Introduction
Rheumatoid arthritis (RA) is an autoimmune disease,
which might induce ankylosis, malformation, even loss of normal
joint function (1). Early diagnosis
is usually difficult due to atypical clinical features and the
negative result of rheumatoid factor testing (2). Thus, the best time period for starting
the treatment could be easily missed and as a result, patients
could suffer irreversible joints damage leading to permanent
disabilities (3). Therefore, a quick
and accurate diagnosis of RA has been in the centre of attention
(4,5).
In this study, we investigated the diagnostic value
of high-frequency color Doppler ultrasonography (HCDU) examination
in combination with anti-cyclic citrullinated peptide (anti-CCP)
antibody testing in RA patients with finger joint damage.
Materials and methods
General information
From January to December 2015, 80 patients (with 162
affected joints) who were diagnosed with RA with finger joint
damage were enrolled for this study. There were 44 males and 36
females and the age range was from 21 to 68 years (average,
57.2±3.6 years). The disease courses ranged from 8 to 22 months
(mean disease course, 25.6±2.2 months). All the patients met the
1987 American clinical diagnostic criteria (6). During the same period, 50 healthy
individuals (100 joints) were enrolled in our control group. They
were physically examined in the Yantai Yuhuangding Hospital
(Shandong, China). There were 30 males and 20 females in the
control group, aged 22 to 67 years (average, 56.5±3.3 years).
Aomparison between general information in both groups did not
reveal any significant differences.
Methods
HCDU examination and the serum anti-CCP antibody
testing by ELISA were conducted. HCDU examinations were conducted
as follows: Cross sections and different gestures of the
articulationes digitorum manus were scanned with a transducer
frequency of 12 MHz, using HCDU scanner (Shanghai Chuangxun Medical
Equipments Co., Ltd., Shanghai, China). Serum CCP antibody tests
using ELISA were conducted by strictly following the instructions
provided by the CCP IgG test kit (Beijing Euroimmun Medical
Diagnosis Technology Co., Ltd., Beijing, China).
Statistical analysis
