Introduction
Conservative treatment for anterior cruciate (ACL)
ligament has modest efficacy. A study (1) suggested that 95% of the patients who
had adopted long-term conservative treatment had to receive
meniscectomy after 20 years while 52% of these patients, at the
average age of 53 only, had to receive total knee arthroplasty
(TKA) after 30 years; moreover, because conservative treatment may
further affect the stability of lateral knee joint, in most cases,
surgery is recommended. In the USA, there are >100,000 patients
receiving ACL reconstruction every year (2,3).
Presently, arthroscopic ACL reconstruction techniques mainly
include: transtibial (TT), anteromedial portal (AMP) or transportal
(TP) and outside-in (OI) techniques. The TT technique means
drilling a tibial tunnel to create a femoral tunnel in ACL
reconstruction while the AMP and the OI techniques require an
additional incision on the anteromedial or OI aspect of the femur
to create a solitary femoral tunnel. Similar to other literature
(4), the AMP and the OI techniques
are collectively referred to as the independent drilling (ID)
techniques in this report. Plenty of studies showed that femoral
tunnels could not be precisely placed in the natural ACL anatomic
insertion by using the standard transtibial (sTT) technique
(5,6), which, as a result, caused abnormal
rotation of knee joints (7,8) and failed to reduce the occurrence of
knee osteoarthritis (KOA). At present, the sTT technique has been
basically abandoned by surgeons. In contrast, the ID techniques are
efficient in the placement of femoral tunnel in the natural ACL
insertion for anatomic reconstruction. Since the ID techniques have
overcome the deficiencies of the sTT technique, it has become a
trend to employ the ID techniques in ACL reconstruction (9–11).
However, in recent years, a new technique has been introduced to
the field, the modified transtibial (mTT) technique. The mTT
technique is not only as efficacious as the ID techniques in
respect of anatomic reconstruction (4,12,13), but
requires fewer incisions compared to the latter. Moreover, most
surgeons in the field of sports medicine have grasped the TT
technique and thus they are likely to acknowledge the mTT
technique. Is the mTT technique or the ID techniques better for ACL
reconstruction? This report gives a meta-analysis of the latest
studies on the sTT, ID and mTT techniques, which evaluated these
techniques by comparing their clinical data and provided a
theoretical basis for surgeons to select the optimal surgical
methods.
Data collection methods
Search strategy and study
selection
We conducted online searches of PubMed (1982 to
April 2017), Cochrane (4th issue, 2017) and Embase (1982 to June
2017), the following words were selected to perform the search task
in the PubMed, Embase and Cochrane databases by means of medical
subject headings and text-word searching: ‘anterior cruciate
ligament’ and (‘transtibial’ or ‘modified transtibial’ or
‘anteromedial portal’ or ‘outside-in’ or ‘independent drilling’).
Titles and abstracts of the retrieved articles were assessed to
exclude the ineligible ones from the meta-analysis. Further
inclusion and exclusion was carried out by means of full-text
assessment for eligibility.
The inclusion criteria are as follows: i) clinical
studies on comparison between the TT (or mTT) and the ID techniques
for ACL reconstruction; ⅱ) single-bundle ACL reconstruction; ⅲ)
patients suffering from ACL fracture without any other ligament
injuries; ⅳ) complete reports on postoperative kinematic and
clinical evaluation results; and ⅴ) prospective clinical studies
(level of evidence: level I and II).
The exclusion criteria are as follows: i) studies on
comparison between the TT technique and other drilling methods, or
between the sTT and the mTT techniques or the TP and the OI
techniques; ⅱ) studies on double-bundle ACL reconstruction; ⅲ) ACL
accompanied by posterior cruciate ligament (PCL), medial collateral
ligament (MCL) or lateral collateral ligament (LCL) injuries; ⅳ)
absence of reports on postoperative clinical outcomes or failure in
acquiring necessary data; and ⅴ) retrospective clinical studies or
those with lower levels of evidence (level III or IV or below).
These criteria were also applied to the references
of each article included in this study for screening to prevent
careless omission.
Data extraction and analysis
The data extracted from the included articles were:
first author, year of publication, research type, level of
evidence, average age of patients, sample size, follow-up duration,
occurrence of meniscus injury, International Knee Documentation
Committee (IKDC) subjective/objective score, laxity of knee joint,
Lachman test, pivot-shift test, Lysholm score and Tegner activity
scale. When having any questions about an article, the authors of
this report tried to reach and communicate with the correspondence
author(s) of the article.
Since the TT groups of the included articles either
referred to the sTT or the mTT technique, in this study, they were
divided into the sTT and the mTT subgroups for comparison with the
ID techniques.
RevMan 5.3 software was employed to perform data
analysis. The standardized mean differences (SMDs) of continuous
variables were used as analytical results while the random effects
model with 95% confidence intervals (CIs) was applied to the
analysis; on the other hand, the odds ratios (ORs) of dichotomous
variables were adopted to present analytical results and similarly,
the random effects model with 95% CI was applied to the analysis.
I2 was used to assess heterogeneity. If I2
<50%, there was low heterogeneity. P<0.05 suggested a
significant difference in analytical results. In some studies
(14–17), continuous variables were expressed by
medians and numerical ranges. The method put forward by Hozo et
al (18) in 2005 was employed to
estimate means and variances; some used means and P-values to
report continuous variables. In this study, the methods provided in
the Cochrane Handbook for Systematic Reviews of Interventions were
adopted as variance estimators.
Results
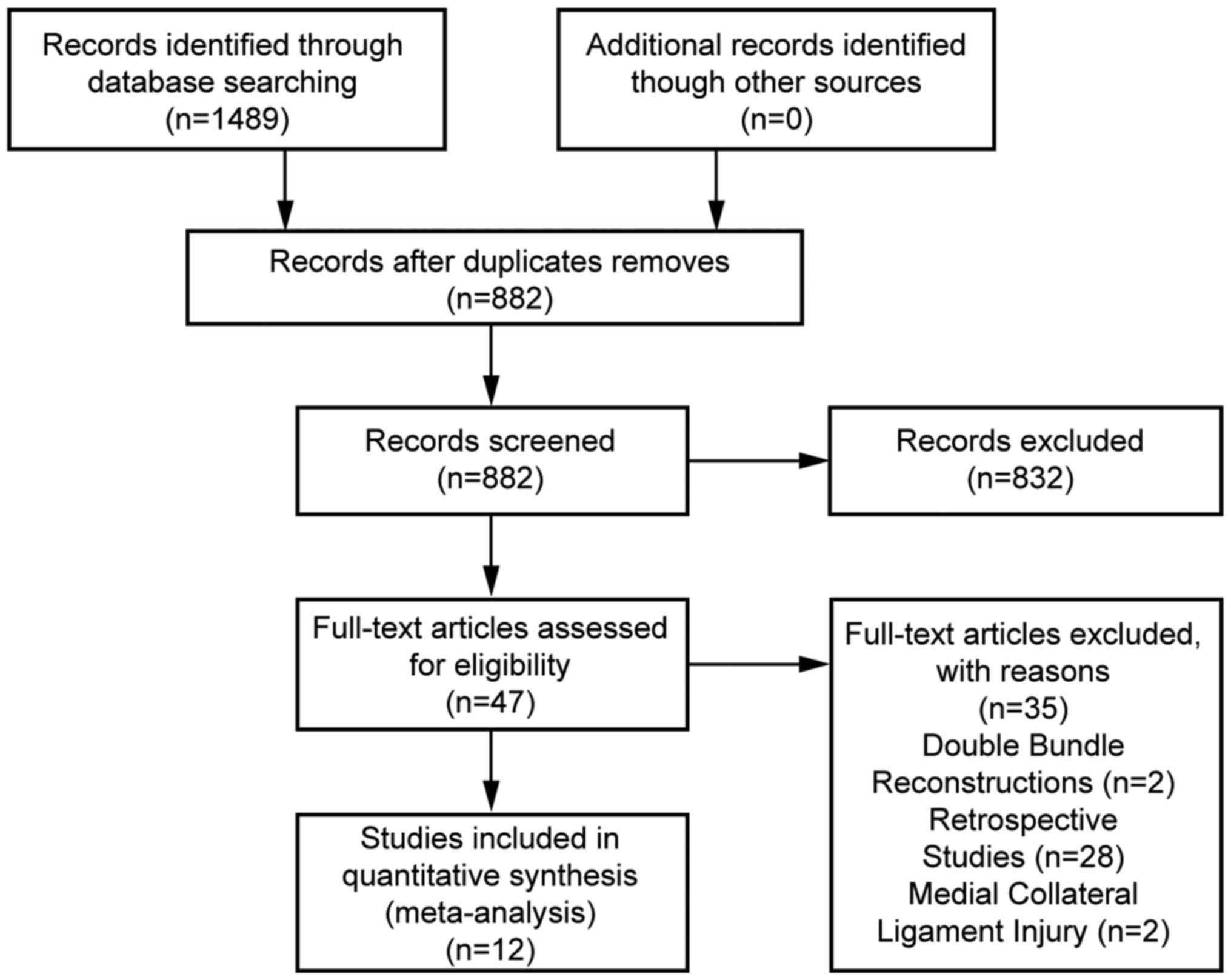
Identification process
With the above-mentioned key words, 689 articles
were retrieved from the PubMed database while 721 were retrieved
from the Embase database and 79 were from the Cochrane database.
