Introduction
The number of elderly patients undergoing surgery
due to hip fracture is increasing both in China and around the
world (1). It is predicted that by
2050, 6.3 million new cases of hip fracture will be diagnosed each
year (2). Hip fracture is common in
the elderly, and is associated with significant morbidity and
mortality (3). The mortality during
hospital stay is 2.3–13.9%, 6-month mortality ranges from 12–23%,
and 1-year mortality is ~37.1% for men and ~26.4% for women
(4). The main reported causes of
mortality following hip fracture are cardiovascular, neurological
and pulmonary (5). Numerous
guidelines and researches recommend that patients with hip fracture
should undergo surgery within 24–48 h and early surgical treatment
can relieve pain, and reduce the incidence of postoperative
complications and mortality (6–9). Despite
remarkable benefits of early surgery following hip fracture on
outcomes and elderly patients exhibit numerous complications. The
most common coexisting diseases include cardiovascular disease
(35%), respiratory disease (14%) and cerebrovascular disease (13%),
and ~70% of patients are classified as American Society of
Anesthesiologists (ASA) stage III or IV (10) in poor health and time to surgery is
prolonged due to direct oral anticoagulants and other factors,
including waiting for routine medical clearance and unavailability
of the operating suite or surgeon (11,12). In
China, very elderly are frequently defined as ≥80 years old
patients, and it has been estimated that the lifetime risk for an
80-year-old man or woman to sustain a hip fracture is 9 and 19%,
respectively (13). A survey has
indicated that very elderly patients with hip fracture in Xuanwu
Hospital, Capital Medical University (Beijing, China) account for
35% of all very elderly patients, which is significantly increased
compared with the numbers reported in Sweden (the percentage of
very elderly patients with hip fracture in Sweden accounts for 9%
for men and 19% for women of very elderly patients) (13). High morbidity and mortality are
expected due to the advanced age and comorbidities of these
patients (14). Preoperative
management serves an important role in decreasing the morbidity and
mortality of patients. Multiple interventions have been employed to
minimize complications and duration of hospitalization including
preoperative analgesia (9,15). Severe pain is frequently observed in
the preoperative period. Preoperative analgesia is administered to
relieve pain and decrease the systemic stress response (16). Systemic analgesia using opioids and
nonsteroidal analgesia may lead to significant adverse effects
particularly in elderly patients due to age-associated
pharmacokinetic and pharmacodynamic alterations (17). Previous studies have demonstrated the
advantages of epidural analgesia by comparing epidural analgesia
with conventional drug analgesia in elderly patients with hip
fractures (18,19). The results of these studies indicated
that epidural analgesia can reduce the incidence of preoperative
cardiovascular events, however, epidural block has an impact on
circulation, and patients with hip fracture receive anticoagulant
therapy immediately following admission, which may lead to epidural
hematoma and other severe consequences (18,19).
Peripheral nerve blockade is a potential substitute for epidural
analgesia (20), which requires
further study. Due to the advantages of fascia iliaca compartment
block, its application in analgesia prior to hip fracture surgery
is increasing, but a number of studies have investigated the effect
of single fascia iliaca compartment block (21,22).
Very elderly patients mostly exhibit one or more comorbidities and,
therefore, the preoperative waiting time may be prolonged. In these
cases continuous fascia iliaca compartment block (CFICB) may be
more advantageous and two studies have indicated that CFICB is
effective in hip fracture analgesia (23,24).
However, whether ultrasound-guided CFICB is more advantageous
compared with traditional analgesic drugs and whether it helps to
reduce the incidence of perioperative complications in very elderly
patients complicated with cardiovascular, neurological or pulmonary
disease have not yet been reported. It is hypothesized that fascia
iliaca blocks by means of continuous catheters may greatly reduce
the morbidity in patients with hip fracture for the evaluation of
the influence and prevalence of resultant side effects from opiate
medications. It is therefore of interest to evaluate the
effectiveness of preoperative analgesia provided by CFICB or
systemic analgesia in very elderly patients with hip fracture. The
aim of the present study was to investigate the effect of
ultrasound-guided CFICB in very elderly patients with hip fracture
complicated with cardiovascular, neurological or pulmonary disease
in the preoperative waiting period.