SPSS 21.0 (IBM SPSS, Armonk, NY, USA) was used for
data analysis. We applied t-test or Chi-square test for comparison
between groups. P<0.05 was considered to indicate a
statistically significant difference.
Results
Comparison of the anti-CCP antibody
testings
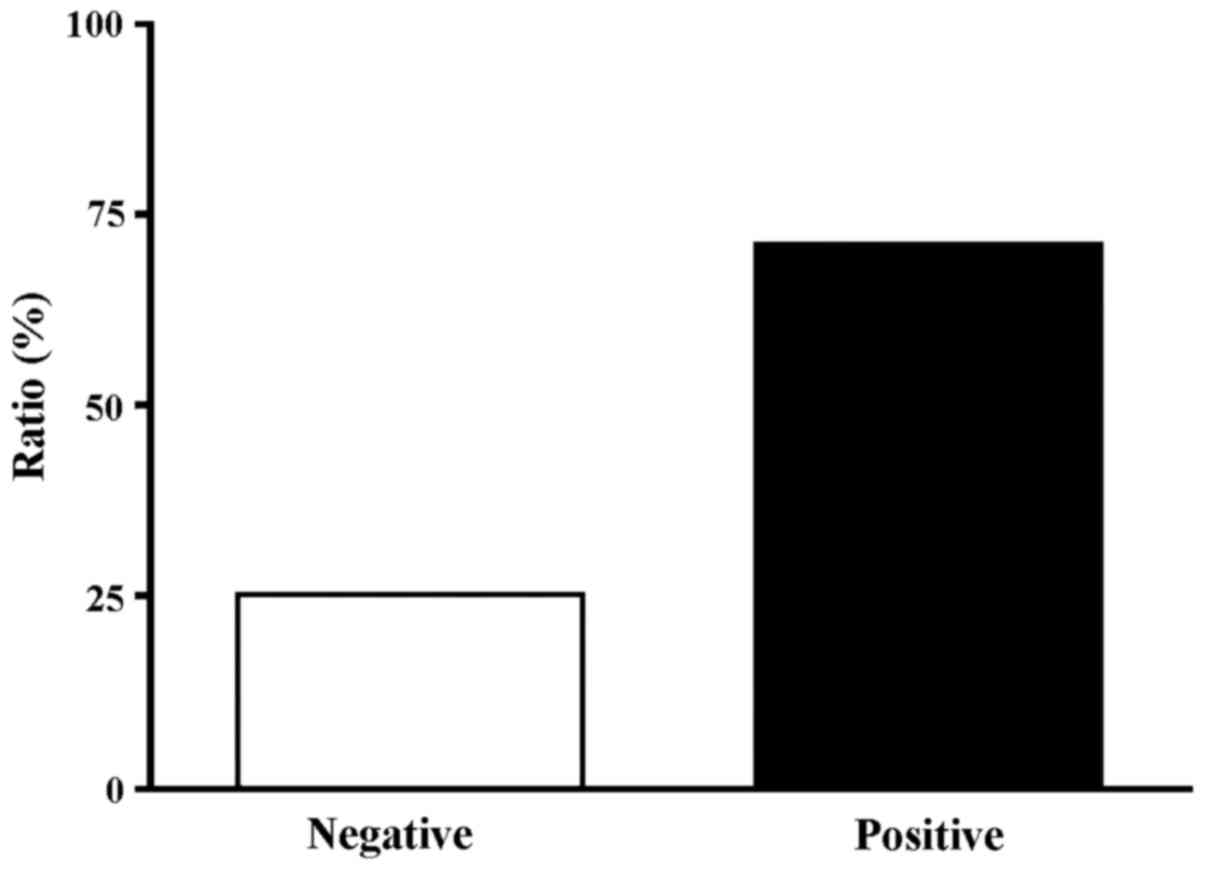
Results obtained from ELISA tests suggested that the
positive rate of anti-CCP antibody in the study group was 73.8%
(59/80 cases), and the negative rate was 26.2% (21/80 cases)
(Fig. 1). The positive rate in the
control group was only 10% (5/50 cases), and the negative rate was
90% (45/50).
Comparison of the HCDU
examination
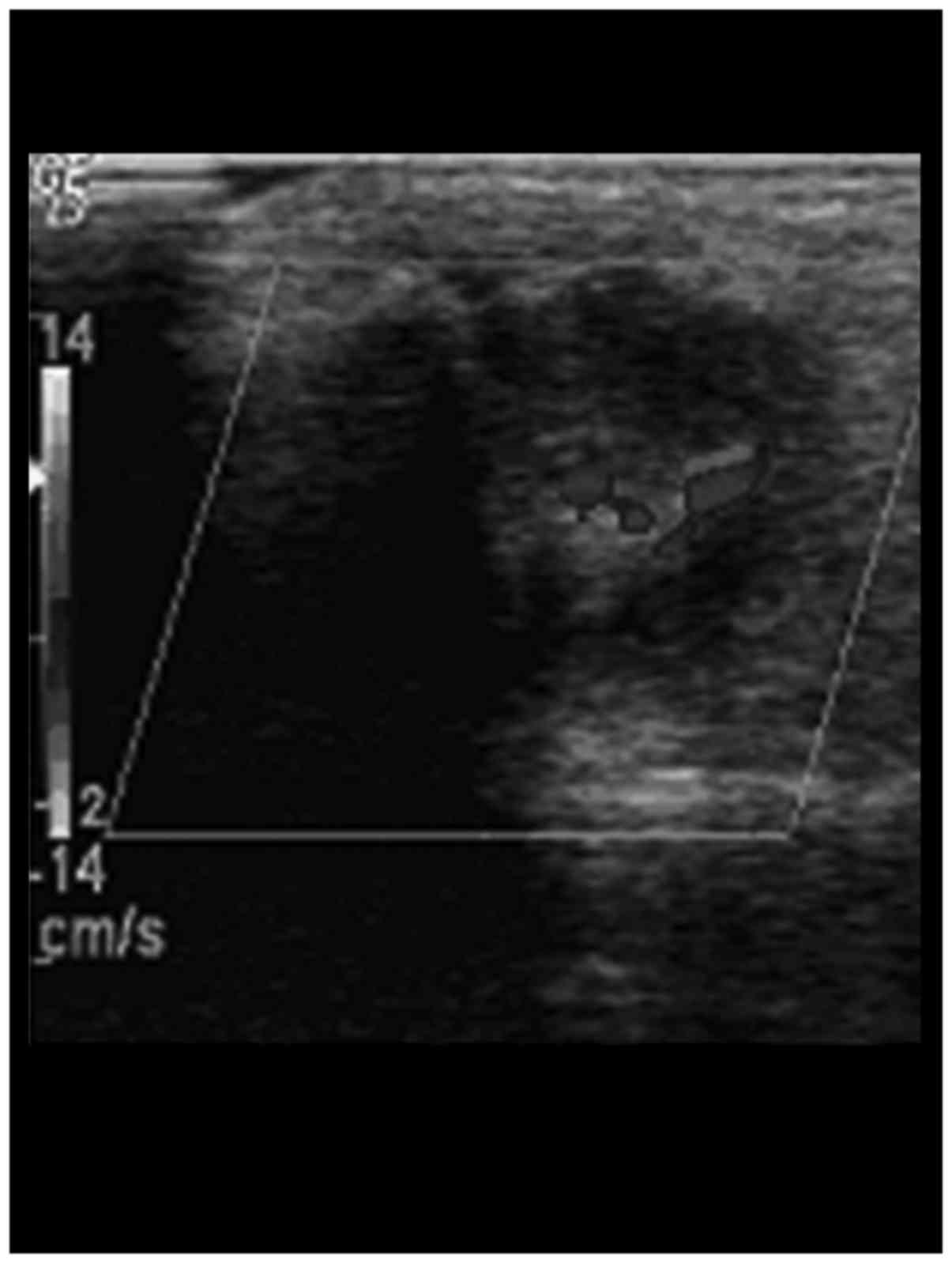
HCDU examination results showed that the
articulationes interphalangeae of digitus medius in patients with
bone erosion in the study group showed articular surface roughness,
and continuous interruption at the margins (Fig. 1). The detectable blood signal rate of
articulationes interphalangeae in the study group was 65.7%, and
blood signals were detected inside the articulationes
interphalangeae and at the margins (Fig.