After removing duplicates, there remained 882 records in total. The
authors of this report selected 50 articles eligible for the
meta-analysis after going through the titles and abstracts of all
records. Subsequently, a full-text assessment for eligibility of
these 50 articles was performed and 12 studies (Fig. 1) involving 681 patients were included
in the meta-analysis according to the foregoing inclusion and
exclusion criteria. The first authors, years of publication,
research types, levels of evidence, sample sizes, follow-up
durations, occurrence of meniscus injury and the involved drilling
techniques for comparison of these 12 articles are shown in
Table I.
 | Table I.Basic information of included
studies. |
Table I.
Basic information of included
studies.
| Author | Year | Experimental
design | Level of
evidence | Age in years mean
(range) | Sample size | Meniscus
injury | Follow-up duration
(months) | Techniques for
comparison |
|---|
| Matassi et
al (21) | 2015 |
| II | 31
(18–48) | 40 | – | 12 | TT/OI |
| Lanzetti et
al (14) | 2017 |
| II | 25.71±3.02 | 44 | + | >24 | TT/OI |
| Sohn et al
(15) | 2014 |
| II | 29.3 (15–51) | 60 | – | 15.7 | mTT/AMP/OI |
| Zhang et al
(25) | 2012 | RCT | I | 28
(17–48) | 76 | – | >12 | TT/AMP |
| Noh et al
(16) | 2013 |
| I | 23
(18–45) | 61 | – | 30.2 | TT/AMP |
| Musahl (17) | 2015 |
| II | 29 | 40 | – | 24 | mTT/AMP |
| Youm et al
(23) | 2014 |
| I | 28.7±10.9 | 40 | + | 24 | mTT/AMP |
| Hussein et
al (20) | 2012 | RCT | I | 33.4 (16–63) | 150 | – | 51.15 | TT/AMP/AMP(DB) |
| Bohn et al
(19) | 2015 | RCT | I | 25.9±6.3 | 23 | – | 13 | TT/AMP |
| Koutras et
al (26) | 2013 |
| II | 23.9 | 51 | – | 6 | TT/AMP |
| Xu et al
(24) | 2012 |
| II | 32.0±4.8 | 65 | – | 16 | TT/AMP |
| Yanasse et
al (22) | 2016 |
| II | 18–45 | 31 | – | 13 | TT/OI |
Measurements meta-analysis
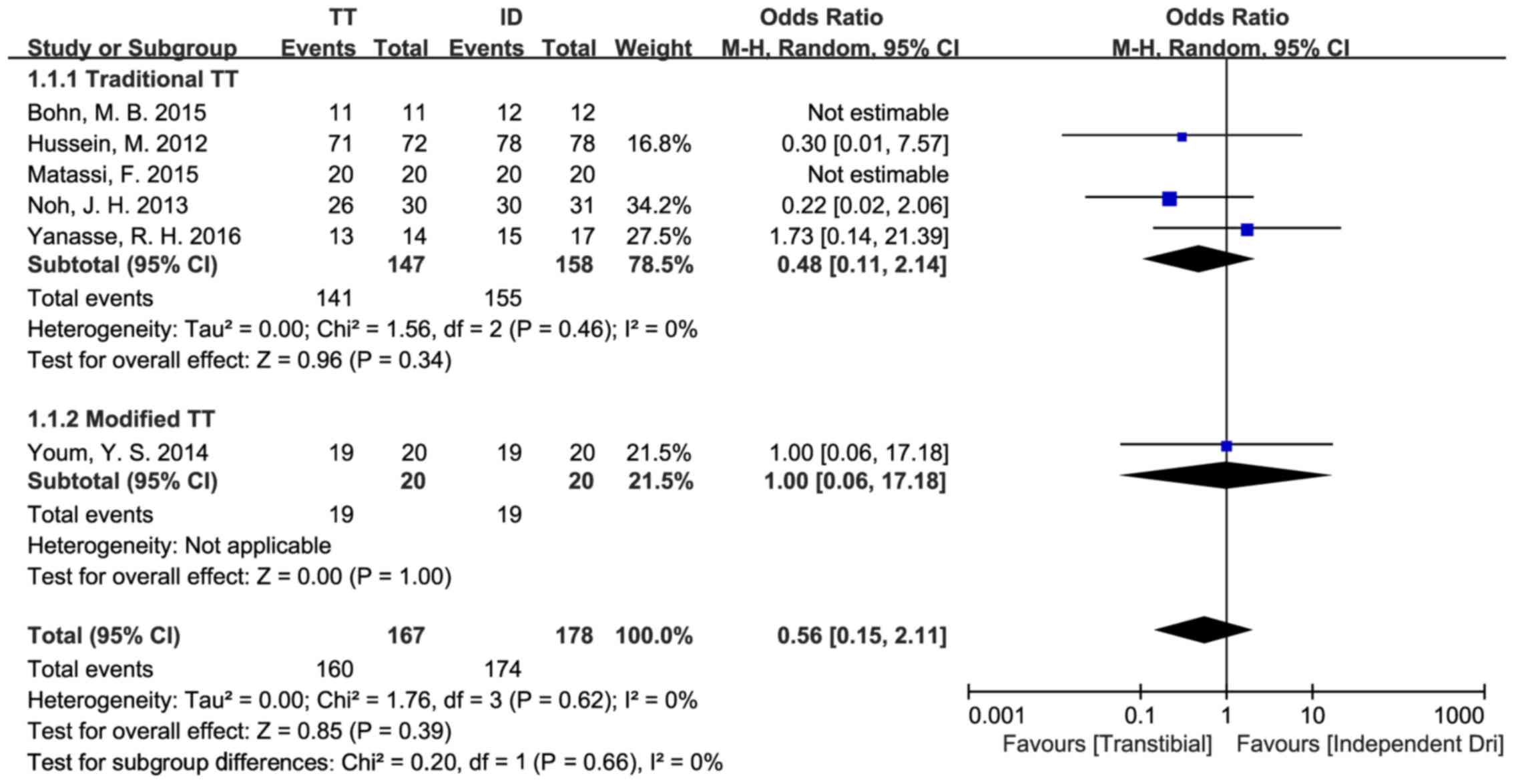
The IKDC objective score was analyzed as a
dichotomous variable (16,19–22) and
the OR value was defined as ‘(number of patients rated A and
B)/(number of patients rated C and D)’. There were 305 patients in
five studies included in the comparison between the sTT and the ID
techniques. Through analysis, there were no statistically
significant differences in the IKDC objective scores of the sTT and
the ID group [OR=0.48, 95% CI (0.11, 2.14), P=0.34]. The data
showed low heterogeneity (P=0.46, I2=0%). In addition,
based on the comparison of the IKDC objective scores between the
mTT and the ID techniques, a study (sample size, 38) indicated no
statistical differences between the two types of techniques in this
respect [OR=1.00, 95% CI (0.06, 17.18), P=1.00] (23) (Fig.
2).
