Introduction
Acute pancreatitis is a commonly seen
gastrointestinal disorder and its incidence is on the increase
worldwide. As a rapidly progressive disease severe acute
pancreatitis (SAP) has a high mortality rate accompanied with a
high incidence of complications, which are life-threatening. Bai
et al (1) reported that the
overall mortality rate of SAP in China and in western countries was
11.8 and 10–40%, respectively (2).
Ultrasound-guided percutaneous drainage (PCD) has become an
important means of treatment of severe pancreatitis, and a large
number of inflammatory mediators, enzymes, and toxic metabolites
can be drained in vitro, thus reducing the stimulation of
retroperitoneal plexus and pancreatic edema, improving pancreatic
microcirculation, thereby promoting intestinal function recovery
(3). The most severe acute
pancreatitis in a short organ failure or with acute abdominal
cavity effusion most likely is repaired by absorption (4). Some scholars believe that the early
treatment of aseptic fluid accumulation may lead to exogenous
infection and aggravate pancreatitis (5). Early PCD combined with early antibiotic
use can reduce the release of inflammatory mediators and the
recovery of infection (6).
There is disagreement on the efficacy and safety of
early PCD in treating severe acute pancreatitis. This study aimed
to compare the efficacy of early PCD in patients with severe acute
pancreatitis combined with acute pancreatic fluid accumulation
using a retrospective approach.
Patients and methods
Patients
A total of 178 patients diagnosed as acute and
severe acute pancreatitis complicated with acute fluid accumulation
in peritoneal cavity admitted from January 2011 to January 2015 to
Chuiyangliu Hospital (Beijing, China) were retrospectively
analyzed. This study was approved by the Ethics Committee of
Chuiyangliu Hospital Affiliated to Tsinghua University. Informed
consent was obtained from all the participants prior to the study.
Based on the treatment, the patients were divided into the
following groups: PCD group and conservative treatment control
group. There were 76 cases in the PCD group, of whom 32 were male
and 44 were female, and 102 cases in the conservative treatment
control group, of whom 48 were male and 54 were female. Inclusion
criteria were: i) age range, 18–75 years; ii) in line with the
diagnosis of severe acute pancreatitis in ‘diagnosis and treatment
of acute pancreatitis guide’ (7);
and iii) SIRS still existed 24 h after admission for fluid
infusion. Exclusion criteria for the study were: i) combined with
severe basal heart and lung disease; ii) combined with coagulation
disorders; and iii) patients had to be treated early by surgery
with abdominal hypertension caused by multiple organ dysfunction.
PCD criteria for the drainage group were: i) occurrence of acute
abdominal fluid accumulation with abdominal pressure
(intraperitoneal pressure >15 mmHg); ii) ultrasound or CT
examination showed a large number of intra-abdominal effusion depth
>5 cm; and iii) fluid amount increased in the continuous reviews
twice, and the fluid growth rate was >2 cm/24 h.
Methods
Patients in the control group underwent conservative
treatment, were given regular fasting, sustained gastrointestinal
decompression, liquid resuscitation, maintance of water and
electrolyte balance, intravenous injection of trypsin inhibitors,
proton pump inhibitors and antibiotics. On the basis of
conservative treatment, patients in the drainage group underwent
PCD treatment on the second day after admission. According to the
ultrasound localization and percutaneous puncture with the aid of
ultrasound after local anesthesia, after the effusion was
withdrawn, the guide wire was implanted with PTCD catheter along
the guide wire, making sure that catheter implantation was well
placed under ultrasound, the guide wire was pulled out, and the
extracts were sent for routine examination, lipase and bacterial
culture examination. Infections were defined as positive bacterial
cultures of peritoneal drainage or abdominal CT suggestive of an
abdominal infection. Extubation standard was: i) Drainage per day
<10 ml, imaging examination results showed disappearance of
liquid dark area; and ii) intraperitoneal infection was excluded
according to the drainage fluid before extubation fluid. Bowel
sounds recovery time, time-period of SIRS, dietary recovery time,
defecation ventilation time, time-period of abdominal pain,
hospitalization days, and laboratory indicators (white blood cell
count, blood amylase, blood lipase, C-reactive protein and serum
calcium) were assessed. In the follow-up for 2 years, complications
of severe acute pancreatitis were observed.
