Introduction
Von Willebrand's disease (VWD) is the most common
inherited bleeding disorder worldwide, with a prevalence varying
within 0.1–1% of the general population depending on the method of
diagnosis (1–4). The disorder is caused by a quantitative
or qualitative deficiency in the von Willebrand factor (VWF). Since
VWD is an autosomal inherited disorder, men and women are equally
affected. However, more women experience hemostatic challenges
through menstrual bleeding and childbirth (5).
Heavy menstrual bleeding (HMB), which is defined as
>80 ml per menstruation (6), is
common in women with VWD. Previous studies have shown that 78–92%
of women with VWD suffer from HMB, compared with a 10% prevalence
of HMB in all Swedish women of reproductive age (7–9).
HMB can be managed through a range of
pharmacological treatments, such as contraceptive pills,
levonorgestrel-releasing intrauterine systems (LNG-IUS), and
tranexamic acid (TA) (10). For
women with VWD, treatment with D-arginine vasopressin and
VWF/factor VIII concentrates is also an option (11). Despite the availability of extensive
pharmacological options, surgical treatment may be necessary
(10). Kirtava et al
(12) demonstrated that a higher
proportion of women with VWD undergo hysterectomy and at a younger
age compared with women in the general population.
HMB affects numerous aspects of health-associated
quality of life, both physical and mental. It can cause
iron-deficiency anemia in severe cases, and there are
psychological, social and employment consequences associated with
HMB (13). Barr et al
(14) demonstrated that women with
VWD participate less in post-secondary education than the general
population, and suggested that this may be due to iron deficiency
resulting from HMB. Côté et al (15) reported that HMB is also associated
with a marked work loss and has important economic implications for
women.
The majority of studies that have been conducted on
women with VWD are case series using few patients from separate or
solitary hospitals, and the incidence of HMB in women with VWD in
Sweden remains uncertain. Furthermore, little is known about how
such women perceive their health-associated quality of life, and
whether there may be a potential benefit in a closer cooperation
between hematologists and gynecologists. The purpose of the present
study was to investigate whether women in Stockholm diagnosed with
VWD experience HMB and an impaired health-associated quality of
life.
Materials and methods
Patients
The study subjects were recruited from a local
register for patients with VWD at the Coagulation Unit of
Karolinska University Hospital (Stockholm, Sweden). It was optional
for patients to be a part of the register, but all patients were
asked to participate. The local register was searched, having set
the inclusion criteria to a diagnosis of VWD, female gender and an
age of 18–52 years [which is the mean age for menopause in Sweden
(16)]. A total of 30 women were
included in the present study.
Treatments
Patients received one of the following treatment
options: TA, 12 patients; desmopressin, 5 patients; LNG-IUS, 5
patients; progesterone contraceptive pills (PCP), 4 patients;
VWF/factor VIII, 2 patients. It is of note that the efficacy of
treatment varies between different types of VWD and between
patients, so it is difficult to predict the outcome of treatment
(17).
TA prevents the conversion of plasminogen to plasmin
by inhibiting the binding of plasminogen to fibrin, generating an
antifibrinolytic effect. This is administered intravenously, orally
or locally (18). TA alone may be
sufficient to control mucosal bleeds, and is often used to amplify
the effect of desmopressin D-arginine vasopressin (DDAVP) or
VWF/factor VIII concentrates (11).
DDAVP, administered as an intranasal spray or
subcutaneous injection, increases the release of endogenous VWF and
factor VIII from endothelial cells (19). The response to DDAVP depends on the
type of VWD; type 1 typically responds well to this, types 2A, 2M
and 2N respond to an intermediate degree, and type 3 is
unresponsive (20).
LNG-IUS is a hormonal intrauterine device used as an
effective form of birth control in addition to treating excessive
bleeding during menstruation (21).
PCP is a hormonal method of contraception that does
not include estrogens. This may be used for contraception in
addition to representing a treatment option for heavy menstruation
(22).
VWF/factor VIII concentrates may be administered
when the response to DDAVP is insufficient (20). VWF/factor VIII concentrates are
administered intravenously, with a controlled ratio of VWF to
factor VIII. These provide prophylaxis for bleeding in patients
with severe VWD and prevent bleeding following surgery or trauma
(20).
Data collection
A questionnaire, a pictorial blood-loss assessment
chart (PBAC) to assess HMB, and a health survey (SF-36) to evaluate
health-associated quality of life were sent to each participant.
Background information on the type of VWD and any pharmacological
treatment that the patients had received was retrieved from their
medical records.