Patients and methods
Patients
The present study was prospective, randomized and
controlled, and had been registered at www.chictr.org.cn (registration number:
ChiCTR-IPR-15007283). This study was approved by the Ethics
Committee of Xuanwu Hospital of Capital Medical University and all
patients had signed informed consent. Elderly patients admitted to
Xuanwu Hospital, Capital Medical University (Beijing, China) due to
hip fracture from October 2015 to December 2016 were included in
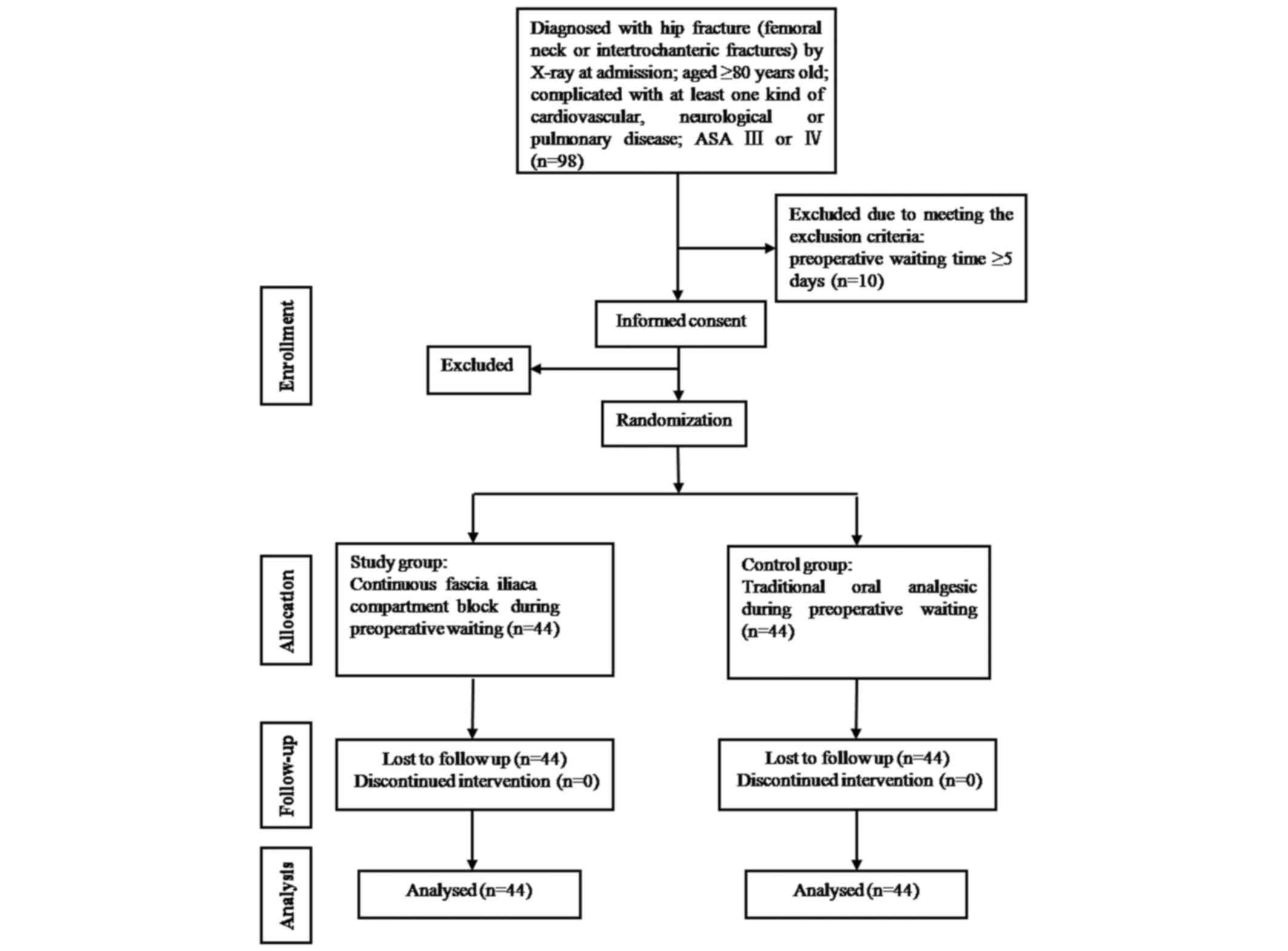
the present study (Fig. 1). The
following inclusion criteria were used in the present study: i)
Diagnosis of hip fracture (femoral neck or intertrochanteric
fractures) by X-ray at admission; ii) age ≥80 years; iii)
complication with at least one kind of cardiovascular, neurological
or pulmonary disease; iv) ASA classification III or IV; and iv)
being male or female. Exclusion criteria were: i) Presence of more
than one fracture; ii) allergy to amides, paracetamol and tramadol;
iii) infection at fascia iliaca compartment puncture site; iv)
peripheral neuropathy; v) contraindication of intraspinal block;
vi) renal insufficiency and dementia; vii) preoperative waiting
time ≥5 days; and vii) refusing to participate in this study.
Treatment groups and the protocol
Patients meeting the inclusion criteria were
randomly assigned into two groups, the control group and the study
group, by a computer-generated random number table method (MATLAB
2014a; MathWorks, Natick, MA, USA) with randomized group
information sealed in an opaque envelope, the envelopes were
numbered and used sequentially. All patients were assessed
cognitive function with the Mini-Mental State Examination at
admission. The control group received traditional analgesia
including 50 mg Tramadol (batch no. 10087215; Mundipharma
International, Ltd., Cambridge, UK) and 500 mg paracetamol (batch
no. 140616620; Johnson & Johnson, New Brunswick, NJ, USA)
orally three times a day from admission to surgery. The patients in
the control group were not subjected to CFICB and were
administrated with saline. In the study group, after the patients
were diagnosed with hip fracture by X-ray at admission, the
fracture side received ultrasound-guided CFICB following
establishment of the upper limb venous pathway. The CFICB operation
was performed as follows: Patients were in supine position and the
puncture site was selected at 1 cm to the junction point at 1/3 of
the connection of anterior superior spine and pubic tubercle. A
M-Turbo ultrasound apparatus (Sonosite, Inc., Bothell, WA, USA)
high-frequency probe was placed in parallel to the inguinal fold to
distinguish the femoral fascia and fascia iliaca, the needle was
inserted with out-of-plane technique at an angle of 45° and the tip
of the needle was pointed to the head. Once needle-tip placement
under the fascia iliaca by hydrolocation was confirmed, the probe
was rotated 90° into a longitudinal parasagittal orientation to
visualize the needle tip in-plane and to track cephalad spread of
the injectate under fascia iliaca. A total of 50 ml 0.4%
ropivacaine (batch no. NAKR; AstraZeneca, Cambridge, UK) was
injected and formed a fluid-filled space beneath the fascia.