Statistical analysis
SPSS 12.0 software (BM Corp., Armonk, NY, USA) was
used for statistical analysis. The measurement data between the two
groups were expressed as mean ± standard deviation (±SD). The
Student's t-test was used and categorical data were analyzed by the
Chi-square test. P<0.05 indicated a significant difference.
Results
General results
The present study enrolled 178 patients diagnosed as
severe acute pancreatitis complicated with acute pancreatic fluid
accumulation during the period 2011–2015 in the Department of
Gastroenterology. The PCD drainage group comprised 76 patients, of
whom 32 were male and 44 were female, with a mean age of 44.0±3.4
years. A total of 102 patients were in the control group, of whom
41 were male and 61 were female, with a mean age of 45.5±3.3 years.
General information of patients in the two groups were comparable
(P>0.05) as shown in Table I.
 | Table I.Patient characteristics. |
Table I.
Patient characteristics.
| Characteristics | PCD | Control |
|---|
| Patient, no. | 76 | 102 |
| Mean ± standard
deviation age (years) | 44.0±3.4 | 45.5±3.3 |
| Sex, male/female | 32/44 | 41/61 |
| Cause of acute
pancreatitis |
| Bile duct
diseases | 53 | 68 |
| Alcohol | 15 | 25 |
| Hyperlipidemia | 8 | 7 |
| Infection | 0 | 2 |
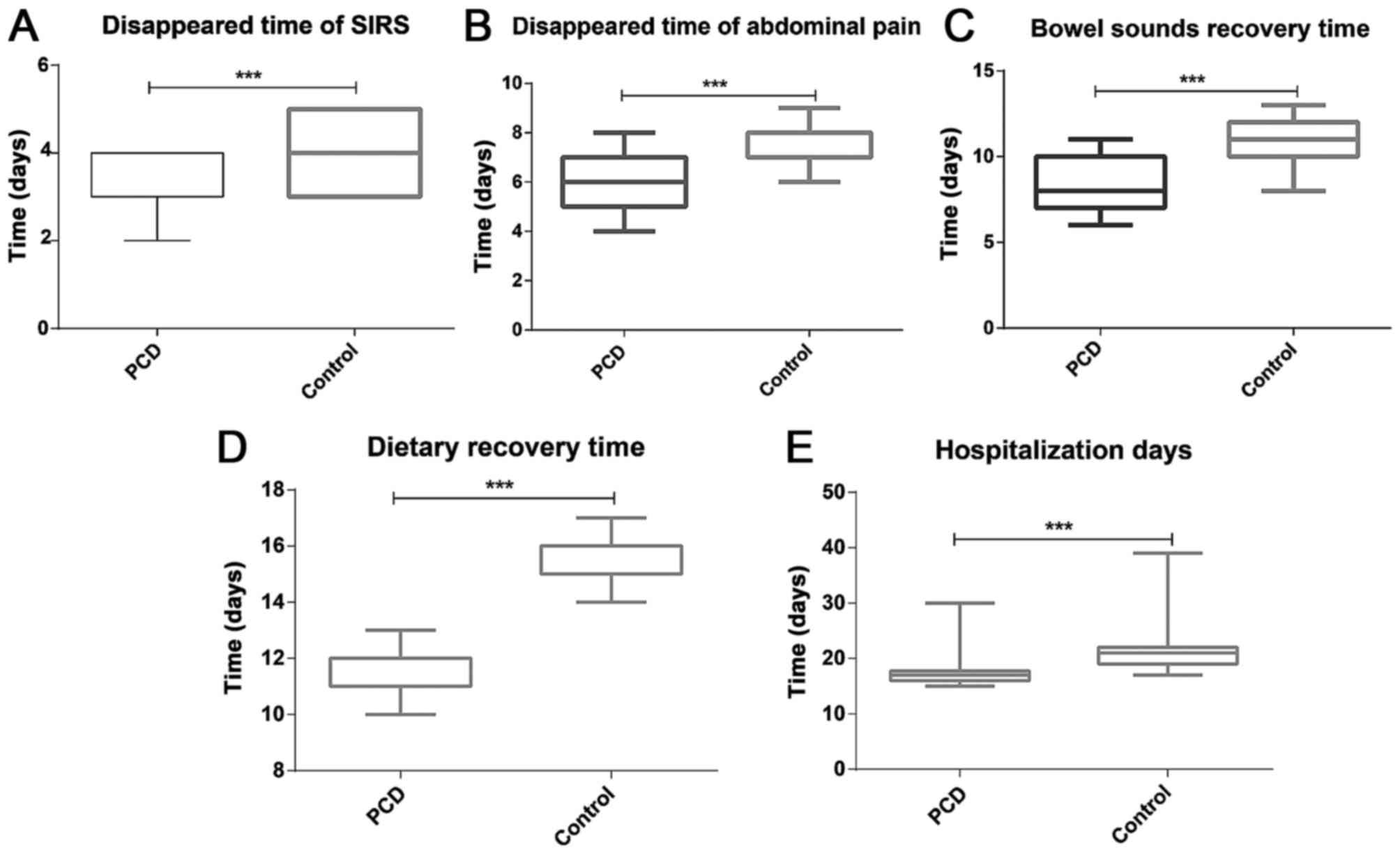
Clinical efficacy results
The time-period of SIRS, time-period of abdominal
pain, bowel sounds recovery time, dietary recovery time, and
hospitalization days were shorter in the PCD group than those in
the control group (P=0.001) (Table
II and Fig. 1).
