Introduction
The diagnosis and treatment of bone nonunion has
been extensively studied (1). The
diagnosis and follow-up of nonunion rely predominantly on the
interpretation of X-ray findings, which depend on the clinician's
experience and the degree of bone callus mineralization during the
fracture healing process (2). X-ray
results are also affected by the projection, film processing
conditions and subjective factors, resulting in poor accuracy
(3). Furthermore, the X-ray
resolution may be compromised when the bone mineral content is
<25% (4). Development of a novel
and feasible method of monitoring bone healing is therefore
urgently needed. B-mode ultrasound, response to vibration,
mechanical impedance analysis and the creation of artificial neural
networks have been extensively studied with respect to the
function, mechanical status and changes of bone (3,4).
However, the feasibility of measuring serum biomarker
concentrations for the monitoring of fracture healing remains
unclear.
The present study investigated the diagnosis of
fracture healing at the molecular level with the aim of developing
a method for early diagnosis and outcome prediction of fracture
nonunion, and of providing an objective method of assessing the
efficacy of bone-growth drugs. As changes in bone metabolism
precede changes in morphology, changes in biomarker levels can be
detected earlier than changes in bone density and bone mass
(2). However, the balance between
bone formation and bone resorption in fracture nonunion remains
unclear (5). The coupling of bone
resorption and formation is closely associated with collagen
metabolism, growth factors, vascular mediators and osteoblast
activity (6). This study measured
the serum concentrations of markers of bone turnover during the
bone healing process. The serum biomarker concentrations were
compared with the morphological changes on X-rays to determine
whether they reflected bone nonunion, and to establish a database
of serum biomarker concentrations. A rabbit model of bone nonunion
was monitored by regular X-ray examinations. Serum biomarker
concentrations were measured to investigate their usefulness for
the early diagnosis of bone nonunion, and their changes in
concentration during early bone nonunion.
Materials and methods
Reagents and apparatus
An ELISA kit for the determination of osteocalcin
(OC; EIA-3375) was purchased from USCN Life Science, Inc. (Wuhan,
China), whereas bone-specific alkaline phosphatase (BSAP;
GCNML003), C-terminal telopeptide of type I collagen
(CTX;XYI20748), N-terminal telopeptide of type I collagen
(NTX;XYE10384) and tartrate-resistant acid phosphatase 5b (TRACP
5b; YZBIDSDO/2005) ELISA kits were purchased from Shanghai Langdun
Shengwu (Shanghai, China). The present study used the following
materials: Surgical instruments: Scalpel handle, scalpel blades,
mosquito forceps, bone scalpel, rongeur, tissue scissors, suture
scissors, sterile surgical towels, no. 1 silk sutures, operating
table, bone wax and tape to secure the rabbits on the operating
table; testing instruments: Vernier caliper (Ningbo Dahong
Instrument, Ningbo, China) and X-ray machine (Shimadzu Corp.,
Kyoto, Japan); drugs: amoxicillin, 3% pentobarbital sodium,
ketamine, iodine (all Sanye Pharmaceutical Co., Ltd., Haikou,
China) and lime (Tunchang Yinxin Lime Factory, Tunchang, China);
and animal housing and feeding equipment: Rabbit cages and rabbit
feed.
Animals and treatment
A total of 20 purebred New Zealand rabbits (10 male
and 10 female; age, 5–6 months; weight, 2.5–3.0 kg) were purchased
from the Medical Experimental Center of Hainan Provincial People's
Hospital (Haikou, China) and maintained in separate cages for 12
weeks with natural light at 18–20°C. Rabbits were fed on a diet of
grass, hay, fresh vegetables, carrots, a limited amount of pellets
three times a day and 300 ml clean drinking water. Rabbits were
randomly divided into two groups of 10 rabbits each: A bone defect
group and a bone fracture group. In the bone defect group, a 15-mm
section of bone (including the periosteum) was removed from the
mid-radius, and the medullary cavities of the bone stumps were
closed with bone wax. In the bone fracture group, the mid-radius
was fractured, and no bone wax was used. No fracture fixation was
performed in either group. Following the surgical procedure, the
rabbits were housed in separate cages and allowed free activity.
All animals received care in compliance with the ‘Principles of
laboratory animal care’ (7).
Surgical methods
Rabbits were anesthetized with an intravenous
injection of 3% pentobarbital sodium (20 mg/kg) via an ear vein and
an intramuscular injection of 50 mg/kg ketamine. Once anesthetized,
the rabbit was positioned on the operating table and secured with
rope. The right forelimb was shaved and disinfected with iodine. A
2.5–3.0-cm skin incision was made over the mid-radius and the
radius was exposed. In the bone defect group, a 15-mm length of
bone was removed from the mid-radius. The Vernier caliper was used
to ensure that the length of bone removed was accurate to within
0.1 mm. The bone stumps were trimmed using rongeurs, and the defect
was closed with bone wax. In the bone fracture group, the
mid-radius was fractured. No fracture fixation was performed in
either group. The skin wounds were closed using no. 1 silk sutures
and were disinfected with iodine twice daily following the surgical
procedure. The sutures were removed after 12 days. All rabbits were
fed oral amoxicillin (0.2–0.3 g/kg) twice daily for 1 week
following the surgical procedure.
X-ray and biomarker examinations
X-rays were taken of the right forelimb of each
rabbit preoperatively and at 2, 3, 4, 5, 6, 7, 8, 10 and 12 weeks
postoperatively to evaluate bone healing. A 2-ml blood sample was
also taken at each time point and was stored at −80°C for
measurement of serum biomarker concentrations.
ELISA determination of biomarker
concentrations
The serum biomarker concentrations measured were
those of OC and BSAP, which served as markers of bone formation,
and those of CTX, NTX and TRACP 5b, which served as markers of bone
resorption.
All biomarker concentrations were measured by biotin
double-antibody sandwich ELISA, according to the manufacturers'
protocols. For each concentration determination, the ELISA plate
was embedded with the respective monoclonal antibody and the
biomarker was subsequently added. After the monoclonal antibody had
been incubated with the biomarker, a biotin-labeled antibody
against the biomarker was added to the mixture, thus binding to
streptavidin-horseradish peroxidase and forming immune complexes.
The complexes were subsequently incubated and rinsed with the wash
solution provided in the kit to eliminate unbound enzyme, developed
in a blue stain with chromogen A and B, and finally developed in a
yellow stain with the acid. The degree of staining was positively
correlated with the concentration of the biomarker in the
specimen.
Statistical analysis of serum
biomarker concentrations
All data are expressed as means ± standard deviation
and were analyzed using SPSS 20.0 software (SPSS, Inc., Chicago,
IL, USA). One-way analysis of variance was used to estimate average
values, followed by effect comparisons between groups, a spherical
test, intragroup (repeated) effect comparisons, and interaction
effect comparisons. P<0.05 was considered to indicate a
statistically significant difference. Sample sizes were determined
based on a preselected power level of 0.8.
