Introduction
Worldwide, ovarian cancer is the most common, with
the highest incidence and mortality, of all gynecologic
malignancies (1). Ovarian cancer is
a diverse disease and it presents high morbidity and mortality as
it is often diagnosed at a late stage (2). Previous research has reported that the
incidence rate of ovarian cancer is increasing worldwide and
presents a rapid expansion trend (3). Women with ovarian cancer demonstrated
continued symptoms of depression and anxiety for cancer survivors
who had undergone chemotherapy treatment, according to a
meta-analysis of prevalence rates (4). Ineffective or prolonged management of
treatment could contribute to worsening of symptoms, treatment
noncompliance and even reduced health-related quality of life
(5).
Previous studies of ovarian cancer have been
large-scale, multiregional and longitudinal cohorts for diagnosis,
treatments and prognosis in preclinical and clinical trials
(6–8). Increasing reports were engaged to
research and improve treatment for patients with ovarian cancer,
focusing on the improvement of diagnosis and the identification of
novel therapies (3). In addition,
the overall prognosis and therapy for patients with ovarian cancer
remained poor despite increasing improvements in perioperative
management, surgical techniques and other treatments (9,10).
Therefore, effective therapeutic agents and protocols for patients
with ovarian cancer are urgently required due to the high rate of
occurrence and likelihood of metastasis following curative
resection in clinics (11).
Treatments for ovarian cancer have been demonstrated
to be poor at prevention and ineffective, resulting in a bad
prognosis (12). The majority of
newly diagnosed ovarian cancer cases are often at an advanced stage
due to the lack of sensitive screening diagnosis at the early stage
(13). Traditional treatments,
including radiotherapy, chemotherapy and surgery, are limited to
palliative approaches for patients with advanced ovarian cancer
(2,14). However, many patients with advanced
ovarian cancer respond poorly to such treatments, with these
traditional treatments demonstrating limited efficacy (15). Therefore, adjunctive therapeutic
options are important for patients after receiving one or more
anticancer treatments.
Immunotherapy is an efficient treatment for cancer
due to its antitumor effects induced by stimulating host immune
responses for cytotoxic lymphocyte activities against cancer cells
in the microenvironment (16).
Molecular mechanisms that inhibit systemic metastasis of ovarian
cancer would be a novel therapeutic candidate for patients with
ovarian cancer (17,18). Cellular immunotherapy exhibits
immense potential to be a highly-targeted alternative to
traditional treatments, which possesses the lowest or no toxicity
to normal cells and demonstrates notable capacity to eradicate
tumor cells (19–21). Cellular immunotherapy often employs
active immunization with immune cells, including infiltrating T
cells, effectors T cells and cytotoxic T cells, using adoptive
transfer of T cells from the patients themselves to directly target
antigens on malignant cells (22,23). The
present study generated an efficient cellular therapy by using NK
cells in an ovarian xenograft mouse model. The results suggested
that natural killer (NK) immunotherapy inhibits the systemic
metastasis of tumors in mice with ovarian cancer, which provided
preclinical information of the potential role of NK cells for
patients with ovarian cancer.
Materials and methods
Ethics statement
The present study was approved by the Ethics
Committee of Weifang City People's Hospital (Weifang, China).
Cells culture and reagents
Ovarian cancer cells from one patient with ovarian
cancer (54.2 years old) were collected with written informed
consent on May 2015 in Weifang People's Hospital (Weifang, China).
Cells were cultured in Dulbecco's modified Eagle's medium (DMEM,
Biowhittaker; Lonza Group, Ltd., Basel, Switzerland) supplemented
with 10% fetal bovine serum (FBS; Biowhittaker; Lonza Group, Ltd.)
at 37°C and 5% CO2 for 24 h. Peripheral blood
mononuclear cells (PBMCs) were isolated from healthy mice and
cultured as described in a previous study (24). SKOV3, OVCAR3, CAOV-3 and A2780 cells
were purchased from the Cell Bank of the Chinese Academy of Science
(Shanghai, China). All tumor cells were cultured in DMEM
supplemented with 10% heat-inactivated FBS and 1%
penicillin/streptomycin under standard culture conditions (5%
CO2, at 37°C) for 12 h.
Lactate dehydrogenase (LDH) assay
The ovarian tumor cells were cultured until a 90%
confluency of monolayer cells was reached and then the media was
removed. The ovarian tumor cells were washed with PBST three times
and subsequently incubated with Triton X-100 (1%) for 30 min at
37°C. LDH activity in the lysates was measured by using a Promega
CytoTox 96 assay kit (Promega Corporation, Madison, WI, USA). The
procedures were conducted according to the manufacturer's
protocol.
Cell invasion and migration
assays
Patient-derived ovarian cancer cells were treated
with NK cells (effector:target ratios=15:1) for 24 h at 37°C and
non-treated cells were used as control. For the invasion assay,
NK-treated cells were suspended at a density of 1×105/ml
cells in 500 µl serum-free DMEM. Matrigel-coated and uncoated
Transwell inserts (8 µm pore size; Merck KGaA, Darmstadt, Germany)
were used to evaluate cell invasion and migration, respectively.
The ovarian tumor cells (2×105) were then subjected to
the tops of BD BioCoat Matrigel Invasion Chambers (BD Biosciences,
Franklin Lakes, NJ, USA) for 48 h at 37°C according to the
manufacturer's protocol. For the migration assay, patient-derived
ovarian cancer cells were treated with NK cells and PBS for 48 h
using a control insert (BD Biosciences) instead of a Matrigel
Invasion Chamber. DMEM and DMEM with 5% FBS was plated in the upper
and lower chambers, respectively. Cells were then fixed in 4%
paraformaldehyde for 15 min at 37°C and stained with 0.1% crystal
violet dye (Sigma-Aldrich; Merck KGaA) for 20 min at 37°C. Tumor
cell invasion and migration was counted in at least three randomly
stained fields under a light microscope (Olympus Corporation,
Tokyo, Japan) for every membrane (magnification, ×40).