| Table II.Results of clinical efficacy. |
Table II.
Results of clinical efficacy.
| Variable | Time-period of SIRS
(days) | Time-period of
abdominal pain (days) | Bowel sounds recovery
time (days) | Dietary recovery time
(days) | Hospitalization time
(days) |
|---|
| Treatment | 3.16±0.71 | 5.89±1.25 | 8.37±1.56 | 11.59±0.93 | 17.41±3.24 |
| Control | 3.99±0.74 | 7.31±0.95 | 10.74±1.43 | 15.43±0.87 | 21.23±3.65 |
| P-value | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 |
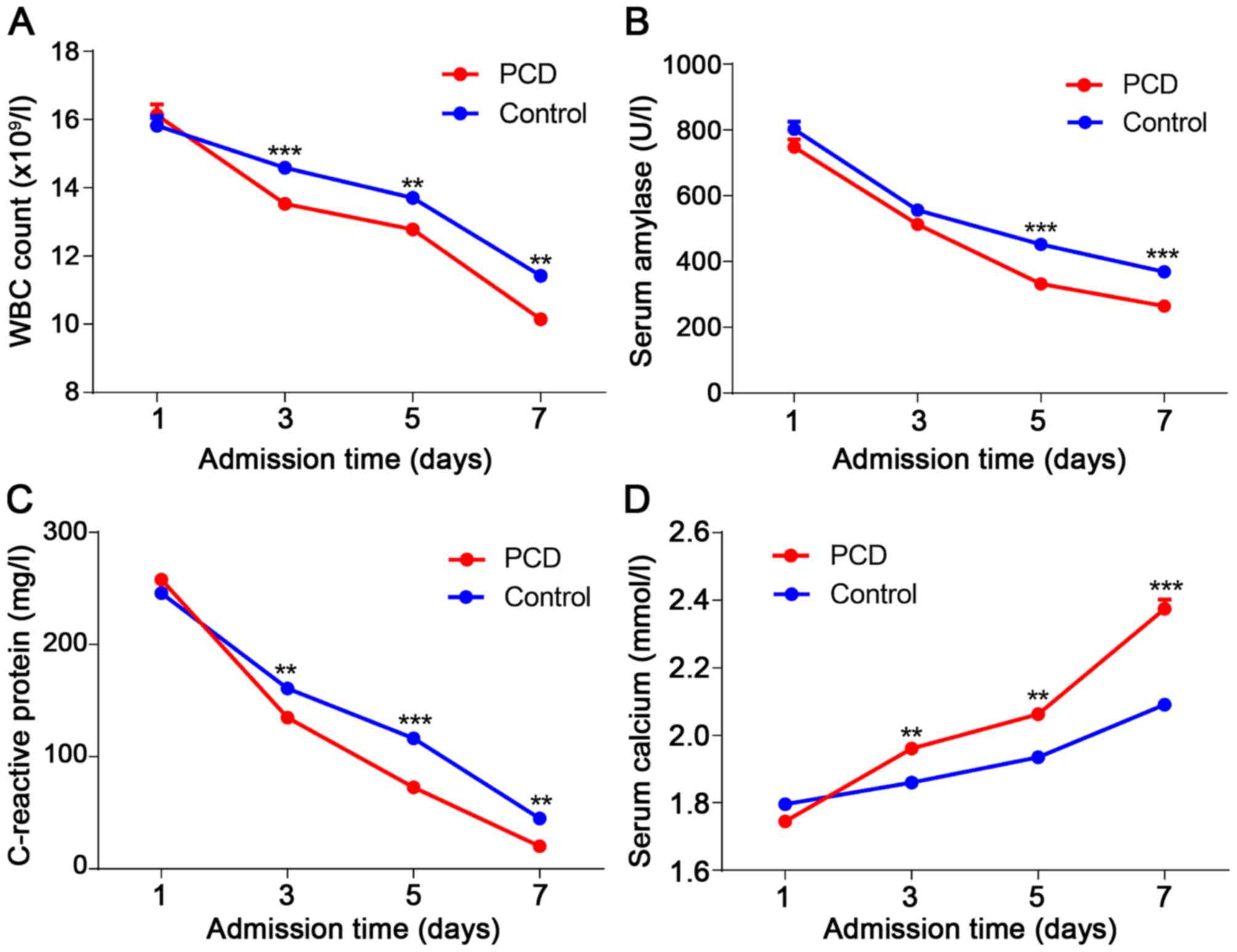
Laboratory indicators
Improvements of white blood cell count (WBC count),
serum amylase, C-reactive protein (CRP), and serum calcium were
better than those of the control group (P<0.001) (Fig. 2).
Clinical outcomes
There were 76 patients in the PCD group and 73 were
successfully treated. Three patients who underwent external
drainage or surgical treatment were transferred to surgical
departments. One patient succumbed to multiple organ failure. Of
the total 102 patients in the control group, 89 patients underwent
conservative treatment of the disease and were significantly
improved, 13 were surgically treated, and 3 succumbed to multiple
organ failure. The surgical rates in the PCD and control groups
were 7.9 and 12.8%, respectively (P=0.042). The mortality rate in
the PCD and control groups was 1.3 and 2.9%, respectively
(P>0.05). The cure rate of the PCD and control group was 98.6
and 97.1%, respectively (P>0.05) (data not shown).
Adverse events and complications
In this study, 1 case had bleeding in the PCD group,
while in 5 cases drainage tube obstruction occurred, and the 5
cases achieved recanalization through the guide wire. No drainage
tube slippage and intra-abdominal infection occurred. Pancreatitis
