Introduction
Postoperative cognitive dysfunction (POCD) is a
frequent neurological complication after anesthesia. The main
clinical manifestations include mental disorder, anxiety,
personality changes, and memory impairment; the personality, social
skill, and cognitive changes occurring postoperatively are typical
manifestations of POCD (1). The
incidence rate of POCD among adults older than 75 years of age
after general anesthesia was reported to be 40–50% (1). It was demonstrated that the type of
operation, genetics, cholinergic function, Alzheimer's disease
molecular neuropathology basis, and anesthesia were correlated with
β-amyloid protein (Aβ) and cholinergic system dysfunction, as well
as the roles of different narcotic drugs (2).
Neurological damage and persistent inflammation can
cause a significant increase in Aβ and can be used as one of the
potential serological markers for diagnosing POCD. The increase in
Aβ in the brain may be closely associated with cognitive
dysfunction. Furthermore, Aβ in the brain may accumulate and the
cerebrospinal fluid concentration may be increased; therefore,
plasma Aβ concentration may reflect the concentration of Aβ in the
cerebrospinal fluid (3). This
further reflects the degree of POCD, and Aβ is expected to become
one of the serological biomarkers for predicting the occurrence and
prognosis of POCD (3). Recent
findings showed that, in subtotal gastrectomy patients, the
occurrence and development of POCD may be significantly correlated
with regional cerebral oxygen saturation (rSO2)
(4). In elderly patients, the
incidence rate of gastric cancer is increasing annually (5). Subtotal gastrectomy is a major
operation for gastric cancer, the operative time is long and is
further extended by waiting for pathological results and dissecting
local lymph nodes. When the long operative time under general
anesthesia causes hypoventilation or other respiratory system
complications, the gas exchange capacity is impaired and
desaturation rSO2 often results, which may be
significantly correlated with neurological complications, cognitive
function, and prolonged length of stay (6,7).
Therefore, it is important to detect early diagnosis indicators and
serological markers of POCD so that it can be prevented after
subtotal gastrectomy.
The present study examined the role of Aβ and
rSO2 on POCD of elderly patients undergoing subtotal
gastrectomy and its significance and provides theoretical support
for the prevention and treatment of POCD based on a review of
previous studies.
Materials and methods
Patients
In total, 168 patients (mean age, 64.5±10.7 years)
who underwent subtotal gastrectomy under general anesthesia from
June 2014 to December 2015 in Traditional Chinese Medical Hospital
of Rizhao were included.
Patients diagnosed and confirmed as having stomach
cancer or ulcers pathologically by imaging and in line with the
subtotal gastrectomy treatment evidence and patients >60 years
of age, were included in the study.
Exclusion criteria for the study were: i)
Immunosuppressant treatments; ii) acute and chronic bacterial
and/or viral infection; iii) autoimmune diseases; iv) connective
tissue diseases; v) malignancy; vi) liver and kidney dysfunction;
vii) chronic muscle disease; viii) peripheral vascular disease,
chronic heart failure, thyroid disease, liver and kidney
dysfunction, cancer, major trauma in the previous six months and a
history of surgical operation; ix) diabetes; x) New York Heart
Association class III and IV; xi) in the previous six months,
myocardial infarction, percutaneous transluminal coronary
angioplasty, coronary artery bypass graft surgery history, and
recent application of adrenocortical hormone or other
immunomodulatory agents; as well as patients not cooperating with
their families, or history of mental illness.
Research methods
Mini-Mental State Examination (MMSE) (8): 1 point for each correct answer, 0
points for wrong or unknown, 9 points for inappropriate answer, 8
points for refusing to answer or not understanding. When
calculating the total score, 8 and 9 points were regarded as 0. The
highest score was 30 points. The division of dementia was
correlated with educational background; thus, if the elderly adult
was illiterate and scored <17 points, graduated from primary
school and scored <20 points, graduated from secondary school or
over and scored <24 points, the patient was considered to have
dementia. Allocation of points was: Normal, 27–30 points; mild,
21–26 points; moderate, 10–20 points; and severe, 0–9 points.