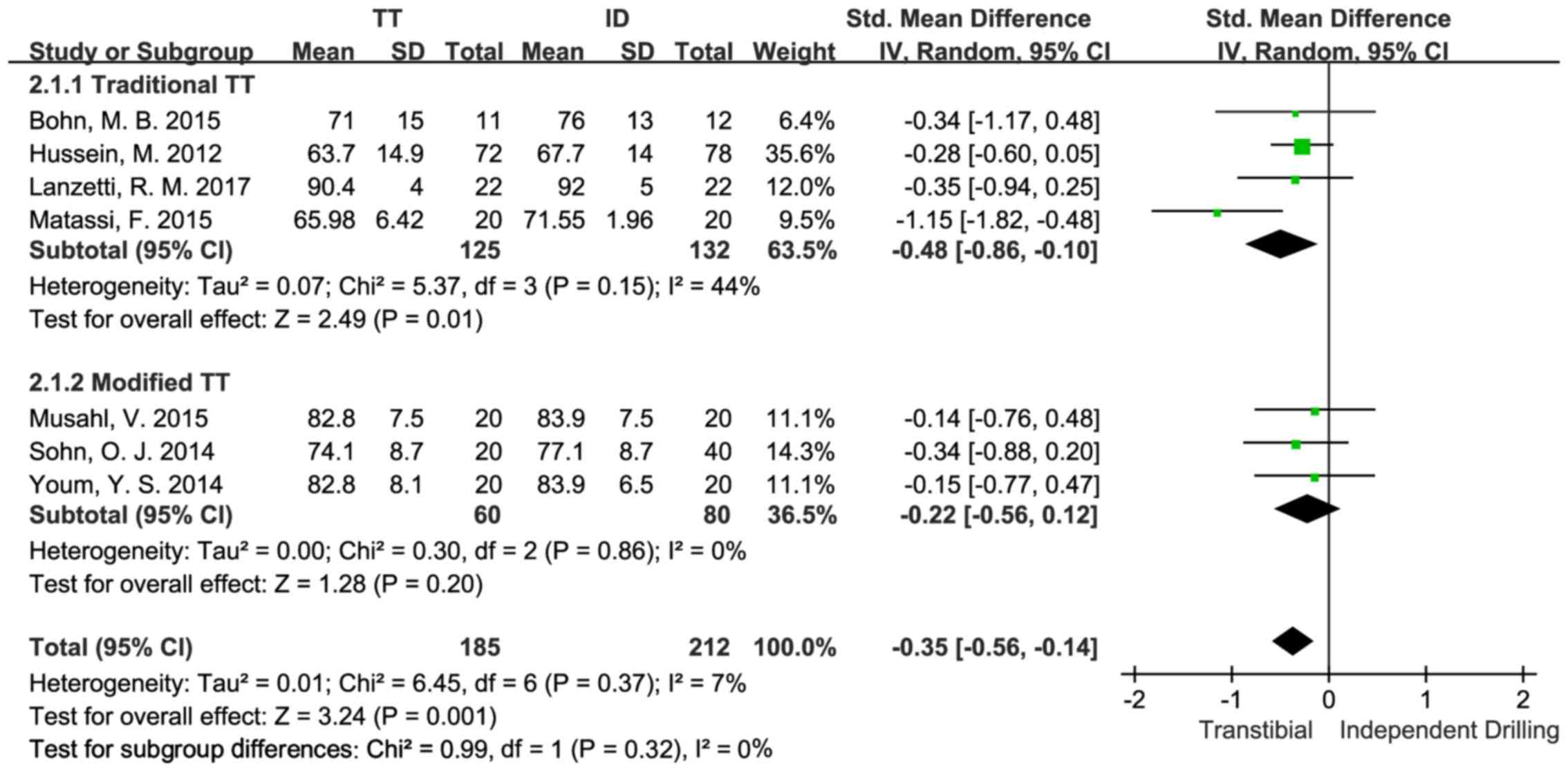
An analysis on the IKDC subjective score as a
continuous variable was performed (14,19–21).
There were 257 patients in four studies included in the comparison
between the sTT and the ID techniques. The study results suggested
statistically significant differences between the sTT group and
that of the ID group in their IKDC subjective scores [SMD=−0.48,
95% CI (−0.86,-0.10), P=0.01], with the ID group having a higher
score. The data showed moderate heterogeneity (P=0.15,
I2=44%). Besides, there were 140 patients in three
studies (15,17,23)
included in the comparison between the mTT and the ID techniques.
According to the study results, there were no statistically
significant differences in the IKDC subjective scores of the mTT
and the ID group [SMD=−0.22, 95% CI (−0.56,0.12), P=0.20]. The data
showed no heterogeneity (P=0.86, I2=0%) (Fig. 3).
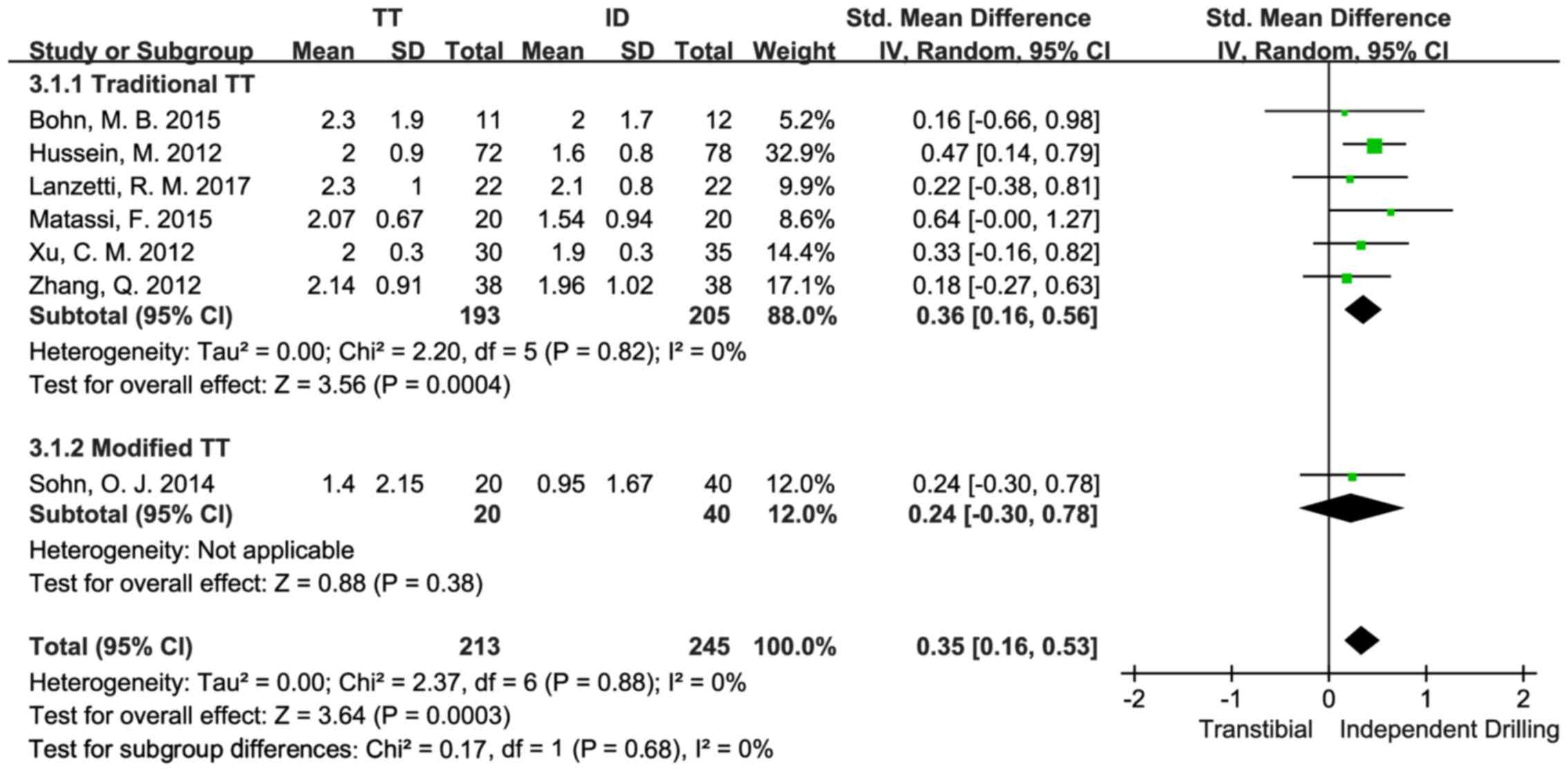
The difference in the anterior displacement of the
tibia between bilateral knee joints was employed to assess the
difference in anterior displacement of the tibia between the
operated and the intact knees (14,19–21,24,25). In
four studies, the KT-1000 knee arthrometer was adopted while the
KT-2000 knee arthrometer was applied to another two studies. The
difference in bilateral knee joints was analyzed as a continuous
variable. There were 398 patients in six studies included in the
comparison between the sTT and the ID techniques. The study results
indicated statistically significant differences between the sTT and
the ID groups in D-value in anterior displacement of the tibia
between the operated and the intact knees [SMD=0.36, 95% CI
(0.16,0.56), P=0.0004], with the ID group having a smaller D-value.