complications in this study included pancreatic pseudocyst,
pancreatic abscess and multiple organ failure. Among them, there
were 5 cases of pancreatic abscess in the PCD group, 1 of multiple
organ failure that was transferred for surgical treatment, and 8 of
pancreatic pseudocysts. However, in the control group, there were 8
cases of pancreatic abscess, 5 of multiple organ failure and they
were transferred for surgical treatment. Pancreatic pseudocysts
occurred in 12 cases. No significant differences in adverse events
and complications were found between the two groups (P>0.05).
Early PCD treatment showed no effect of reducing the incidence of
pancreatitis. No significant difference in the incidence of
pancreatic pseudocysts was found between the two groups, indicating
that early PCD did not increase the probability of pancreatic
pseudocysts (Table III).
| Table III.Outcome of adverse events and
complications. |
Table III.
Outcome of adverse events and
complications.
|
| Bleeding | Tube obstruction | Intra-abdominal
infection | Pancreatic
abscess | Pancreatic
pseudocysts | Multiple organ
failure |
|---|
| PCD | 1 | 5 | 0 | 8 | 5 | 1 |
| Control | 0 | 0 | 0 | 12 | 8 | 5 |
Discussion
As reported, percutaneous catheter drainage (PCD)
was a minimally invasive intervention for severe acute pancreatitis
(SAP) (8). Since PCD was first
introduced by Freeny et al (9), it has been used as a definitive
treatment in approximately one-third of patients with infected
necrosis. The 2012 Atlanta Amendment proposed a viable PCD for
acute necrotic deposits of more than 5 cm in patients diagnosed as
severe acute pancreatitis. Therefore, it lays a theoretical basis
for acute fluid accumulation in early PCD drainage, however, a
large number of clinical studies are still lacking (10).