Subsequently, the catheter was inserted with the puncture needle
and the tip of the catheter was 5–10 cm beyond the tip of the
needle. Following confirmation of the correct location of the
catheter, the catheter was fixed tightly and connected to the
electronic analgesic pump to continuously infuse 0.2% ropivacaine
at a rate of 5 ml/h until the day of surgery. The local anesthetic
moved cephalad and reached the nerves of the lumbar plexus,
including the femoral, lateral cutaneous and obturator. If the
analgesic effect was inadequate (VAS score >30 mm), 5 ml of 0.2%
ropivacaine would be added into the fascia iliaca compartment. In
the morning of the day of surgery, the catheter was removed from
the fascia iliaca compartment. Ultrasound-guided CFICB was
performed by an anesthesiologist with experience in
ultrasound-guided nerve block.
According to the type of fracture, the patients were
treated with proximal femoral nail antirotation, hemiarthroplasty,
cannulated screws or total hip replacement. Subcutaneous injection
of enoxaparin sodium (40 mg/day; batch no. 4sj11; Sanofi S.A.,
Paris, France) was given to all patients preventively after
admission, which was discontinued 12 h prior to surgery and
continued on the first day after surgery. All patients received
combined subarachnoid and epidural anesthesia in L2-3 or L3-4
interspace and subarachnoid injection of 0.5% bupivacaine (batch
no. 73141014; Shanghai Harvest Pharmaceutical Co., Ltd, Shanghai,
China) 1.0–1.5 ml for 35–40 sec. After the injection, a 3 cm
catheter was placed into the epidural cavity, 2% lidocaine (batch
no. 20150401; Beijing Yimin Pharmaceutical Co., Ltd, Beijing,
China) was administered through the epidural catheter in doses of 3
ml as needed, and the level of anesthesia was maintained at
~T10. After surgery, all patients entered the post
anesthesia care unit for at least 1 h and then were transferred to
the wards. All patients received patient-controlled intravenous
analgesia within 48 h after surgery, and the analgesic regimen was
1.5 µg/kg sufentanil (batch no. 1150309; Yichang Humanwell
Pharmaceutical Co., Ltd, Yichang, China) and 8 mg ondansetron
hydrochloride (batch no. 140202A02; Ningbo Tenet Pharmaceutical
Co., Ltd, Zhenhai, China), diluted with normal saline to 100 ml, at
a background dose of 1–2 ml/h and a single added dose of 1 ml, with
a lockout interval of 10 min. From day 3 to discharge, the patients
received oral analgesic drugs.
Primary outcome measure
The present study used VAS scores (0–100, with 0
indicating no pain and 100 indicating the worst imaginable pain) to
evaluate the analgesic effect and recorded VAS scores at rest
(lying flat) and on movement (movement-associated pain was elicited
by passively elevating the fractured leg to 15°) prior to
administration of analgesia (t0), 1 h after administration of
analgesia (t1), in the morning of the day of surgery (before
surgery; t2), in the morning of the day after surgery (t3) and in
the second morning after the day of surgery (t4). The patients used
VAS (0–100) to evaluate the satisfaction with the analgesic regimen
in the preoperative waiting period.
Secondary outcome measures
The present study recorded the number of patients
developing analgesia-induced complications, including nausea,
vomiting, respiratory depression (respiratory rate of <10/min)
and excessive sedation (Ramsay score ≥3 points, where score 1 point
indicated not quiet, agitated patients; 2 points: Quiet and
cooperative patients; 3 points: Drowsy and obeying directive; 4
points: Drowsy and responding to tactile stimulation; 5 points:
Lethargic and only responding to strong stimulation; 6 points: In
deep sleep, no response to calling). The number of patients needing
additional rescue analgesia and CFICB complications were also
recorded, including local anesthetic toxicity, puncture site
infection and hematoma. Nausea and/or vomiting were treated using
intravenous administration of ondansetron. Respiratory depression
was treated by close surveillance together with naloxone and
oxygen.
Other outcome measures
Incidence of cardiovascular, pulmonary and cerebral
complications during hospital stay was also recorded.
Cardiovascular complications included acute myocardial infarction,
angina pectoris, new arrhythmia (atrial fibrillation, ventricular
premature beats and tachycardia), acute heart failure, cardiac
arrest and deep venous thrombosis of lower extremities. Diagnosis
of myocardial infarction was reached if: i) CK-MB isoenzyme or
troponin-I concentrations were above the laboratory myocardial
infarction threshold (CK-MB, >4.99 ng/ml; cTNI, >0.02 ng/ml);
and ii) either new Q waves (≥0.03 s) or persistent alterations (4
days) were identified in the ST-T segment. Unstable angina was
defined as severe precordial chest pain with a duration of ≥30 min
and unresponsive to standard therapy, associated with ST-segment or
T-wave alterations without Q waves or cardiac enzyme abnormalities.
Congestive heart failure was defined using clinical (shortness of
breath, rales, jugular venous distention, peripheral edema and
third heart sound) and radiological (cardiomegaly, interstitial
edema, alveolar edema) signs and required modified medication
involving minimum treatment with diuretic drugs. New arrhythmia was
confirmed by 12-lead electrocardiogram. Pulmonary complications
included pulmonary infection, pulmonary embolism and respiratory
failure, and cerebral complications included new cerebral
infarction and delirium. The above complications were diagnosed by
clinical symptoms associated with relevant auxiliary examinations.
The incidence of cardiovascular, pulmonary and cerebral
complications was recorded in three periods: The preoperative
waiting period, surgery and form the end of surgery to discharge.
Four different periods, including hospital admission, preoperative
period, surgery and following surgery, were denoted as N1, N2, N3
and N4, respectively. In addition, the preoperative waiting time,
length of stay, hospital costs and mortality during hospitalization
were recorded.
Analgesic effects, analgesia-induced complications
and CFICB-associated complications were evaluated and recorded by
the acute pain service. Patients' general characteristics,
including gender, age, weight, height, ASA grade and type of
surgery; perioperative complications; preoperative waiting time;
length of stay; hospital costs and other data were collected by
another anesthesiologist in a blinded manner.