The patient administered questionnaire was used to
investigate whether the women experienced HMB, the perceived impact
of menstruation on overall life activities and the pharmacological
treatment for HMB. The questionnaire consisted of 102 questions on
11 themes (Table I) and was
originally developed by a research group at the Coagulation Unit at
Karolinska University Hospital during an unpublished study on
health-associated quality of life in women with HMB. The questions
regarding life conditions (questions 1–12) are used in clinical
practice at the Coagulation Unit, whereas questions 13–17 were
constructed by the research group at the Coagulation Unit and
assessed the amount of menstrual blood loss, the duration of
menstruation and the need for advice on menstruation. Questions
18–29, which examined the perceived impact of menstruation on
overall life activities, originate from studies conducted by Ruta
et al (23) and Coulter et
al (24). In order to limit the
scope of this study to relevant data, questions 30–101 in the
questionnaire were not analyzed. These questions explored
self-esteem, sexual functioning and mental health more thoroughly
and will be examined in a subsequent study.
 | Table I.Themes in a questionnaire that
included 11 different topics regarding various aspects of life
associated with HMB. |
Table I.
Themes in a questionnaire that
included 11 different topics regarding various aspects of life
associated with HMB.
| Questions | Theme |
|---|
| 1–12 | Life
conditions |
| 13–17 | Menstruation |
| 18–29 | Assessment of
functioning and health associated with HMB |
| 30–37 | Body image and
self-esteem associated with menstruation |
| 38–41 | Sexual
relationships |
| 42–60 | Female sexual
function index |
| 61–65 | Sexuality |
| 66–77 | Female sexual
distress scale |
| 78–87 | Rosenberg's
self-esteem scale |
| 88–101 | Hospital anxiety
and depression scale |
| 102 | Pharmacological
treatment for HMB |
A PBAC was used to clinically assess the amount of
menstrual blood loss and the duration of flow according to the
method developed by Higham et al (25), conducted prospectively by comparison
of the tampons/pads supplied with a scoring table. A score of
>100 was interpreted as a HMB.
In order to assess health-associated quality of
life, a health survey form, known as a Short Form-36 (SF-36), was
used. SF-36 is a widely used health survey constructed to measure
health-associated quality of life in eight dimensions with 36
questions (26). The dimensions are
presented in Table II. The answers
obtained from the 36 questions were scored according to SF-36
algorithms and interpreted according to a SF-36 scale, with a
minimum score of 0 and a maximum score of 100 (27). Reference material for Swedish women
in the general population was obtained from a previous study
(26) and originates from 4,582
Swedish women of 15–93 years, (mean age, 42.7 years).
| Table II.Health-associated quality of life
according to the eight dimensions of Short Form-36 and the
definitions of the lowest and highest scores in each dimension. |
Table II.
Health-associated quality of life
according to the eight dimensions of Short Form-36 and the
definitions of the lowest and highest scores in each dimension.
| Dimension | Lowest possible
score | Highest possible
score |
|---|
| Physical
functioning | Very limited,
including daily activities of personal hygiene and dressing | Not limited, can
perform all types of physical activities |
| Physical
health | Limited performance
at work or regular activities due to poor physical health | Not limited, can
perform and regular activities work |
| Bodily pain | Severe pain | No pain |
| General health | Perceives general
health status as poor and believes it will deteriorate | Perceives general
health status as excellent |
| Vitality | Feels constantly
tired and worn out | Feels constantly
alert and energetic |
| Social
functioning | Limited in social
activities due to physical or mental health status | Not limited, can
maintain normal social activities |
| Emotional
impact | Limited in work and
regular activities due to emotional status | Not limited, can
perform work and regular activities |
| Mental health | Feels constantly
depressed or nervous | Feels constantly
calm, harmonious and happy |
In order to perform a more thorough analysis, median
SF-36 health profiles were drawn for the study population. Median
SF-36 scores were calculated in each of the eight dimensions of
SF-36 for the total study population and for the following
subgroups: Women with VWD type 1, type 2 and type 3, women with no
menstrual bleeding, women with normal menstrual bleeding, and women
with HMB.
Statistical analysis
In order to identify the characteristics associated
with HMB and the various SF-36 scores, the study population was
arranged into subgroups according to the type of VWD and the amount
of menstrual bleeding. For the variables for which the answers
could be ranked according to an ordinal scale, the average ranking
sum was calculated for each subgroup and compared using a
non-parametric Kruskal-Wallis test. The null hypothesis was that
the populations from which the samples were collected had the same
distribution, and therefore had the same median. A statistically
significant result (P<0.05) with the Kruskal-Wallis test
indicated that at least one group was different from the
others.
The median SF-36 health profiles for the study
population and the subgroups were plotted and compared with the
median SF-36 health profiles of Swedish women from the general
population. In order to detect statistically significant
differences between the median SF-36 values of the study population
and the Swedish women of the general population, approximate
confidence intervals with P<0.10 were constructed for the median
values of the total study population and the subgroups with n≥15.
The approximate confidence intervals for the median values were
obtained through ranking of the SF-36 values in each dimension, and
the results obtained were compared to corresponding tabulated ranks
(28) for a 90% confidence interval.
A 90% confidence interval was selected due to the size of the study
population and the relatively low number of ranks obtained.