Expansion of NK cells in vitro
NK cell expansion was performed in vitro by
using VarioMACS (Miltenyi Biotec GmbH, Bergisch Gladbach, Germany)
and cultured in MEM medium (Thermo Fisher Scientific, Inc.,
Waltham, MA, USA) for 72 h at 37°C. On day 5, MEM medium (Thermo
Fisher Scientific, Inc.) was refreshed with the addition of
autoplasma (1%) (Sigma-Aldrich; Merck KGaA) and interleukin-2 (500
IU/ml) (Sigma-Aldrich; Merck KGaA). Culture continued for 14 days
at 37°C. Cells were then fixed with 4% paraformaldehyde for 15 min
at 37°C and the viability of expanded NK cells was determined by 5%
propidium iodide staining for 2 h at 37°C as described previously
(25). In vitro-expanded NK
cells were stained with primary antibodies and analyzed using a
flow cytometer with antibodies and FCS Express™ 4 IVD
software (De Novo Software, Glendale, CA, USA), as described in a
previous study (24).
Animal experiments
A total of 40 female specific pathogen-free female
BALB/c (6-week old; body weight, 28–32 g) nude mice were purchased
from Harbin Veterinary Research Institute (Harbin, China). All mice
were feed under pathogen-free conditions. All rats were housed
under controlled temperatures in 23±1°C with a relative humidity of
50±5% and a 12 h light/dark cycle with ad libitum access to food
and water. A density of 1×106 CAOV-3 cells were injected
into the right flank of female BALB/c nude mice in a total volume
of 200 µl PBS. Therapy for tumor-bearing mice by NK cells was
initiated when tumor diameters reached 6–8 mm on day 7 after tumor
inoculation. Mice with ovarian carcinoma were randomly divided into
two groups (n=20 in each experimental group) and injected
intratumorally with 2×106 NK cells or the same volume
PBS as a control. The treatment was continued five times, with
injections administered at intervals of every 2 days. Tumor
diameters (n=6) were recorded once every 2 days and tumor volume
was calculated using the following formula: 0.52 × smallest
diameter2 × largest diameter. Tumor metastasis was
evaluated by tumor occurrence in other subcutaneous sites. Mice
were sacrificed when the tumor diameter reached 12 mm.
Splenocyte collection and cytotoxic T
lymphocyte (CTL) responses
Splenocytes were obtained from the spleens of
experimental mice following treatment. The monoplast suspension of
splenocytes was then washed with PBST. Ovarian tumor cells were
subsequently inactivated using ultraviolet ray for 2 h at 37°C and
then subjected to incubation with splenocytes for 48 h at 37°C.
Interferon (IFN)-γ release was determined using an ELISA kit (cat.
no. MIF00; Bio-Rad Laboratories, Inc., Hercules, CA, USA) after
culture for 72 h at 37°C, according to the manufacturer's
instructions. Meanwhile, T cells (1×106) from the
splenocytes were purified (25) and
co-cultured with fresh ovarian tumor cells in DMEM for 4 h at 37°C
at the effector: Target ratios of 5:1, 15:1 and 30:1. Specific CTL
activity to the target cells was determined by LDH Assay Kit (cat.
no. ab102526; Abcam, Cambridge, UK) (26).
Flow cytometry
Ovarian tumor cells were isolated from experimental
mice as described previously (27)
and washed three times with PBS. Cell suspensions were filtered
through a 100 µm nylon strainer. Tumor cells were blocked with 2%
BSA (Sigma-Aldrich; Merck KGaA) for 2 h at 37°C and then washed
with PBS three times at room temperature. Cells were then labeled
with the following antibodies sourced from Abcam: CD69 (1:1,000;
cat. no. ab202909), CD3 (1:1,000; cat. no. ab16669) and CD45
(1:1,000; cat. no. ab10558), plus CD4 (1:1,000; cat. no. ab183685)
and CD8 (1:1,000; cat. no. ab22378) staining for 2 h at room
temperature to determine the frequency of CD4 and CD8 cell subsets
in the total infiltrated immune cells. Cells were washed with PBS
three times at room temperature and then incubated with horseradish
peroxidase-conjugated Goat Anti-Rabbit Imunnoglobulin G H&L
(Alexa Fluor® 488; 1:2,000; cat. no. ab150077; Abcam)
for 1 h at 37°C. The stained cells were analyzed using FCS
Express™ 4 IVD software (De Novo Software).
Immunohistochemistry
Paraffin-embedded tumor tissue sections (5 µm) were
fixed using and 4% formaldehyde for 2 h at room temperature and
epitope retrieval was performed by heating the samples to 100°C for
30 min in a citrate solution (10 mmol/l; pH 6.0) followed by
dewaxing in xylene and rehydration in graded ethanol solutions for
further analysis. The paraffin sections were subjected to hydrogen
peroxide (3%) for 10–15 min and subsequently blocked using a
regular blocking solution (5% BSA; Sigma-Aldrich; Merck KGaA) for
10–15 min 37°C. Finally, the sections were incubated at 4°C for 12
h with the following primary antibodies sourced from Abcam: Anti-NK
(1:100; cat. no. ab36388), anti-KI67 (1:500; cat. no. ab15580),
anti-major histocompatibility complex (MHC) I (HLA-A; 1:500; cat.
no. ab209541) and anti-leukomonocyte antibody (CD3; 1:1,000; cat.
no. ab16669) and CEA (1:500; cat. no. ab33562). Sections were then
washed three times with PBS and incubated with horseradish
peroxidase-conjugated goat anti-rabbit IgG monoclonal antibodies
(1:2,000; cat. no. PV-6001; OriGene Technologies, Inc., Beijing,
China) for 1 h at 37°C and counterstained with hematoxylin or
4′,6-diamidino-2-phenylindole. The relative expression of NK1.1,
MHC I and lymphocytes were determined by the means of six random
views under the microscope.
Terminal
deoxynucleotidyl-transferase-mediated dUTP nick end labeling
(TUNEL) analysis
Tumor tissue sections (5 µm) were fixed with 4%
paraformaldehyde solution for 2 h at 4°C. Sections were washed
three times with PBS and then permeabilized by immersing cells
slides in a 0.2% TritonX-100 solution with PBS for 14 min at 4°C.
Subsequently, sections were incubated with an equilibration buffer
for 14 min at 4°C and were then incubated with 50 µl reaction
mixture at 37°C for 60 min and washed 3 times with PBS. The tissues
were washed with PBS three times at room temperature and then the
TUNEL Apo-Green Detection kit (cat. no. A111-01-VAZ; Biotool,
Stratech Scientific Ltd., Suffolk, UK) was used according to the
manufacturers protocol to detect TUNEL-positive cells. Finally,
tissue section was placed on glass slides and tissue section images
were captured at 6 fields of view using fluorescent microscope
(Olympus Corporation) at a magnification of ×40.