Montreal Cognitive Assessment (MoCA)
(9)
The testing included visual memory, executive
capacity, naming, memory, attention, verbal fluency, abstract
thinking, delayed memory, and orientation, for a total of 30
points. One point was added to the test results if the subject had
<12 years of education, and the education level bias was
correlated. Higher scores indicated better cognitive function of
the subjects; ≥26 points indicated normal cognition.
Sample collection
After the patients fasted overnight, 3-ml venous
blood was extracted from their elbow; 1.2 ml blood was injected
into an ordinary plastic tube, and 1.8 ml was injected into an
anticoagulant tube containing 0.2-ml 3.8% sodium citrate and
centrifuged for 10 min at 1,006.2 × g within 1 h after sample
collection. The serum or plasma after extraction was placed in a
0.5 ml EP tube, stored at −30°C and then tested within 1 month.
Expression levels of serum Aβ
Enzyme-linked immunosorbent assay (ELISA) was used
to test the expression levels of serum Aβ. The reagents employed in
the present study were purchased from Wuhan Boster Biological
Engineering Co., Ltd. (Wuhan, China), and ELISA was performed in
full accordance with the operating instructions.
Operative methods
The patients fasted for 8 h before the operation.
The peripheral venous access was opened, and radial artery puncture
catheterization was conducted under local anesthesia and then
connected to the pressure sensor to monitor arterial pressure.
Anesthesia was induced with 0.05 mg/kg intravenous midazolam, 0.3
mg/kg etomidate, 10 µg/kg fentanyl, and 0.5 mg/kg cisatracurium;
after endotracheal intubation, mechanical gas exchange was carried
out. The abdomen was explored through a central abdominal incision;
the greater curvature was separated, and then the lesser curvature
(including the right and left gastric arteries). The duodenum and
stomach walls were separated and the body of stomach was cut-off
for gastrointestinal anastomosis. After anastomosis was complete
and the confirmation that there was no residual fistula, the
surrounding lymph nodes were further dissected and then the abdomen
was closed.
Measurement of rSO2
Statistical analysis
Measurement data were presented as mean ± standard
deviation (mean ± SD). SPSS 17.0 software (Chicago, IL, USA) was
used for processing. The repeated measures analysis of variance was
applied for statistical analysis, the t-test for two independent
samples was used for the measurement data among groups, the paired
t-test was used for comparison between groups, and the countable
data were tested with χ2 test. P<0.05 was considered
to indicate a statistically significant difference.
Results
Comparison of baseline data of the
included patients
We enrolled, recorded, and carried out statistical
analysis of the age, weight, body mass index (BMI), and other
baseline data of 168 patients with subtotal gastrectomy [28 with
POCD (POCD group) and 140 without POCD (control group)] and 168
healthy patients (healthy control group), and there was no
statistically significant difference in baseline data among the
three groups (P>0.05) (Table
I).
 | Table I.Comparison of baseline data of
included patients (mean ± SD). |
Table I.
Comparison of baseline data of
included patients (mean ± SD).
| Groups | N | Age (years) | BMI
(kg/m2) | Operation time
(min) | Blood loss (ml) | MAP (mmHg) |
|---|
| POCD | 28 | 64.5±12.7 | 21.7±1.2 | 192.3±27.4 | 178.3±22.9 | 78.3±12.4 |
| Control | 140 | 66.7±9.5 | 20.4±0.8 | 196.5±20.1 | 183.4±20.5 | 77.3±10.4 |
| Healthy control | 168 | 65.6±10.8 | 20.7±1.3 | – | – | 76.5±10.9 |
| T-value | – | 0.33 | 1.49 | 0.93 | 0.37 | 1.33 |
| P-value | – | 0.47 | 0.12 | 0.18 | 0.29 | 0.28 |
MMSE and MoCA scores of patients in
each group
MMSE and MoCA were administered to all the patients
on the day before the operation, and on the second and ninth days
after the operation. In total, 28 cases demonstrated cognitive
dysfunction (POCD group) and 140 patients (control group) did not
demonstrate cognitive dysfunction. MMSE and MoCA scores of the
patients in the POCD group were statistically significantly
decreased compared with the control group (P<0.05) (Table II).
| Table II.MMSE and MoCA scores of surgical
patients in each group. |
Table II.