Statistical analysis
All the analyses were performed using SPSS software
(version 18.0; SPSS, Inc., Chicago, IL, USA). The sample size was
estimated based on two-way repeated measures analysis of variance
comparison of the VAS scores between groups. VAS scores were
measured at five different time points outlined above for each
patient. A total of 40 patients in each group were required to
complete the study and the assumptions of 5% type I error rate, 80%
power and 0.45 effect size were considered. Based on the assumption
of a dropout rate of ~10%, 44 patients would be required to be
enrolled in each group. A total of 88 patients were included in the
statistical analysis, 44 cases were included in the control group
and 44 cases in the study group.
Data are presented as mean ± standard deviation for
continuous variables and as frequency (%) for categorical
variables. For continuous variables, the normal distribution
assumption was assessed. Equal variance assumption was also
assessed. The differences of these characteristics between the
control group and study group were performed using independent
two-sample t-tests. Categorical variables were summarized using
frequency and percentage and compared using Chi-square test.
Intergroup differences in VAS scores were assessed by two-way
repeated measures analysis of variance with Bonferroni post hoc
test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Demographic data
From October 2015 to December 2016, a total of 88
patients were included in the statistical analysis, 44 cases were
included in the control group and 44 cases in the study group.
General patients' characteristic and surgical characteristics were
summarized in Table I. No
significant differences were identified between the two groups,
including age, height, weight and ASA classification (Table I). The duration of hospital stay of
the control group was significantly longer compared with the study
group.
 | Table I.Characteristics of patients. |
Table I.
Characteristics of patients.
|
Characteristics | Control group
(n=44) | Study group
(n=44) | P-value |
|---|
| Waiting time before
surgery (days) | 3.34±0.89 | 3.27±0.82 | 0.709 |
| Hospital stay
(days) | 13.55±6.03 | 9.98±2.46 | 0.001 |
| Hospital expenses
(¥RMB) |
65,786.82±19,741.77 |
61,425.02±13,159.95 | 0.226 |
| Male (n, %) | 14 (31.8%) | 16 (36.4%) | 0.653 |
| Age (years) | 83.73±3.40 | 84.05±5.04 | 0.730 |
| Weight (kg) | 60.18±10.83 | 58.70±12.35 | 0.552 |
| Height (cm) | 159.93±7.12 | 163.20±9.38 | 0.069 |
| ASA stage (n) |
|
| 0.676 |
|
III | 40 | 42 |
|
| IV | 4 | 2 |
|
| Type of surgery
(n) |
|
| 0.752 |
|
Hemiarthroplasty | 9 | 6 |
|
|
Proximal femoral nail
antirotation | 33 | 34 |
|
|
Cannulated screws | 1 | 2 |
|
| Total
hip replacement | 1 | 2 |
|
| Anesthesia method
(n) |
|
| 1.000 |
|
Combined spinal-epidural
anesthesia | 44 | 44 |
|
| Duration of
anesthesia (min) | 168.73±47.13 | 158.48±36.71 | 0.258 |
| Duration of
operation (min) | 95.07±42.53 | 82.25±32.79 | 0.117 |
| Total liquid intake
(ml) | 985.23±156.48 | 965.91±158.40 | 0.566 |
| Crystalloid
solution volume (ml) | 628.41±238.06 | 613.64±206.40 | 0.757 |
| Colloidal solution
volume (ml) | 279.55±241.68 | 304.55±263.21 | 0.644 |
| Bleeding (ml) | 180.68±89.76 | 168.18±111.13 | 0.563 |
| Urine volume
(ml) | 411.59±179.29 | 373.86±199.27 | 0.353 |
| Intraoperative
blood infusion (n, %) | 9 (20.5%) | 9 (20.5%) | 1.000 |
| MMSE | 20.95±1.57 | 21.18±1.77 | 0.526 |
Pain assessment
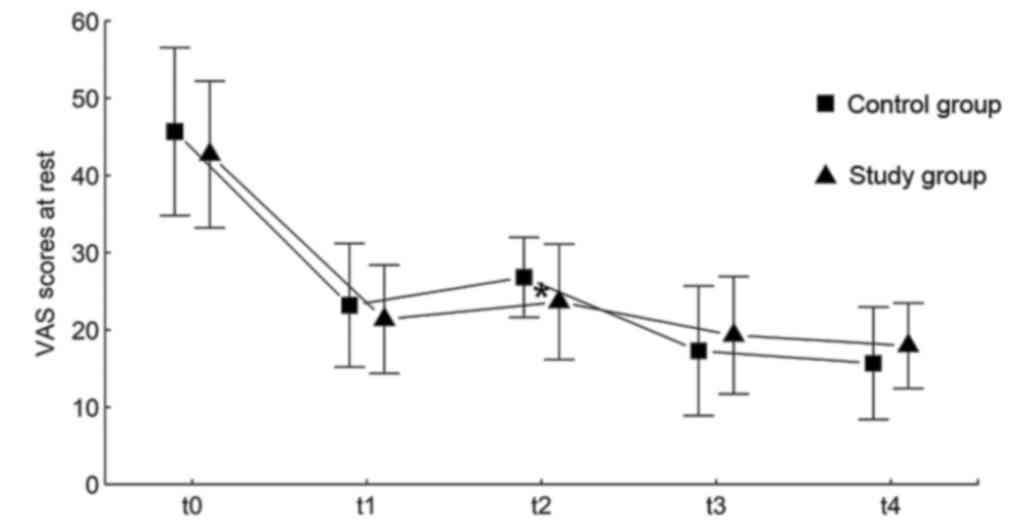
Although the differences were small, VAS pain scores
at rest of the study group were lower compared with the control
group (P=0.023) at the time point t2. There were no significant
differences in the VAS pain scores at rest between the groups at
the other time points (P=0.178 at t0; P=0.260 at t1; P=0.240 at t3;
P=0.103 at t4; Fig. 2; Data are
presented as the mean ± standard deviation).