Statistical analysis
All data were reported as the mean ± standard error
of the mean. All data were analyzed using SPSS Statistics 19.0
(SPSS, Inc., Chicago, IL, USA). Unpaired data were analyzed by the
Student's t-test. Comparisons of data between multiple groups were
analyzed by one-way analysis of variance followed by a Bonferroni
post-hoc test. P<0.05 was considered to indicate a statistically
significant difference.
Results
NK cells inhibit ovarian cancer cell
growth, migration and invasion
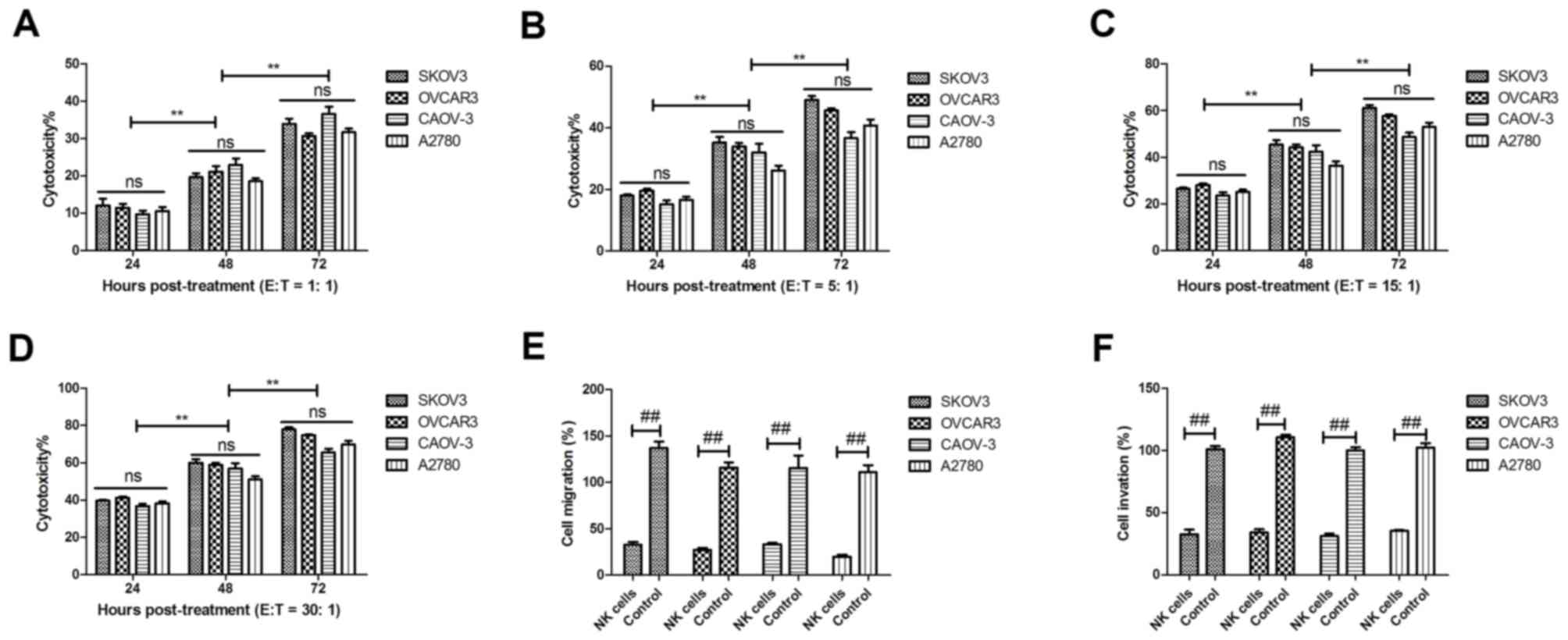
Ovarian cancer cell lines (SKOV3, OVCAR3, CAOV-3 and
A2780) were cultured and analyzed for inhibitory effects on growth
and migration of NK cells. Cytotoxic effects of NK cells against
SKOV3, OVCAR3, CAOV-3 and A2780 and were evaluated by LDH assays
in vitro. SKOV3, OVCAR3, CAOV-3 and A2780 cells were
co-cultured with NK cells (effector: Target=30:1, 15:1, 5:1 or 1:1)
for 24, 48 and 72 h. As demonstrated in Fig. 1A-D, NK cells from patients with
ovarian cancer lysed cancer cells in a dose-dependent and
time-dependent manner.
Migration and invasion are key characteristics for
metastasis of ovarian tumor cells. Therefore, the present study
analyzed the inhibitory effects of NK cells on migration and
invasive ability in a parallel assay. As expected, the capacities
of tumor migration and invasion were significantly suppressed
following treatment with NK cells (effector: Target=5:1) compared
with the levels in control cells (Fig.
1E and F). These data suggest that effector NK cells are able
to lyse ovarian SKOV3, OVCAR3, CAOV-3 and A2780 cells, and also
inhibit migration and invasion of these ovarian cancer cells.