MMSE and MoCA scores of surgical
patients in each group.
| Item | Groups | N | One day before
operation | Two days after
operation | Nine days after
operation | P-value |
|---|
| MMSE | POCD | 28 | 28.3±1.6 | 26.3±1.4 | 22.3±3.2 | 0.01 |
|
| Control | 140 | 29.2±1.7 | 29.5±2.8 | 28.4±2.2 | 0.38 |
|
| t-test | – | 0.33 | 8.36 | 10.29 | – |
|
| P-value | – | 0.69 | 0.04 | 0.04 | – |
| MoCA | POCD | 28 | 29.6±0.4 | 21.1±1.8 | 21.4±1.3 | 0.03 |
|
| Control | 140 | 28.7±1.5 | 26.3±2.6 | 28.3±0.8 | 0.98 |
|
| t-test | – | 0.42 | 20.48 | 20.78 | – |
|
| P-value | – | 0.38 | 0.02 | 0.02 | – |
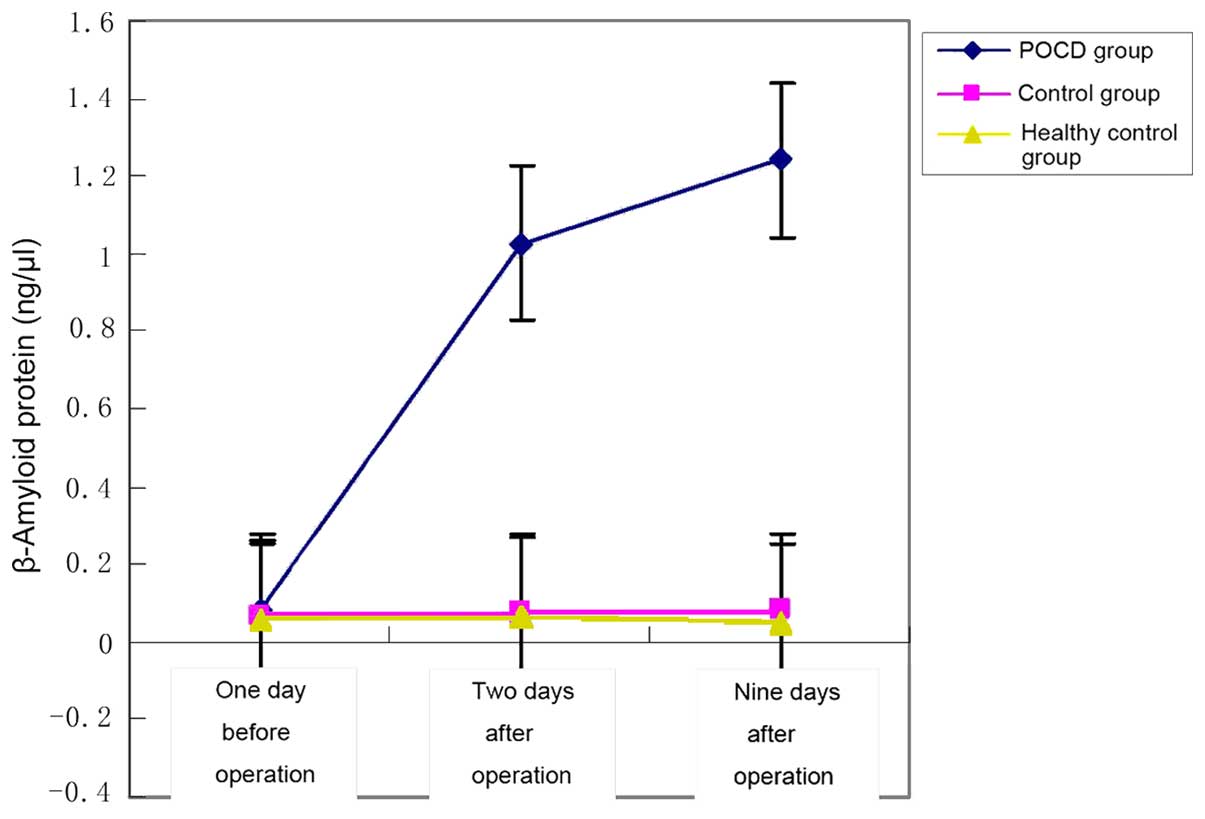
ELISA was used to test the peripheral
Aβ levels of patients and healthy controls
We tested Aβ levels of the 168 patients with
subtotal gastrectomy and 168 healthy controls and found that serum
Aβ levels of POCD patients were statistically significantly higher
than those in the control and healthy control groups (P<0.05)
(Table III and Fig. 1).