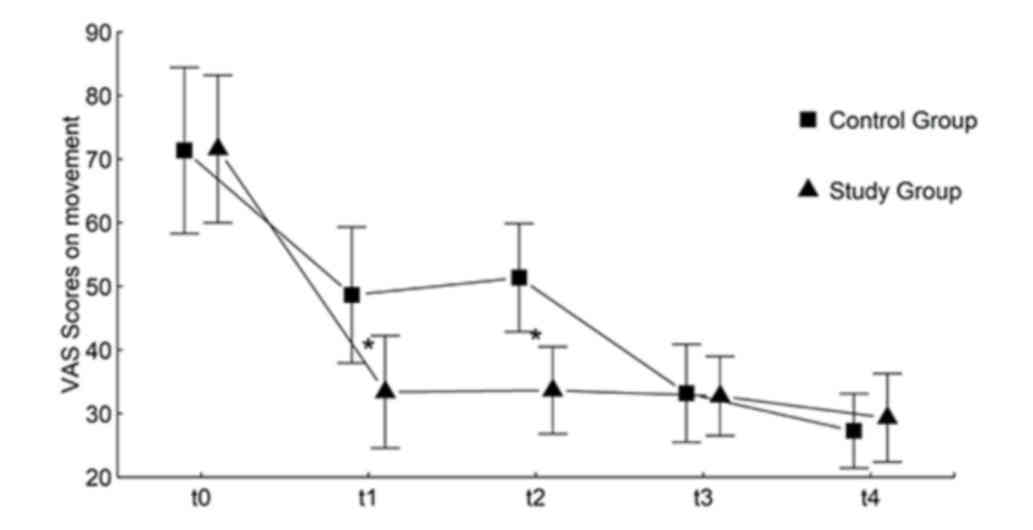
VAS pain scores at passive movement of the study
group were significantly lower compared with the control group at
the time point t1 (P<0.05) and t2 (P<0.05). There were no
significant differences in VAS pain scores at passive movement
between the groups at the other time points (P=0.931 at t0; P=0.762
at t3; and P=0.139 at t4; Fig. 3;
Data are presented as mean ± standard deviation).
Scores for patients' satisfaction with the analgesic
regimen in the preoperative period were increased in the study
group compared with the control group (45.68±11.29 in the control
group vs. 74.77± 9.52 in the study group; P<0.001; Table II).
| Table II.Analgesia satisfaction scores and
analgesia-associated side effects. |
Table II.
Analgesia satisfaction scores and
analgesia-associated side effects.
| Parameters | Control group
(n=44) | Study group
(n=44) | P-value |
|---|
| Satisfaction with
the analgesic regimen in the preoperative period | 45.68±11.29 | 74.77±9.52 | <0.001 |
| Nausea (n, %) | 12 (27.3%) | 7 (15.9%) | 0.195 |
| Vomiting (n,
%) | 5 (11.4%) | 4 (9.1%) | 1.000 |
Intergroup differences in VAS scores were assessed
by two-way repeated measures analysis of variance with Bonferroni
post hoc test. For VAS pain scores at rest, there were no
significant differences between the groups (P=0.472). Significant
time effect (P<0.001) and significant interaction effect between
time and group (P=0.034) were identified; a significant difference
of VAS at rest between groups at time point t2 and no significant
difference at other time points were observed. For VAS pain scores
at passive movement, there were significant differences between
groups (P<0.001), significant time effect (P<0.001) and
significant interaction effect between time and group (P<0.001);
a significant difference of VAS at passive movement between groups
at t1 and t2 and no significant difference at other time points
were suggested.
Side effects
The incidence of nausea and vomiting were similar
between the control group and the study group in the preoperative
period (P=0.195 and P=1; respectively; Table II). All patients in the present
study did not demonstrate symptoms of respiratory depression and
excessive sedation in the preoperative waiting period. The study
group did not develop CFICB complications (local anesthetic
toxicity, puncture site infection and hematoma in preoperative
waiting period; data not shown).
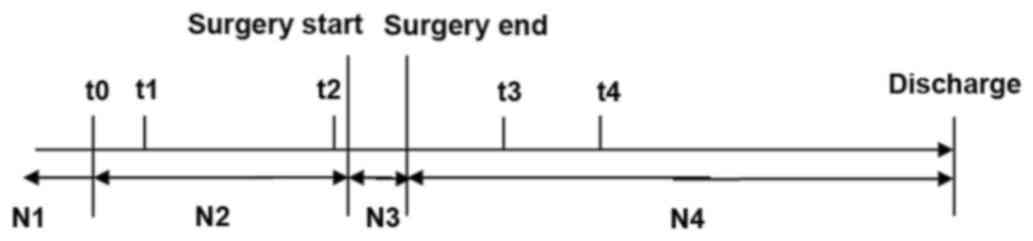
Number of complications
The number of complications was calculated at four
different periods, including hospital admission, preoperative
period, surgery and following surgery, and were denoted as N1, N2,
N3 and N4, respectively (Fig. 4).
The alterations in the number of complications between two
different time points were analyzed, as shown in Table III. Patients in the study group
were less likely to have increased complications compared with
patients in the control group over the N2-N4 period (from
preoperative period to after surgery; P=0.016; Table III).
| Table III.Number of complications in the four
time periods in the control and study groups. |
Table III.