The data showed low heterogeneity (P=0.82, I2=0%).
Besides, there was a study (sample size, 60) comparing the mean
difference in the anterior displacement of the tibia between the
operated and the intact knees of the mTT and ID groups (15). From the study results, no statistical
differences in this respect between the sTT and the ID techniques
were found [OR=0.24, 95% CI (−0.30, 0.78), P=0.38] (Fig. 4).
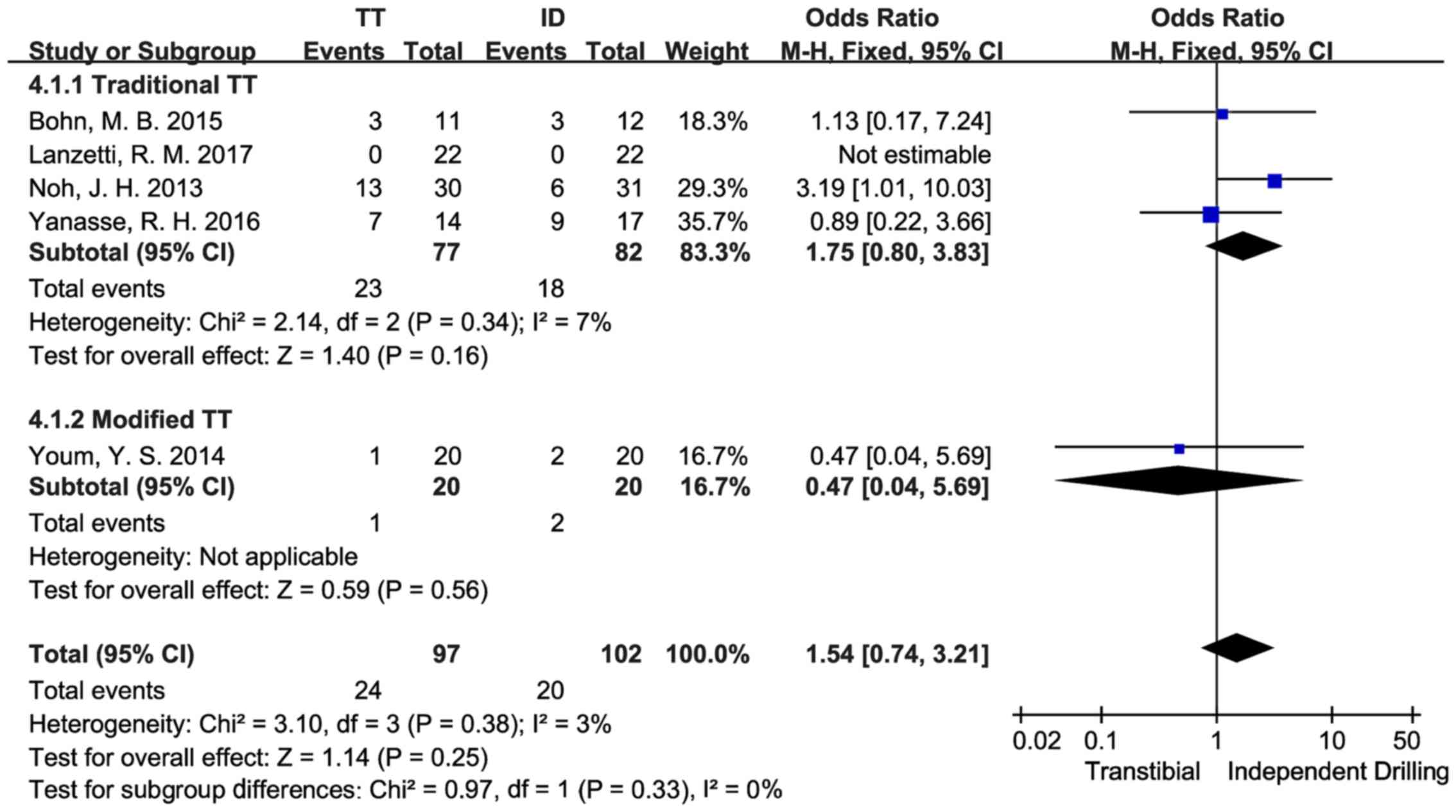
An analysis on the Lachman test results as
dichotomous variables was conducted (14,16,19,22) and
the OR value was defined as ‘(number of patients with positive test
results)/(number of patients with negative test results)’. There
were 159 patients in four studies included in the comparison
between the sTT and the ID techniques. Through analysis, there were
no statistically significant differences in the Lachman test
results between the sTT and the ID group [OR=1.72, 95% CI (0.74,
3.97), P=0.21]. The data showed low heterogeneity (P=0.34,
I2=7%). There was also a study (sample size, 40)
comparing the Lachman test results of the mTT and the ID techniques
(23), according to which, no
statistical difference between the mTT and the ID techniques was
found in Lachman test [OR=0.47, 95% CI (0.04, 5.69), P=0.56]
(Fig. 5).
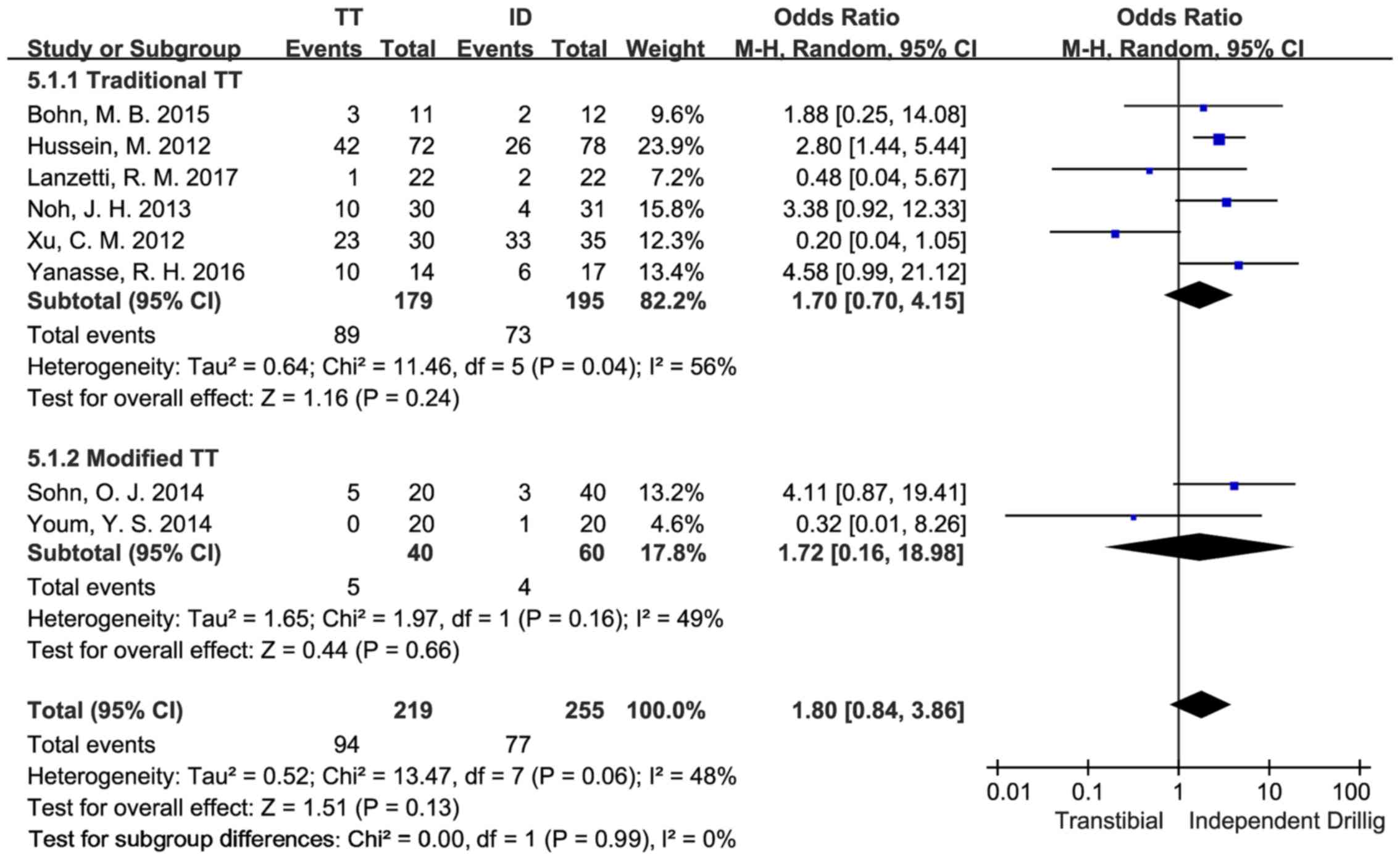
The pivot-shift test results were analyzed as
dichotomous variables (14,16,19,14)
and the OR value was defined as ‘(number of patients with positive
test results/number of patients with negative test results)’. There
were 364 patients in six studies included in the comparison between
the sTT and the ID techniques. According to the study results, no
statistically significant differences were found in the pivot-shift
test results between the sTT group and the ID group [OR=1.70, 95%
CI (0.70, 4.15), P=0.24]. The data showed moderate heterogeneity
(P=0.04, I2=56%). There were 100 patients in two studies
(15,23) included in the comparison between the
mTT and the ID techniques. The results showed no statistically
significant differences in the pivot-shift test results between the
mTT and the ID group [OR=1.72, 95% CI (0.16, 18.98), P=0.66]. The
data showed moderate heterogeneity (P=0.16, I2=49%)
(Fig. 6).
