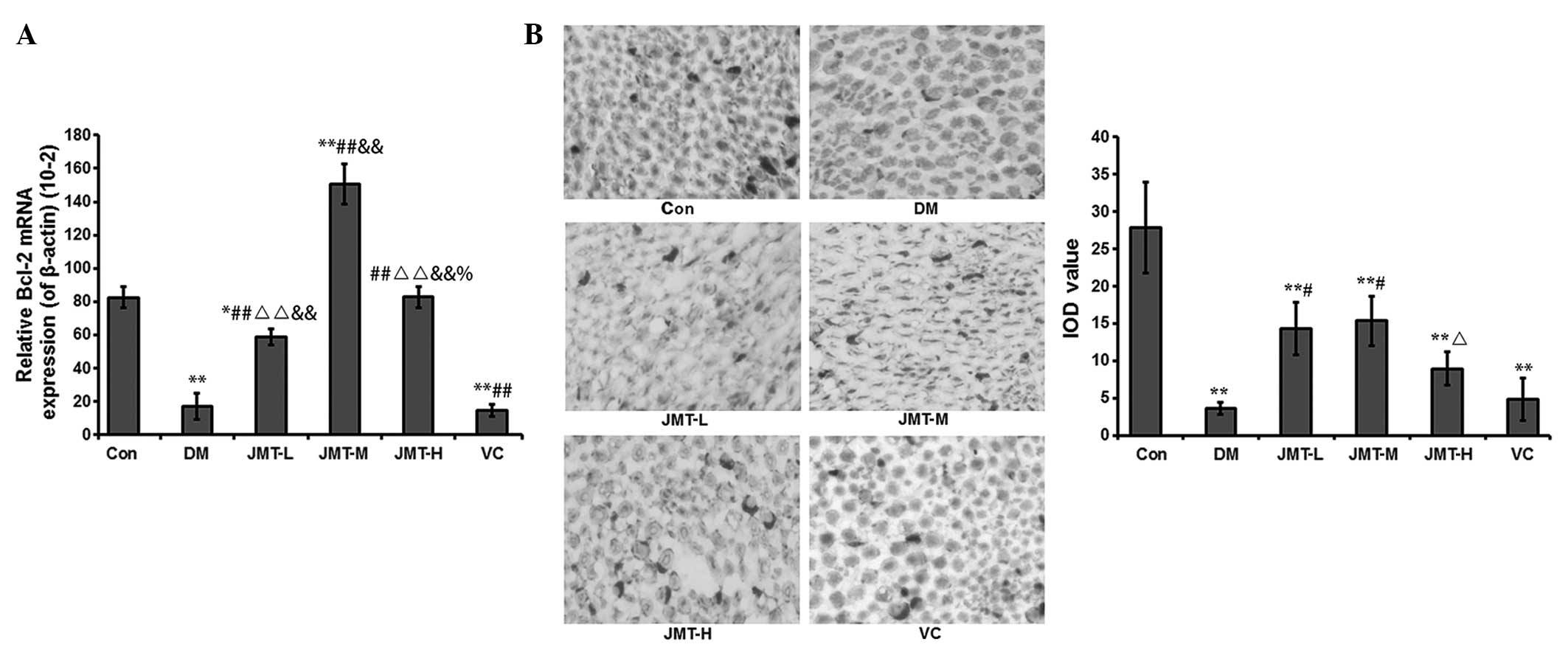
Effect of JMT on apoptosis-related
gene (Bcl-2, caspase-3 and cleaved-PARP-1) expression in the
sciatic nerve of the diabetic rat model
In the DM group, a strong decrease in Bcl-2 mRNA and
protein levels was induced compared with the Con group (−79.2 and
−87.2%, respectively, both P<0.01). Compared with the DM group,
the Bcl-2 levels were increased in each treatment group. The
results for the protein levels were as follows: JMT-L, 4.0-fold;
JMT-M, 4.3-fold; JMT-H, 2.5-fold and VC, 1.3-fold (all P<0.01)
(Fig. 3A and B). The increase was
most evident in the JMT-M group compared with the JMT-L, JMT-H and
VC groups (all P<0.01).