In theory, in the case of acute pancreatic fluid
actively engaged in any kind of invasive procedure, the bacteria
outside of the body could enter the third interval through the
iatrogenic operation, which could increase the risk of retrograde
infection. However, there are also the opposite hypotheses. Some
studies have reported that drainage treatment of acute aseptic
fluid accumulation does not increase the risk of infection
complications of pancreatitis (11,12). In
a study of 32 patients with severe pancreatitis, the average time
for the recovery of CRP level in the operating group was 43.8 days
compared with the PCD group (23.8 days), which was significantly
increased (P=0.034). Therefore, it is considered that PCD is more
conducive to the control of inflammatory response and infection
(6). Studies on the early PCD
drainage of acute pancreatic fluid accumulation to improve the
clinical efficacy of acute pancreatitis are few, this retrospective
study was carried out based on this need.
Time-period of systemic inflammatory response
(SIRS), time-period of abdominal pain, bowel sounds recovery time,
dietary recovery time and hospitalization days were shorter in the
PCD group than those in the control group (P=0.001), suggested that
early PCD can more significantly improve the condition of patients
with severe acute pancreatitis than conservative treatment. In a
comparison of laboratory indicators, white blood cell count, serum
amylase, C-reactive protein and serum calcium in the PCD group were
all better than those of the control group (P<0.001), which
indicated that the early PCD treatment could improve the laboratory
indicators and decrease inflammatory response. Therefore, early PCD
treatment can improve the symptoms of patients, which has a certain
effect on diagnosis and treatment of severe acute pancreatitis. The
CRP level predicts the severity of acute pancreatitis (13). In a study of 30 SAP patients treated
with PCD, 19 were completely cured. The PCD CRP levels were 172.8
and 102.5 mg/l after PCD (P<0.05). Therefore, PCD can reduce
inflammation and reduce the risk of infection (14). In this study, the decrease of CRP in
drainage group was significantly better than the control group,
suggesting that PCD group achieved a better prognosis than the
control group.
At present, there are still controversies on PCD
treatment for these patients in clinic. Theoretically, any kind of
invasive operation on acute pancreatic fluid accumulation may
increase the risk of retrograde infection. In a control study of 40
patients, 4 (4/20) cases of infection were reported in the
conservative group, 11 cases (11/20) infection in the peritoneal
drainage group, and one death, so drainage group increased the risk
of infection by 35% (15). However,
some studies have reported that draining treatment of aseptic fluid
accumulation in acute pancreatitis did not increase the risk of
pancreatitis infection complications (11,12). In
this study, the PCD group was first performed drainage after
puncture and before extubation for bacteria culture, among them, 5
cases had pancreatic abscess, while there was no significant
differences in the abscess incidence between the control group and
PCD group, indicating that the early PCD did not increase the
probability of intra-abdominal infection. In this study, 1 patient
died in the PCD group and 3 in the control group; the difference
was not statistically significant. Therefore, the early PCD
treatment did not increase the mortality of severe acute
pancreatitis.
In the present study, the cure rate and mortality in
the PCD and control groups were similar, although the cure rate and
mortality in the PCD group were better, statistical difference was
lacking, suggesting that early PCD did not significantly improve
the patient's final outcome of the disease (P>0.05). The rate of
surgical transfer in the PCD group was significantly lower than
that of the control group (P<0.05), suggesting that early PCD
can ease further deterioration of the severity of acute
pancreatitis and reduce the probability of surgery, which was an
alternative medical treatment.
For adverse events and complications of
pancreatitis, 1 case occurred bleeding in the PCD group and 5 had
occlusion, they were all properly treated. In the complication of
pancreatitis-related outcomes, there was no significant difference
in the incidence of complications comparing the two groups. Early
PCD treatment showed no effect of reducing the incidence of
complications. Considering the small sample size, this study failed
to reflect the effect.
In summary, early PCD treatment of patients with
severe acute pancreatitis combined with acute pancreatic fluid
accumulation can effectively improve the symptoms and prevent
further deterioration of the disease. However, early PCD would not
increase the probability of intra-abdominal infection. Therefore,
our results showed that the early PCD treatment of severe acute
pancreatitis combined with acute pancreatic fluid accumulation was
safe and effective. Some of the limitations of this study are
noteworthy, first, it was a retrospective, single-center study;
second, the sample size was limited. To further investigate the
efficacy and safety of early acute pancreatitis in patients
combined with acute pancreatitis, prospective studies containing
large samples are required.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HL and YW designed the study. CX and HA collected
the patient data. CG and HC analyzed the patient data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Chuiyangliu Hospital Affiliated to Tsinghua University (Beijing,
China). Informed consent was obtained from all the participants
prior to the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bai Y, Liu Y, Jia L, Jiang H, Ji M, Lv N,
Huang K, Zou X, Li Y, Tang C, et al: Severe acute pancreatitis in
China: Etiology and mortality in 1976 patients. Pancreas.
