Introduction
Thrombosis is the most common cause of vascular
occlusion in ischemic stroke. Timely and accurate assessment of the
location, clot burden and size of the thrombus is of great
significance for guiding and monitoring the clinical treatment. The
hyperattenuated middle cerebral artery (MCA) sign on computed
tomography (CT) was the first imaging method for directively
detecting intra-arterial thrombus, but its diagnostic sensitivity
is only 22.6–40% (1,2), limiting its diagnostic value. In this
century, the susceptibility vessel sign (SVS) of the MCA on
gradient-recalled echo (GRE) imaging was demonstrated to be well
correlated with the hyperdense MCA sign on CT, and had a high
sensitivity varying in between 40 and 100% to detect intra-arterial
thrombus (3,4). The GRE SVS reflected thrombus composed
of deoxyhemoglobin produced by desaturation of oxyhemoglobin. Thus,
GRE SVS is present in older thrombi. In hyperacute clot cases, the
main component may still be oxyhemoglobin, and such emboli would
not be identified as GRE SVS on T2* imaging (4). The SVS on susceptibility-weighted
imaging (SWI) is based on a similar theory and also has a high
sensitivity and specificity to detect the intra-arterial thrombus
in acute stroke (5). Numerous
studies have assessed the predictive value of the characteristics
of SVS regarding the outcome of patients who had received
tissue-plasminogen activator (t-PA) administration or endovascular
treatment, and found that the location, clot burden and morphology
of the SVS may predict the absence of early recanalization or poor
outcome (6–12). However, none of these studies has
focused on SVS of patients untreated with reperfusion therapy.
Therefore, the present study used SWI to explore the association of
SVS with the clinical outcome for acute ischemic stroke patients
not subjected to thrombolysis.
Materials and methods
Patients
A retrospective study of patients with acute
ischemic stroke who were admitted to the People's Hospital of
Zhengzhou University (Zhengzhou, China) from January 2013 to May
2015 was performed. Patients were enrolled if they met the
following inclusion criteria: i) Acute cerebral infarction
confirmed by diffusion-weighted imaging (DWI); ii) cerebral
infarction distributed in the anterior circulation territory and
non-lacunar infarcts; and iii) a stroke magnetic resonance (MR)
imaging protocol including DWI, SWI and MR angiography (MRA)
performed within 3.0 days of the onset of symptoms. All patients
were treated with anti-platelet or anti-coagulant therapy. Patients
who had undergone thrombolytic therapy or endovascular treatment
were excluded. Stroke severities were evaluated by the National
Institutes of Health Stroke Scale (NIHSS) on admission. A favorable
outcome was defined as having a modified Rankin Scale (mRS) of 0–2
at 3.0 months after stroke, while a poor outcome was defined as
having an mRS >2 (13). The
Institutional Review Board of the People's Hospital of Zhengzhou
University (Zhengzhou, China) approved the present study; all
patients provided their informed consent for the entry of their
data/images into the stroke database.
The following baseline demographic and clinical
information on all patients was retrieved: Age, sex, time from
onset to treatment, time from onset to imaging, vascular risk
factors, atrial fibrillation, blood pressure before treatment,
fasting blood glucose and stroke etiology. Vascular risk factors
were identified as follows: i) Hypertension, a history of using
anti-hypertensive agents, a systolic blood pressure ≥140 mm Hg or a
diastolic blood pressure ≥90 mm Hg at hospital discharge; ii)
diabetes mellitus, use of hypoglycemics, random glucose level ≥11.1
mmol/l, or glycosylated hemoglobin >6.4% on admission; iii)
hyperlipidemia, use of anti-hyperlipidemic agents, or serum
cholesterol level >220 mg/dl; or iv) hyperhomocysteinemia, serum
homocysteine level >15 µmol/l. Stroke etiology was determined at
hospital discharge using the Trial of ORG 10 172 in Acute Stroke
Treatment (TOAST) criteria: i) Large-artery atherosclerosis; ii)
cardioembolism; or iii) a different determined or undetermined
etiology of stroke (14).
Small-vessel occlusion was excluded to ensure that the infarction
was derived from the large blood vessels.