Results
Observation of the rabbits following
the surgical procedure
None of the rabbits developed infection of the
surgical incision, and none died during the experimental period.
All the rabbits were included in all the analyses.
X-ray findings
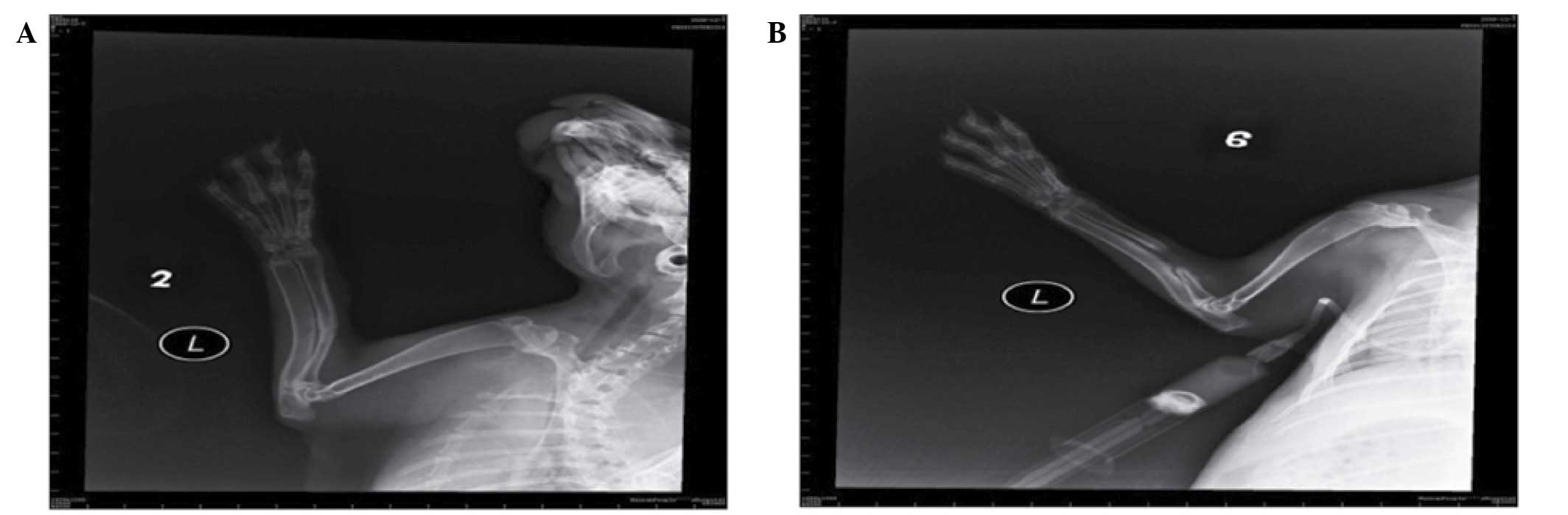
In the bone defect group, bone callus formation was
observed in three rabbits at 2 weeks and the bone calluses
stabilized at 5 weeks, but none of the bones had healed at 8 weeks
(Fig. 1A). In the bone fracture
group, the fracture line was distorted at 2 weeks and a large
number of bone calluses formed at 6–8 weeks (Fig. 1B).
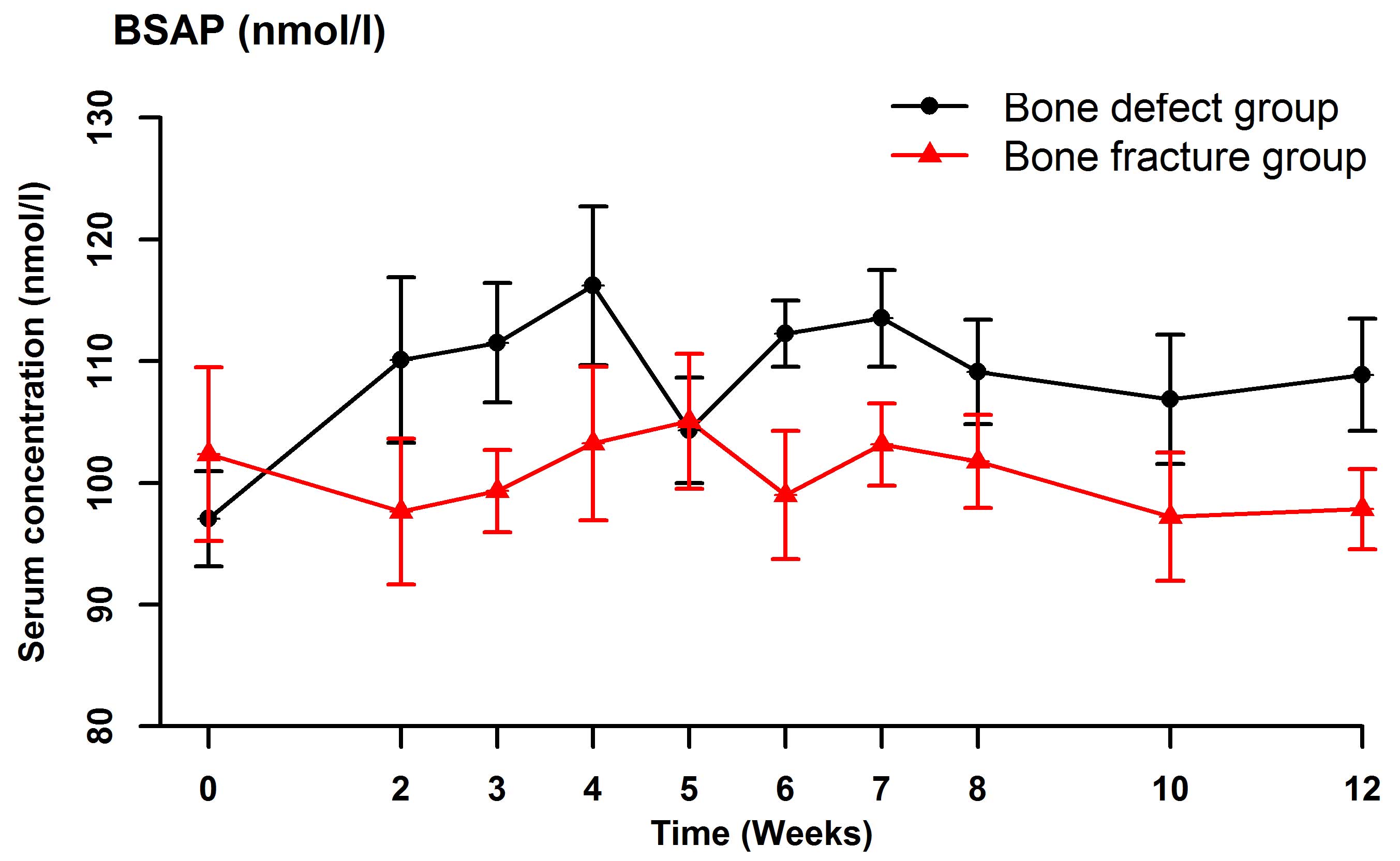
Serum biomarker concentrations
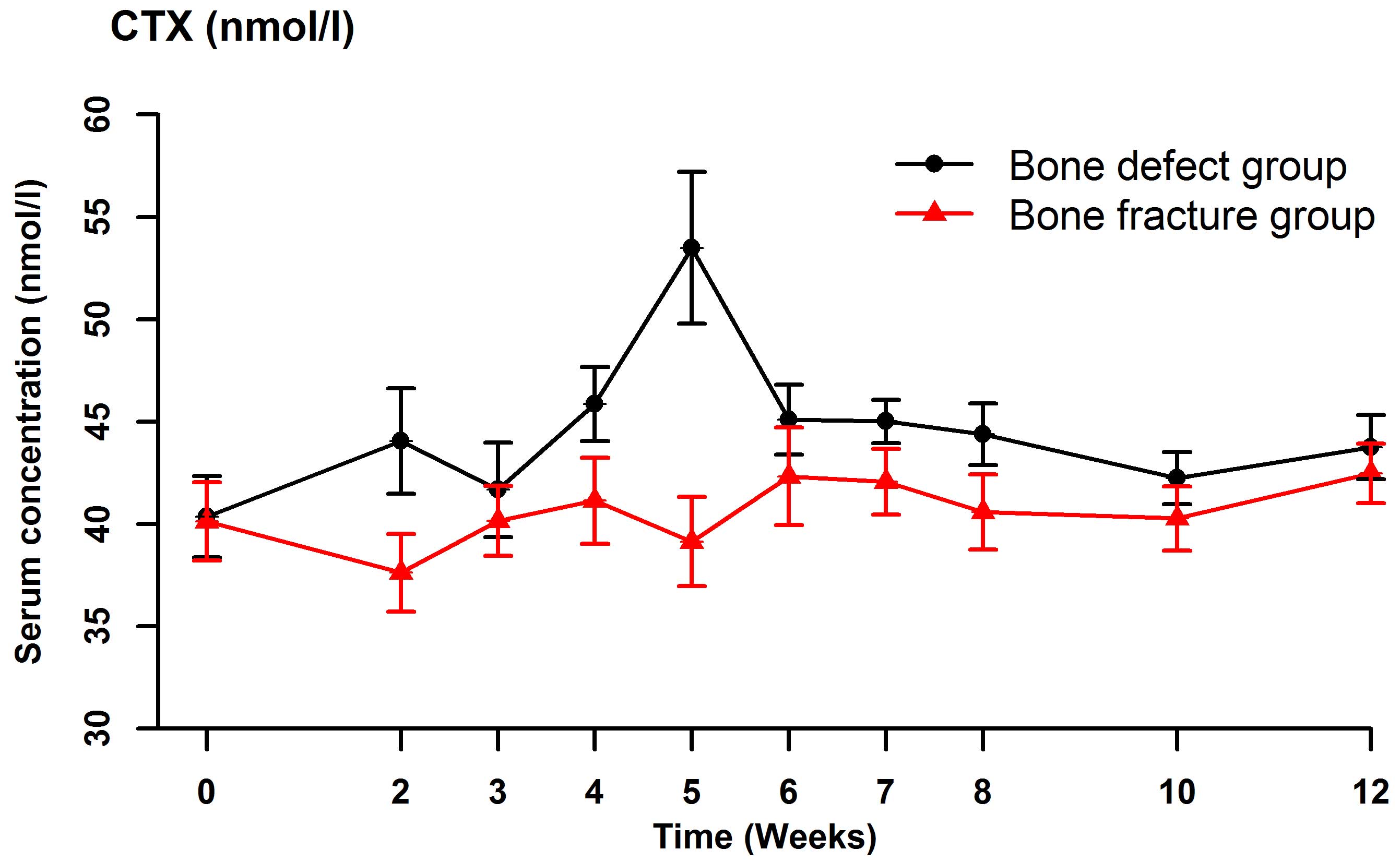
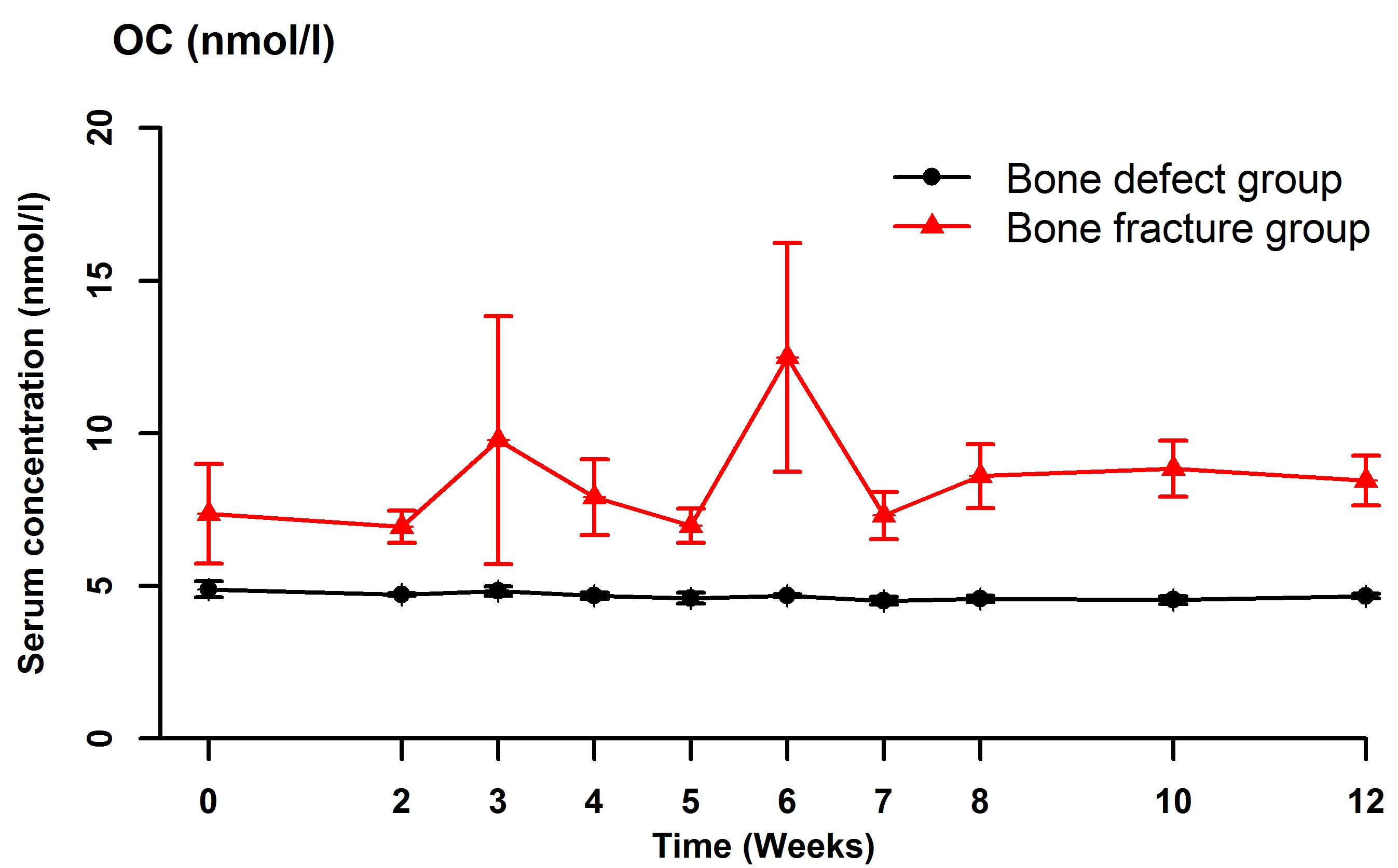
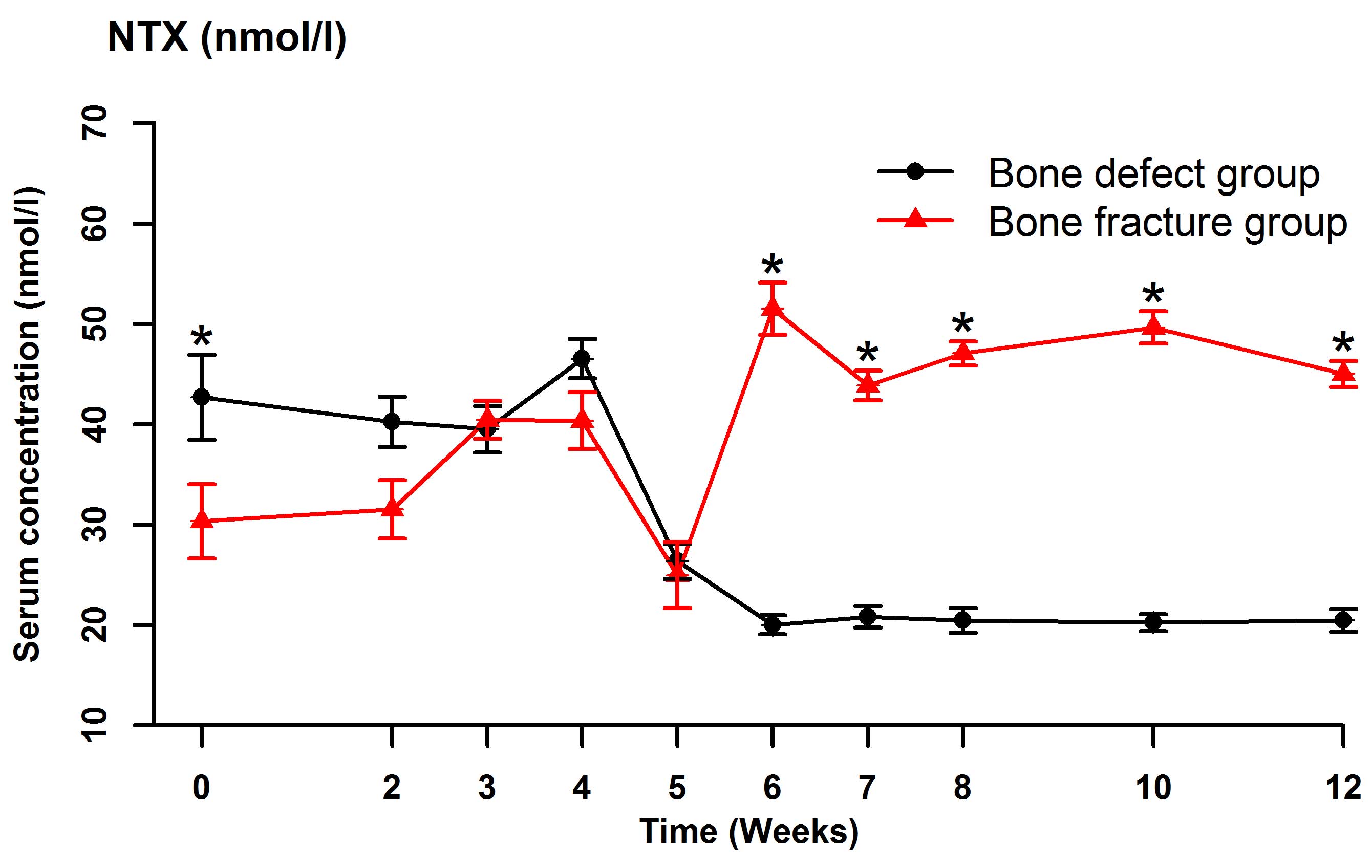
Serum BSAP (Fig. 2),
CTX (Fig. 3), OC (Fig. 4) and NTX (Fig. 5) concentrations were significantly
different between the two groups (OC: F=22.989, P<0.001; BSAP:
F=16.051, P=0.001; CTX: F=27.737, P<0.001; NTX: F=187.512,
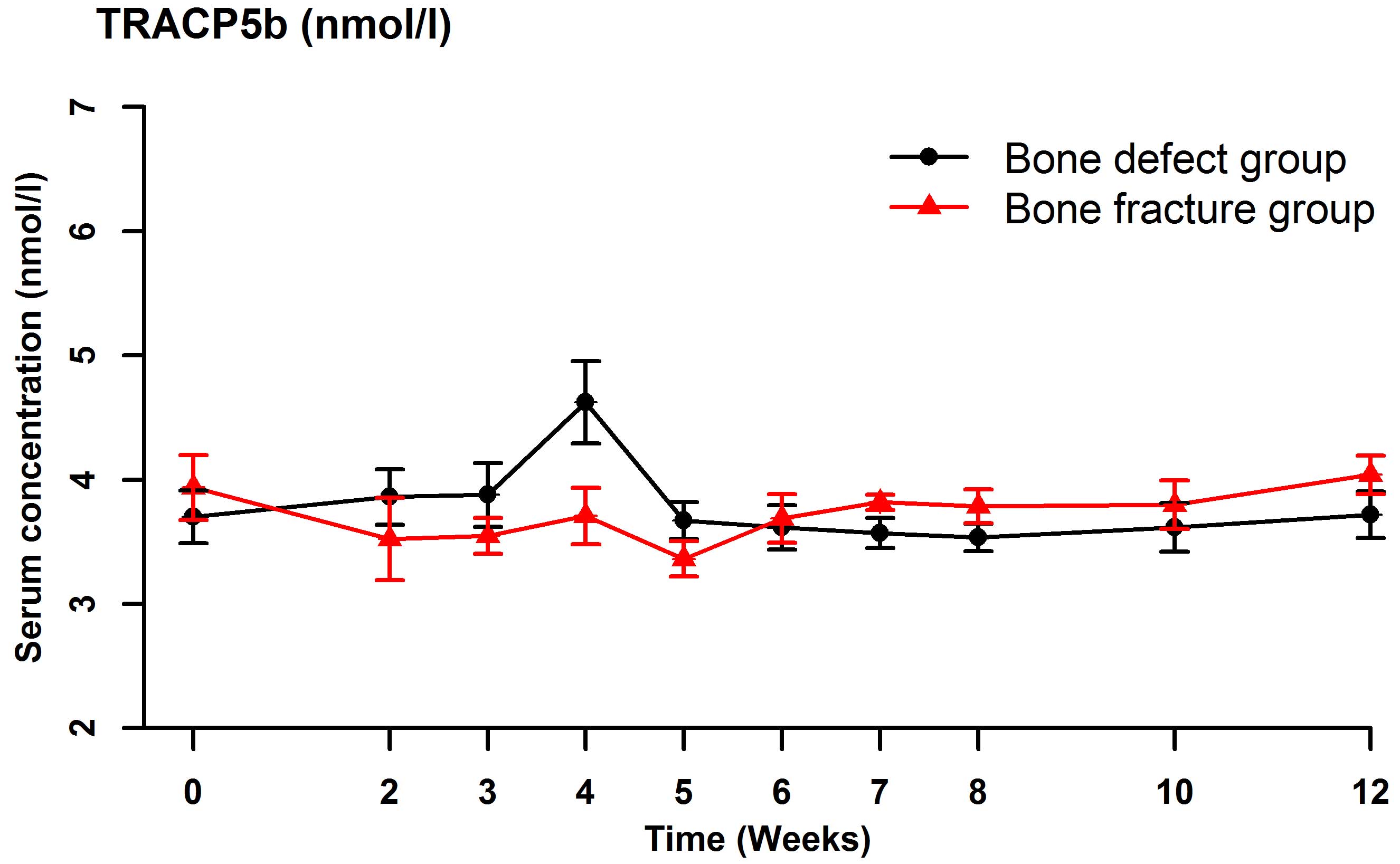
P<0.001). There were no significant differences in the serum OC,
BSAP, CTX or TRACP 5b (Fig. 6)
concentrations within each group at the various time points. In the
bone defect group, serum BSAP concentration increased
postoperatively and peaked at 4 weeks, began to decrease at 5 weeks