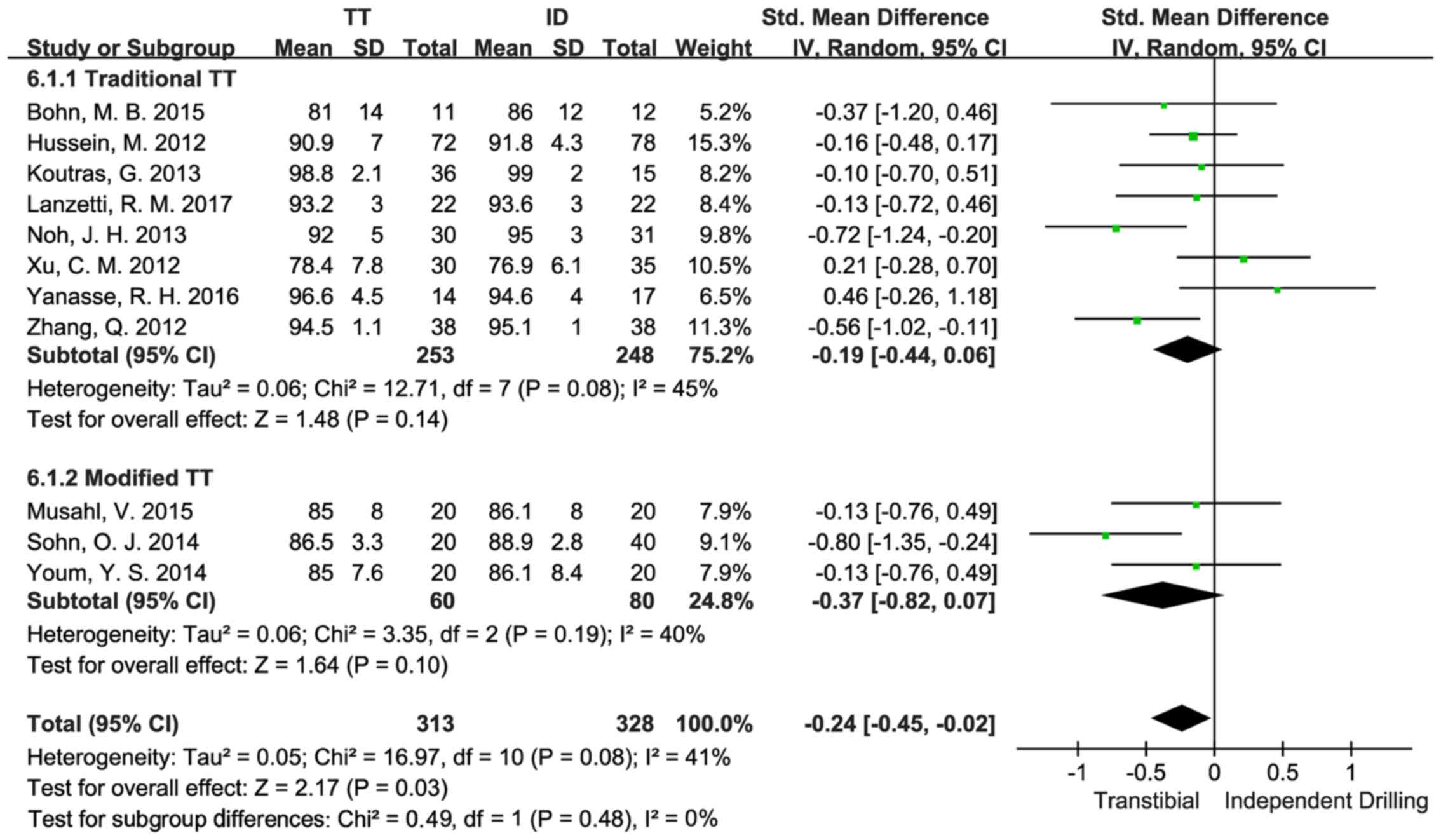
The Lysholm knee score was analyzed as a continuous
variable (14,16,19,14)
in eight articles where a total number of 501 patients were
included in the comparison between the sTT and the ID techniques.
The results indicated no statistically significant differences in
Lysholm knee score between the sTT and the ID group [SMD=−0.19, 95%
CI (−0.44, 0.06), P=0.14]. The data showed a certain degree of
heterogeneity within the tolerance interval (P=0.08,
I2=45%). In addition, there were 140 patients in three
studies (15,17,23),
included in the comparison between the mTT and the ID techniques.
The results suggested that there was no statistically significant
difference in Lysholm knee score between the mTT and the ID group
[SMD=−0.37, 95% CI (−0.82, 0.07), P=0.10] with the data showing
moderate heterogeneity (P=0.19, I2=40%) (Fig. 7).