| Table III.ELISA was used to test the peripheral
Aβ levels of patients and healthy controls (ng/µl). |
Table III.
ELISA was used to test the peripheral
Aβ levels of patients and healthy controls (ng/µl).
| Groups | N | One day before
operation | Two days after
operation | Nine days after
operation | P-value |
|---|
| POCD | 28 | 69.81±6.33 |
102.7±14.5a |
112.4±14.2c | 0.002 |
| Control | 140 | 64.27±13.25 |
75.24±11.3b |
82.3±10.1d | 0.231 |
| Healthy
control | 168 | 65.37±10.81 | 67.3±2.5 | 65.2±4.38 | 0.819 |
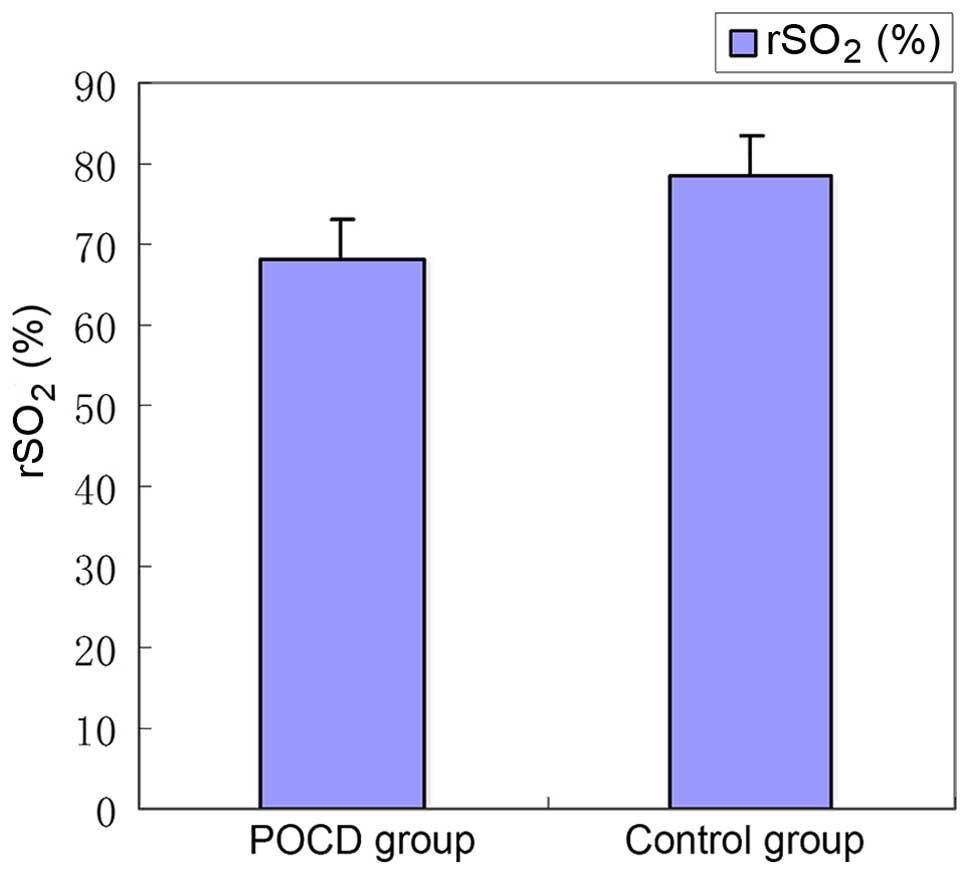
Comparison of rSO2 levels
in the two surgical groups
A comparison of the intraoperative mean
rSO2 of patients in the POCD and control groups showed
that the mean rSO2 in the sPOCD group during the
operation was significantly lower than that in the control group,
and the difference was statistically significant (P<0.05)
(Table IV and Fig. 2).