NK cell distribution in xenograft
murine model of ovarian cancer and MHC I molecule expression in NK
cell-treated tumors
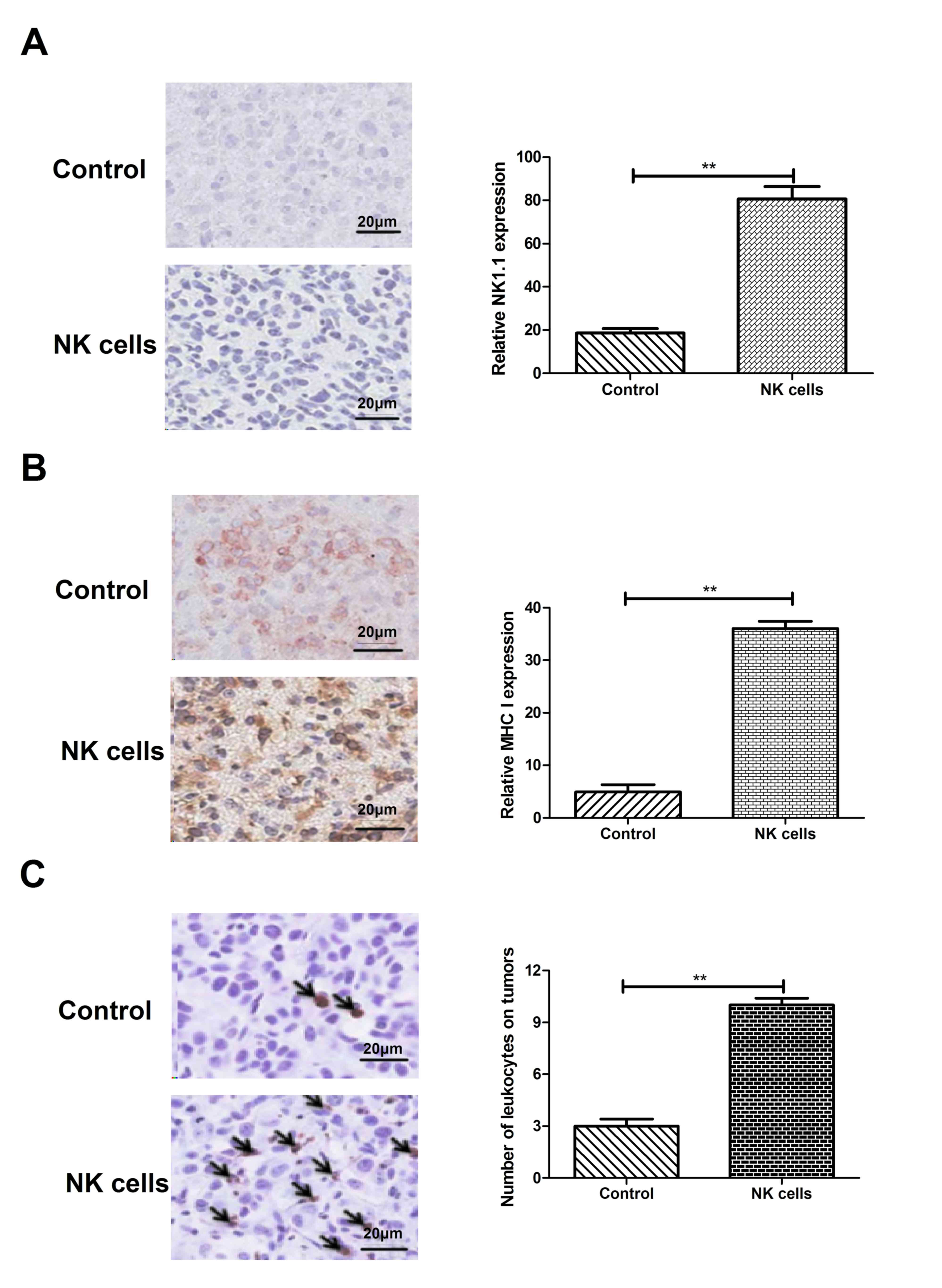
The molecular mechanism of NK cells for xenograft
mice has been elucidated and has demonstrated beneficial outcomes
in preclinical trails (28). The
present study investigated whether NK cells could increase tumor
invasion and MHC I molecule expression in the tumors of xenograft
mice. NK cell distribution was analyzed using immunohistochemistry
against NK cell marker NK1.1 in the xenograft ovarian tumors. As
demonstrated in Fig. 2A, the level
of NK1.1-positive cells was significantly lower in tumors from the
BALB/c-nude mice without NK cell treatment compared with the level
in those treated with NK cells. In addition, the present study
evaluated MHC I molecule expression in the patient-derived
xenograft murine model of ovarian cancer, as MHC class I molecules
emit inhibitory signals for NK cells (29). The results in Fig. 2B demonstrate that MHC I expression
was significantly higher in the xenograft mice in the presence of
NK cells compared with the level in the control mice. Furthermore,
the total leukocytes were analyzed in presence of NK cells in
xenograft mice. As demonstrated in Fig.
2C, the total number of leukocytes was significantly
upregulated in the NK cell treatment group compared to the number
in the control group. These results indicate that NK cell treatment
increased NK1.1 and MHC I molecule expression, which would increase
the possibility that NK cells may recognize invasive and/or
migrating ovarian tumor cells.
NK cells suppress metastasis of
patient-derived ovarian cancer cells in a xenograft murine
model
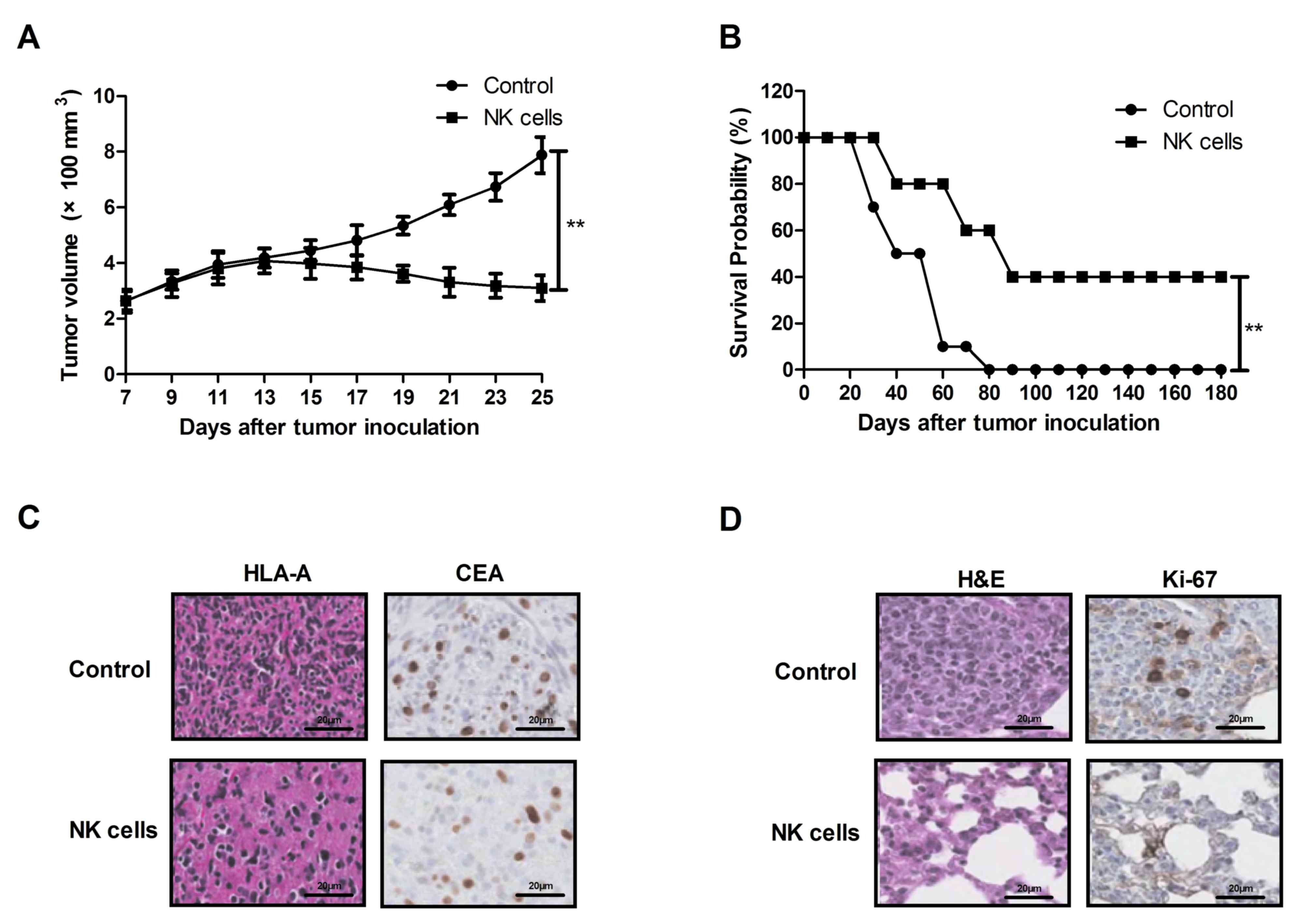
In the present study, BALB/c-nude mice were used to
analyze suppression efficacy of NK cells on ovarian cancer cell
metastasis. According to the hypothesis, immune deficient
BALB/c-nude mice were implanted with patient-derived CAOV-3 cells
(1×106 density) in a total volume of 200 µl by injection
of the right flank. Compared with the control treatment mice, NK