Ethical approval
The questionnaire was accompanied by a letter
explaining how and why the study was being performed and that
participation was voluntary, and written informed consent was
obtained from the patients. Ethical permission for the present
study was granted by the Central Ethical Review Board of Karolinska
Institute, Stockholm, Sweden (ethical permission registration no.
2007/1373-31/4).
Results
Characteristics of the study
population
The characteristics of the study population (30
women with VWD) were analyzed with regard to the type of VWD and
age. No statistically significant differences were observed in the
distribution of VWD types between the patients (Tables III and IV).
| Table III.Distribution of VWD type 1, 2 and
3. |
Table III.
Distribution of VWD type 1, 2 and
3.
| Parameter | Study population, n
(%) |
|---|
| Total | 30 (100) |
| VWD type 1 | 15 (50.0) |
| VWD type 2 | 11 (36.7) |
| VWD type 3 | 4 (13.3) |
| Table IV.Age distribution in the study
population. |
Table IV.
Age distribution in the study
population.
| Parameter | Value |
|---|
| Total patient
number, n | 30 |
| Mean age ± SD,
years | 35.1±8.1 |
| Minimum age,
years | 19 |
| Maximum age,
years | 51 |
HMB in women with VWD
The amount of menstrual bleeding based on the
woman's own experience, the incidence of HMB, and clinical
measurements, including frequency of menses, duration of flow and
volume of monthly blood loss, for the study population is presented
in Table V. The incidence of HMB
based on the women's personal evaluations was shown to be 50.0% in
the study population (n=30). The incidence of HMB based on clinical
measurements was shown to be 53.3%. Of the 15 women who reported
HMB, 73.3% had clinical measurements consistent with HMB. Of the
women who reported normal menstrual bleeding, 71.4% were revealed
to have clinical measurements that were consistent with HMB.
| Table V.Amount of menstrual bleeding in women
with VWD type 1, 2, and 3. |
Table V.
Amount of menstrual bleeding in women
with VWD type 1, 2, and 3.
| Menstrual
bleeding | Total (n=30), n
(%)a | HMB incidence,
nb | VWD type 1 (n=15),
n (%) | VWD type 2 (n=11),
n (%) | VWD type 3 (n=4), n
(%) |
|---|
| None | 8
(26.7) | 0 | 3
(20.0) | 3 (27.2) | 2 (50.0) |
| Normal | 7
(23.3) | 5 | 2
(13.3) | 4 (36.4) | 1 (25.0) |
| HMB | 15 (50.0) | 11 | 10 (66.7) | 4 (36.4) | 1 (25.0) |
In the study population, 66.7% of the women with VWD
type 1 reported HMB compared with 36.4% of the women with VWD type
2 and 25.0% of the women with VWD type 3. Likely due to the small
size of the subgroups, no significant differences (P>0.05) were
observed when comparing the amount of menstrual bleeding in women
with VWD type 1, 2 and 3. The reasons for having no menstrual
bleeding were pregnancy or breastfeeding (2 women), treatment with
LNG-IUS (4 women), continuous treatment with contraceptive pills (1
woman) and surgery (1 woman). In total, 5 women experienced their
menstrual bleeding as normal, although they had clinical
measurements consistent with HMB. Furthermore, 4 women reported
their menstruation as HMB, although they lacked clinical
measurements consistent with HMB (Table
V).
Treatment for HMB
The majority of the women (24/30; 80.0%) received
pharmacologic treatment for HMB (Table
VI). Based on clinical measurements of menstrual bleeding, the
treatment was demonstrated to be effective in 10/24 (41.7%) of the
cases, whereas based on the women's evaluation, treatment was
considered to be effective in 15/24 (62.5%) of the cases (data not
shown). Only 3 women with menstruation did not receive any
pharmacological treatment for HMB, and 2 of these had clinical
measurements consistent with HMB (Table
VI).
| Table VI.Pharmacological treatment of HMB. The
number of women who received pharmacological treatment for HMB, the
type of treatment they received, and the resulting menstrual
bleeding based on clinical measurements. |
Table VI.
Pharmacological treatment of HMB. The
number of women who received pharmacological treatment for HMB, the
type of treatment they received, and the resulting menstrual
bleeding based on clinical measurements.