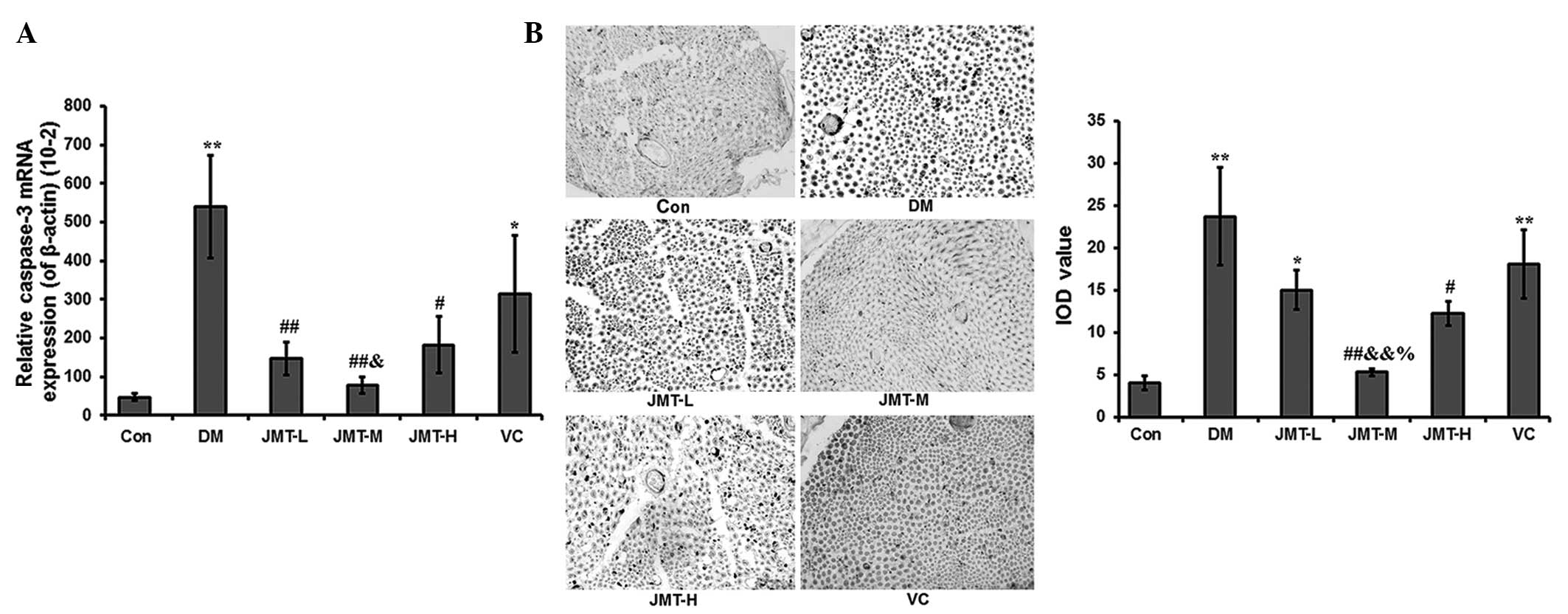
Caspase 3 mRNA and protein levels in the DM group
were markedly increased compared with those in the Con group (11.7-
and 5.9-fold, respectively, both P<0.01). This increase was then
decreased in each treatment group. The results for the protein
levels were as follows: JMT-L, −36.6%; JMT-M, −77.6%; JMT-H, −48.3%
and VC, 23.9% (all P<0.01) (Fig. 4A
and B).