MRI protocol
Multimodal MRI was performed on a Siemens Magnetom
Trio, Tim 3.0 T system (Siemens AG, Munich, Germany) using
commercially available hardware and software. The following
sequences were obtained: DWI [repetition time (TR), 3,100 msec;
echo time (TE), 82 msec; b-value, 1,000 sec/mm2;
acquisition matrix, 128×128; field of view (FOW), 240 mm; section
thickness, 6.0 mm; section gap; 1.2 mm; duration; 48 sec). SWI
(TR/TE/flip angle, 27 msec/20 msec/15°C; FOV, 240 mm, acquisition
matrix, 384×32; section thickness, 3.0 mm; duration, 3.0 min 27
sec). Three-dimensional time-of-flight MRA (TR/TE/flip angle, 20
msec/3.2 msec/18°; FOV, 230 mm, acquisition matrix, 256×256;
section thickness, 0.9 mm; duration, 3.0 min 6.0 sec).
Imaging analysis
All images were collected from the picture archiving
and communication system of the hospital as Digital Imaging and
Communications in Medicine-format data and imported to syngo
fastView version 02184790 (Siemens AG) for analysis. The MRA
rating, diffusion lesion volumes and SVS features were
independently assessed by two neurologists (H.L. and W.M.), who
were blinded to patient information, except for the clinical
history of ischemic stroke. Any disagreement was decided by
consultation with a neuroradiologist (Y.L.). The SVS was defined as
a hypointense signal on SWI within a vascular cistern, exceeding
the size of the homologous contralateral arterial diameter
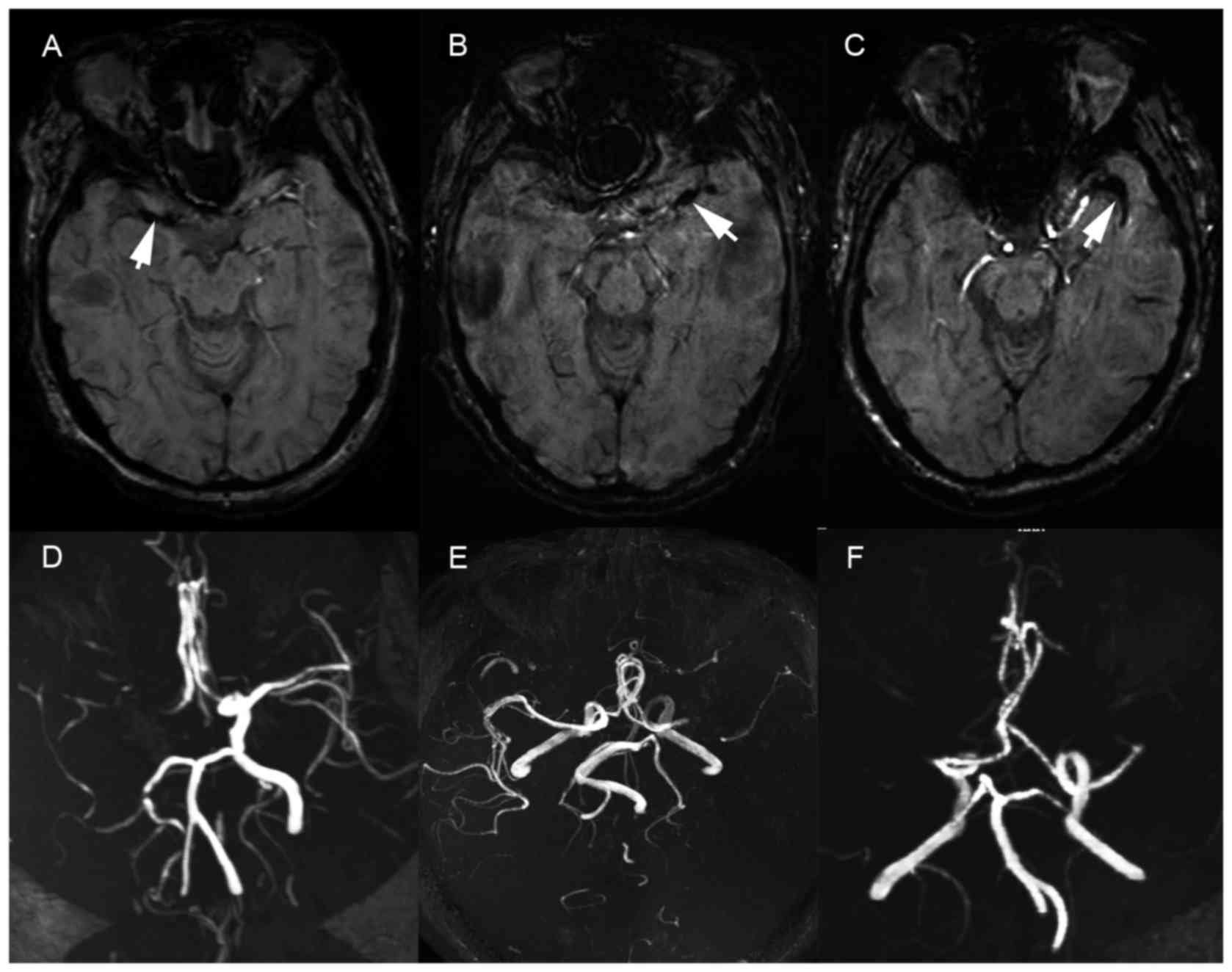
(4). The location and the length of
SVS were also assessed. Proximal M1 SVS was defined as an SVS at
the origin of the M1, distal M1 SVS was defined as any SVS not
including the origin of the M1 and distal MCA SVS was considered as
an SVS further away from M1 (Fig. 1)
(8). The thrombus length was
measured as the whole extension of the thrombus on SWI (15). All areas of diffusion were measured
by drawing regions of interest around the lesions by manual editing
on a slice-by-slice basis. DWI lesion volumes were identified as
the regions with an intensity higher than that in the contralateral
lobe by 3.0 standard deviations (SDs). Volumes were calculated by
multiplying overall outlined lesion areas by the slice thickness.
MRA was rated by using the modified thrombolysis in cerebral
infarction (TICI) score (16). The
vascular stenosis site was rated using the following assessment: 1,
internal carotid artery (ICA); 2, proximal MCA, including M1