|
| Treatment, n | Type of
pharmacological treatment, n |
|---|
|
|
|
|
|---|
| Clinical menstrual
bleeding | Yes | No | LNG-IUS | PCP | DDAVP | TA | VWF/FVIII | Other |
|---|
| None (n=8) | 5 |
3a | 4 |
1b | 0 | 0 | 0 | 0 |
| Normal (n=6) | 5 | 1 | 1 | 1 | 4 | 0 | 0 | 1 |
| HMB (n=16) | 14 | 2 | 0 | 2 | 1 | 12 | 2 | 0 |
| Total
(n=29)c | 24 | 6 | 5 | 4 | 5 | 12 | 2 | 1 |
Impact of menstruation on overall life
activities
The perceived impact of menstruation on overall life
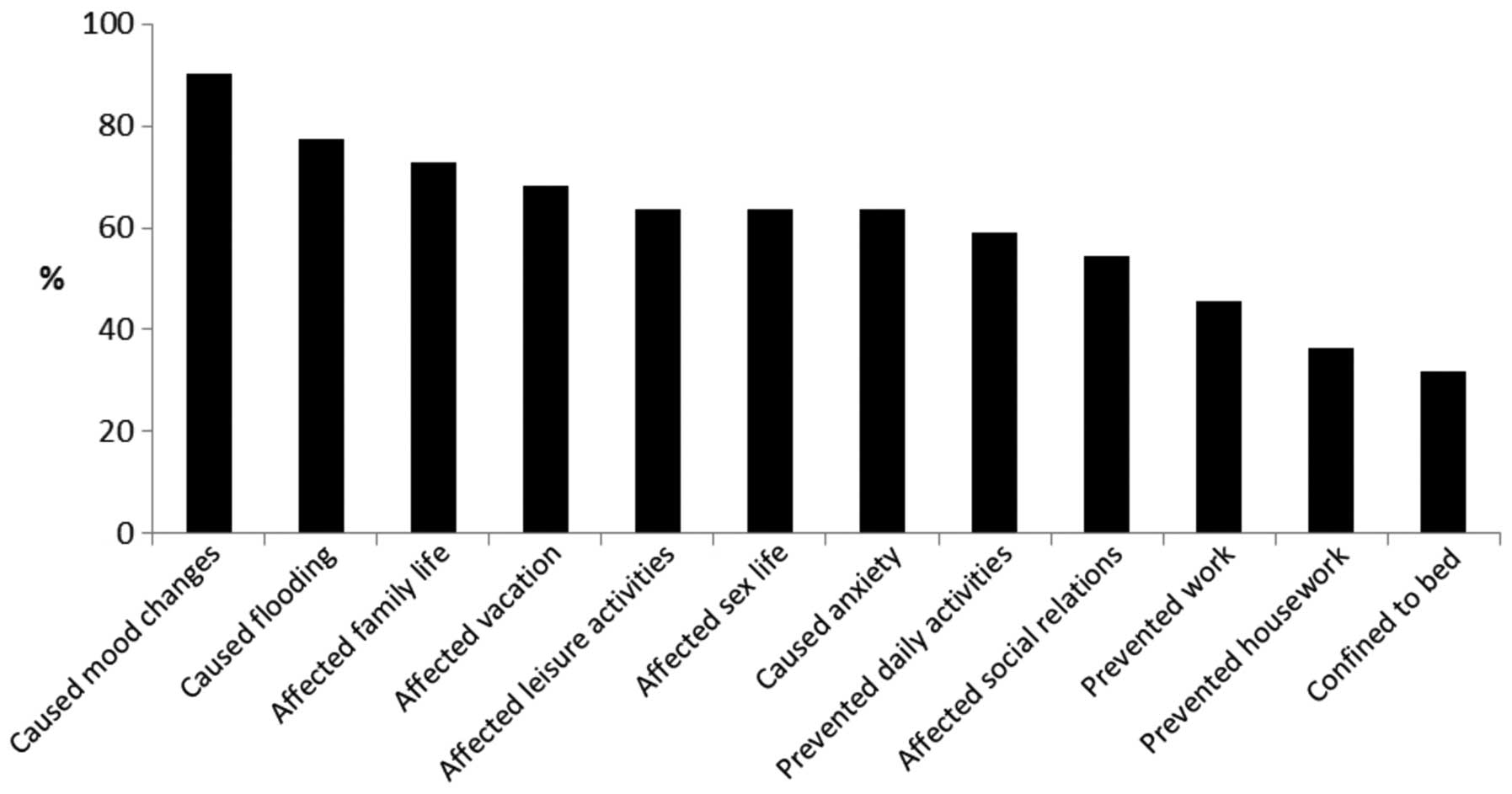
activities was found to be substantial (Fig. 1). The data showed that of the 22
women with menstruation, 1 woman reported no limitations in overall
life activities, 2 women reported limitations in less than three
areas of overall life activities, and the remaining 19 women
reported limitations in three areas or more of their overall life
activities. Menstruation was reported to affect women in a high
percentage of cases in the following ways: Mood changes (90.9%),
heavy bleeding (77.3%), family life (72.7%) and vacations (68.2%),
with over two thirds of women with VWD reporting limitations in
these areas. Menstruation also affected leisure activities (63.6%)
and sex life (63.6%), caused anxiety (63.6%), prevented daily
activities (59.1%)and markedly affected social relations (54.5%),
with over half of the women reporting these limitations.
Approximately half of the women (45.5%) reported that their ability
to work was negatively affected by menstruation. The ability to
carry out housework was less affected by menstruation, although
more than one third (36.4%) reported limitations. Approximately one
third of women (31.8%) with VWD were confined to bed for over half
a day during the menstrual period.