cell treatment demonstrated a significant inhibitory effect on
tumor growth of ovarian cancer cells on day 25 (Fig. 3A; n=20/group). In addition, median
survival of the mice in the NK cell treatment group was
significantly longer than those of the PBS treatment group in a
180-day observation (Fig. 3B;
n=10/group). These results indicate that treatment with NK cells
had beneficial effects on the inhibition of ovarian cancer cell
metastasis in vivo and tumor formation of patient-derived
ovarian cancer cells.
It was observed that 10 experimental mice had >1
tumor in the control group, while only 2 experimental mice had
>1 tumor in the NK group. The mean tumor diameters are
demonstrated in Table I.
Furthermore, formation of xenograft ovarian tumors was also
confirmed by immunohistochemistry and pathology (Fig. 3C and D). These results indicate that
metastasis of ovarian tumor cells was inhibited by circulating
immune cells in the blood stream, which suggests that sufficient
supplementation of NK cells in the circulating system may be a
promising immunotherapeutic strategy for patients with ovarian
cancer.
 | Table I.Number of tumors and tumor diameter
in mice demonstrating >1 tumor on day 25. |
Table I.
Number of tumors and tumor diameter
in mice demonstrating >1 tumor on day 25.
|
| Tumor
parameter |
|---|
|
|
|
|---|
| Group | n | Diameter, mm |
|---|
| PBS |
|
|
| 1 | 2 | 4.02, 4.52 |
| 2 | 2 | 3.18, 3.86 |
| 3 | 2 | 4.14, 4.32 |
| 4 | 2 | 3.45, 3.66 |
| 5 | 3 | 4.42, 4.32,
3.45 |
| 6 | 2 | 3.22, 4.32 |
| 7 | 2 | 2.56, 4.35 |
| 8 | 2 | 4.56, 4.86 |
| 9 | 2 | 6.32, 4.04 |
| 10 | 3 | 5.21, 4.12,
2.18 |
| Natural killer cell
treatment |
|
|
| 1 | 2 | 3.02, 3.98 |
| 2 | 2 | 3.92, 4.28 |
In vivo therapeutic effects of NK
cells against xenograft mice with ovarian tumors
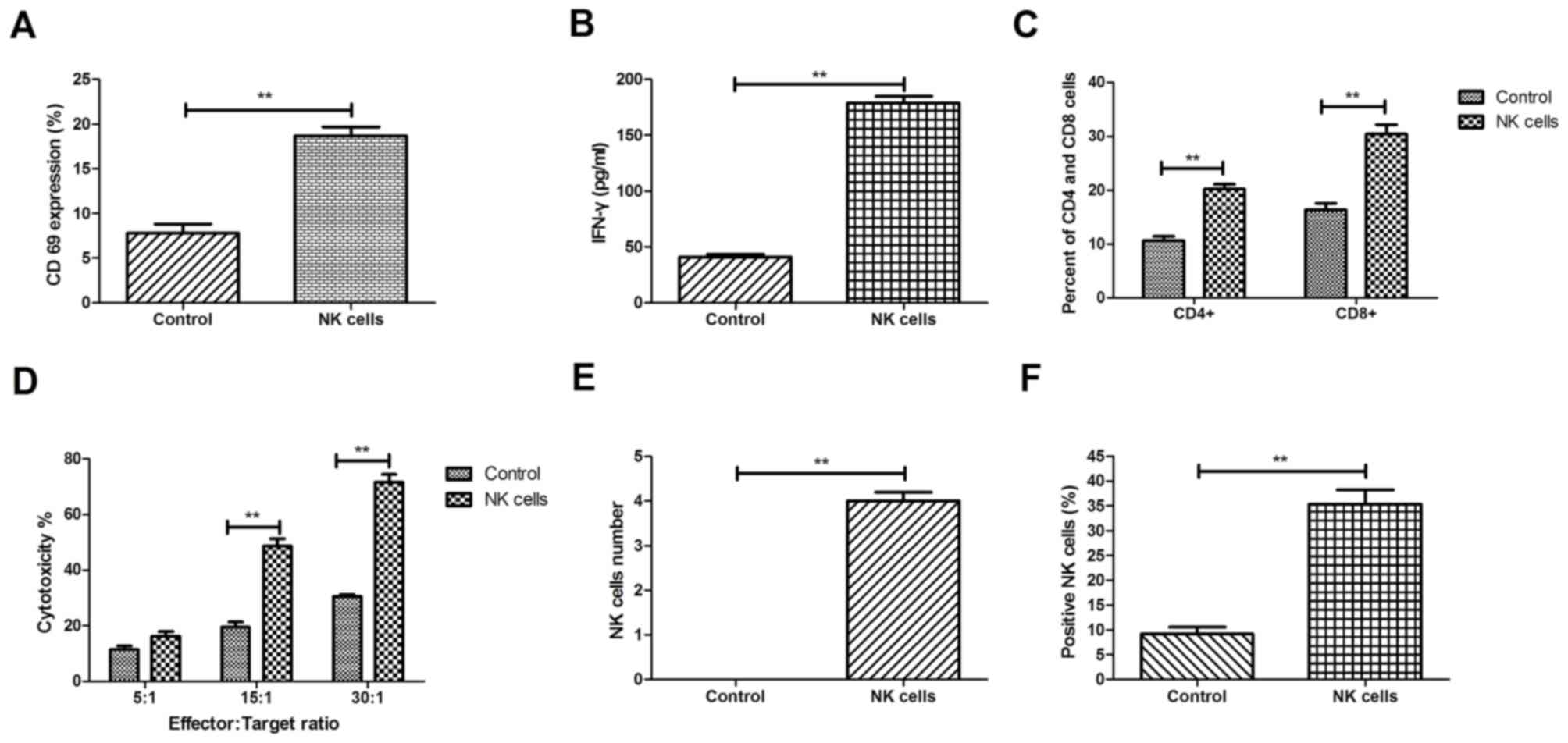
As it was observed that NK cells stimulated the
immune system in xenograft mice with ovarian tumors and
demonstrated antitumor effects, the activation status of T cells by
the release of the T cell cytokine IFN-γ and CD69 was further
analyzed. As demonstrated in Fig.