segment of the MCA; 3, distal MCA, M2 segment of the MCA or further
branches.
Statistical analysis
First, all patients were classified into 2 groups
based on the presence of SVS. Clinical, radiological and laboratory
findings were compared between the 2 groups. Values are expressed
as the mean ± SD, median (25th, 75th percentile) or n (%).
Statistical comparisons were performed by independent samples
t-test for normally distributed continuous variables, the
Mann-Whitney U test for abnormally distributed continuous or
ordinal variables, and the χ2 test for categorical
variables. Furthermore, all patients were divided into 2 groups
based on a good or poor outcome at 3 months, and the clinical,
radiological and laboratory findings were compared between the 2
groups. Multivariate logistic regression analysis was used to
identify independent factors associated with poor outcome.
Variables identified on univariate analyses with P<0.05 were
entered into the multivariate analysis. Results are expressed as
adjusted odds ratios (ORs) and the corresponding 95% confidence
intervals (CIs). In addition, for patients with SVS, univariate and
multivariate analyses were performed to determine whether the
location and length of SVS were independent parameters associated
with poor outcome. Statistical significance was set at P<0.05.
All statistical analyses were performed using SPSS version 21 (IBM
Corp., Armonk, NY, USA).
Results
Patient characteristics
The 127 consecutive patients who met the inclusion
criteria were enrolled in the present study. A total of 11 patients
were excluded due to the following reasons: 6 were lost to
follow-up, 4 had received thrombolytic therapy and 1 had received
endovascular treatment. Of the 116 remaining patients who were
included in the study, 68.1% were men, the mean age of all patients
was 59.91±13.86 years, 20 were confirmed to have ICA stenosis, 64
had MCA M1 stenosis, 21 had stenosis at M2 or further branches of
the MCA and 11 had normal arteries. Stroke etiology according to
the TOAST classification was large artery atherosclerosis (n=98),
cardioembolism (n=10) and other determined and undetermined
etiologies (n=8). Sixty patients had infarction in the right
cerebral hemisphere and 56 had infarction in left hemisphere
(Table I).
 | Table I.Clinical characteristics and
radiological parameters of patients with and without SVS. |
Table I.