| Table IV.Comparison of rSO2 levels
between the two surgical groups. |
Table IV.
Comparison of rSO2 levels
between the two surgical groups.
| Groups | N | rSO2
(%) |
|---|
| POCD | 28 | 68.2
(60–88)a |
| Control | 140 | 78.3
(69–92)a |
| t-test | – | 12.7 |
| P-value | – | 0.03 |
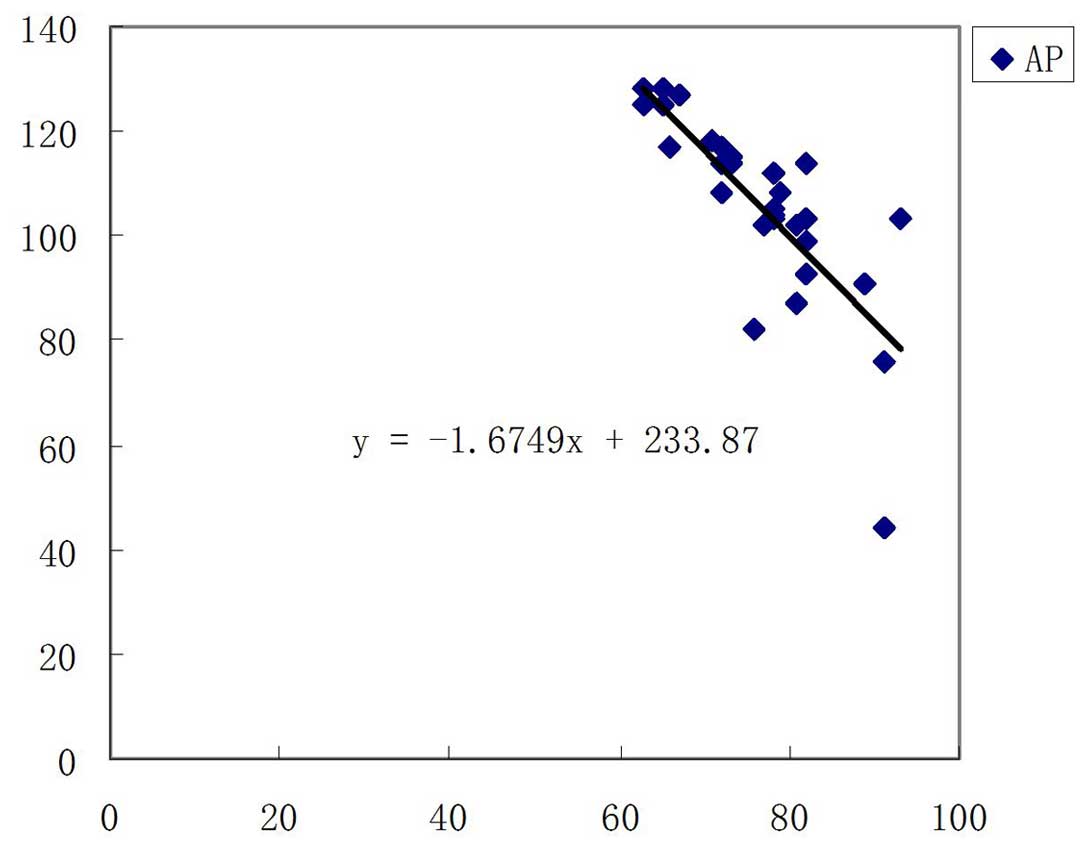
Correlation analysis of Aβ and
rSO2
We carried out the correlation analysis with Aβ as
an independent variable and gender, age, BMI, MMSE and MoCA scores,
and rSO2 as dependent variables. The results showed
that, Aβ levels were negatively correlated with rSO2,
and the difference was statistically significant (P<0.05)
(Table VA and B, and Fig. 3).