Health-associated quality of life
Completed SF-36 health surveys were received from 29
of the 30 women in the study population. Median SF-36 health
profiles for the total study population and for the subgroups for
women with VWD type 1, 2 and 3, and women with no menstrual
bleeding, normal menstrual bleeding and HMB, are presented in
Fig. 2. Significant differences were
not identified in any of the eight dimensions of SF-36 when the
median SF-36 scores of the total study population were compared
with the median SF-36 scores of Swedish women in the general
population (Fig. 2A). However, in
the SF-36 dimension of vitality, the score of the Swedish women in
the general population was equal to the upper limit of the
confidence interval for women with VWD, and the statistical
difference was almost reached statistically significant. The median
SF-36 scores of women with VWD type 1, 2 and 3 appeared to be lower
compared with the scores of Swedish women in the general
population, although no significant differences were be identified
(Fig. 2B). The median SF-36 scores
of women with no menstruation, normal menstrual bleeding and HMB
were compared separately with the median SF-36 scores of Swedish
women in the general population (Fig.
2C). In the dimension of bodily pain, the group of women with
HMB had significantly lower scores compared with those of women in
the general Swedish population (Fig.
2D). This implies that the women in the study population with
HMB experienced an impaired health-associated quality of life due
to pain.
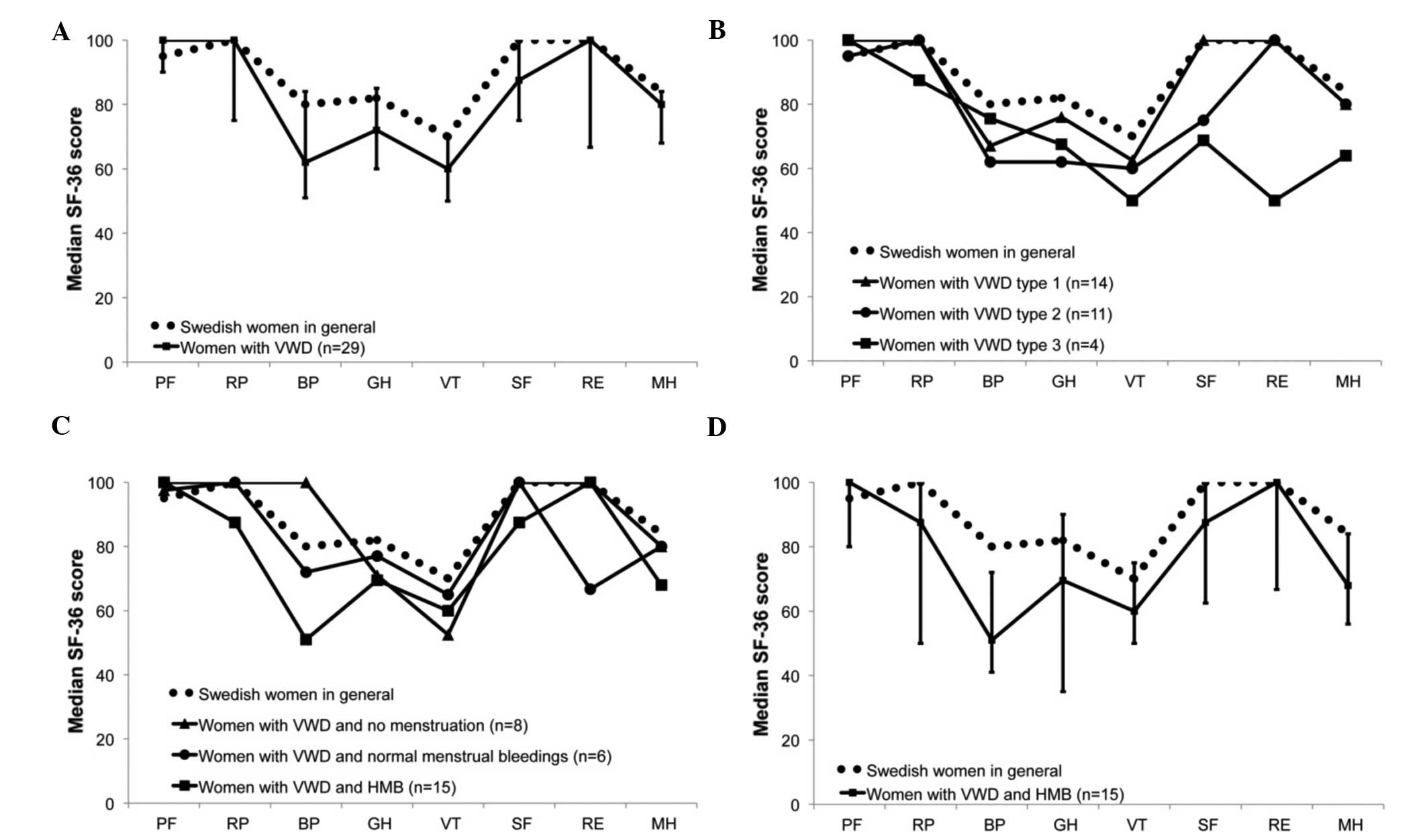 | Figure 2.Health profiles for the study
population. Median SF-36 scores in each dimension of SF-36
presented as health profiles for the total study population and
subgroups of the study population. (A) The health profile of the
total study population compared with the health profile of Swedish
women of the general population. Error bars represent the
approximate confidence interval (P<0.10) for the median SF-36
scores of the study population. (B) The health profiles for women
with VWD type 1, 2 and 3 compared with the health profile of
Swedish women in the general population. (C) The health profiles of
women with no menstrual bleeding, normal menstrual bleeding and HMB
compared with the health profile of Swedish women in the general
population. (D) The health profiles of women with HMB compared with
the health profiles of Swedish women in the general population.