Clinical characteristics and
radiological parameters of patients with and without SVS.
| Variable | SVS(+) (n=43) | SVS(−) (n=73) | P-value |
|---|
| Age (years) | 60.35±13.21 | 59.66±14.31 | 0.796a |
| Sex, female | 10 (23.26) | 27 (36.99) | 0.125a |
| Time to MR imaging
(h) | 38 (24–50) | 40 (24–60) | 0.513b |
| Time to treatment
(h) | 24 (9–36) | 24 (15–48) | 0.114b |
| Systolic BP (mm
Hg) | 149.72±23.59 | 137.74±17.29 | 0.005a |
| Blood glucose
(mmol/l) | 5.56 (4.83–6.31) | 5.34 (4.44–6.80) | 0.424b |
| Stroke risk
factors |
|
|
|
|
Hypertension | 23 (53.49) | 35 (47.95) | 0.564a |
|
Hyperlipidemia | 19 (44.19) | 29 (39.73) | 0.522a |
| Diabetes
mellitus | 12 (27.91) | 15 (20.55) | 0.365a |
| Atrial
fibrillation | 4 (9.3) | 3 (4.1) | 0.465a |
|
Hyperhomocysteinemia | 27 (62.80) | 36 (49.32) | 0.159a |
|
Smoking | 12 (27.91) | 27 (36.99) | 0.317a |
| TOAST type |
|
| 0.062a |
| Large
artery atherosclerosis | 38 | 60 |
|
|
Cardioembolism | 5 | 5 |
|
| Other
etiologies | 0 | 8 |
|
| Infarct side,
right | 22 (51.2) | 38 (52.05) | 0.926a |
| Grade of TICI | 0 (0–1) | 2 (1–3) |
<0.001b |
| Location of
stenosis |
|
| 0.032a |
| ICA | 6 | 14 |
|
| Proximal
MCA | 29 | 35 |
|
| Distal
MCA | 8 | 13 |
|
| Normal
arteries | 0 | 11 |
|
| DWI lesion volume
(ml) | 65.08
(21.43–140.96) | 12.96
(4.71–33.52) |
<0.001b |
| NIHSS on
admission | 12 (5–20) | 5 (2–8) |
<0.001b |
| Favorable
outcome | 18 (41.9) | 58 (79.5) |
<0.001a |
Characteristics of SVS (+) vs. SVS (−)
patients
SVS were seen in 43 of the 116 patients. The
patients' clinical characteristics and imaging findings according
to the SVS presence are listed in Table
I. Compared with those in the SVS(−) group, patients with
SVS(+) had a higher systolic pressure (149.72±23.59 vs.
137.74±17.29 mmHg; P=0.005), lower TICI scores [0 (0–1) vs. 2
(1–3); P<0.001], larger infarction areas
[65.08 (21.43–140.96) vs. 12.96 (4.71–33.52) ml; P<0.001] and
higher NIHSS scores on admission [12 (5–20) vs. 5 (2–8);
P<0.001]. The TOAST classification of patients with SVS(+)
identified all of them as having had cardioembolic stroke or large
artery atherosclerosis. Of the 43 SVS(+) patients, 18 (41.9%) had
favorable outcomes, while 58 (79.5%) of the 73 SVS(−) patients
achieved good outcomes (P<0.001).
Factors associated with poor outcome
in patients with acute ischemic stroke
Table II presents
univariate analysis of the variables between patients with and
without favorable outcome. Patients with a poor outcome were older
than those with a good outcome (65.35±12.04 vs. 57.35±13.96 years;
P=0.002), more of them had atrial fibrillation (15 vs. 1.3%;
P=0.003) and the presence of SVS (62.5 vs. 23.7%; P<0.001) than
patients with a good outcome. The DWI lesion volumes were larger
[39.27 (17.24–154.47) vs. 13.53 (6.60–44.69) ml; P=0.001] and the
NIHSS scores on admission were higher [13.5 (7.25–22.75 vs. 5
(2–8); P<0.001] in patients with a poor
outcome than in those with a good outcome. The TICI scores were
lower in patients with a poor outcome [1 (0–2) vs. 2 (0–2);
P=0.043]. Compared with patients with favorable outcome, the TOAST
classification of patients with poor outcome was more likely to be
large artery atherosclerosis or cardioembolism (P=0.029). Finally,
seven factors including age, atrial fibrillation, the presence of
SVS, DWI lesion volume, NIHSS on admission, TICI score and TOAST
classification were entered into multivariate regression. The
results presented in Table III
revealed that besides NIHSS on admission and age, the presence of
SVS was an independent factor to predict poor outcome (OR, 3.390;
95% CI, 1.122–10.240; P=0.030).
| Table II.Univariate analysis of the variables
between patients with and without favorable outcome. |
Table II.