| Table V.Correlation analysis and multiple
linear regression analysis. |
Table V.
Correlation analysis and multiple
linear regression analysis.
| A, Correlation
analysis (r) of Aβ and clinical testing indicators |
|---|
|
|---|
| Indicators | Gender | Age | BMI |
rSO2 | MMSE | MoCA |
|
|---|
| Aβ |
| r | 0.02 | 0.35 | 0.29 | −1.6749 | −0.14 | −0.38 |
|
|
P-value | >0.05 | >0.05 | >0.05 | <0.05 | >0.05 | >0.05 |
|
|
| B, Multiple linear
regression analysis of Aβ level influencing factors |
|
|
| 95% CI |
|
|
|
| Variable | β | SE | β′ | t-test | P-value | Upper limit | Lower limit |
|
|
rSO2 | 0.571 | 0.16 | 0.784 | 0.432 | <0.05 | 0.29 | 0.87 |
Comparison of intraoperative data and
postoperative length of stay between POCD group and control
group
To study the intraoperative influence of POCD,
intraoperative data and postoperative length of stay were compared
between the POCD and control patients. Operation time,
intraoperative blood loss, and cardiopulmonary bypass time were not
significantly different between the two groups (P>0.05), but
postoperative length of stay was significantly prolonged in the
POCD group (P<0.05) (Table
VI).
| Table VI.Comparison of intraoperative data and
postoperative length of stay between POCD and control groups. |
Table VI.
Comparison of intraoperative data and
postoperative length of stay between POCD and control groups.
| Groups | No. of cases | Operation time
(min) | Amount of bleeding
(ml) | Postoperative
length of stay (days) |
|---|
| POCD | 28 | 187.4±21.4 | 287.4±68.7 | 22.4±2.8 |
| Control | 140 | 190.3±25.3 | 298.6±48.2 | 14.3±1.7 |
| T-value | – | 1.28 | 0.59 | 18.5 |
| P-value | – | 0.21 | 0.48 | 0.012 |
Discussion
At present, the pathogenesis of POCD remains
unclear. However, the dysfunction involving the central nervous
system, endocrine system, and immune system may contribute to the
pathogenesis of POCD (10).
Furthermore, Aβ is produced by many cells and circulates in the
blood, cerebrospinal fluid, and brain interstitial fluid, and the
studies show that Aβ is neurotoxic, and Aβ1-42 is especially toxic
(11,12).
Aβ deposition is not only correlated with neuronal
degenerative disease, but can also activate a series of
pathological changes in the central nervous system, including
activation of astrocytes and microglia, breakdown of the
blood-cerebrospinal fluid barrier, and microcirculation
disturbance. In a previous report, neuronal degeneration was often
seen in the region of the senile plaques in the brains of patients
with Alzheimer's disease, which may cause death (13). In the current study, we found that
expression levels of serum Aβ were statistically significantly
higher in patients with POCD than controls and healthy controls
(P<0.05). We believe that this may be correlated with longer
operative times and potential brain damage caused by
hypoventilation. Therefore, we confirmed this hypothesis by further
monitoring the intraoperative rSO2. We found that, in
the patients with postoperative POCD, the rSO2 level was
significantly higher than those of patients without
(P<0.05).
rSO2 monitoring is continuous and
non-invasive. The oxygen saturation of cerebral hemoglobin can be
intraoperatively monitored in real time by monitoring the mixing
transmission intensity of the oxyhemoglobin and reduced hemoglobin
of head and neck. The normal value of rSO2 is 55–75%.