35:232–237. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Raraty MG, Connor S, Criddle DN, Sutton R
and Neoptolemos JP: Acute pancreatitis and organ failure:
Pathophysiology, natural history, and management strategies. Curr
Gastroenterol Rep. 6:99–103. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zerem E, Imamovic G, Omerović S and
Imširović B: Randomized controlled trial on sterile fluid
collections management in acute pancreatitis: Should they be
removed? Surg Endosc. 23:2770–2777. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vege SS, Gardner TB, Chari ST, Munukuti P,
Pearson RK, Clain JE, Petersen BT, Baron TH, Farnell MB and Sarr
MG: Low mortality and high morbidity in severe acute pancreatitis
without organ failure: A case for revising the Atlanta
classification to include ‘moderately severe acute pancreatitis’.
Am J Gastroenterol. 104:710–715. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Babu RY, Gupta R, Kang M, Bhasin DK, Rana
SS and Singh R: Predictors of surgery in patients with severe acute
pancreatitis managed by the step-up approach. Ann Surg.
257:737–750. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ai XB, Qian XP, Pan WS, Xu J, Wu LQ, Zhang
WJ and Wang A: Ultrasound-guided percutaneous catheter drainage in
early treatment of severe acute pancreatitis. World J Emerg Med.
1:45–48. 2010.PubMed/NCBI
|
|
7
|
La Greca A, Di Grezia M, Magalini S, Di
Giorgio A, Lodoli C, Di Flumeri G, Cozza V, Pepe G, Foco M, Bossola
M, et al: Comparison of cholecystectomy and percutaneous
cholecystostomy in acute cholecystitis: Results of a retrospective
study. Eur Rev Med Pharmacol Sci. 21:4668–4674. 2017.PubMed/NCBI
|
|
8
|
Mortelé KJ, Girshman J, Szejnfeld D,
Ashley SW, Erturk SM, Banks PA and Silverman SG: CT-guided
percutaneous catheter drainage of acute necrotizing pancreatitis:
Clinical experience and observations in patients with sterile and
infected necrosis. AJR Am J Roentgenol. 192:110–116. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Freeny PC, Hauptmann E, Althaus SJ,
Traverso LW and Sinanan M: Percutaneous CT-guided catheter drainage
of infected acute necrotizing pancreatitis: Techniques and results.
AJR Am J Roentgenol. 170:969–975. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Banks PA, Bollen TL, Dervenis C, Gooszen
HG, Johnson CD, Sarr MG, Tsiotos GG and Vege SS: Acute Pancreatitis
Classification Working Group: Classification of acute pancreatitis
- 2012: Revision of the Atlanta classification and definitions by
international consensus. Gut. 62:102–111. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Walser EM, Nealon WH, Marroquin S, Raza S,
Hernandez JA and Vasek J: Sterile fluid collections in acute
pancreatitis: Catheter drainage versus simple aspiration.
Cardiovasc Intervent Radiol. 29:102–107. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hookey LC, Debroux S, Delhaye M,
Arvanitakis M, Le Moine O and Devière J: Endoscopic drainage of
pancreatic-fluid collections in 116 patients: A comparison of
etiologies, drainage techniques, and outcomes. Gastrointest Endosc.
63:635–643. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Banks PA and Freeman ML: Practice
Parameters Committee of the American College of Gastroenterology:
Practice guidelines in acute pancreatitis. Am J Gastroenterol.
101:2379–2400. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Navalho M, Pires F, Duarte A, Gonçalves A,
Alexandrino P and Távora I: Percutaneous drainage of infected
pancreatic fluid collections in critically ill patients:
Correlation with C-reactive protein values. Clin Imaging.
30:114–119. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zerem E: Reply to: Draining sterile fluid
collections in acute pancreatitis? Primum non nocere! Surg Endosc.
25:979–980. 2011. View Article : Google Scholar : PubMed/NCBI
|