Univariate analysis of the variables
between patients with and without favorable outcome.
| Variable | mRS score >2
(n=40) | mRS score ≤2
(n=76) | P-value |
|---|
| Age (years) | 65.35±12.04 | 57.05±13.96 | 0.002a |
| Sex, female | 15 (37.5) | 22 (28.9) | 0.348a |
| Time to MR imaging
(h) | 40 (25.25–59) | 36 (24–58.5) | 0.409b |
| Time to treatment
(h) | 25.5 (16.5–48) | 24 (8–47) | 0.115b |
| Systolic BP (mm
Hg) | 140.5
(130.5–156) | 138
(128.25–153.75) | 0.221b |
| Blood glucose
(mmol/l) | 5.74
(4.76–7.68) | 5.34
(4.44–6.41) | 0.113b |
| Stroke risk
factors |
|
|
|
|
Hypertension | 23 (57.5) | 35 (46.05) | 0.271a |
|
Hyperlipidemia | 20 (50) | 28 (36.8) | 0.171a |
|
Diabetes mellitus | 10 (25) | 17 (22.4) | 0.75a |
| Atrial
fibrillation | 6 (15) | 1 (1.3) | 0.003a |
|
Hyperhomocysteinemia | 23 (57.5) | 40 (52.6) | 0.617a |
|
Smoking | 10 (25) | 29 (38.2) | 0.154a |
| TOAST type |
|
| 0.029a |
| Large
artery atherosclerosis | 34 | 64 |
|
|
Cardioembolism | 6 | 4 |
|
| Other
etiologies | 0 | 8 |
|
| Infarct side,
right | 22 (55) | 38 (50) | 0.608a |
| Grade of TICI | 1 (0–2) | 2 (0–2) | 0.043b |
| Location of
stenosis |
|
| 0.543a |
|
ICA | 8 | 12 |
|
|
Proximal MCA | 6 | 15 |
|
| Distal
MCA | 24 | 40 |
|
| Normal
arteries | 2 | 9 |
|
| DWI lesion volume
(ml) | 39.27
(17.24–154.47) | 13.53
(6.60–44.69) | 0.001b |
| NIHSS on
admission | 13.5
(7.25–22.75) | 5 (2–8) |
<0.001b |
| SVS | 25 (62.5) | 18 (23.7) |
<0.001a |
| Table III.Multivariate logistic regression
analysis for factors associated with an mRS score >2. |
Table III.
Multivariate logistic regression
analysis for factors associated with an mRS score >2.
| Factor | OR | 95% CI | P-value |
|---|
| For all enrolled
patients |
|
|
|
|
Age | 1.085 | 1.036–1.136 | 0.001 |
| Entry
NIHSS | 1.278 | 1.145–1.426 | <0.001 |
|
SVS | 3.39 | 1.122–10.240 | 0.03 |
| For patients with
SVS |
|
|
|
| Entry
NIHSS | 1.341 | 1.123–1.602 | 0.001 |
In the 43 patients with SVS, proximal M1 SVS was
seen in 18 (41.9%) patients; distal M1 SVS in 10 (23.3%) and distal
MCA SVS in 15 (34.9%). At 3 months after stroke, 18 patients
achieved a favorable outcome, while the outcome was poor in 25
patients. Univariate analysis of the variables between SVS positive
patients with and without favorable outcome are listed in Table IV. Patients with a poor outcome not
only had larger infarction volumes on DWI [92.44 (28.62–245.91) vs.
27.18 (11.82–99.93) ml; P=0.016] and higher NIHSS scores on
admission [17.6±8.12 vs. 6.39±3.99; P<0.001], but also a higher
rate of SVS located at the proximal M1 (P=0.044) and a greater SVS
length [19.7 (13.6–33.75) vs. 10.3 (8.1–20.98) mm; P=0.017].
Finally, NIHSS on admission, DWI lesion volume, the location of SVS
and the length of SVS were subjected to multivariate regression
analysis. However, only NIHSS on admission was an independent
predictor of poor outcome in this model (OR, 1.341; 95% CI,
1.123–1.602; P=0.001; Table
III).
| Table IV.Univariate analysis of the variables
between SVS positive patients with and without favorable
outcome. |
Table IV.