and stabilized after 6 weeks (Fig.
2). Serum CTX concentrations fluctuated during the first 4
weeks, peaked at 5 weeks, then decreased and stabilized after 6
weeks (Fig. 3). Serum OC
concentrations did not significantly alter following the surgical
procedure (Fig. 4). In the bone
defect group, the serum NTX concentrations were significantly lower
at 5 weeks compared with the other time points prior to and
following the surgical procedure (Fig.
5). There were significant differences between the serum NTX
concentrations at 7, 8, 10, and 12 weeks and at 3, 4 and 5 weeks.
The serum NTX concentrations stabilized following 6 weeks. Serum
TRACP 5b concentration increased following the surgical procedure
and peaked at 4 weeks, then decreased and remained low (Fig. 6).
Discussion
In recent years, bone defects caused by nonunion,
delayed healing, and other factors have attracted increasing
attention, and have been studied in animal experiments (8). Animals have anatomical and
physiological characteristics similar to those of humans, and
animal experiments can be used to model human conditions such as
bone nonunion with good reproducibility. Experimental studies of
bone nonunion have focused on large animals such as pigs, horses,
cows, sheep and monkeys (9,10). However, use of these large animals
has some disadvantages, such as high cost, demanding feeding
conditions, and difficult experimental designs (11). Although small animals are not
suitable for models of fracture fixation, they recover rapidly from
trauma and are suitable for cytological studies of fracture healing
(6). A previous study reported that
rabbits are ideal for cytological studies of fracture healing due
to the similarities between rabbit and human limbs, the small body
size, ease of handling, rapid tissue repair, short breeding cycle,
simple breeding management, low cost, and availability of large
sample sizes (12). New Zealand
white rabbits were therefore chosen for the present study.
Establishment of useful animal models of bone
defects is necessary for tissue engineering research of bone
nonunion. The length of the bone defect should be sufficient to
prevent union of the bone. Bone healing depends predominantly on
the size of the defect, but is also influenced by the age, body
mass and sex of the animal (13).
The forelegs of New Zealand white rabbits have a radius and an
ulna. When a defect is created in the mid-radius, the ulna
continues to support the forelimb (9). As internal fixation is not needed, this
is a commonly used model. Johnson et al (14) demonstrated that certain bone defects
are not conducive to bone growth and repair, such as a defect
length of >3–4 times the diameter of the bone shaft in an adult
animal, a defect covered by local muscle tissue, or a defect in a
bone with low red bone marrow content. The optimal length of an
experimental defect in the radius is controversial. According to
the Stephen standard, the defect should have a length of 1.5–2.0
times the diameter of the bone (13,15). As
the diameter of the radius in New Zealand rabbits is 4.0–5.0 mm,
many investigators use 15-mm long mid-radius bone defects. Kasten
et al (16), Niemeyer et
al (17) and other researchers
(18–21) have demonstrated that the area of the
bone defect was filled with fibrous scar tissue without a bony
connection, the bone wax was not absorbed, the bone stumps were
hardened, the medullary cavity was blocked, and a small bone callus
had formed 10 weeks following the creation of a 15-mm long defect
in the radius of a rabbit.
In the present study, the results of the X-ray
examinations indicated that the 15-mm bone defects were connected
by fibrous tissue and that the medullary cavity at the bone stumps
was blocked at 12 weeks postoperatively. The fracture healing time
in rabbits is usually ~6 weeks, and absence of healing after 12
weeks indicates nonunion. The 15-mm bone defects in the rabbits of
the present study had not healed after 12 weeks, indicating
successful establishment of a bone nonunion model.