The ratio of cerebral arterial/venous flow is 15:85 (14). Therefore, rSO2 mainly
shows cerebral venous oxygen saturation and reflects the balance
between supply and demand of oxygen (13,15). As
the most sensitive system to hypoxia stimulation in the body, the
central nervous system has a high oxygen demand. The cerebral blood
flow accounts for 15% of total cardiac output under a rest state,
and oxygen consumption accounts for 23% of total oxygen
consumption. Under a normal physiological status, Aβ that can be
detected in the blood and cerebrospinal fluid is usually at lower
levels, because the body has a strong scavenging activity for Aβ
(16). If peripheral Aβ antibody
(immunoglobulin G) permeates into the brain, it can bond with Aβ,
forming a kind of immune complex precipitation and activating the
microglia, thereby cleaning up the deposition of Aβ. However,
intraoperative hypopnea results in microglial physiological
dysfunction and often reduces the scavenging activity for Aβ,
thereby resulting in Aβ deposition in local neurons. This results
in neuron deficiency and cutin hyperplasia, and induces neuronal
apoptosis in a dose-dependent manner (7,17–20).
This is in accordance with our study outcomes. We have discovered
that the peripheral blood Aβ level has an apparent negative
correlation with rSO2. However the internal relations of
this correlation need to be validated via animal experiment and
cell experiment. According to the above results, we believe that
reasonable control of time of subtotal gastrectomy and ventilatory
capacity during the operation is clinically significant for
reducing the incidence of postoperative POCD (21,22).
In conclusion, the expression level of Aβ in serum
of the patients with POCD was significantly increased, and the
combined Aβ and rSO2 may be indicators for diagnosis and
prevention of POCD after subtotal gastrectomy under general
anesthesia.
References
|
1
|
Vatter H, Konczalla J and Seifert V:
Endothelin related pathophysiology in cerebral vasospasm: what
happens to the cerebral vessels? Acta Neurochir Suppl. 110:177–l80.
2011.PubMed/NCBI
|
|
2
|
Peng L, Xu L and Ouyang W: Role of
peripheral inflammatory markers in postoperative cognitive
dysfunction (POCD): a meta-analysis. PLoS One. 8:e796242013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hu Y, Shi S, Liu X, Hu Z, Huang W, Wang D,
Xu J, Cheng B, Fang X and Shu Q: Effects of heart bypass surgery on
plasma Aβ40 and Aβ42 levels in infants and young children. Medicine
(Baltimore). 95:e26842016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Saito S and Ishii H: Early detection of
iliac artery rupture by sudden steep reduction of regional
saturation of oxygen at the ipsilateral foot during transcatheter
aortic valve implantation - a case report. Masui. 65:184–188.
2016.(In Chinese). PubMed/NCBI
|
|
5
|
Venerito M, Vasapolli R and Malfertheiner
P: Prevention, early diagnosis and therapy of gastric cancer. MMW
Fortschr Med. 158:39–43. 2016.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tuna AT, Akkoyun I, Darcin S and Palabiyik
O: Effects of carbon dioxide insufflation on regional cerebral
oxygenation during laparoscopic surgery in children: a prospective
study. Rev Bras Anestesiol. 66:249–253. 2016.(In Portuguese).