2). The eroded cartilage and subcortex medullary bone substance
in the study group had lower echogenicity and irregularly defined
tumor-like lesion. The internal echo was uneven (Table I).
 | Table I.Comparison of the HCDU diagnoses for
the two groups (n=130). |
Table I.
Comparison of the HCDU diagnoses for
the two groups (n=130).
|
|
| Cortex of bone | Medullary substance
of bone |
|---|
|
|
|
|
|
|---|
| Group | No. of arthroses | Continuously
smooth | Discontinuously
rough | Not displayed | Tumor-like
lesion |
|---|
| Control, n=50 | 100 | 100 | 0 | 100 | 0 |
| Study, n=80 | 162 | 28 | 134 | 32 | 134 |
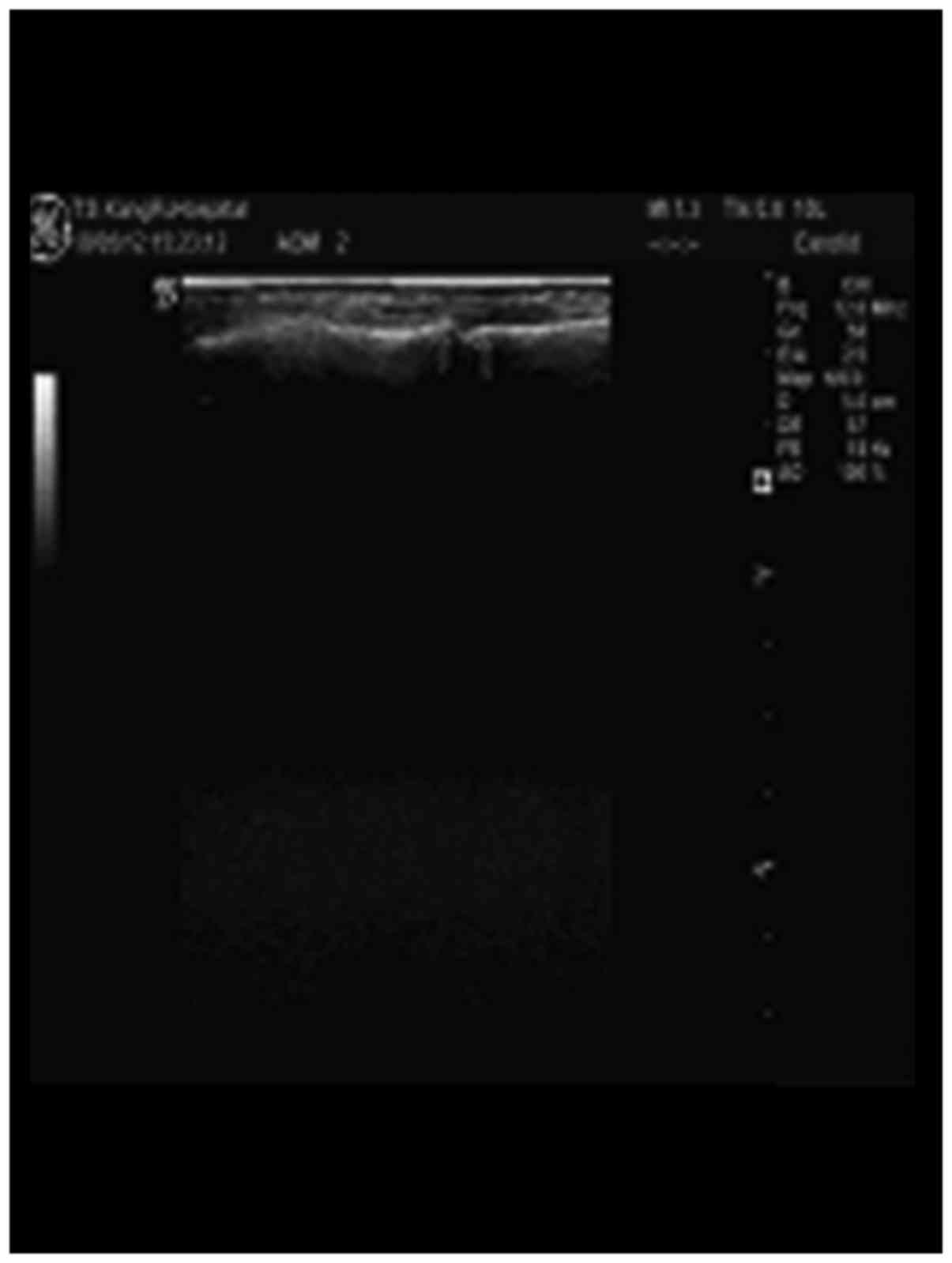
No blood signals were detected in the finger joints
in the control group, cortical bones and articular surfaces were
relatively smooth with continuous integrity. The ultrasonic
manifestation of cortical bones and subchondral bones showed a
strong echo line with continuous smoothness at the posterior edge
of cartilage. Behind that was the attenuation region and the
medullary substance of bone that could not be displayed (Fig. 3 and Table
I).