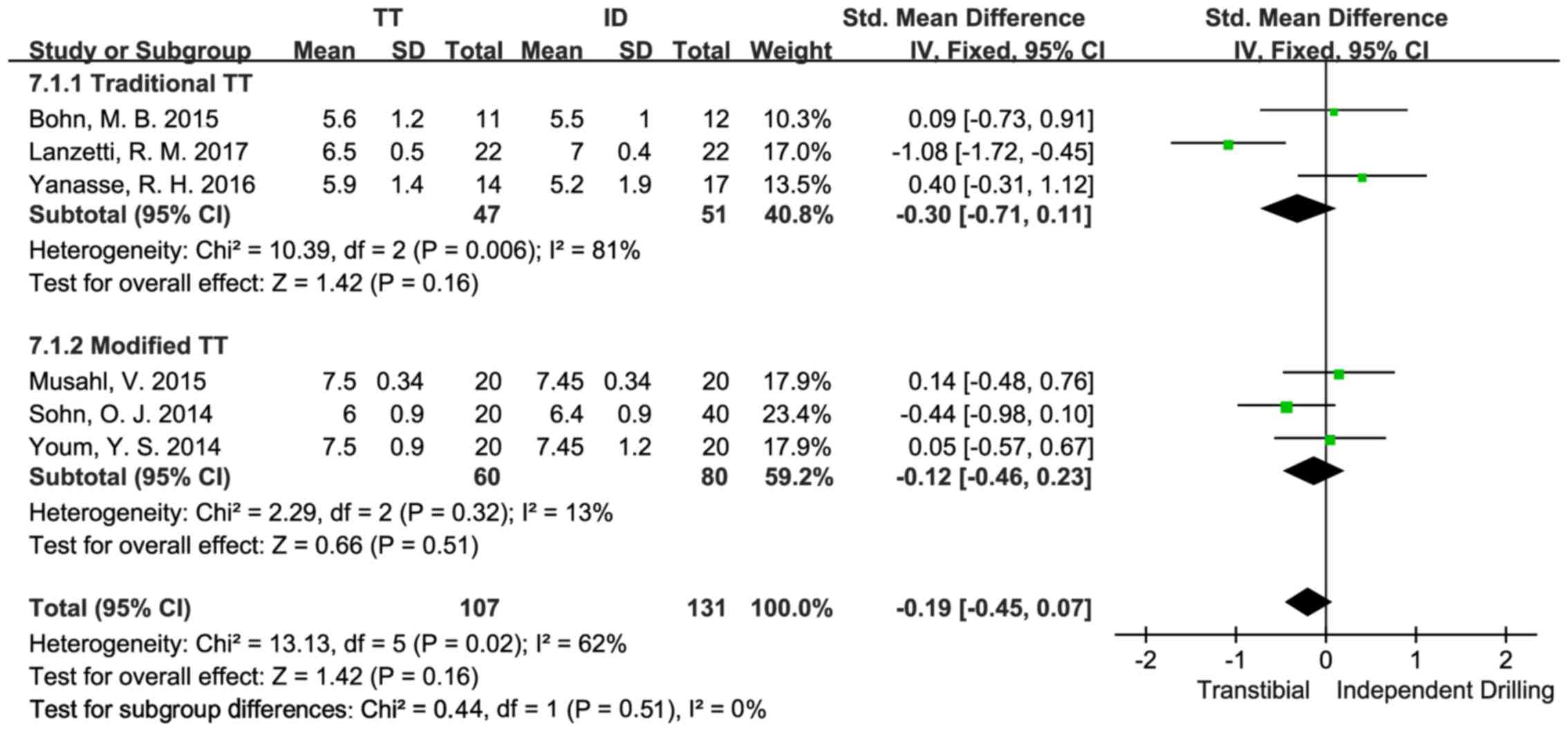
The Tegner activity scale was analyzed as a
continuous variable (14,19,22), in
three articles where 98 patients were included in the comparison
between the sTT and the ID techniques. According to the study
results, no statistically significant differences were seen in
Tegner activity scale between the sTT and the ID group [SMD=−0.22,
95% CI (−1.16, 0.73), P=0.66]. The data showed high heterogeneity
(P=0.006, I2=81%). Besides, there were 140 patients in
three studies (15,17,23)
included in the comparison between the mTT and the ID techniques.
The results indicated no statistically significant differences in
Tegner activity scale between the mTT and the ID group [SMD=−0.11,
95% CI (−0.48, 0.25), P=0.55], with the data showing low
heterogeneity (P=0.32, I2=13%) (Fig. 8).
Susceptibility analysis
A series of susceptibility analysis was performed to
assess the stability of this meta-analysis. To accurately identify
the reasons for data instability, the susceptibility analysis was
further carried out by selecting the included studies with the
sample sizes >20 cases and randomized controlled trial (RCT),
changing the random effects model into the fixed-effects model and
ruling out singular values. According to the susceptibility
analysis on comparison between the sTT and ID techniques, when the
studies having smaller sample sizes (<20 cases) were excluded,
there were statistically significant differences in Lachman test
between the sTT and the ID groups [OR=3.19, 95% CI (1.01, 10.03),
P=0.05]; if only the studies with RCT were included, the data of
the two groups would show significant statistical differences
[OR=2.39, 95%CI (0.90, 6.35), P=0.08]. In terms of pivot-shift
test, if only the studies with RCT were included, the meta-analysis
results would suggest significant statistical differences, with the
ID group having more negative results [OR=2.81, 95% CI (1.59,
4.96), P=0.0004]; when the random effects model applied to the
meta-analysis was replaced by the fixed-effects model,
statistically significant differences between the data of the two
groups could also be found [OR=2.00, 95% CI (1.25, 3.19),
P=0.004].
In comparison between the sTT and ID techniques,
when the article contributed by Matassi et al (21) was removed from the analysis of IKDC
subjective score, the data heterogeneity significantly dropped
(P=0.97, I2=0%) and significant statistical differences
between the two groups were observed [SMD=−0.30, 95% CI (−0.57,
−0.03), P=0.03]; as to Lachman test, when Yanasse's et al
(22) study was excluded, the
analytical results showed statistically significant differences
between the two groups [OR=2.39, 95% CI (0.90, 6.35), P=0.08], with
the ID group having less positive results and without data
heterogeneity (P=0.35, I2=0%); in terms of pivot-shift
test, the analytical results suggested significant statistical
differences after the article of Xu et al (24) was excluded [OR=2.75, 95% CI (1.64,
4,63), P=0.0001] and meanwhile, the data heterogeneity was
significantly reduced (P=0.63, I2=0%); when the study of
Lanzetti's et al (14) was
excluded from the analysis on Tegner activity scale, there remained
no statistically significant differences between the two groups
[SMD=0.27, 95% CI (−0.27, 0.80), P=0.33] and yet the data
heterogeneity was decreased significantly (P=0.57,
I2=0%) (Table II).
| Table II.Comparison of susceptibility analysis
results between the sTT and the ID techniques. |
Table II.
Comparison of susceptibility analysis
results between the sTT and the ID techniques.
|
| IKDC objective
score | IKDC subjective
score |
|---|
|
|
|
|
|---|
|
| No. of
patients | OR | P-value | No. of
patients | SMD | P-value |
|---|
| Basic analysis | 305 | 0.48 (0.11,
2.14) | 0.34 | 257 | −0.48 (−0.86,
−0.10) | 0.01 |
| n ≥20 | 251 | 0.24 (0.04,
1.53) | 0.13 | 234 | −0.53 (−1.02,
−0.04) | 0.03 |
| RCT | 234 | 0.24 (0.04,
1.53) | 0.13 | 173 | −0.28 (−0.58,
0.02) | 0.06 |
| Fixed-effects
model | 305 | 0.47 (0.12,
1.80) | 0.27 | 257 | −0.41 (−0.66,
−0.16) | 0.001 |
| Singular value
removal | / | / | / | 217 | −0.30 (−0.57,
−0.03) | 0.03 |
|
|
| Knee
laxity | Lachman
test |
|
|
|
|
|
| No. of
patients | SMD | P-value | No. of
patients | OR | P-value |
|
| Basic analysis | 398 | 0.36 (0.16,
0.56) | 0.0004 | 159 | 1.72 (0.74,
3.97) | 0.21 |
| n ≥20 | 375 | 0.37 (0.17,
0.58) | 0.0004 | 105 | 3.19 (1.01,
10.03) | 0.05 |
| RCT | 249 | 0.35 (0.10,
0.60) | 0.006 | 84 | 2.39 (0.90,
6.35) | 0.08 |
| Fixed-effects
model | 398 | 0.36 (0.16,
0.56) | 0.0004 | 159 | 1.75 (0.80,
3.83) | 0.16 |
| Singular value
removal | / | / | / | 159 | 1.72 (0.74,
3.97) | 0.21 |
|
|
| Pivot-shift
test | Lysholm knee
score |
|
|
|
|
|
| No. of
patients | OR | P-value | No. of
patients | SMD | P-value |
|
| Basic analysis | 374 | 1.70 (0.70,
4.15) | 0.24 | 501 | −0.19 (−0.44,
0.06) | 0.14 |
| n ≥20 | 320 | 1.22 (0.34,
4.36) | 0.76 | 396 | −0.27 (−0.58,
0.04) | 0.09 |
| RCT | 234 | 2.81 (1.59,
4.96) | 0.0004 | 310 | −0.41 (−0.69,
−0.13) | 0.004 |
| Fixed-effects
model | 374 | 2.00 (1.25,
3.19) | 0.004 | 501 | −0.20 (−0.38,
−0.02) | 0.03 |
| Singular value
removal | 309 | 2.75 (1.64,
4.63) | 0.0001 | / | / | / |
|
|
|
| Tegner activity
scale |
|
|
|
|
|
|
| No. of
Patients | SMD | P-value |
|
| Basic analysis |
| 98 |
| −0.22 (−1.16,
0.73) |
| 0.66 |
| n ≥20 |
| / |
| / |
| / |
| RCT |
| / |
| / |
| / |
| Fixed-effects
model |
| 98 |
| −0.30 (−0.71,
0.11) |
| 0.16 |
| Singular value
removal |
| 54 |
| 0.27 (−0.27,
0.80) |
| 0.33 |
In comparison between the mTT and ID techniques,
considering the limited literature, only the susceptibility
analysis that replaced the random effects model with the
fixed-effects model was conducted (Table III). In terms of Lysholm knee
score, there were statistically significant intergroup differences
when the fixed-effects model was applied to the analysis
[SMD=−0.39, 95% CI (−0.03, −0.74), P=−0.03]. The susceptibility
analysis on other items showed no significant changes in the
meta-analysis results (SMDs or ORs) and statistical significance
(P-value). Only the subgroups of a study were not given any
susceptibility analysis.