4A, CD69 expression was significantly increased following NK
cell treatment compared with the expression level following the
control treatment, as determined by the mean fluorescence
intensity. Furthermore, the release of the T cell cytokine IFN-γ
was also significantly increased in xenograft mice with ovarian
cancer following treatment with NK cells compared with the level in
the control mice (Fig. 4B). In
addition, the percentage of CD4+ and CD8+ T
cells was upregulated following NK cell treatment compared with the
percentage in the control treatment (Fig. 4C). CTL responses were initiated by
stimulation with NK cell-treated tumor cells. The present data
indicate that stronger CTL responses were presented (~60%)
following treatment with NK cells on day 7 (Fig. 4D). Furthermore, the number of NK
cells was also increased in xenograft mice administrated with NK
cells compared with the rate in the control treatment, as
determined by TUNEL-positive apoptotic cells (Fig. 4E). The NK cells were evaluated in the
tumors from experimental tumor-bearing mice that were treated with
intravenous transplantation of 1×106 NK cells. The
results in Fig. 4F indicate a
significantly higher degree of NK cell infiltration in xenograft
tumors from the NK cell-treated group compared with the level in
the control treatment group. These results suggest that NK cells
induced the infiltration of lymphocytes in the tumors of
experimental mice, which suggests that in vivo treatment of
supplementation with NK cells has positive effects against ovarian
xenograft tumors.
Discussion
Currently, various strategies and medications for
the treatment of human ovarian cancer have been studied and
developed (30). Immunotherapy, as a
main therapy or adjunctive, is an efficient treatment and serves an
essential role in the modern healthcare system worldwide (31). The effects of immunotherapy represent
a targeted treatment by activating the host immune cells stimulated
by homologous cancer cells of ovarian tumors (32). The present study investigated
immunotherapy of NK cells from patients with ovarian cancer in
xenograft BALB/c nude mice. The experimental design demonstrated
that NK cell treatment inhibited tumor growth and prolonged the
survival of mice with ovarian cancer. The cytotoxic activities of
these NK cells killed ovarian cancer cells through inducing
apoptosis, inhibiting proliferation and suppressing migration and
invasion of ovarian tumor cells.
Immunotherapy has been demonstrated to alleviate
gene therapy- and chemoradiotherapy-related side effects, enhance
therapeutic effects of surgery and prolong the survival of patients
with ovarian cancer (33). From
previous reports, it has been concluded that the functions of the
immune system are essential for eradication of ovarian malignant
cells in cancer treatment of humans and animals (34–36).
Failure of the immune cells to monitor tumor cells may lead to the
emergence and development of cancer (37,38).
Additionally, previous studies have elaborated on the various
mechanisms used by tumor cells to escape from immune-mediated
cytotoxicity (39–41). The most important of these escape
factors was the lack of recognition of tumor antigens (42).
The present study investigated the effects of NK
cell immunotherapy on inhibiting the growth of ovarian cancer
cells, the survival rate and conditions of long-term survival in
mice with ovarian cancer. The therapeutic effect on mouse survival
was evaluated by analysis of immunotherapy of NK cells in
vivo. Although a previous study has reported that NK cells
inhibited systemic metastasis of glioblastoma cells and exhibited
therapeutic effects against glioblastomas in the brain (24), to the best of our knowledge, no study
has previously reported the therapeutic effects of NK cells for
ovarian cancer. The present study demonstrated that NK cells from
patients with ovarian cancer not only inhibited ovarian tumor cell
growth, but also suppressed tumor cell migration and invasion.
To date, previous reports have clearly indicated
that cellular immunity of NK cells may either provide strong
antitumor effects or cure cancer patients in the advanced stage
(43,44). In the present study, peripheral blood
from patients with ovarian cancer was extracted and lymphocytes
were sensitized by tumor cells from the patients themselves, which
improved clinical protocols and inhibited immune escape and
tumor-induced immune suppression, with little or no side effects.
The present results showed that release of the T cell cytokine
IFN-γ and CD69 expression were upregulated after NK cell treatment
by intravenous injection. These data are similar to a previous
report involving prescriptions of intravenous injection of immune
cells for patients with ovarian cancer (45).
Notably, increasing levels of CD4, CD8, NK1.1 and
IFN-γ release were observed in the present study in the NK cell
treatment group. Expression of immune factors in plasma are
biomarkers that are important mediators of CTLs following
immune-related anticancer treatments, which contribute to the
immunological memory of cancer patients (46,47).
Changes in levels of various immune factors in the blood of mice
suggested that the immune system was enhanced by the immunotherapy
treatment at the indicated dose used in the present experiment. The
present study also demonstrated that antitumor activities of
immunotherapy significantly inhibited metastatic tumor cells.