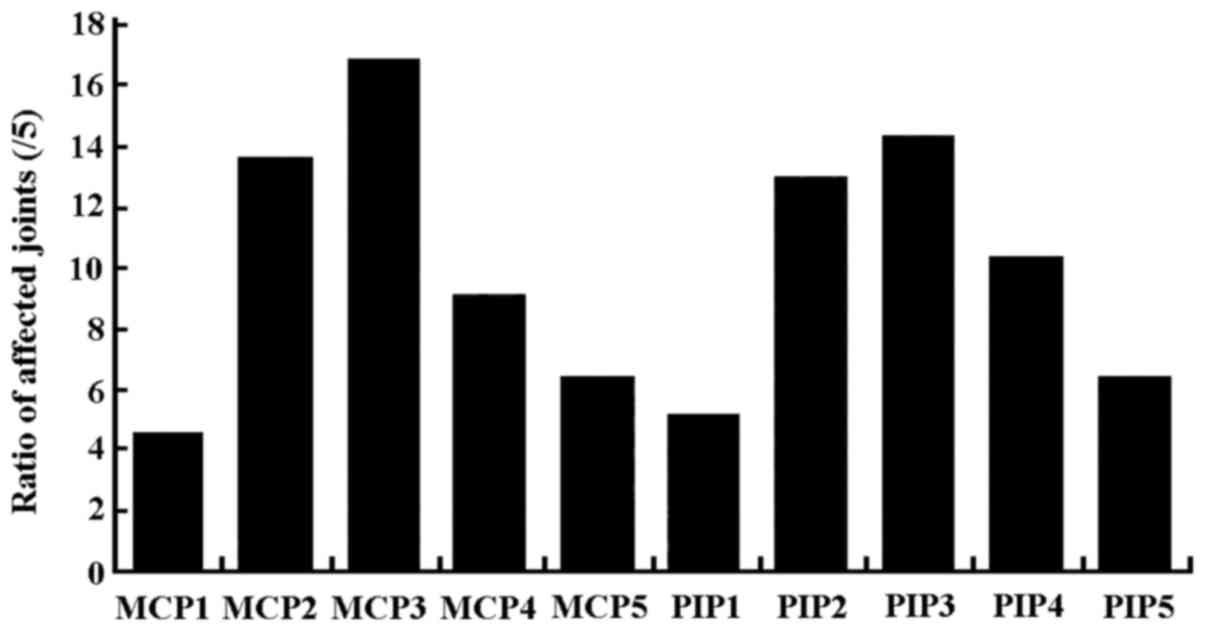
Affected levels of bone erosion of 80
patients
HCDU examination results showed that the
predominantly affected joint by bone erosion was MCP3 (16.7%),
followed by PIP3 (14.1%), MCP2 (13.5%) and PIP2 (12.8%). The
slightest affected joint was the thumb metacarpophalangeal joint,
followed by thumb, little finger metacarpophalangeal joint and
proximal interphalangeal joint (Fig.
4).
Result of diagnosing RA with a combination method of
CCP antibody testing and HCDU examination. The sensitivity of
diagnosing RA with both anti-CCP antibody testing and HCDU
examination was obviously lower than using each one of these
methods alone (P<0.05). The specificity was significantly higher
(P<0.05; Table II) (Fig. 5).
| Table II.Result of diagnosing RA with a
combination method of CCP antibody testing and HCDU
examination. |
Table II.
Result of diagnosing RA with a
combination method of CCP antibody testing and HCDU
examination.
| Method | Sensitivity, % | Specificity, % |
|---|
| CCP antibody
testing | 72.7 | 82.4 |
| HCDU examination | 71.1 | 83.8 |
| Combination of 2
methods |
47.3a,b |
98.5a,b |
Discussion
RA is a chronic inflammatory disorder that
characteristically affects the small joints in hands and feet
(7). RA generally starts in hand and
foot joints progressing to other areas including the knees, hips,
and shoulders. The key RA symptom is swollen joints, but RA can
also cause fatigue, fever, and weight loss. RA symptoms can cause
the joints to become permanently deformed over time which may lead
to permanent disability. As there is no cure for this disease,
disability caused by RA is irreversible. Prior studies demonstrated
that early diagnosis and treatment were effective on the patient
condition and lowered the osteoarticular damage and improved
prognosis. X-ray, often, is used as a routine method for RA
diagnosis; however, depending on the method of X-ray examination,
RA could only be detected several years after the appearance of the
symptoms (6,8,9).
Blood test to detect rheumatoid factors is also a
diagnostic tool which has its limitations (10–12). In
recent years, HCDU examination has received significant
consideration for indication of early diagnosis in arthritis with
no trauma that can be repeatedly operated (13–15). In
this study, the HCDU examination was indicated in RA patients
suffering from comparative articular surface roughness and
continuous interruption at the margins. Blood signals could be
observed on inner finger joints and at the margins. The eroded
cartilage and subcortex medullary substance of bone had low
echogenicity and irregularly defined tumor-like lesion, and the
internal echo was uneven. By contrast, HCDU examination on the
control group showed no blood signals in the finger joints,
cortical bones and articular surfaces were relatively smooth with
continuous integrity. Ultrasonic manifestation of cortical bones
and subchondral bones had a strong echo line with continuous
smoothness at the posterior edge of cartilage. Behind that was the
attenuation region and the medullary substance of bone could not be
displayed.