| Table III.Comparison of susceptibility analysis
results between the mTT and the ID techniques. |
Table III.
Comparison of susceptibility analysis
results between the mTT and the ID techniques.
|
| Fixed-effects
model | P-value |
|---|
| IKDC subjective
score | −0.22 (−0.56,
0.12) | 0.20 |
| Lysholm knee
score | −0.39 (−0.73,
−0.04) | 0.03 |
| Tegner activity
scale | −0.11 (−0.48,
0.25) | 0.55 |
| Pivot-shift
test | 2.24 (0.61,
8.17) | 0.22 |
Discussion
The latest meta-analysis based on the 12 articles
showed that the ID techniques, compared to the sTT technique,
presented a higher IKDC subjective score and a lower degree of
laxity. However, no significant differences were found in the
results of the IKDC objective score, pivot-shift test and Lachman
test; the comparison of the above-mentioned indicators between the
mTT and the ID techniques also suggested no significant
differences.
Compared to the sTT group, the ID group had a lower
degree of laxity. The data showed low heterogeneity. Authors of
this report considered it as a result of the non-anatomic site of
the bone tunnel. In contrast, Daniel (27) reported that the differences in
anterior displacement of the tibia between bilateral knees of 95%
of those having intact knee joints remained <3 mm and they held
that the difference in anterior laxity between bilateral knees
>3 mm indicated ACL injuries. In this study, the difference in
anterior laxity between bilateral knees was <3 mm and yet, it
still represented postoperative differences between the two
surgical methods. A majority of studies (28–30)
indicated that the sTT technique, as non-anatomic reconstruction
showing weak anti-rotation ability, was likely to cause impingement
of intercondylar fossa and osteoarthritis. The meta-analysis
results were in line with this theory and explained the reasons why
anatomic reconstruction has the advantage over the traditional
isometric reconstruction.
Compared to the sTT group, the ID group had a high
IKDC subjective score, which showed moderate heterogeneity. The
higher IKDC subjective score indicated a higher level of functions
or a lower degree of symptoms, with the emphasis placed on the
assessment of a patient's range of movement and exercise intensity,
instead of the patient's sensations in daily activities, which is
the focus of the Lysholm knee scoring scale. The differences in
IKDC subjective scores may be affected by the recovery level of the
physiological structure. Specifically, it is probably because the
sTT technique cannot facilitate the recovery of the physiological
ligament position that it had a lower IKDC subjective score in the
analysis.
As to the comparison of the pivot-shift test, IKDC
objective scores and Lachman test, no statistical differences in
the ORs were seen between the groups. Moreover, there were few
positive results, which indicated that the patients' ACLs had been
recovered after operations.
The comparison of IKDC subjective scores, Lysholm
knee scores and Tegner activity levels between the mTT and the ID
groups showed no significant differences. The mTT technique was put
forward by Piasecki et al (31) in 2011. According to their study,
anatomic reconstruction could be achieved with the TT technique by
changing the knee joint position. Youm et al (23) and Lee et al (32) had put the theory into practice and
reported that the TT and IDD techniques were much alike in tunnel
characteristics and clinical results. Since the TT technique has
been widely accepted in Asia (33–36), it
requires further analysis to demonstrate the reliability and
benefits of the mTT technique. Therefore, the meta-analysis also
provided the comparison between the mTT and ID techniques in order
to explore whether the mTT technique could present desirable
clinical outcomes. The results suggested that the mTT technique was
comparable to the ID techniques in terms of patients' subjective
sensations, recovery level of motor abilities and daily activities
by comparison of IKDC subjective scores, Lysholm knee scores and
Tegner activity levels between the mTT and the ID groups. However,
considering the limited data size and short follow-up visit, it
still requires massive clinical data to support the conclusion.
In this report, only the single-bundle studies were
analyzed because according to the autopsy studies (37) in southern China, the average length
of tibial insertions was 15.18±2.65 mm only, failing to meet the
indication of double-bundle reconstruction. Generally, patients who
have the tibial insertions <16 mm are recommended to receive
single-bundle anatomic reconstruction (38–40).
Similar to other system evaluations, this study also
has limitations: i) it includes a small number of RCTs and lacks
quality randomized controlled studies; ⅱ) some studies included in
the meta-analysis have modest sample sizes and there is
statistically significant heterogeneity due to the differences in
research design, patient diversity and operation plans; ⅲ) the
studies having relatively short follow-up fail to provide long-term
clinical evidence; ⅳ) there are few studies on comparison between
the mTT and ID techniques written in Chinese, making the
meta-analysis less convincing; and v) the meta-analysis is only a
statistical test subject to numerous methods and thus it cannot
control all relevant factors.
In conclusion, compared to the sTT technique, the
mTT technique, similar to the ID techniques, has a lower level of
laxity and a higher IKDC subjective score. Since the TT technique
is familiar to almost all surgeons, the mTT technique is expected
to gain widespread recognition and become the new reconstruction
standard in the future. Yet, it still requires extensive research
data to support the conclusion.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
ZY was responsible for the conception and design of
the study. QZ and YK were responsible for data collection/entry,
data analysis/statistics, data interpretation and literature
analysis/search. ZY and QZ were responsible for the preparation of
the manuscript. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nebelung W and Wuschech H: Thirty-five
years of follow-up of anterior cruciate ligament-deficient knees in
high-level athletes. Arthroscopy. 21:696–702. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brown CH Jr and Carson EW: Revision
anterior cruciate ligament surgery. Clin Sports Med. 18:109–171.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Harner CD, Giffin JR, Dunteman RC,
Annunziata CC and Friedman MJ: Evaluation and treatment of
recurrent instability after anterior cruciate ligament
reconstruction. Instr Course Lect. 50:463–474. 2001.PubMed/NCBI
|
|
4
|
Riboh JC, Hasselblad V, Godin JA and
Mather RC III: Transtibial versus independent drilling techniques
for anterior cruciate ligament reconstruction: A systematic review,
meta-analysis, and meta-regression. Am J Sports Med. 41:2693–2702.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tompkins M, Milewski MD, Brockmeier SF,
Gaskin CM, Hart JM and Miller MD: Anatomic femoral tunnel drilling
in anterior cruciate ligament reconstruction: Use of an accessory
medial portal versus traditional transtibial drilling. Am J Sports
Med. 40:1313–1321. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Robin BN and Lubowitz JH: Disadvantages
and advantages of transtibial technique for creating the anterior
cruciate ligament femoral socket. J Knee Surg. 27:327–330. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Webster KE, Palazzolo SE, McClelland JA
and Feller JA: Tibial rotation during pivoting in anterior cruciate
ligament reconstructed knees using a single bundle technique. Clin
Biomech (Bristol, Avon). 27:480–484. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang Y, Xu C, Dong S, Shen P, Su W and
Zhao J: Systemic review of anatomic single-versus double-bundle
anterior cruciate ligament reconstruction: Does femoral tunnel
drilling technique matter? Arthroscopy. 32:1887–1904. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Duquin TR, Wind WM, Fineberg MS, Smolinski
RJ and Buyea CM: Current trends in anterior cruciate ligament
reconstruction. J Knee Surg. 22:7–12. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chechik O, Amar E, Khashan M, Lador R,
Eyal G and Gold A: An international survey on anterior cruciate
ligament reconstruction practices. Int Orthop. 37:201–206. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
McRae SM, Chahal J, Leiter JR, Marx RG and
Macdonald PB: Survey study of members of the Canadian Orthopaedic
Association on the natural history and treatment of anterior
cruciate ligament injury. Clin J Sport Med. 21:249–258. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lee SR, Jang HW, Lee DW, Nam SW, Ha JK and
Kim JG: Evaluation of femoral tunnel positioning using
3-dimensional computed tomography and radiographs after single
bundle anterior cruciate ligament reconstruction with modified
transtibial technique. Clin Orthop Surg. 5:188–194. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Haro MS, Riff A and Bach BR Jr: Tips for
successful transtibial anterior cruciate ligament reconstruction. J
Knee Surg. 27:331–342. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lanzetti RM, Lupariello D, De Carli A,
Monaco E, Guzzini M, Fabbri M, Vadalà A and Ferretti A: Can the
outside-in half-tunnel technique reduce femoral tunnel widening in
anterior cruciate ligament reconstruction? A CT study. Eur J Orthop
Surg Traumatol. 27:659–664. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sohn OJ, Lee DC, Park KH and Ahn HS:
Comparison of the modified transtibial technique, anteromedial
portal technique and outside-in technique in ACL reconstruction.