Number of complications in the four
time periods in the control and study groups.
| Time period | Control group
(n=44) | Study group
(n=44) | P-value |
|---|
| N2 vs. N1 |
|
| 1.000 |
| No
change | 40 | 41 |
|
|
Increase | 4 | 3 |
|
| N3 vs. N1 |
|
| 1.000 |
| No
change | 40 | 40 |
|
|
Increase | 4 | 4 |
|
| N4 vs. N1 |
|
| 0.059 |
| No
change | 32 | 39 |
|
|
Increase | 12 | 5 |
|
| N3 vs. N2 |
|
| 0.306 |
|
Decrease | 2 | 0 |
|
| No
change | 41 | 43 |
|
|
Increase | 1 | 1 |
|
| N4 vs. N2 |
|
| 0.016 |
|
Decrease | 2 | 0 |
|
| No
change | 33 | 42 |
|
|
Increase | 9 | 2 |
|
Patient mortality
A total of 3 patients succumbed to mortality in
postoperative hospitalization. A total of 2 cases (4.5%) succumbed
to mortality in the control group, including 1 mortality due to
respiratory failure and 1 mortality due to acute myocardial
infarction and heart failure. A patient (2.3%) in the study group
succumbed to sudden cardiac mortality associated with malignant
arrhythmia.
Discussion
Patients with hip fracture are often in considerable
pain and, if untreated, may develop various complications that
delay operative intervention and prolong hospitalization (25). Pain management is believed to be
critical in both the pre- and post-operative periods for patients
with geriatric hip fractures (26–28). For
most fractures, administration of systemic analgesics including
opioids, paracetamol and non-steroidal anti-inflammatory drugs is
preferred for pain management. Despite the relative safety of
paracetamol, both opioids and nonsteroidal analgesia can induce
significant adverse effects especially in the elderly population
(17,29). According to the guidelines from the
National Institute for Health and Clinical Excellence, neural
blockade by trained personnel is recommended for a reasonable
opioid dosage (30).
The present study demonstrated that pain relief was
superior in the study group (patients aged ≥80 years old,
complicated with at least one type of cardiovascular, neurological
or pulmonary disease), compared with the control group, during the
preoperative period. In addition, CFICB was associated with greater
patient satisfaction, which was consistent with the results of
Candal-Couto et al (23) and
Dulaney-Cripe et al (24).
Diakomi et al (31) concluded
that performing an FICB prior to positioning for spinal anesthesia
provided superior pain management compared with intravenous
fentanyl administration facilitated spinal performance. According
to Diakomi et al (31) and
the present study, FICB provided superior analgesia not only prior
to positioning for spinal anesthesia but also during the
preoperative period. The study group in the present study did not
develop CFICB-associated complications. The present results
suggested that a fascia iliaca compartment block performed via a
catheter provided a significant benefit to very elderly patients
with hip fractures. Hip innervation involves the lateral cutaneous
nerve of the thigh, the femoral nerve and the obturator nerve
(32). Fascia iliaca compartment
block utilizes the space under the iliac fascia where the femoral,
obturator and lateral cutaneous nerves are located (33). The block acts by suppressing the
sensation of pain in the femoral nerve, lateral femoral cutaneous
nerve of the thigh and obturator nerve (22). The incidence of nausea and vomiting
were similar between the control group and the study group during
pre-operative period, which may have been due to the small number
of patients enrolled in this study. In other countries, a majority
of patients with hip fracture undergo single fascia iliaca
compartment block in the emergency room prior to surgery (21,22),
while in the present study, continuous block and perineural
catheter placement permitted the provision of continuous peripheral
nerve block, thereby extending the duration of analgesia.
Szucs et al (34) have demonstrated that continuous
femoral nerve block provided a more effective perioperative
analgesia compared with a standard opiate-based regimen for
patients undergoing fixation of fractured neck of femur. Another
study suggested that both ultrasound-guided continuous femoral
nerve block and fascia iliaca compartment block with a novel
cannula-over-needle provide effective anesthesia and postoperative
analgesia for elderly patients with hip replacement (35). It has been reported that 3-in-1
femoral nerve block is also effective in hip fracture analgesia
(20,36). Femoral nerve block is recognized as
an effective method; however, it is controversial due to its
potential for nerve injury and femoral nerve block can cause
quadriceps weakness (37). The FICB
technique is somehow favorable compared with the femoral nerve
block technique, as it is not necessary to use a neurostimulator
during the procedure (38). The site
of injection with the FICB is distant from any nerves or blood
vessels, where intravascular or intraneural injection is
contraindicated in principle (39).
The fascia iliaca compartment block is more effective compared with
the 3-in-1 block in producing simultaneous blockade of the lateral
femoral cutaneous nerve of the thigh and femoral nerves in adults
(40). The three nerves, including
femoral nerve, lateral femoral cutaneous nerve of the thigh and
obturator nerve, were more successfully blocked by FICB (>90%)
compared with the 3-in-1 block (20%) (33). In addition, performing the fascia
iliaca compartment block is easier to teach and learn compared with
the 3-in-1 block, and more convenient and cost-effective (41). Therefore, the continuous FICB was
selected in the present study.
The sensorial innervation of the hip is provided by
the nerves in the lumbar plexus and sacral plexus (42). Although whether lumbar or sacral
plexus have a primary effect on sensorial innervation of the hip
remains unknown, according some previous studies (39,40) and
the present study, the lumbar plexus block can provide effective
analgesia. In addition, the two groups of patients included in the
present study did not undergo FICB after surgery, as neural
blockade could intervene with postoperative mobilization in those
patients.