The existing methods used to study nonunion include
measurements of bone morphometry, bone mineral density, and the
bone metabolic index (22). The bone
metabolic index is of particular interest because it can be
measured non-invasively and repeatedly (23). Bone formation, bone resorption, and
static conditions contribute to the process of bone reconstruction
(24). Bone turnover involves the
continuous removal of old bone by osteoclasts and simultaneous
formation of osteoid and mineralization by osteoblasts. These two
processes are tightly coupled. The bone resorption-remodeling
process is regulated by osteoblasts (25). The bone mass is determined by the
balance of bone formation and bone resorption in the same bone
reconstruction unit (17). When this
balance is disrupted and the rate of bone resorption is higher than
the rate of bone formation, nonunion occurs (26). Serum biomarker concentrations can
reflect the status of the bone turnover process by indirectly
measuring osteoblast and osteoclast activity (27).
A number of sensitive and specific biomarkers have
been studied for the monitoring of bone loss, prediction of
fracture risk, evaluation of drug treatment responses, and
differential diagnosis of metabolic bone diseases (28). The main biomarkers are BSAP, CTX,
NTX, and TRACP 5b (23,25). Measurement of the serum
concentrations of these biomarkers enables the earlier assessment
of treatment effects than measurement of bone density.
BSAP is an extracellular enzyme produced by
osteoblasts that is not affected by diseases of the liver, kidney,
or intestines (29). The serum BSAP
concentration is a specific and sensitive indicator of osteoblast
activity and bone formation, and a high concentration indicates a
high level of osteoblast activity (27). Previous studies have reported that
the serum BSAP concentration reflects bone turnover (27,28).
Southwood et al (30) studied
a rabbit model of femur defects, and found that the serum BSAP
concentration was low during the first 4 weeks after the surgical
procedure, increased to a peak at 8 weeks, and then decreased.
Moghaddam et al (31)
compared 15 patients with atrophic nonunion following a long bone
shaft fracture with 15 matched patients with normal fracture
healing selected from a pool of 248 patients who underwent
orthopedic surgery. They measured serum biomarker concentrations at
1, 2, 4, 8, 12 and 52 weeks after surgery, and demonstrated that
the serum BSAP and procollagen type I N-terminal propeptide
concentrations initially increased and then decreased during the
first week following the surgical procedure. There were no
significant differences in the absolute or relative concentrations
of these biomarkers between the two groups during the healing
process. In the bone defect group in the present study, the serum
BSAP concentration increased postoperatively and peaked at 4 weeks,
then began to decrease at 5 weeks and stabilized after 6 weeks. The
serum BSAP concentrations were significantly different between the
two groups, but were not significantly different between the
various time points within each group. These results indicated that
the bone defect stimulated bone formation resulting in an increase
in serum BSAP concentrations, which was similar to the results
obtained by Southwood et al (30) and Moghaddam et al (31). Changes in the serum BSAP
concentration can be used to monitor bone healing in experimental
rabbits.
In both animals and humans, OC is produced and
secreted by non-proliferating osteoblasts (32). OC is the main component of
non-collagenous proteins in the bone tissue, and contains 49 amino
acids and 3 carboxyglutamic acid residues (33). The biological activity of OC depends
on vitamins K and D. Mature OC is predominantly located in bone
tissue outside the mesenchymal cells and dentin, and a small amount
is released into the blood (33). In
1988, Eastell et al (34)
proposed that the serum OC concentration is a sensitive and
specific biomarker of bone turnover and bone formation. OC is
currently a major focus of studies of bone metabolism. In
vitro and in vivo experiments have demonstrated that OC
is associated with the regulation of bone resorption as well as in
osteoblast differentiation and matrix mineralization (33–35).
Delmas et al (36)
demonstrated that serum OC concentrations reflect bone turnover
when bone formation is coupled with bone resorption, but reflects
only bone formation when bone formation is not coupled with bone
resorption. Previous Chinese studies have reported that a high
serum OC concentration was associated with high bone mineral
density, suggesting that bone formation and bone mass will increase
when the serum OC concentration is high (31,32). The
serum OC concentration therefore reflects bone mineral density and
can be used to predict bone nonunion. In the present study, the
serum OC concentration did not change following the surgical
procedure in the bone defect group, in spite of changes in the bone
mineral density. This indicates that the serum OC concentration is
not a sensitive indicator of bone nonunion in rabbits.
TRACP is one of six acid phosphatase isozymes and is
predominantly secreted by osteoclasts (37). The serum TRACP concentration may
reflect osteoclast activity and bone resorption in vivo
(38). Under normal conditions, two
types of TRACP 5 are present in human serum: 5a and 5b (39). Sialidase converts TRACP 5a to TRACP
5b, which is the purified human osteoclast TRACP. The serum TRACP
5b concentration is regarded as the optimal biomarker of bone
resorption due to its high specificity, lack of diurnal variation,
and independence of diet and liver or kidney diseases. Measurement
of the serum TRACP 5b concentration can also be used for the early
detection of osteoporosis, thereby reducing the risk of fractures
(40).
CTX contains important intermolecular cross-linking
agents of type I collagen and residues of cross-linking agents, and
is not degraded by the kidney (39).
The serum CTX concentration is therefore an ideal marker of bone
resorption. CTX has three different forms: CTX-matrix
metalloproteinase, α-CTX, and β-CTX, which are collectively termed
CrossLaps. α-CTX and β-CTX both have only eight amino acid
sequences (40,41).
Moghaddam et al (31) measured serum biomarker concentrations
in 15 patients with atrophic nonunion with 15 matched patients with
normal fracture healing selected from a pool of 248 patients who
underwent orthopedic surgery, as described above. At 1 week after
surgery, the serum CTX concentration was significantly lower in the
nonunion group compared with the normal healing group. At 4 and 8
weeks, the serum TRACP 5b concentration was significantly lower in
the nonunion group. The absolute and relative serum TRACP 5b
concentrations were not significantly different between the two
groups at any of the time points. In the bone defect group in the
present study, the serum TRACP 5b concentration increased following
the surgical procedure and peaked at 4 weeks, then decreased and
remained low. The serum CTX concentrations changed in a similar
pattern in the bone defect and bone fracture groups, but with
significant differences between the two groups. The serum CTX
concentrations peaked at 5 weeks following the surgical procedure
in the bone defect group, but there were no significant differences
in CTX concentration between the various time points within each
group. The serum TRACP 5b and CTX concentrations increased
following surgery in the bone defect group, indicating increased
bone resorption. The serum TRACP 5b and CTX concentrations may
reflect the early healing process, and may be useful for clinical
monitoring.
NTX is a low-molecular-weight peptide that contains
hydroxylysyl pyridinoline and lysyl pyridinoline, one of which is
connected to each end of the peptide chain (42). NTX is a type I collagen cross-linked
telopeptide and the total N-terminal cross-linking agent (41–43).