The positive blood ratio in interphalangeal joint
detected with HCDU previously (16)
was 10%, while the ratio in this study was 65.7%. Our results
suggested that by HCDU examination, the predominantly affected
joint by bone erosion was MCP3 (16.7%), followed by PIP3 (14.1%),
MCP2 (13.5%) and PIP2 (12.8%). The least affected joint was the
thumb metacarpophalangeal joint, followed by thumb, little finger
metacarpophalangeal joint and proximal interphalangeal joint.
Anti-CCP antibody test is particularly useful in the diagnosis of
RA. Anti-CCP antibody is a rheumatoid factor and elevated level of
anti-CCP is a sign that the patient may be more likely to develop
the disease (17,18). Studies suggested (19) that CCP antigens appeared in the RA
patients in early stage, and stimulated the proliferation of T
cells. However, the appearance of the anti-CCP antibodies was
highly related to the osteoarticular damage.
A prior study that conducted radiological evaluation
of the RA patients with 6 years of follow-up showed that patients
who were tested positive for anti-CCP antibody suffered more severe
bone damage than those with negative results (20). Other studies suggested that anti-CCP
antibody was related to RA bone erosion to a certain degree
(21). Results obtained in this
study showed that the positive rate of anti-CCP antibody in the
study group was 73.8%, and the negative rate was 26.2% (Fig. 5). The positive rate in the control
group was 10% (and the negative rate was 90%. Reports on the use of
HCDU examination in combination with anti-CCP antibody testing in
diagnosing RA are rare. Our results suggested that the sensitivity
of diagnosing RA with both anti-CCP antibody testing and HCDU
examination was obviously lower than using each of those methods
alone, while the specificity was significantly higher.
We concluded that a combination of HCDU examination
and anti-CCP antibody testing can be considered useful to improve
the early diagnostic rate of RA. HCDU examination is a sensitive,
secure, atraumatic and easily-operated diagnostic method for early
RA patients with finger joint damage. Combined with anti-CCP
antibody testing, it will provide a better chance for RA patients,
and give them hope for a better treatment and improved
prognosis.
References
|
1
|
Botar-Jid C, Bolboaca S, Fodor D, Bocsa C,
Tamas MM, Micu M, Dudea SM, Vasilescu D and Badea R: Gray scale and
power Doppler ultrasonography in evaluation of early rheumatoid
arthritis. Med Ultrason. 12:300–305. 2010.PubMed/NCBI
|
|
2
|
Ceccarelli F, Perricone C, Fabris M,
Alessandri C, Iagnocco A, Fabro C, Pontarini E, De Vita S and
Valesini G: Transforming growth factor β 869C/T and interleukin 6
−174G/C polymorphisms relate to the severity and progression of
bone-erosive damage detected by ultrasound in rheumatoid arthritis.
Arthritis Res Ther. 13:R1112011. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rizzo C, Ceccarelli F, Gattamelata A,
Vavala C, Valesini G and Iagnocco A: Ultrasound in rheumatoid
arthritis. Med Ultrason. 15:199–208. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hsu HJ, Yang YH, Shieh TY, Chen CH, Kao
YH, Yang CF and Ko EC: Role of cytokine gene (interferon-γ,
transforming growth factor-β1, tumor necrosis factor-α,
interleukin-6, and interleukin-10) polymorphisms in the risk of
oral precancerous lesions in Taiwanese. Kaohsiung J Med Sci.
30:551–558. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Orguc S, Tikiz C, Aslanalp Z and Erbay PD:
Comparison of OMERACT-RAMRIS scores and computer-aided dynamic
magnetic resonance imaging findings of hand and wrist as a measure
of activity in rheumatoid arthritis. Rheumatol Int. 33:1837–1844.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yang H, Rivoire J, Hoppe M, Srikhum W,
Imboden J, Link TM and Li X: Computer-aided and manual
quantifications of MRI synovitis, bone marrow edema-like lesions,
erosion and cartilage loss in rheumatoid arthritis of the wrist.