There are numerous ways to perform the FICB,
including the loss of resistance (‘2-pop technique’) (21), ultrasound guided blocks (43) or the nerve stimulators for femoral
nerve localization (44). Nerve
stimulator-based femoral nerve block is characterized by
stimulation of the leg muscles, which may cause discomfort to the
patient and compromise the fracture alignment (45). Ultrasound guidance does not require a
nerve stimulator, facilitates the FICB technique and reduces the
risk of block failure or nerve injury (43,46).
The results of the present study indicated that the
length of stay was shorter and costs of hospitalization were
slightly lower in the study group compared with the control group.
After hip fracture, pain is an important determinant of function,
which therefore determines length of stay and clinical outcome,
defined by complication and mortality rates (47). Adequate analgesia allows for
increased mobility of patients and reduced duration of
hospitalization (24,28). A shorter stay is beneficial to
patients in terms of reduced risk of hospital-acquired
complications and the associated reduction of costs of
hospitalization is economically beneficial for the healthcare
system (24,48). In addition, in the present study, the
duration of hospital stay was shorter in the study group compared
with the control group, which may have been associated with the
number of patients with increased complications being smaller in
the study group compared with the control group.
Patients in the study group were less likely to have
increased complications compared with patients in the control group
over the N2-N4 period (from preoperative period to after surgery),
and the results of the analysis of postoperative morbidity outcomes
should be interpreted cautiously, as these factors, including the
supplement of oxygen, fluid management and mobilization, were not
controlled. However, failure to stabilize the medical conditions
prior to surgery poses an increased risk of postoperative cardiac
and pulmonary complications, prolonged hospitalization and
mortality (49). The present study
indicated that ultrasound-guided CFICB induced a satisfactory
analgesic effect, which may be associated with decreased incidence
of complications in the study group, compared with the control
group after surgery.
In addition, mortality during hospital stay was 2/44
(4.5%) in the control group and 1/44 (2.3%) in the study group,
which was consistent with earlier studies that reported in-hospital
mortality rates of 2.3–13.9% in unselected groups of patients with
hip fracture (4).
There are several limitations of the present study
and it was mainly limited by its size. Due to a small number of
cases, whether ultrasound-guided CFICB can reduce the incidence of
postoperative cardiovascular, pulmonary and cerebral complications
in very elderly patients with hip fracture requires further
confirmation by multicenter and large-sample size studies.
Furthermore, the patients were not blind to group allocation due to
the ethical considerations. As it was considered ethically
unacceptable to insert a placebo fascia iliaca compartment catheter
for blinding purposes only, no further damage could be simulated in
the control group patients, and, therefore the patients in the
control group were not subjected to CFICB and administrated with
saline. Furthermore, the present study only recorded patients'
mortality during the hospital stay, without a follow up for a
longer period.
In conclusion, the present study demonstrated that
ultrasound guided continuous fascia iliaca compartment block may
provide a superior analgesia for very elderly patients with hip
fracture compared with patients receiving systemic analgesia-based
regimen during the preoperative period.
Acknowledgements
Not applicable.
Funding
The present study was supported by Beijing Municipal
Admi-nistration of Hospitals' Ascent Plan (grant no. DFL20150802)
and Beijing Municipal Commission of Health and Family Planning
(grant no. PXM2017_026283_000002).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YM and TW designed the study. JW performed the
collection and entry of the data. JX analyzed the data. YM prepared
the manuscript. FL participated in the collection of the data and a
literature analysis. All the authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Xuanwu Hospital, Capital Medical University (Beijing, China).
Signed written informed consents were obtained from the
patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Johnell O and Kanis JA: An estimate of the
worldwide prevalence, mortality and disability associated with hip
fracture. Osteoporos Int. 15:897–902. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Watters CL and Moran WP: Hip fractures-a
joint effort. Orthop Nurs. 25:157–165; quiz 166–167. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Marks R: Hip fracture epidemiological
trends, outcomes, and risk factors, 1970–2009. Int J Gen Med.
3:1–17. 2010.PubMed/NCBI
|
|
4
|
Boddaert J, Cohen-Bittan J, Khiami F,
Khiami F, Le Manach Y, Raus M, Beinis JY, Verny M and Riou B:
Postoperative admission to a dedicated geriatric unit decreases
mortality in elderly patients with hip fracture. PLoS One.
9:e837952014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rosencher N, Vielpeau C, Emmerich J,
Fagnani F and Samama CM: ESCORTE group: Venous thromboembolism and
mortality after hip fracture surgery: The ESCORTE study. J Thromb
Haemost. 3:2006–2014. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mak JC, Cameron ID and March LM: National
health and medical research council: Evidence-based guidelines for
the management of hip fractures in older persons: An update. Med J
Aust. 192:37–41. 2010.PubMed/NCBI
|
|
7
|
Simunovic N, Devereaux PJ, Sprague S,
Guyatt GH, Schemitsch E, Debeer J and Bhandari M: Effect of early
surgery after hip fracture on mortality and complications:
Systematic review and meta-analysis. CMAJ. 182:1609–1616. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moja L, Piatti A, Pecoraro V, Ricci C,
Virgili G, Salanti G, Germagnoli L, Liberati A and Banfi G: Timing
matters in hip fracture surgery: Patients operated within 48 hours
have better outcomes. A meta-analysis and meta-regression of over
190,000 patients. PLoS One. 7:e461752012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Colais P, Di Martino M, Fusco D, Perucci
CA and Davoli M: The effect of early surgery after hip fracture on
1-year mortality. BMC Geriatr. 15:1412015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Association of Anaesthetists of Great
Britain and Ireland, . Griffiths R, Alper J, Beckingsale A,
Goldhill D, Heyburn G, Holloway J, Leaper E, Parker M, Ridgway S,
et al: Management of proximal femoral fractures 2011: Association
of Anaesthetists of Great Britain and Ireland. Anaesthesia.