Knee Surg Relat Res. 26:241–248. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Noh JH, Roh YH, Yang BG, Yi SR and Lee SY:
Femoral tunnel position on conventional magnetic resonance imaging
after anterior cruciate ligament reconstruction in young men:
Transtibial technique versus anteromedial portal technique.
Arthroscopy. 29:882–890. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Musahl V: A modified transtibial technique
was similar to an anteromedial portal technique for anterior
cruciate ligament reconstruction. J Bone Joint Surg Am.
97:13732015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hozo SP, Djulbegovic B and Hozo I:
Estimating the mean and variance from the median, range, and the
size of a sample. BMC Med Res Methodol. 5:132005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bohn MB, Sørensen H, Petersen MK, Søballe
K and Lind M: Rotational laxity after anatomical ACL reconstruction
measured by 3-D motion analysis: A prospective randomized clinical
trial comparing anatomic and nonanatomic ACL reconstruction
techniques. Knee Surg Sports Traumatol Arthrosc. 23:3473–3481.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hussein M, van Eck CF, Cretnik A, Dinevski
D and Fu FH: Prospective randomized clinical evaluation of
conventional single-bundle, anatomic single-bundle, and anatomic
double-bundle anterior cruciate ligament reconstruction: 281 cases
with 3- to 5-year follow-up. Am J Sports Med. 40:512–520. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Matassi F, Sirleo L, Carulli C and
Innocenti M: Anatomical anterior cruciate ligament reconstruction:
Transtibial versus outside-in technique: SIGASCOT Best Paper Award
Finalist 2014. Joints. 3:6–14. 2015.PubMed/NCBI
|
|
22
|
Yanasse RH, Lima AA, Antoniassi RS,
Ezzedin DA, Laraya MH and Mizobuchi RR: Transtibial technique
versus two incisions in anterior cruciate ligament reconstruction:
Tunnel positioning, isometricity and functional evaluation. Rev
Bras Ortop. 51:274–281. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Youm YS, Cho SD, Lee SH and Youn CH:
Modified transtibial versus anteromedial portal technique in
anatomic single-bundle anterior cruciate ligament reconstruction:
Comparison of femoral tunnel position and clinical results. Am J
Sports Med. 42:2941–2947. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xu CM, Yang L, Hu YH and Huangfu XQ:
Transplantation of single-bundle four-strand hamstring tendon via
anteromedial approach for anterior cruciate ligament
reconstruction. Chin J Tissue Eng Res. 16:9975–9979. 2012.
|
|
25
|
Zhang Q, Zhang S, Li R, Liu Y and Cao X:
Comparison of two methods of femoral tunnel preparation in
single-bundle anterior cruciate ligament reconstruction: A
prospective randomized study. Acta Cir Bras. 27:572–576. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Koutras G, Papadopoulos P, Terzidis IP,
Gigis I and Pappas E: Short-term functional and clinical outcomes
after ACL reconstruction with hamstrings autograft: Transtibial
versus anteromedial portal technique. Knee Surg Sports Traumatol
Arthrosc. 21:1904–1909. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Daniel DM: Assessing the limits of knee
motion. Am J Sports Med. 19:139–147. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zavras TD, Race A, Bull AM and Amis AA: A
comparative study of ‘isometric’ points for anterior cruciate
ligament graft attachment. Knee Surg Sports Traumatol Arthrosc.
9:28–33. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kilinc BE, Kara A, Oc Y, Celik H, Camur S,
Bilgin E, Erten YT, Sahinkaya T and Eren OT: Transtibial vs
anatomical single bundle technique for anterior cruciate ligament
reconstruction: A Retrospective Cohort Study. Int J Surg. 29:62–69.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Franceschi F, Papalia R, Rizzello G, Del
Buono A, Maffulli N and Denaro V: Anteromedial portal versus
transtibial drilling techniques in anterior cruciate ligament
reconstruction: Any clinical relevance? A retrospective comparative
study. Arthroscopy. 29:1330–1337. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Piasecki DP, Bach BR Jr, Orias Espinoza AA
and Verma NN: Anterior cruciate ligament reconstruction: Can
anatomic femoral placement be achieved with a transtibial
technique? Am J Sports Med. 39:1306–1315. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Lee JK, Lee S, Seong SC and Lee MC:
Anatomic single-bundle ACL reconstruction is possible with use of
the modified transtibial technique: A comparison with the
anteromedial transportal technique. J Bone Joint Surg Am.
96:664–672. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Misonoo G, Kanamori A, Ida H, Miyakawa S
and Ochiai N: Evaluation of tibial rotational stability of
single-bundle vs. anatomical double-bundle anterior cruciate
ligament reconstruction during a high-demand activity - a
quasi-randomized trial. Knee. 19:87–93. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yagi M, Kuroda R, Nagamune K, Yoshiya S
and Kurosaka M: Double-bundle ACL reconstruction can improve
rotational stability. Clin Orthop Relat Res. 454:100–107. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Terabe Y, Harada A, Tokuda H, Okuizumi H,
Nagaya M and Shimokata H: Vitamin D deficiency in elderly women in
nursing homes: Investigation with consideration of decreased
activation function from the kidneys. J Am Geriatr Soc. 60:251–255.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Fujita N, Kuroda R, Matsumoto T, Yamaguchi
M, Yagi M, Matsumoto A, Kubo S, Matsushita T, Hoshino Y, Nishimoto
K, et al: Comparison of the clinical outcome of double-bundle,
anteromedial single-bundle, and posterolateral single-bundle
anterior cruciate ligament reconstruction using hamstring tendon
graft with minimum 2-year follow-up. Arthroscopy. 27:906–913. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Beyaz S, Güler UO, Demir Ş, Yüksel S,
Çınar BM, Özkoç G and Akpınar S: Tunnel widening after
single-versus double-bundle anterior cruciate ligament
reconstruction: A randomized 8-year follow-up study. Arch Orthop
Trauma Surg. 137:1547–1555. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Schreiber VM, van Eck CF and Fu FH:
Anatomic Double-bundle ACL Reconstruction. Sports Med Arthrosc Rev.
18:27–32. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Siebold R: The concept of complete
footprint restoration with guidelines for single- and double-bundle
ACL reconstruction. Knee Surg Sports Traumatol Arthrosc.
19:699–706. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chiba D, Tsuda E, Sasaki S, Liu X and
Ishibashi Y: Anthropometric and skeletal parameters predict
2-strand semitendinosus tendon size in double-bundle anterior
cruciate ligament reconstruction. Orthop J Sports Med.
5:23259671177201482017. View Article : Google Scholar : PubMed/NCBI
|