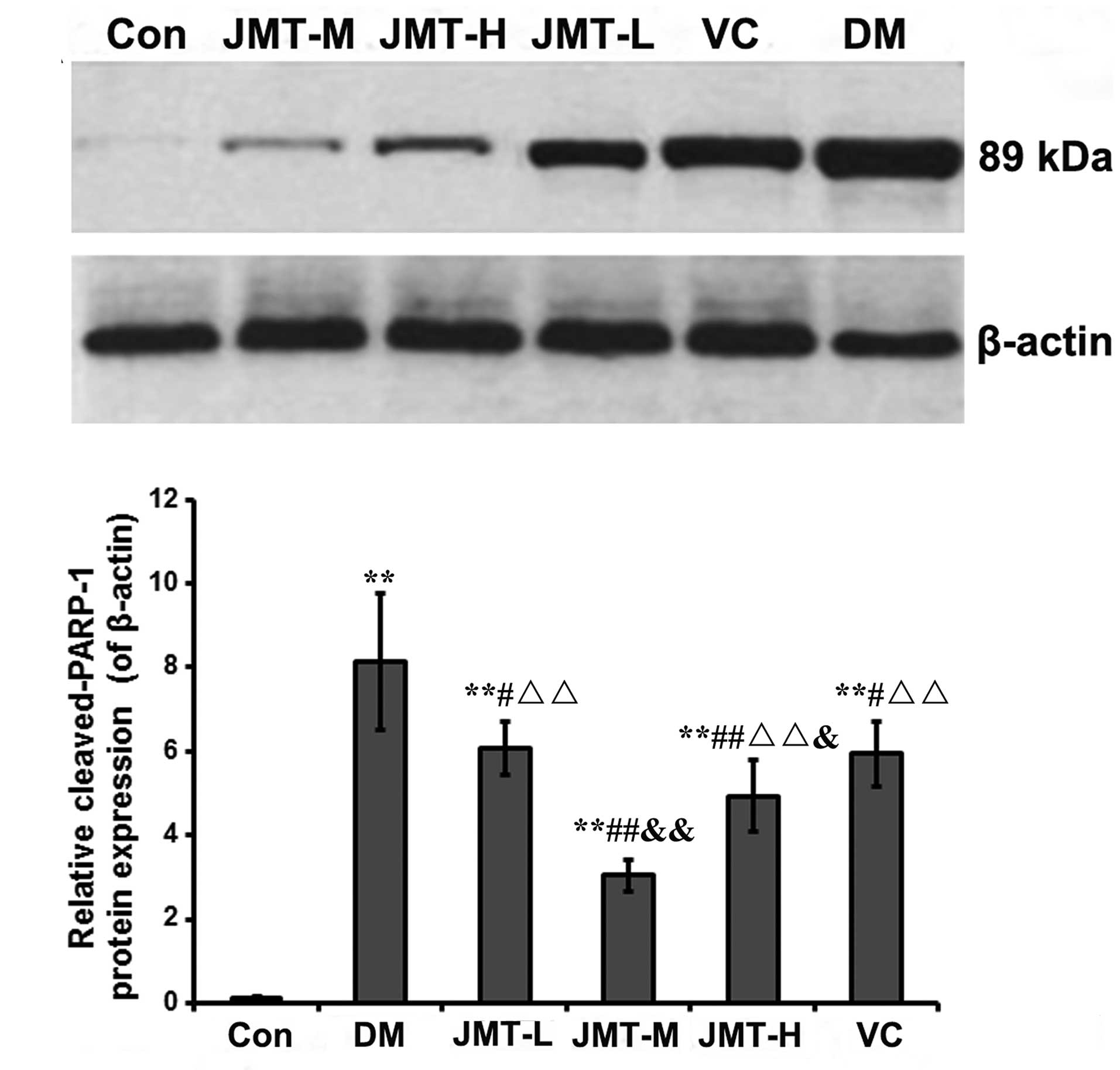
The DM group exhibited a significant increase in
cleaved-PARP-1 levels compared with the Con group (62.6-fold,
P<0.01). The cleaved-PARP-1 levels were decreased in each
treatment group compared with those in the DM group (JMT-L, −25.4%;
JMT-M, −62.5%; JMT-H, −39.4% and VC, 27.0%; all P<0.05)
(Fig. 5). The decrease in the JMT-M
group was more notable than that in the JMT-L, JMT-H and VC groups
(all P<0.01).
Discussion
In the DPN state, there is an imbalance between
nerve damage and repair, favoring nerve damage, and leading to
decreased sensory perception (9,10);
therefore, finding ways to restore this balance is of the prime
importance. A number of clinical observations have suggested that
JMT could improve limb pain, numbness and other neurological
symptoms in patients with DPN (8,18).
Furthermore, previous studies have suggested that JMT exerts
anti-lipid peroxidation effects (18,19).
There is, however, a lack of data regarding the effect of JMT on
nerve cells in diabetes.
In the present study it was observed that, following
treatment, the rats in the JMT groups had an improved pain
threshold compared with the diabetic controls, and the JMT-M group
had a pain threshold that was similar to normal control rats.
8-OHdG and NADPH p22phox, markers of oxidative DNA
damage, were significantly decreased by JMT. Changes in the levels
of certain key factors involved in apoptosis, Bcl-2, caspase 3 and
cleaved-PARP-1, were all ameliorated by JMT; however, no
differences in body weight and fasting blood levels were found
among the different diabetic groups, suggesting that JMT does not
improve DPN by enhancing diabetes control, but through direct
effects on oxidation and nerve cells.