Error bars represent the approximate confidence interval
(P<0.10) for the median SF-36 scores of women with HMB. VWD, von
Willebrand's disease; HMB, heavy menstrual bleeding; PF, Physical
Functioning; RP, role-physical; BP, bodily pain; GH, general
health; VT, vitality; SF, social functioning; RE, role-emotional;
MH, mental health. |
Comparison of the SF-36 scores between the types of
VWD demonstrated the absence of significant differences in
SF-scores between women with VWD type 1, 2 and 3. Similarly,
according to the amount of menstrual bleeding, there were no
significant differences in the SF-36 scores between women without
menstruation, with normal menstrual bleeding and with HMB.
Discussion
The present study presented two important results:
Firstly, women with VWD were found to experience severe HMB,
although the majority of these women were receiving pharmacologic
treatment. Therefore, the pharmacologic treatment of HMB in women
with VWD appears to be insufficient, and requires optimization.
Secondly, the perceived impact of menstruation on the overall life
activities was demonstrated to be substantial, and the majority of
women in the study population were limited in several areas. The
health-associated quality of life was lower in the study population
compared with the Swedish women in the general population. A
significant difference was identified in the bodily pain SF-36
dimension in the study population with HMB, as compared with
Swedish women in the general population.
The study population was carefully selected from the
Coagulation Unit at the Karolinska University Hospital, and all
women had a known and documented diagnosis on the type of VWD.
Therefore, despite the small size of the study population, the
selection process may still be regarded as a strength of the
present investigation.
The incidence of HMB in the present study
(50.0–53.3%) was concordant with the results of recent studies
performed by Rae et al (29),
Byams et al (30) and Kirtava
et al (12) that reported
incidence of 45.2, 51.7 and 44%, respectively. Regarding the study
population, the women in the aforementioned studies were connected
to hematology centers, as in the present study.
Among the 22 women with menstruation, 5 women
evaluated their menstrual bleeding as normal although their PBAC
scores were consistent with HMB. One possible explanation is that
their menstruation was decreased (but remained heavy) following
treatment with TA for instance, as compared with their menstruation
flow prior to treatment, and hence they considered it normal.
Another explanation may be that they compared their menstruation to
that of their mother or sister, and taking into account the
hereditary nature of VWD, this assessment may be false. Among the
22 women with menstruation, 4 women experienced their menstruation
as HMB though they lacked clinical measurements consistent with
HMB.
Women with VWD who were treated with LNG-IUS had no
or normal menstrual bleeding, whereas women treated with TA
continued to have HMB. These results were concordant with a
long-term follow-up (5 years) study conducted by Chi et al
(31) on LNG-IUS in 18 women with
HMB, who had inherited bleeding disorders and a median PBAC score
of 255. Follow-up demonstrated that 42% of the women had no
menstrual bleeding, and the remaining had a PBAC score of <100,
indicating normal menstrual bleeding (31). In a recent review on TA for the
treatment of HMB, Leminen et al (32) compared the effect of TA to that of
LNG-IUS, and concluded that TA was significantly less effective
than LNG-IUS at reducing HMB. In addition, TA reduced menstrual
bleeding by 47% compared with 83% following treatment with
LNG-IUS.
The number of women with VWD and HMB treated with
LNG-IUS appears to be low. The reasons for this are various, and
may include a cautious view among women on hormonal contraceptives,
a wish to get pregnant or not having received appropriate
counseling on menstrual bleeding, thus indicating an importance of
thorough counseling from gynecologists.
Women with VWD perceived limitations in overall life
activities due to menstruation. These results were concordant with
those of previous studies, which demonstrated that a higher number
of women with VWD compared with women in the general population
perceived limitations in their overall life activities due to
menstruation (12,29). Kirtava et al (12) performed a case control study on 62
women with VWD and demonstrated that 23 (32.1%) of these women
perceived menstrual bleeding to limit their overall life activities
and negatively affect their lives. Among the 70 controls of the
study, only 7 women (10.0%) perceived limitations (12). A study performed by Rae et al
(29) concluded that among 84 women
with inherited bleeding disorders and HMB, the majority (77.5%)
reported that menstrual bleeding interfered with daily
activities.