Univariate analysis of the variables
between SVS positive patients with and without favorable
outcome.
| Variable | mRS score >2
(n=25) | mRS score ≤2
(n=18) | P-value |
|---|
| Age (years) | 63.52±12.04 | 55.94±13.82 | 0.063a |
| Time to MR imaging
(h) | 39.84±20.16 | 33.11±17.11 | 0.258a |
| Time to treatment
(h) | 27.68±20.57 | 20.06±13.93 | 0.155a |
| Systolic BP (mm
Hg) | 154.4±23.54 | 143.22±22.71 | 0.127a |
| Blood glucose
(mmol/l) | 5.82
(4.85–7.59) | 5.37
(4.59–5.83) | 0.184b |
| Stroke risk
factors |
|
|
|
|
Hypertension | 13 (52) | 10 (55.6) | 0.818a |
|
Hyperlipidemia | 11 (44) | 8 (44.4) | 0.977a |
|
Diabetes mellitus | 6 (24) | 6 (33.3) | 0.501a |
| Atrial
fibrillation | 4 (16) | 0 (0) | 0.211a |
|
Hyperhomocysteinemia | 16 (64) | 11 (61.1) | 0.847a |
|
Smoking | 6 (24) | 6 (33.3) | 0.501a |
| TOAST type |
|
| 1.0a |
|
Large-artery
atherosclerosis | 23 | 17 |
|
|
Cardioembolism | 2 | 1 |
|
| Infarct side,
right | 14 (56) | 8 (44) | 0.661a |
| Grade of TICI | 0 (0–1) | 0 (0–1.25) | 0.382b |
| Location of
stenosis |
|
| 0.818a |
|
ICA | 4 | 2 |
|
|
Proximal MCA | 17 | 12 |
|
| Distal
MCA | 4 | 4 |
|
| DWI lesion volume
(ml) | 92.44
(28.62–245.91) | 27.18
(11.82–99.93) | 0.016b |
| Initial NIHSS | 17.6±8.12 | 6.39±3.99 |
<0.001a |
| Location of
SVS |
|
| 0.040a |
|
Proximal M1 | 14 | 4 |
|
| Distal
M1 | 3 | 7 |
|
| Distal
MCA | 8 | 7 |
|
| Length of SVS
(mm) | 19.7
(13.6–33.75) | 10.3
(8.1–20.98) | 0.017b |
Discussion
The present study demonstrated that the presence of
SVS was an independent predictor of poor outcome for patients with
acute anterior circulation stroke. For patients with SVS, only
NIHSS on admission but not the location and length of SVS was a
predictive factor of poor outcome at 3 months after stroke.
Magnetic susceptibility effects of the deoxygenated
hemoglobin in the red thrombus result in a hypointense signal on
T2* imaging. Cho et al (4)
defined these hypointense signals within the vascular cisterns on
T2* as ‘SVS’. The GRE SVS may reflect the thrombus composition.
Hemoglobin desaturation from oxyhemoglobin to deoxyhemoglobin
occurs within a few h. Thus, the GRE SVS is present in older
thrombi. Numerous studies have explored the predictive value of SVS
regarding early recanalization or outcome for patients with acute
stroke who had received reperfusion therapy. The presence of SVS
was reported to not be associated with recanalization or outcome,
but its location such as the proximal M1 (7,8,17), its clot burden score (CBS) such as
T2*-CBS >6 (10) and its
morphology such as angle and length (11) were all found to have a predictive
value regarding recanalization or outcome after t-PA therapy
(17).
To the best of our knowledge, the present study was
the first to investigate the association of SVS with the outcome
for acute stroke patients who had not received any reperfusion
therapy. The results demonstrated that in contrast to factors such
as age and NIHSS on admission, SVS was also an independent factor
to predict poor outcome 3 months after stroke. The following
reasons may explain this phenomenon. First, SVS reflects red
thrombi composed of erythrocyte-rich material (4). Patients with SVS have higher NIHSS
scores and larger DWI infarction volumes. The initial neurological
severity has an adverse impact on the clinical outcome.