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li XM, Li F, Liu ZK and Shao MT:
Investigation of one-lung ventilation postoperative cognitive
dysfunction and regional cerebral oxygen saturation relations. J
Zhejiang Univ Sci B. 16:1042–1048. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ong HL, Subramaniam M, Abdin E, Wang P,
Vaingankar JA, Lee SP, Shafie S, Seow E and Chong SA: Performance
of Mini-Mental State Examination (MMSE) in long-stay patients with
schizophrenia or schizoaffective disorders in a psychiatric
institute. Psychiatry Res. 241:256–262. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Marceau EM, Lunn J, Berry J, Kelly PJ and
Solowij N: The Montreal Cognitive Assessment (MoCA) is sensitive to
head injury and cognitive impairment in a residential alcohol and
other drug therapeutic community. J Subst Abuse Treat. 66:30–36.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nesaratnam A, Nesaratnam N and Agius M:
Cognitive impairment following use of anaesthetic agents: a review
of the literature, and implications for future practice. Psychiatr
Danub. 26:(Suppl 1). 53–55. 2014.PubMed/NCBI
|
|
11
|
Xu Z, Dong Y, Wang H, Culley DJ,
Marcantonio ER, Crosby G, Tanzi RE, Zhang Y and Xie Z:
Age-dependent postoperative cognitive impairment and
Alzheimer-related neuropathology in mice. Sci Rep.
4:37662014.PubMed/NCBI
|
|
12
|
Vlisides P and Xie Z: Neurotoxicity of
general anesthetics: an update. Curr Pharm Des. 18:6232–6240. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Erdem AF, Kayabasoglu G, Tas Tuna A,,
Palabiyik O, Tomak Y and Beyaz SG: Effect of controlled hypotension
on regional cerebral oxygen saturation during rhinoplasty: a
prospective study. J Clin Monit Comput. 30:655–660. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ide K and Secher NH: Cerebral blood flow
and metabolism during exercise. Prog Neurobiol. 61:397–414. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Picton P, Dering A, Alexander A, Neff M,
Miller BS, Shanks A, Housey M and Mashour GA: Influence of
ventilation strategies and anesthetic techniques on regional
cerebral oximetry in the beach chair position: a prospective
interventional study with a randomized comparison of two
anesthetics. Anesthesiology. 123:765–774. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Barten DM, Guss VL, Corsa JA, Loo A,
Hansel SB, Zheng M, Munoz B, Srinivasan K, Wang B, Robertson BJ, et
al: Dynamics of β-amyloid reductions in brain, cerebrospinal fluid,
and plasma of β-amyloid precursor protein transgenic mice treated
with a γ-secretase inhibitor. J Pharmacol Exp Ther. 312:635–643.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hametner C, Stanarcevic P, Stampfl S,
Rohde S, Veltkamp R and Bösel J: Noninvasive cerebral oximetry
during endovascular therapy for acute ischemic stroke: an
observational study. J Cereb Blood Flow Metab. 35:1722–1728. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mousa WF, Mowafi HA, Al-Metwalli RR,
Al-Ghamdi AA and Al-Gameel HZ: Preoperative mannitol infusion
improves perioperative cerebral oxygen saturation and enhances
postoperative recovery after laparoscopic cholecystectomy. Saudi
Med J. 36:1199–1204. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xie Z and Tanzi RE: Alzheimer's disease
and post-operative cognitive dysfunction. Exp Gerontol. 41:346–359.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jo YY, Kim JY, Park CK, Chang YJ and Kwak
HJ: The effect of ventilation strategy on arterial and cerebral
oxygenation during laparoscopic bariatric surgery. Obes Surg.
26:339–344. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ding L, Zhang H, Mi W, Sun L, Zhang X, Ma
X and Li H: Effects of carbon dioxide pneumoperitoneum and steep
Trendelenburg positioning on cerebral blood backflow during robotic
radical prostatectomy. Nan Fang Yi Ke Da Xue Xue Bao. 35:712–715.
2015.(In Chinese). PubMed/NCBI
|
|
22
|
Lin R, Zhang F, Xue Q and Yu B: Accuracy
of regional cerebral oxygen saturation in predicting postoperative
cognitive dysfunction after total hip arthroplasty: regional
cerebral oxygen saturation predicts POCD. J Arthroplasty.
28:494–497. 2013. View Article : Google Scholar : PubMed/NCBI
|