The health-associated quality of life according to
SF-36 appeared to be lower in the study population compared with
Swedish women in the general population. However, the differences
in median SF-36 scores were not statistically significant. It is
possible that the lack of statistical significance was due to the
small sample size of the study population, since several earlier
studies demonstrated that women with VWD had lower
health-associated quality of life compared with women in the
general population (14,28). The studies by Solovieva (33) and de Wee et al (34) reported that the ‘vitality’ SF-36
dimension was negatively affected in women with VWD. In the present
study, women with HMB had a significantly lower SF-36 score in the
dimension ‘bodily pain’. These results were concordant with those
obtained by Rae et al (29)
who used the self-administered health survey, Health Utilities
Index of Canada. In a group of 84 women with inherited bleeding
disorders and HMB, Rae et al (29) demonstrated that the health-associated
quality of life scores were lower in the dimensions ‘pain’ and
‘cognition’. They also reported that women with VWD (n=259)
experienced significantly more pain than women with other bleeding
disorders (n=56) and men with VWD (n=97).
To quantify menstrual blood loss, self-reported
measurements including information from the questionnaire and PBAC
were used. There are conflicting results regarding the accuracy of
the PBAC (35,36). However, the PBAC is an easily
administrated method that is employed in clinical practice and
research on menstrual bleeding.
In conclusion, in the present study, 50.0% of the
study population reported HMB, even though the majority (80%)
received pharmacologic treatment for HMB. This indicates that
treatment does not prevent HMB in numerous cases. In addition,
LNG-IUS should be used more as a cessation of menstruation, since
it often improves the quality of life. Furthermore, the perceived
impact of menstruation on overall life activities was substantial.
To prevent unnecessary limitations in overall life activities and
health-associated quality of life, thorough counseling regarding
menstrual bleeding and pain is important in the care of women with
VWD.
Acknowledgements
The authors of the present study are grateful to
Mrs. Elisabeth Berg, Department of Learning, Informatics,
Management and Ethics, Karolinska Institute for advice on
statistics.
Glossary
Abbreviations
Abbreviations:
|
HMB
|
heavy menstrual bleeding
|
|
LNG-IUS
|
levonorgestrel-releasing intrauterine
system
|
|
SF-36
|
short form-36
|
|
PBAC
|
pictorial blood-loss assessment
chart
|
|
VWD
|
von Willebrand's disease
|
|
VWF
|
von Willebrand factor
|
References
|
1
|
Bowman M, Hopman W, Rapson D, Lillicrap D
and James P: The prevalence of symptomatic von Willebrand disease
in primary care practice. J Thromb Haemost. 8:213–216. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Castaman G, Eikenboom JC, Bertina RM and
Rodeghiero F: Inconsistency of association between type 1 von
Willebrand disease phenotype and genotype in families identified in
an epidemiological investigation. Thromb Haemost. 82:1065–1070.
1999.PubMed/NCBI
|
|
3
|
Rodeghiero F, Castaman G and Dini E:
Epidemiological investigation of the prevalence of von Willebrand's
disease. Blood. 69:454–459. 1987.PubMed/NCBI
|
|
4
|
Werner EJ, Broxson EH, Tucker EL, Giroux
DS, Shults J and Abshire TC: Prevalence of von Willebrand disease
in children: A multiethnic study. J Pediatr. 123:893–898. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
James AH: Von Willebrand disease in women:
Awareness and diagnosis. Thromb Res. 124(Suppl 1): S7–S10. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
National Institute for Health and Clinical
Excellence: Guidance: Heavy Menstrual Bleeding. National
Collaborating Centre for Women's and Children's Health (UK)
(London). 2007.
|
|
7
|
Hallberg L, Högdahl AM, Nilsson L and Rybo
G: Menstrual blood loss-a population study. Variation at different
ages and attempts to define normality. Acta Obstet Gynecol Scand.
45:320–351. 1966. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lukes AS, Kadir RA, Peyvandi F and Kouides
PA: Disorders of hemostasis and excessive menstrual bleeding:
Prevalence and clinical impact. Fertil Steril. 84:1338–1344. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Committee on Adolescent Health Care;
Committee on Gynecologic Practice: Committee Opinion No. 580: Von
Willebrand disease in women. Obstet Gynecol. 122:1368–1373. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Davidson BR, Dipiero CM, Govoni KD,
Littleton SS and Neal JL: Abnormal uterine bleeding during the
reproductive years. J Midwifery Womens Health. 57:248–254. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lassila R, Holme PA, Landorph A, Petrini
P, Onundarson PT and Hillarp A: Nordic haemophilia council's
practical guidelines on diagnosis and management of von Willebrand
disease. Semin Thromb Hemost. 37:495–502. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kirtava A, Drews C, Lally C, Dilley A and
Evatt B: Medical, reproductive and psychosocial experiences of
women diagnosed with von Willebrand's disease receiving care in
haemophilia treatment centres: A case-control study. Haemophilia.