Furthermore, proximal M1 SVS, SVS with T2*-CBS >6 and longer SVS
are resistant to intravenous thrombolysis (6,10,11); in
other words, distal MCA SVS, SVS with T2*-CBS <6, shorter SVS
are relatively easy to resolve and patients with such presentations
are more likely to benefit from reperfusion therapy. At present, as
none of the patients had received t-PA therapy, patients with
distal MCA SVS or shorter SVS did not benefit from reperfusion
treatment, so their outcome increased the probability of poor
prognosis for patients with SVS.
Certain characteristics of SVS, such as proximal M1
location and the length were negative predictors regarding
recanalization and clinical outcome for patients who received
intravenous thrombolysis (6,8,10,11) or
intra-arterial intervention (12).
However, the association of these parameters with the outcome for
patients not subjected to thrombolysis had remained elusive. The
present study found that in patients with SVS, the outcome was more
favorable if it was not located at the proximal M1 SVS and if SVS
had a shorter length. However, multivariate regression analysis
revealed that none of them was an independent predictor regarding
outcome. As mentioned above, an SVS at the proximal M1 represents a
larger thrombus compared with the other distal thrombi with SVS,
and a greater length of the SVS is indicative of a larger thrombus.
Therefore, SVS that are longer and located at the proximal M1 are
difficult to resolve by t-PA (8). By
contrast, patients whose SVS is shorter or located at the distal M1
or MCA are more likely to achieve recanalization and have a
favorable outcome. In the present study, as patients with small
thrombi, such as SVS with a short length located at the distal MCA,
did not benefit from reperfusion therapy, these parameters had no
obvious predictive value regarding clinical outcome.
The results of the present study revealed that the
TOAST category of patients with SVS was mostly cardioembolic stroke
or large artery disease. None of the patients with SVS had any
other etiologies of stroke, such as moyamoya disease or cryptogenic
stroke. As previous studies demonstrated that the location, burden,
morphology and length of the SVS were associated with no
recanalization or poor outcome after intravenous thrombolysis or
mechanical thrombectomy with stent retrievers, secondary prevention
such as anti-thrombosis or anti-coagulation therapy to prevent the
occurrence of SVS is important.
The present study supplemented previous studies,
which assessed the association between SVS and recanalization or
outcome for acute stroke patients who received reperfusion therapy.
Of note, the present study had several limitations. First, the
sample size was small. Furthermore, it was a retrospective study
and certain patients were lost to follow-up. This may have
contributed to selection bias. Third, sequence SWI was sensitive to
motion artifacts, which added difficulty to the identification of
SVS in certain patients.
In conclusion, the presence of SVS was found to be
an independent factor to predict poor outcome for patients with
acute stroke who had not received reperfusion therapy. The location
and length of SVS were not predictors of clinical outcome for such
patients.
Acknowledgements
The present study was supported by the Science and
Technology Project of Henan Province (grant no. 162102310295).
Glossary
Abbreviations
Abbreviations:
|
SVS
|
susceptibility vessel sign
|
|
MRI
|
magnetic resonance imaging
|
|
MCA
|
middle cerebral artery
|
|
SWI
|
susceptibility-weighted imaging
|
|
t-PA
|
tissue-plasminogen activator
|
|
DWI
|
diffusion-weighted imaging
|
|
MRA
|
magnetic resonance angiography
|
|
NIHSS
|
National Institutes of Health Stroke
Scale
|
|
mRS
|
modified Rankin Scale
|
|
CBS
|
clot burden score
|
|
TOAST
|
Trial of ORG 10 172 in Acute Stroke
Treatment
|
References
|
1
|
Somford DM, Nederkoorn PJ, Rutgers DR,
Kappelle LJ, Mali WP and van der Grond J: Proximal and distal
hyperattenuating middle cerebral artery signs at CT: Different
prognostic implications. Radiology. 223:667–671. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schellinger PD, Chalela JA, Kang DW,
Latour LL and Warach S: Diagnostic and prognostic value of early MR
Imaging vessel signs in hyperacute stroke patients imaged <3 h
and treated with recombinant tissue plasminogen activator. AJNR Am
J Neuroradiol. 26:618–624. 2005.PubMed/NCBI
|
|
3
|
Flacke S, Urbach H, Keller E, Träber F,
Hartmann A, Textor J, Gieseke J, Block W, Folkers PJ and Schild HH:
Middle cerebral artery (MCA) susceptibility sign at
susceptibility-based perfusion MR imaging: Clinical importance and
comparison with hyperdense MCA sign at CT. Radiology. 215:476–482.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cho KH, Kim JS, Kwon SU, Cho AH and Kang
DW: Significance of susceptibility vessel sign on T2*-weighted
gradient echo imaging for identification of stroke subtypes.