The high glucose levels observed in diabetes
increase the levels of reactive oxygen species (ROS) through a
number of pathways, intensifying the oxidative stress in all cells,
including nerve cells (22). High
levels of ROS can lead to DNA damage, which may initiate apoptosis;
therefore, any biomarkers of DNA oxidative damage should indicate
the level of oxidative stress. NADPH oxidase is an enzyme made up
of six subunits, including one p22phox subunit. NADPH
oxidase generates a variety of ROS, including the superoxide anion,
and measuring the expression of p22phox subunits is a
surrogate of NADPH oxidase expression and of ROS production that
can attack the DNA (23). When ROS
attack the DNA, the guanines at the C-8 position in the DNA chain
can be hydroxylated, thus forming 8-OHdG. The presence of 8-OHdG
therefore indicates the occurrence of DNA oxidative damage
(24).
Following DNA damage, PARP is activated as a DNA
damage receptor. PARP-1 is cleaved by caspases, producing the
apoptosis-related 24-kDa fragment and the 89-kDa cleaved-PARP-1
fragment. This 89-kDa fragment can be measured as a surrogate of
PARP-1 activation (25,26). Cleavage of caspase 3 generates the
17-kDa active subunit, which activates the caspase-activated
deoxyribonuclease, which degrades DNA and eventually causes cell
death (27). The amount of activated
caspase-3 (17 kDa) therefore reflects levels of apoptosis. Bcl-2 is
a protein involved in apoptosis regulation and has anti-apoptotic
effects through its interactions with a number of factors and
pathways (28). As is well known,
the diabetic condition shifts these markers towards apoptosis in
nerves (9,10), and the present results showed that
JMT partly rescues this undesirable shift, as indicated by
decreased p22phox, 8-OHDG, cleaved-PARP-1 and caspase 3,
and by increased Bcl-2.
Using an electronic von Frey instrument to detect
the mechanical pain threshold of rats, it was observed in the
present study that rats receiving JMT had a better pain threshold
than diabetic rats; furthermore, the rats from the JMT-M group had
a similar threshold to the normal control rats. The von Frey
instrument is commonly used to study pain thresholds in diabetic
rat models (29,30), although there is some suggestion that
other methods may provide better information on the time and
sensitivity of the response with more consistent results (31–33).
Despite this, the results suggested that JMT was effective at
alleviating hyperalgesia in DPN rats. Since there were no changes
in body weight or in the glucose levels of the JMT-treated rats,
the results additionally suggested that the effects of JMT on DPN
were due to a direct reduction in oxidative stress and apoptosis,
rather than a decreased diabetes burden.
A previous study using JMT, in which no changes in
body weight and blood levels were observed following JMT treatment,
supports the theory that JMT acts by decreasing oxidative stress
and apoptosis, and revealed that JMT could improve sciatic nerve
health by increasing levels of CNTF, which is involved in a number
of survival pathways of nerve cells, favoring their repair
(18). The present study suggests
that JMT also reduces the oxidative stress on nerve cells in
diabetes; however, the exact association between CNTF and oxidative
stress in diabetic nerve cells remains to be further explored. JMT
has additionally been shown to improve the symptoms of diabetic
gastric autonomic neuropathy (18).
An in vitro study using rat Schwann cells showed that a
high-glucose medium inhibited their proliferation, and that JMT had
a positive effect by partly restoring cell growth (19). Furthermore, the results of the
present study are supported by a previous study in
high-glucose-cultured rat Schwann cells showing that JMT increased
the expression of Bcl-2 (anti-apoptosis) and decreased the
expression of caspase 3 (pro-apoptosis) (34).
These results suggest that JMT has an anti-apoptotic
activity that could lead to decreased DPN symptoms, and are
consistent with previous studies showing the beneficial effects of
antioxidants on DPN (35,36) and with the results using vitamin C.
In the present study, however, JMT had a greater effect than
vitamin C, and on more parameters. As a complex mix of Chinese
herbs JMT is designed to produce a combination of effects and it is
only possible to offer speculation regarding which herbs could be
responsible for the results observed in this study.
Jiangtangshuluofang, which also contains Radix Rehmanniae and Radix
Astragali, among other ingredients, has been shown to decrease the
apoptosis of Schwann cells (17,37).
Although Radix Astragali has been shown to decrease the apoptosis
of Schwann cells in isolation, this action increased in combination
with other traditional Chinese medicinal herbs (17,38).