Notably, tumor shrinkage was observed in the majority of
tumor-bearing mice treated with NK cells.
In conclusion, the beneficial outcomes of
immunotherapy with NK cells on the inhibition of tumor growth and
increasing the survival rate were observed following NK cell
treatment in an 18-day period. The present data suggested that
immunotherapy using NK cells is an effective treatment for mice
with ovarian cancer and indicated that higher expression of immune
factors contributed to long-term survival of mice with ovarian
cancer. The present results indicate that the clinical relevance of
immunotherapy for patients with cancer requires further development
in prospective larger-scale investigations.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YS perfomed most of the experiments. ZY, ZZ, HX, XM
and ZX performed some experiments and analyzed the data. JX and CS
designed the study. All authors have read and approved this
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Weifang City People's Hospital (Weifang, China).
Written informed consent was obtained from the single patient for
use of their cells.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Korkmaz T, Seber S and Basaran G: Review
of the current role of targeted therapies as maintenance therapies
in first and second line treatment of epithelial ovarian cancer; In
the light of completed trials. Crit Rev Oncol Hematol. 98:180–188.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ebell MH, Culp MB and Radke TJ: A
systematic review of symptoms for the diagnosis of ovarian cancer.
Am J Prev Med. 50:384–394. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Raavé R, de Vries RB, Massuger LF, van
Kuppevelt TH and Daamen WF: Drug delivery systems for ovarian
cancer treatment: A systematic review and meta-analysis of animal
studies. PeerJ. 3:e14892015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Watts S, Prescott P, Mason J, McLeod N and
Lewith G: Depression and anxiety in ovarian cancer: A systematic
review and meta-analysis of prevalence rates. BMJ Open.
5:e0076182015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Davis LL and Carpenter JS: A systematic
review of nonpharmacologic interventions for treatment-related
symptoms in women with ovarian cancer. Clin J Oncol Nurs.
19:535–542. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huo YR, Richards A, Liauw W and Morris DL:
Hyperthermic intraperitoneal chemotherapy (HIPEC) and cytoreductive
surgery (CRS) in ovarian cancer: A systematic review and
meta-analysis. Eur J Surg Oncol. 41:1578–1589. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Garziera M, Montico M, Bidoli E, Scalone
S, Sorio R, Giorda G, Lucia E and Toffoli G: Prognostic role of
serum antibody immunity to p53 oncogenic protein in ovarian cancer:
A systematic review and a meta-analysis. PLoS One. 10:e01403512015.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bacalbașa N and Bălescu I: Total pelvic
exenteration for pelvic recurrence after advanced epithelial
ovarian cancer-A case report and literature review. J Med Life.
8:263–265. 2015.PubMed/NCBI
|
|
9
|
Sarafraz-Yazdi E, Gorelick C, Wagreich AR,
Salame G, Angert M, Gartman CH, Gupta V, Bowne WB, Lee YC, Abulafia
O, et al: Ex vivo efficacy of anti-cancer drug PNC-27 in the
treatment of patient-derived epithelial ovarian cancer. Ann Clin
Lab Sci. 45:650–658. 2015.PubMed/NCBI
|
|
10
|
Lin JJ, Egorova N, Franco R, Prasad-Hayes
M and Bickell NA: Ovarian cancer treatment and survival trends
among women older than 65 years of age in the United States,
1995–2008. Obstet Gynecol. 127:81–89. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Duda K, Cholewa H, Łabuzek K,
Boratyn-Nowicka A and Okopień B: Novel strategies of ovarian cancer
treatment. Pol Merkur Lekarski. 39:337–342. 2015.(In Polish).
PubMed/NCBI
|
|
12
|
Kobayashi M, Chiba A, Izawa H, Yanagida E,
Okamoto M, Shimodaira S, Yonemitsu Y, Shibamoto Y, Suzuki N and
Nagaya M: DC-vaccine study group at the Japan Society of Innovative
Cell Therapy (J-SICT): The feasibility and clinical effects of
dendritic cell-based immunotherapy targeting synthesized peptides
for recurrent ovarian cancer. J Ovarian Res. 7:482014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sundar S, Neal RD and Kehoe S: Diagnosis
of ovarian cancer. BMJ. 351:h44432015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Barrett CL, DeBoever C, Jepsen K, Saenz
CC, Carson DA and Frazer KA: Systematic transcriptome analysis
reveals tumor-specific isoforms for ovarian cancer diagnosis and
therapy. Proc Natl Acad Sci USA. 112:E3050–E3057. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wands JR: Prevention of hepatocellular
carcinoma. N Engl J Med. 351:1567–1570. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bronte G, Cicero G, Sortino G, Pernice G,
Catarella MT, D'Alia P, Cusenza S, Lo Dico S, Bronte E, Sprini D,
et al: Immunotherapy for recurrent ovarian cancer: A further piece
of the puzzle or a striking strategy? Expert Opin Biol Ther.
14:103–114. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tse BW, Collins A, Oehler MK, Zippelius A
and Heinzelmann-Schwarz VA: Antibody-based immunotherapy for
ovarian cancer: Where are we at? Ann Oncol. 25:322–331. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fauci JM, Sabbatino F, Wang Y,
Londoño-Joshi AI, Straughn JM Jr, Landen CN, Ferrone S and
Buchsbaum DJ: Monoclonal antibody-based immunotherapy of ovarian
cancer: Targeting ovarian cancer cells with the B7-H3-specific mAb
376.96. Gynecol Oncol. 132:203–210. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lage A: Immunotherapy and complexity:
Overcoming barriers to control of advanced cancer. MEDICC Rev.
16:65–72. 2014.PubMed/NCBI
|
|
20
|
Massarelli E, Papadimitrakopoulou V, Welsh
J, Tang C and Tsao AS: Immunotherapy in lung cancer. Transl Lung
Cancer Res. 3:53–63. 2014.PubMed/NCBI
|
|
21
|
‘Immunotherapy of metastatic breast cancer
patients with vitamin D-binding protein-derived macrophage
activating factor (GcMAF)’ by Yamamoto N, Suyama H, Yamamoto N and
Ushijima N. Int J Cancer. 135:15092014.PubMed/NCBI
|
|
22
|
Matsuda G, Imadome K, Kawano F, Mochizuki
M, Ochiai N, Morio T, Shimizu N and Fujiwara S: Cellular
immunotherapy with ex vivo expanded cord blood T cells in a
humanized mouse model of EBV-associated lymphoproliferative
disease. Immunotherapy. 7:335–341. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pan QZ, Tang Y, Wang QJ, Li YQ, Zhang L,
Li XD, Zhao JJ, Weng DS, Liu Q, Huang LX, et al: Adjuvant cellular
immunotherapy in patients with resected primary non-small cell lung
cancer. Oncoimmunology. 4:e10380172015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lee SJ, Kang WY, Yoon Y, Jin JY, Song HJ,
Her JH, Kang SM, Hwang YK, Kang KJ, Joo KM and Nam DH: Natural
killer (NK) cells inhibit systemic metastasis of glioblastoma cells
and have therapeutic effects against glioblastomas in the brain.