Stroke. 36:2379–2383. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Park MG, Yoon CH, Baik SK and Park KP:
Susceptibility vessel sign for intra-arterial thrombus in acute
posterior cerebral artery infarction. J Stroke Cerebrovasc Dis.
24:1229–1234. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kimura K, Iguchi Y, Shibazaki K, Watanabe
M, Iwanaga T and Aoki J: M1 susceptibility vessel sign on T2* as a
strong predictor for no early recanalization after IV-t-PA in acute
ischemic stroke. Stroke. 40:3130–3132. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Aoki J, Kimura K, Shibazaki K, Saji N,
Uemura J, Sakamoto Y and Nagai K: The susceptibility vessel sign at
the proximal M1: A strong predictor for poor outcome after
intravenous thrombolysis. J Neurol Sci. 348:195–200. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Aoki J, Kimura K, Shibazaki K, Sakamoto Y,
Saji N and Uemura J: Location of the susceptibility vessel sign on
T2*-weighted MRI and early recanalization within 1 hour after
tissue plasminogen activator administration. Cerebrovasc Dis Extra.
3:111–120. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aoki J, Kimura K, Shibazaki K, Saji N,
Uemura J, Sakamoto Y and Nagai K: The susceptibility vessel sign at
the proximal M1: A strong predictor for poor outcome after
intravenous thrombolysis. J Neurol Sci. 348:195–200. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Legrand L, Naggara O, Turc G, Mellerio C,
Roca P, Calvet D, Labeyrie MA, Baron JC, Mas JL, Meder JF, et al:
Clot burden score on admission T2*-MRI predicts recanalization in
acute stroke. Stroke. 44:1878–1884. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yan S, Hu H, Shi Z, Zhang X, Zhang S,
Liebeskind DS and Lou M: Morphology of susceptibility vessel sign
predicts middle cerebral artery recanalization after intravenous
thrombolysis. Stroke. 45:2795–2797. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Soize S, Batista AL, Regent C Rodriguez,
Trystram D, Tisserand M, Turc G, Serre I, Ben Hassen W, Zuber M,
Calvet D, et al: Susceptibility vessel sign on T2* magnetic
resonance imaging and recanalization results of mechanical
thrombectomy with stent retrievers: A multicentre cohort study. Eur
J Neurol. 22:967–972. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yan S, Hu H, Shi Z, Zhang X, Zhang S,
Liebeskind DS and Lou M: Morphology of susceptibility vessel sign
predicts middle cerebral artery recanalization after intravenous
thrombolysis. Stroke. 45:2795–2797. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Adams HP Jr, Bendixen BH, Kappelle LJ,
Biller J, Love BB, Gordon DL and Marsh EE III: Classification of
subtype of acute ischemic stroke. Definitions for use in a
multicenter clinical trial. TOAST. Trial of Org 10172 in acute
stroke treatment. Stroke. 24:35–41. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Naggara O, Raymond J, Ayllon M Domingo,
Al-Shareef F, Touzé E, Chenoufi M, Gerber S, Mellerio C, Zuber M,
Meder JF, et al: T2* ‘susceptibility vessel sign’ demonstrates clot
location and length in acute ischemic stroke. PLoS One.
8:e767272013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Higashida RT, Furlan AJ, Roberts H,
Tomsick T, Connors B, Barr J, Dillon W, Warach S, Broderick J,
Tilley B, et al: Trial design and reporting standards for
intra-arterial cerebral thrombolysis for acute ischemic. stroke.
34:e109–e137. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Apoil M, Turc G, Tisserand M, Calvet D,
Naggara O, Domigo V, Baron JC, Oppenheim C and Touzé E: Clinical
and magnetic resonance imaging predictors of very early
neurological response to intravenous thrombolysis in patients with
middle cerebral artery occlusion. J Am Heart Assoc. 2:e0005112013.
View Article : Google Scholar : PubMed/NCBI
|