This indicates that Radix Astragli, or milkvetch root, is at least
partially responsible for the apoptosis results. Another point to
consider is that the medium dose of JMT produced the most
beneficial results in this study. As such, there was not a linear
response to the concentration of the dose. This may be due to the
highest dose having a detrimental effect. The reasons for this
require further investigation, but could be associated with the
effects of ROS, such as the immune response, being inhibited.
In conclusion, the results of the present study
suggest that the Traditional Chinese Medicine JMT may improve the
symptoms of DPN through the inhibition of DNA oxidative damage
caused by oxidative stress and by reducing apoptosis in nerve cells
from DPN rats. These results suggest that JMT could be a good
option to prevent DPN or to improve DPN symptoms in diabetic
patients.
References
|
1
|
Dobretsov M, Romanovsky D and Stimers JR:
Early diabetic neuropathy: Triggers and mechanisms. World J
Gastroenterol. 13:175–191. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dyck PJ, Kratz KM, Karnes JL, et al: The
prevalence by staged severity of various types of diabetic
neuropathy, retinopathy and nephropathy in a population-based
cohort: The Rochester Diabetic Neuropathy Study. Neurology.
43:817–824. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tesfaye S: Advances in the management of
diabetic peripheral neuropathy. Curr Opin Support Palliat Care.
3:136–143. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Edwards JL, Vincent AM, Cheng HT and
Feldman EL: Diabetic neuropathy: Mechanisms to management.
Pharmacol Ther. 120:1–34. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Genuth S: Insights from the diabetes
control and complications trial/epidemiology of diabetes
interventions and complications study on the use of intensive
glycemic treatment to reduce the risk of complications of type 1
diabetes. Endocr Pract. 12 Suppl:1:34–41. 2006. View Article : Google Scholar
|
|
6
|
Vinik A, Emir B, Cheung R and Whalen E:
Relationship between pain relief and improvements in patient
function/quality of life in patients with painful diabetic
peripheral neuropathy or postherpetic neuralgia treated with
pregabalin. Clin Ther. 35:612–623. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nicholson B: Differential diagnosis:
Nociceptive and neuropathic pain. Am J Manag Care. 12
(Suppl):S256–S262. 2006.PubMed/NCBI
|
|
8
|
Shakher J and Stevens MJ: Update on the
management of diabetic polyneuropathies. Diabetes Metab Syndr Obes.
4:289–305. 2011.PubMed/NCBI
|
|
9
|
Russell JW, Sullivan KA, Windebank AJ,
Herrmann DN and Feldman EL: Neurons undergo apoptosis in animal and
cell culture models of diabetes. Neurobiol Dis. 6:347–363. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Allen DA, Yaqoob MM and Harwood SM:
Mechanisms of high glucose-induced apoptosis and its relationship
to diabetic complications. J Nutr Biochem. 16:705–713. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
El Boghdady NA and Badr GA: Evaluation of
oxidative stress markers and vascular risk factors in patients with
diabetic peripheral neuropathy. Cell Biochem Funct. 30:328–334.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
12
|
Figueroa-Romero C, Sadidi M and Feldman
EL: Mechanisms of disease: The oxidative stress theory of diabetic
neuropathy. Rev Endocr Metab Disord. 9:301–314. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kasznicki J, Kosmalski M, Sliwinska A, et
al: Evaluation of oxidative stress markers in pathogenesis of
diabetic neuropathy. Mol Biol Rep. 39:8669–8678. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schmeichel AM, Schmelzer JD and Low PA:
Oxidative injury and apoptosis of dorsal root ganglion neurons in
chronic experimental diabetic neuropathy. Diabetes. 52:165–171.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sun LQ, Zhao J, Zhang TT, et al:
Protective effects of Salvianolic acid B on Schwann cells apoptosis
induced by high glucose. Neurochem Res. 37:996–1010. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hernández-Beltrán N, Moreno CB and
Gutiérrez-Álvarez AM: Contribution of mitochondria to pain in
diabetic neuropathy. Endocrinol Nutr. 60:25–32. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Piao Y and Liang X: Chinese medicine in
diabetic peripheral neuropathy: Experimental research on nerve
repair and regeneration. Evid Based Complement Alternat Med.