Skeletal Radiol. 44:539–547. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tamai M, Kawakami A, Iwamoto N, Kawashiri
SY, Fujikawa K, Aramaki T, Kita J, Okada A, Koga T, Arima K, et al:
Comparative study of the detection of joint injury in early-stage
rheumatoid arthritis by magnetic resonance imaging of the wrist and
finger joints and physical examination. Arthritis Care Res
(Hoboken). 63:436–439. 2011.PubMed/NCBI
|
|
8
|
Teruel JR, Burghardt AJ, Rivoire J,
Srikhum W, Noworolski SM, Link TM, Imboden JB and Li X: Bone
structure and perfusion quantification of bone marrow edema pattern
in the wrist of patients with rheumatoid arthritis: A multimodality
study. J Rheumatol. 41:1766–1773. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Carter JD, Patelli M, Anderson SR, Prakash
N, Rodriquez EJ, Bateman H, Sterrett A, Valeriano J and Ricca LR:
An MRI assessment of chronic synovial-based inflammation in gout
and its correlation with serum urate levels. Clin Rheumatol.
34:345–351. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Feehan L, Buie H, Li L and McKay H: A
customized protocol to assess bone quality in the metacarpal head,
metacarpal shaft and distal radius: a high resolution peripheral
quantitative computed tomography precision study. BMC Musculoskelet
Disord. 14:3672013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bensaoud N, Rostom S, Bahiri R and
Hajjaj-Hassouni N: Efficacy of tocilizumab on MRI-determined bone
oedema in rheumatoid arthritis. Clin Rheumatol. 34:1031–1037. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yu JI, Park YR, Lee SS and Chae SC:
Polymorphisms of interleukin-31 are associated with anti-CCP levels
in females with rheumatoid arthritis. J Genet. 93:813–817. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yousefghahari B, Alhooei S,
Soleimani-Amiri MJ and Guran A: Comparison of sensitivity and
specificity of anti-CCP and anti-MCV antibodies in an Iranian
cohort of patients with rheumatoid arthritis. Caspian J Intern Med.
4:702–706. 2013.PubMed/NCBI
|
|
14
|
Arkfeld DG: Biological significance of
anti-cyclic citrullinated peptide antibody in rheumatoid arthritis.
Ann Intern Med. 148:403–404; author reply 403–404. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Alexiou I, Germenis A, Ziogas A,
Theodoridou K and Sakkas LI: Diagnostic value of anti-cyclic
citrullinated peptide antibodies in Greek patients with rheumatoid
arthritis. BMC Musculoskelet Disord. 8:372007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Moghimi J, Ghorbani R, Hasani F and
Sheikhvatan M: Discriminative and diagnostic value of anti-cyclic
citrullinated peptide antibodies in Iranian patients with
rheumatoid arthritis. Rheumatol Int. 33:601–605. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Yang DH, Tu CC, Wang SC, Wei CC and Cheng
YW: Circulating anti-cyclic citrullinated peptide antibody in
patients with rheumatoid arthritis and chronic obstructive
pulmonary disease. Rheumatol Int. 34:971–977. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Perez-Alamino R, Garcia-Valladares I,
Cuchacovich R, Iglesias-Gamarra A and Espinoza LR: Are anti-CCP
antibodies in psoriatic arthritis patients a biomarker of erosive
disease? Rheumatol Int. 34:1211–1216. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vlad V, Berghea F, Libianu S, Balanescu A,
Bojinca V, Constantinescu C, Abobului M, Predeteanu D and Ionescu
R: Ultrasound in rheumatoid arthritis: volar versus dorsal
synovitis evaluation and scoring. BMC Musculoskelet Disord.
12:1242011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kroot EJ, de Jong BA, van Leeuwen MA,
Swinkels H, van den Hoogen FH, van't Hof M, van de Putte LB, van
Rijswijk MH, van Venrooij WJ and van Riel PL: The prognostic value
of anti-cyclic citrullinated peptide antibody in patients with
recent-onset rheumatoid arthritis. Arthritis Rheum. 43:1831–1835.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bas S, Perneger TV, Seitz M, Tiercy JM,
Roux-Lombard P and Guerne PA: Diagnostic tests for rheumatoid
arthritis: Comparison of anti-cyclic citrullinated peptide
antibodies, anti-keratin antibodies and IgM rheumatoid factors.
Rheumatology (Oxford). 41:809–814. 2002. View Article : Google Scholar : PubMed/NCBI
|