Lysyl pyridinoline is predominantly located within the bone and
accounts for 21% of mature collagen, and hydroxylysyl pyridinoline
is located in both cartilage and bone and is a major component of
mature collagen (36). Lysyl
pyridinoline and hydroxylysyl pyridinoline are released from the
bone matrix in the process of osteoclastic bone resorption,
circulate as free amino acids or bound to peptides such as NTX, and
are excreted in the urine (38,44). NTX
is a stable peptide excreted in the urine following bone
resorption; therefore a high serum NTX concentration is likely
highly specific for bone resorption (31). At the beginning of 1990s, Hanson
et al (45) established an
ELISA method to determine NTX concentration, following which the
investigators determined that there were immunologically competent
NTX in the culture medium when osteoclasts were cultured in
vitro. García-Pérez et al (26) reported that the serum NTX
concentration was a sensitive indicator of bone resorption. Rosen
et al (46) demonstrated that
the serum NTX concentration was negatively correlated with the bone
mineral density, and that a higher baseline serum NTX concentration
indicated a more rapid decline in bone density. In the bone defect
group in the present study, the serum NTX concentration was
significantly lower at 5 weeks following the surgical procedure
than prior to surgery and stabilized after 6 weeks. The serum NTX
concentrations were significantly different between the bone defect
and bone fracture groups.
In the present study, the serum OC concentration did
not change significantly following the surgical procedure in the
bone defect group, whereas the serum BSAP, CTX, and TRACP 5b
concentrations fluctuated postoperatively. Although the serum OC,
BSAP, CTX, and TRACP 5b concentrations did not change significantly
following surgery in the bone defect group, this group had a high
bone turnover rate. Measurement of serum biomarker concentrations
may help with clinical evaluation of the early healing process. In
the bone defect group, the serum NTX concentration was
significantly lower at 5 weeks following the surgical procedure
than before surgery, suggesting that the serum NTX concentration
provides an accurate reflection of bone turnover in vivo and
changes quickly following changes in bone resorption. Further
studies are required in order to definitively determine whether the
serum NTX concentration is a sensitive and specific indicator of
bone resorption, and whether the serum NTX concentration accurately
reflects early bone turnover and can predict bone nonunion.
Acknowledgements
The present study was supported by a grant from the
Natural Science Foundation of Hainan Province, China (grant no.
808212).
Glossary
Abbreviations
Abbreviations:
|
BSAP
|
bone-specific alkaline phosphatase
|
|
CTX
|
C-terminal telopeptide of type I
collagen
|
|
ELISA
|
enzyme-linked immunosorbent assay
|
|
NTX
|
N-terminal telopeptide of type I
collagen
|
|
OC
|
osteocalcin
|
|
TRACP 5b
|
tartrate-resistant acid phosphatase
5b
|
References
|
1
|
Court-Brown CM and McQueen MM: Nonunions
of the proximal humerus: their prevalence and functional outcome. J
Trauma. 64:1517–1521. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Blokhuis TJ, de Bruine JH, Bramer JA, den
Boer FC, Bakker FC, Patka P, Haarman HJ and Manoliu RA: The
reliability of plain radiography in experimental fracture healing.
Skeletal Radio. 30:151–156. 2001. View Article : Google Scholar
|
|
3
|
Lotz J, Gaertner T, Hahn M and Prellwitz
W: Collagen type I metabolism after bone surgery. Arch Orthop
Trauma Surg. 119:212–216. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sambrook P and Cooper C: Osteoporosis.
Lancet. 367:2010–2018. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lin JP, Song SF and Yao LL: Research
progress of fracture healing and it's early diagnosis. Ortho J
China. 24:1876–1878. 2009.
|
|
6
|
Gamero P and Somay-Rendu E: Biochemical
markers of bone loss rate and prevalence of osteoporosis at
multiple skeletal sites in Chinese women. Osteoporos Int.
13:669–676. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Laboratory animal welfare, . Public Health
Service policy on humane care and use of laboratory animals by
awardee institutions; notice. Fed Regist. 50:19584–19585.
1985.PubMed/NCBI
|
|
8
|
Kokubu T, Hak DJ, Hazelwood SJ and Reddi
AH: Development of an atrophic nonunion model and comparison to a
closed healing fracture in rat femur. J Orthop Res. 21:503–510.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Reed AA, Joyner CJ, Brownlow HC and
Simpson AH: Human atrophic fracture nonunion are not avascular. J
Orthop Res. 20:593–599. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mumaghan M, Li G and Mash DR: Nonsteroidal
anti-inflammatory drug induced fracture nonunion: An inhibition of
angiognensis? JBJS Am. 88:141–147. 2006.
|
|
11
|
Nunamaker DM: Experimental models of
fracture repair. Clin Orthop. (Suppl 355). 561998. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Peter CP and Cook WO: Effect of
alendronate on fracture healing and bone remodeling in dogs. J
Orthop Res. 14:741996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Korkmaz M, Oztürk H, Bulut O, Unsaldi T
and Kaloğlu C: The effect of definitive continuous distraction
employed with the Ilizarov type external fixation system on
fracture healing: An experimental rabbit model. Acta Orthop
Traumatol Turc. 39:247–257. 2005.(In Turkish). PubMed/NCBI
|
|
14
|
Johnson EE, Urist MR, Schmalzried TP,
Chotivichit A, Huang HK and Finerman GA: Autogeneic cancellous bone
grafts in extensive segmental ulnar defects in dogs. Effects of
xenogeneic bovine bone morphogenetic protein without and with
interposition of soft tissues and interruption of blood supply.
Clin Orthop Relat Res. 254–265. 1989.PubMed/NCBI
|
|
15
|
Cook SD, Wolfe MW, Salkeld SL and Rueger
DC: Effect of recombinant human osteogenic protein-1 on healing of
segmental defects in non-human primate. J Bone Joint Surg Am.
77:734–750. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kasten P, Vogel J, Geiger F, Niemeyer P,
Luginbühl R and Szalay K: The effect of platelet-rich plasma on
healing in critical-size long-bone defects. Biomaterials.