2012:1916322012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shi Y, Liang XC, Wu QL, et al: Effects of
Jinmaitong Capsule on ciliary neurotrophic factor in sciatic nerves
of diabetes mellitus rats. Chin J Integr Med. 19:104–111. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Qu L, Liang XC, Zhang H, Wu QL, Sun LQ and
Gu B: Effect of Jinmaitong serum on the proliferation of rat
Schwann cells cultured in high glucose medium. Chin J Integr Med.
14:293–297. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kim J, Yokoyama K and Araki S: The effects
of Ginkgo biloba extract (GBe) on axonal transport microvasculature
and morphology of sciatic nerve in streptozotocin-induced diabetic
rats. Environ Health Prev Med. 5:53–59. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Varvarovská J, Racek J, Stetina R, et al:
Aspects of oxidative stress in children with type 1 diabetes
mellitus. Biomed Pharmacother. 58:539–545. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pop-Busui R, Sima A and Stevens M:
Diabetic neuropathy and oxidative stress. Diabetes Metab Res Rev.
22:257–273. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bedard K and Krause KH: The NOX family of
ROS-generating NADPH oxidases: Physiology and pathophysiology.
Physiol Rev. 87:245–313. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Toyokuni S: Reactive oxygen
species-induced molecular damage and its application in pathology.
Pathol Int. 49:91–102. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Obrosova IG, Xu W, Lyzogubov VV, et al:
PARP inhibition or gene deficiency counteracts intraepidermal nerve
fiber loss and neuropathic pain in advanced diabetic neuropathy.
Free Radic Biol Med. 44:972–981. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Oliver FJ, de la Rubia G, Rolli V,
Ruiz-Ruiz MC, de Murcia G and Murcia JM: Importance of
poly(ADP-ribose) polymerase and its cleavage in apoptosis. Lesson
from an uncleavable mutant. J Biol Chem. 273:33533–33539. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lamkanfi M, Festjens N, Declercq W, Vanden
Berghe T and Vandenabeele P: Caspases in cell survival,
proliferation and differentiation. Cell Death Differ. 14:44–55.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Qin W, Hu J, Guo M, et al: BNIPL-2, a
novel homologue of BNIP-2, interacts with Bcl-2 and Cdc42GAP in
apoptosis. Biochem Biophys Res Commun. 308:379–385. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fuchs D, Birklein F, Reeh PW and Sauer SK:
Sensitized peripheral nociception in experimental diabetes of the
rat. Pain. 151:496–505. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dobretsov M, Hastings SL, Romanovsky D,
Stimers JR and Zhang JM: Mechanical hyperalgesia in rat models of
systemic and local hyperglycemia. Brain Res. 960:174–183. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Vivancos GG, Verri WA Jr, Cunha TM, et al:
An electronic pressure-meter nociception paw test for rats. Braz J
Med Biol Res. 37:391–399. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Chaplan SR, Bach FW, Pogrel JW, Chung JM
and Yaksh TL: Quantitative assessment of tactile allodynia in the
rat paw. J Neurosci Methods. 53:55–63. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Farghaly HS, Abd-Ellatief RB, Moftah MZ,
Mostafa MG, Khedr EM and Kotb HI: The effects of dexmedetomidine
alone and in combination with tramadol or amitriptyline in a
neuropathic pain model. Pain Physician. 17:187–195. 2014.PubMed/NCBI
|
|
34
|
Wang PY, Liang XC, Zhang H, et al: Effect
of serum containing Jinmaitong Capsule on rats' Schwann cell
apoptosis induced by high glucose concentration. Chin J Integr Med.
19:517–523. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Pazdro R and Burgess JR: The role of
vitamin E and oxidative stress in diabetes complications. Mech
Ageing Dev. 131:276–286. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Vincent AM, Edwards JL, Sadidi M and
Feldman EL: The antioxidant response as a drug target in diabetic
neuropathy. Curr Drug Targets. 9:94–100. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ji JL and Chen DS: Experiment study of
nourishing yin, invigorating qi, extinguishing wind, promoting
blood circulation and draining collateral method of the sciatic
nerve Schwann cells apoptosis of diabetic rats. Zhongguo Zhong Yi
Ji Zheng. 18:1304–1306. 2009.(In Chinese).
|
|
38
|
Liu XY, Zhang YY and Zhang JQ: Effect of
astragalus, salvia, yam and its compound on apoptosis of Schwann
cells co-cultured with endothelial cells in high glucose. Zhong Yao
Yao Li Yu Lin Chuang. 26:41–44. 2010.(In Chinese).
|