BMC Cancer. 15:10112015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Greaves MF and Brown G: Purification of
human T and B lymphocytes. J Immunol. 112:420–423. 1974.PubMed/NCBI
|
|
26
|
Zamarin D, Vigil A, Kelly K, García-Sastre
A and Fong Y: Genetically engineered Newcastle disease virus for
malignant melanoma therapy. Gene Ther. 16:796–804. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Latifi A, Luwor RB, Bilandzic M,
Nazaretian S, Stenvers K, Pyman J, Zhu H, Thompson EW, Quinn MA,
Findlay JK and Ahmed N: Isolation and characterization of tumor
cells from the ascites of ovarian cancer patients: Molecular
phenotype of chemoresistant ovarian tumors. PLoS One. 7:e468582012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Nikolic B, Cooke DT, Zhao G and Sykes M:
Both gamma delta T cells and NK cells inhibit the engraftment of
xenogeneic rat bone marrow cells and the induction of xenograft
tolerance in mice. J Immunol. 166:1398–1404. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Angell TE, Lechner MG, Jang JK, LoPresti
JS and Epstein AL: MHC class I loss is a frequent mechanism of
immune escape in papillary thyroid cancer that is reversed by
interferon and selumetinib treatment in vitro. Clin Cancer Res.
20:6034–6044. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
De Felice F, Marchetti C, Palaia I, Musio
D, Muzii L, Tombolini V and Panici PB: Immunotherapy of ovarian
cancer: The role of checkpoint inhibitors. J Immunol Res.
2015:1918322015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Schwab CL, English DP, Roque DM, Pasternak
M and Santin AD: Past, present and future targets for immunotherapy
in ovarian cancer. Immunotherapy. 6:1279–1293. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kersual N, Garambois V, Chardès T, Pouget
JP, Salhi I, Bascoul-Mollevi C, Bibeau F, Busson M, Vié H,
Clémenceau B, et al: The human Müllerian inhibiting substance type
II receptor as immunotherapy target for ovarian cancer. Validation
using the mAb 12G4. MAbs. 6:1314–1326. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Recchia F, Candeloro G, Rosselli M, Bratta
M, Pasta V, D'Orazi V, Fumagalli LA and Rea S: Adjuvant ovarian
suppression, high-dose chemotherapy and immunotherapy for
premenopausal patients with high-risk breast cancer. Anticancer
Res. 35:6847–6853. 2015.PubMed/NCBI
|
|
34
|
Krishnan V, Berek JS and Dorigo O:
Immunotherapy in ovarian cancer. Curr Probl Cancer. 41:48–63. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Malecki M, Putzer E, Quach C, Dodivenaka C
and Tombokan X: Novel paradigm for immunotherapy of ovarian cancer
by engaging prophylactic immunity against hepatitis B virus. Clin
Transl Med. 5:442016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Khalil HS, Langdon SP, Goltsov A, Soininen
T, Harrison DJ, Bown J and Deeni YY: A novel mechanism of action of
HER2 targeted immunotherapy is explained by inhibition of NRF2
function in ovarian cancer cells. Oncotarget. 7:75874–75901. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Saoji V, Lade NR, Gadegone R and Bhat A:
Immunotherapy using purified protein derivative in the treatment of
warts: An open uncontrolled trial. Indian J Dermatol Venereol
Leprol. 82:42–46. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Dhami S, Nurmatov U, Halken S, Calderón
MA, Muraro A, Roberts G, Toit GD, Kleine-Tebbe J, Larenas-Linnemann
D, Lau S, et al: Allergen immunotherapy for the prevention of
allergic disease: Protocol for a systematic review. Pediatr Allergy
Immunol. 27:236–241. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pawelec G: Immunotherapy and
immunoselection-tumour escape as the final hurdle. FEBS Lett.
567:63–66. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chouaib S: Tumor escape from the immune
response: A major hurdle for successful immunotherapy of cancer?
Tunis Med. 83 Suppl 12:S7–S10. 2005.
|
|
41
|
Plate JM and Fidler MJ: Immunotherapy to
overcome lung tumor cell-induced escape from immunosurveillance.
Immunotherapy. 2:757–760. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Bremers AJ, Andreola S, Leo E, Gallino F,
Rini F, Lombardo C, Belli F, Kuppen PJ, Parmiani G and Castelli C:
T cell responses in colorectal cancer patients: Evidence for class
II HLA-restricted recognition of shared tumor-associated antigens.
Int J Cancer. 88:956–961. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Malmberg KJ: Effective immunotherapy
against cancer: A question of overcoming immune suppression and
immune escape? Cancer Immunol Immunother. 53:879–892. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Tjin EP, Krebbers G, Meijlink KJ, van de
Kasteele W, Rosenberg EH, Sanders J, Nederlof PM, van de Wiel BA,
Haanen JB, Melief CJ, et al: Immune-escape markers in relation to
clinical outcome of advanced melanoma patients following
immunotherapy. Cancer Immunol Res. 2:538–546. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Sutoh M, Kasuya E, Yayou KI, Ohtani F and
Kobayashi Y: Intravenous tryptophan administration attenuates
cortisol secretion induced by intracerebroventricular injection of
noradrenaline. Anim Sci J. 87:266–270. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Sun L, Guo H, Jiang R, Lu L, Liu T and He
X: Engineered cytotoxic T lymphocytes with AFP-specific TCR gene
for adoptive immunotherapy in hepatocellular carcinoma. Tumour
Biol. 37:799–806. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Dong T: CD8+ cytotoxic T lymphocytes in
human influenza virus infection. Natl Sci Rev. 2:264–265. 2015.
View Article : Google Scholar : PubMed/NCBI
|