29:3983–3992. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Niemeyer P, Szalay K, Luginbühl R, Südkamp
NP and Kasten P: Transplantation of human mesenchymal stem cells in
a non-autogenous setting for bone regeneration in a rabbit
critical-size defect model. Acta Biomater. 6:900–908. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Felix R, Herrmann W and Fleisch H:
Stimulation of precipitation of calcium phosphate by matrix
vesicles. Biochem J. 170:681–691. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Anderson HC, Stechschulte DJ Jr, Collins
DE, Jacobs DH, Morris DC, Hsu HH, Redford PA and Zeiger S: Matrix
vesicle biogenesis in vitro by rachitic and normal rat
chondrocytes. Am J Pathol. 136:391–398. 1990.PubMed/NCBI
|
|
20
|
Parker MJ, Raghavan R and Gurusamy K:
Incidence of fracture-healing complications after femoral neck
fractures. Clin Orthop Relat Res. 458:175–179. 2007.PubMed/NCBI
|
|
21
|
Gothlin G and Ericsson JL: Fine structural
localization of alkaline phosphatase in the fracture callus of the
rat. Histochemie. 36:225–236. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Pedersen BJ, Schlemmer A, Hassager C and
Christiansen C: Changes in the carboxyl-terminal propeptide of type
I procollagen and other markers of bone formation upon five days of
bed rest. Bone. 17:91–95. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lian J, Stewart C, Puchacz E, Mackowiak S,
Shalhoub V, Collart D, Zambetti G and Stein G: Structure of the rat
osteocalcin gene and regulation of vitamin D-dependent expression.
Proc Natl Acad Sci USA. 86:1143–1147. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Noite PA, Krans A Vander, Patka P, Janssen
IM, Ryaby JP and Albers GH: Low-intensity pulsed ultrasound device
for the noninvasive treatment of nonunions. J Trauma. 51:693–702.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Geiger F, Lorenz H, Xu W, Szalay K, Kasten
P, Claes L, Augat P and Richter W: VEGF producing bone marrow
stromal cells (BMSC) enhance vascularization and resorption of a
natural coral bone substitute. Bone. 41:516–522. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
García-Pérez MA, Moreno-Mercer J, Tarín JJ
and Cano A: Similar efficacy of low and standard doses of
transdermal estradiol in controlling bone turnover in
postmenopausal women. Gynecol Endocrinol. 22:179–184. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kyro A, Usenius JP, Aarnio M, Kunnamo I
and Avikainen V: Are smokers a risk group for delayed healing of
tibial shaft fractures? Ann Chir Gynaecol. 82:254–262.
1993.PubMed/NCBI
|
|
28
|
Adams CI, Keating JF and Court-Brown CM:
Cigarette smoking and open tibial fractures. Injury. 32:61–65.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kurdy NM: Serology of abnormal fracture
healing: The role of PINP, PICP, and BsALP. J Orthop Trauma.
14:48–53. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Southwood LL, Frisbie DD, Kawcak CE and
McIlwraith CW: Evaluation of serum biochemical markers of bone
metabolism for early diagnosis of nonunion and infected nonunion
fractures in rabbits. Am J Vet Res. 64:727–735. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Moghaddam A, Müller U, Roth HJ, Wentzensen
A, Grützner PA and Zimmermann G: TRACP 5b and CTX as osteological
markers of delayed fracture healing. Injury. 42:758–764. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kaplan FS, Hayes WC, Keaveny TM, Boskey
AL, Einhorn TA and Iannotti JP: Form and function of
boneOrthopaedic basic science. Simon SS: Amercan Academy of
Orthopaedic Surgeons; Rosemont, IL: pp. 127–184. 1994
|
|
33
|
Linkhart SG, Linkhart TA, Taylor AK,
Wergedal JE, Bettica P and Baylink DJ: Synthetic peptidebased
immunoassay for amino-terminal propeptide of type I procollagen:
application for evaluation of bone formation. Clin Chem.
39:2254–2258. 1993.PubMed/NCBI
|
|
34
|
Eastell R, Yergey AL, Vieira NE, Cedel SL,
Kumar R and Riggs BL: Interrelationship among vitamin D metabolism,
true calcium absorption, parathyroid function, and age in women:
Evidence of an age-related intestinal resistance to
1,25-dihydroxyvitamin D action. J Bone Miner Res. 6:125–132. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sato Y, Kaji M, Higuchi F, Yanagida I,
Oishi K and Oizumi K: Changes in bone and calcium metabolism
following hip fracture in elderly patients. Osteoporos Int.
12:445–449. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Delmas PD: Biochemical markers of bone
turnover for the clinical assessment of metabolic bone disease.
Endocrinol Metab Clin North Am. 19:1–18. 1990.PubMed/NCBI
|
|
37
|
Seibel MJ: Molecular markers of bone
turnover:Biochemical technical and analytical aspects. Osteoporos
Int. 11:18–29. 2000. View Article : Google Scholar
|
|
38
|
Lin JP, Song SF and Yao LL: Feasibility of
predicting fracture risk with bone turnover markers and bone
mineral density. Zhongguo Zuzhi Gongcheng Yanjiu yu Linchuang
Kangfu. 14:317–320. 2010.
|
|
39
|
Szulc P and Delmas PD: Biochemical markers
of bone turnover in men. Calcif Tissue Int. 69:229–234. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Laurer HL, Hagenbourger O, Quast S,
Herrmann W and Marzi I: Sequential changes and pattern of bone
specific alkaline phosphtase after trauma. Eur J Trauma. 1:33–38.
2000. View Article : Google Scholar
|
|
41
|
Dahabreh Z, Calori GM, Kanakaris NK,
Nikolaou VS and Giannoudis PV: A cost analysis of treatment of
tibial fracture nonunion by bone grafting or bone morphogenetic
protein-7. Int Orthop. 33:1407–1414. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Borys J, Grabowska SZ, Antonowicz B, Dryl
D, Citko A and Rogowski F: The concentuation of C-terminal
propeptide of type I procollagen in blood serum in the course of
mandibular fracture healing(preliminary report). Rocz Akad Med
Bialmyst. 46:251–262. 2001.
|
|
43
|
Ingle BM, Hay SM, Bottjer HM and Eastell
R: Changes in bone mass and bone turnover following ankle fracture.
Osteporos Int. 10:408–415. 1999. View Article : Google Scholar
|
|
44
|
Kon T, Cho TJ, Aizawa T, Yamazaki M, Nooh
N, Graves D, Gerstenfeld LC and Einhorn TA: Expression of
osteoprotegerin, receptor activator of NF-kappaB ligand
(osteoprotegerin ligand) and related proinflammatory cytokines
during fracture healing. J Bone Miner Res. 16:1004–1014. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Hanson DA, Weis MA, Bollen AM, Maslan SL,
Singer FR and Eyre DR: A specific immunoassay for monitoring human
bone resorption: Quantitation of type I collagen cross-linked
N-telopeptides in urine. J Bone Miner Res. 7:1251–1258. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Rosen HN, Moses AC, Garber J, Ross DS, Lee
SL and Greenspan SL: Utility of biochemical markers of bone
turnover in the follow-up of patients treatment with
biphosphonates. Calcif Tissue Int. 63:363–368. 1998. View Article : Google Scholar : PubMed/NCBI
|