9:292–297. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kuzmina N, Palmblad J and Mints M:
Predictive factors for the occurrence of idiopathic menorrhagia:
Evidence for a hereditary trait. Mol Med Rep. 4:935–939.
2011.PubMed/NCBI
|
|
14
|
Barr RD, Sek J, Horsman J, Furlong W,
Saleh M, Pai M and Walker I: Health status and health-related
quality of life associated with von Willebrand disease. Am J
Hematol. 73:108–114. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Côté I, Jacobs P and Cumming D: Work loss
associated with increased menstrual loss in the United States.
Obstet Gynecol. 100:683–687. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hagstad A: Gynecology and sexuality in
middle-aged women. Women Health. 13:57–80. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sadler JE, Budde U, Eikenboom JC, Favaloro
EJ, Hill FG, Holmberg L, Ingerslev J, Lee CA, Lillicrap D, Mannucci
PM, et al: Update on the pathophysiology and classification of von
Willebrand disease: A report of the Subcommittee on von Willebrand
Factor. J Thromb Haemost. 4:2103–2114. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dunn CJ and Goa KL: Tranexamic acid: A
review of its use in surgery and other indications. Drugs.
57:1005–1032. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kaufmann JE and Vischer UM: Cellular
mechanisms of the hemostatic effects of desmopressin (DDAVP). J
Thromb Haemost. 1:682–689. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mannucci PM: How I treat patients with von
Willebrand disease. Blood. 97:1915–1919. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bahamondes L, Bahamondes MV and Monteiro
I: Levonorgestrel-releasing intrauterine system: Uses and
controversies. Expert Rev Med Devices. 5:437–445. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lethaby A, Irvine GA and Cameron I:
Cyclical progestogens for heavy menstrual bleeding. Cochrane
Database Syst Rev. 2008. View Article : Google Scholar
|
|
23
|
Ruta DA, Garratt AM, Chadha YC, Flett GM,
Hall MH and Russell IT: Assessment of patients with menorrhagia:
How valid is a structured clinical history as a measure of health
status? Qual Life Res. 4:33–40. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Coulter A, Peto V and Jenkinson C: Quality
of life and patient satisfaction following treatment for
menorrhagia. Fam Pract. 11:394–401. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Higham JM, O'Brien PM and Shaw RW:
Assessment of menstrual blood loss using a pictorial chart. Br J
Obstet Gynaecol. 97:734–739. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sullivan M, Karlsson J, Taft C and Ware
JE: SF-36 health survey: Swedish manual and interpretation guide.
Sahlgrenska University Hospital. Gothenburg: 2002.(In Swedish).
|
|
27
|
Sullivan M, Karlsson J and Ware JE Jr: The
Swedish SF-36 health survey - I. Evaluation of data quality,
scaling assumptions, reliability and construct validity across
general populations in Sweden. Soc Sci Med. 41:1349–1358. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Altman DG: Practical statistics for
medical research. Chapman & Hall. London: 1999.
|
|
29
|
Rae C, Furlong W, Horsman J, Pullenayegum
E, Demers C, St-Louis J, Lillicrap D and Barr R: Bleeding
disorders, menorrhagia and iron deficiency: Impacts on
health-related quality of life. Haemophilia. 19:385–391. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Byams VR, Kouides PA, Kulkarni R, Baker
JR, Brown DL, Gill JC, Grant AM, James AH, Konkle BA, Maahs J, et
al: Surveillance of female patients with inherited bleeding
disorders in United States haemophilia treatment centres.
Haemophilia. 17(Suppl 1): 6–13. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chi C, Huq FY and Kadir RA:
Levonorgestrel-releasing intrauterine system for the management of
heavy menstrual bleeding in women with inherited bleeding
disorders: Long-term follow-up. Contraception. 83:242–247. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Leminen H and Hurskainen R: Tranexamic
acid for the treatment of heavy menstrual bleeding: Efficacy and
safety. Int J Womens Health. 4:413–421. 2012.PubMed/NCBI
|
|
33
|
Solovieva S: Clinical severity of disease,
functional disability and health-related quality of life.
Three-year follow-up study of 150 Finnish patients with coagulation
disorders. Haemophilia. 7:53–63. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
de Wee EM, Mauser-Bunschoten EP, Van Der
Bom JG, Degenaar-Dujardin ME, Eikenboom HC, Fijnvandraat K, de
Goede-Bolder A, Laros-van Gorkom BA, Meijer K, Raat H, et al:
Health-related quality of life among adult patients with moderate
and severe von Willebrand disease. J Thromb Haemost. 8:1492–1499.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zakherah MS, Sayed GH, El-Nashar SA and
Shaaban MM: Pictorial blood loss assessment chart in the evaluation
of heavy menstrual bleeding: Diagnostic accuracy compared to
alkaline hematin. Gynecol Obstet Invest. 71:281–284. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Reid PC, Coker A and Coltart R: Assessment
of menstrual blood loss using a pictorial chart: A validation
study. BJOG. 107:320–322. 2000. View Article : Google Scholar : PubMed/NCBI
|