67:85–98. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tran T, Delluc A, de Wit C, Petrcich W, Le
Gal G and Carrier M: The impact of oral anticoagulation on time to
surgery in patients hospitalized with hip0 fracture. Thromb Res.
136:962–965. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Orosz GM, Hannan EL, Magaziner J, Koval K,
Gilbert M, Aufses A, Straus E, Vespe E and Siu AL: Hip fracture in
the older patient: Reasons for delay in hospitalization and timing
of surgical repair. J Am Geriatr Soc. 50:1336–1340. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kanis JA, Johnell O, Oden A, Sembo L,
Redlund-Johnell L, Dawson A, De Laet C and Jonsson B: Long-term
risk of osteoporotic fracture in Malmö. Osteoporos Int. 11:669–674.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Roche JJ, Wenn RT, Sahota O and Moran CG:
Effect of comorbidities and postoperative complications on
mortality after hip fracture in elderly people: Prospective
observational cohort study. Bmj. 331:13742005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jandziol AK and Griffiths R: The
anaesthetic management of patients with hip fractures. Bja Cepd
Reviews. 1:52–55. 2001. View Article : Google Scholar
|
|
16
|
Sciard D, Cattano D, Hussain M and
Rosenstein A: Perioperative management of proximal hip fractures in
the elderly: The surgeon and the anesthesiologist. Minerva
Anestesiol. 77:715–722. 2011.PubMed/NCBI
|
|
17
|
Godoy Monzón D, Vazquez J, Jauregui JR and
Iserson KV: Pain treatment in post-traumatic hip fracture in the
elderly: Regional block vs. Systemic non-steroidal analgesics. Int
J Emerg Med. 3:321–325. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Scheinin H, Virtanen T, Kentala E, Uotila
P, Laitio T, Hartiala J, Heikkilä H, Sariola-Heinonen K, Pullisaar
O, Yli-Mäyry S and Jalonen J: Epidural infusion of bupivacaine and
fentanyl reduces perioperative myocardial ischaemia in elderly
patients with hip fracture-a randomized controlled trial. Acta
Anaesthesiol Scand. 44:1061–1070. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Matot I, Oppenheim-Eden A, Ratrot R,
Davidson E, Eylon S, Peyser A and Liebergall M: Preoperative
cardiac events in elderly patients with hip fracture randomized to
epidural or conventional analgesia. Anesthesiology. 98:156–163.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Luger TJ, Kammerlander C, Benz M, Luger MF
and Garoscio I: Peridural anesthesia or ultrasound-guided
continuous 3-in-1 block: Which is indicated for analgesia in very
elderly patients with hip fracture in the emergency department?
Geriatr Orthop Surg Rehabil. 3:121–128. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Foss NB, Kristensen BB, Bundgaard M, Bak
M, Heiring C, Virkelyst C, Hougaard S and Kehlet H: Fascia iliaca
compartment blockade for acute pain control in hip fracture
patients. Anesthesiology. 106:773–778. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fujihara Y, Fukunishi S, Nishio S, Miura
J, Koyanagi S and Yoshiya S: Fascia iliaca compartment block: Its
efficacy in pain control for patients with proximal femoral
fracture. J Orthop Sci. 18:793–797. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Candal-Couto JJ, McVie JL, Haslam N, Innes
AR and Rushmer J: Pre-operative analgesia for patients with femoral
neck fractures using a modified fascia iliaca block technique.
Injury. 36:505–510. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dulaney-Cripe E, Hadaway S, Bauman R,
Trame C, Smith C, Sillaman B and Laughlin R: A continuous infusion
fascia iliaca compartment block in hip fracture patients: A pilot
study. J Clin Med Res. 4:45–48. 2012.PubMed/NCBI
|
|
25
|
Viscusi ER and Pappagallo M: A review of
opioids for in-hospital pain management. Hosp Pract. 40:149–159.
2012. View Article : Google Scholar
|
|
26
|
Pedersen SJ, Borgbjerg FM, Schousboe B,
Pedersen BD, Jørgensen HL, Duus BR and Lauritzen JB: Hip Fracture
Group of Bispebjerg Hospital: A comprehensive hip fracture program
reduces complication rates and mortality. J Am Geriatr Soc.
56:1831–1838. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Catananti C and Gambassi G: Pain
assessment in the elderly. Surg Oncol. 19:140–148. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chin RP, Ho CH and Cheung LP: Scheduled
analgesic regimen improves rehabilitation after hip fracture
surgery. Clin Orthop Relat Res. 471:2349–2360. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Petre BM, Roxbury CR, McCallum JR,
Defontes KW III, Belkoff SM and Mears SC: Pain reporting, opiate
dosing, and the adverse effects of opiates after hip or knee
replacement in patients 60 years old or older. Geriatr Orthop Surg
Rehabil. 3:3–7. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Abou-Setta AM, Beaupre LA, Rashiq S,
Dryden DM, Hamm MP, Sadowski CA, Menon MR, Majumdar SR, Wilson DM,
Karkhaneh M, et al: Comparative effectiveness of pain management
interventions for hip fracture: A systematic review. Ann Intern
Med. 155:234–245. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Diakomi M, Papaioannou M, Mela A,
Kouskouni E and Makris A: Preoperative fascia iliaca compartment
block for positioning patients with hip fractures for central
nervous blockade: A randomized trial. Reg Anesth Pain Med.
39:394–398. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Birnbaum K, Prescher A, Hessler S and
Heller KD: The sensory innervation of the hip joint-an anatomical
study. Surg Radio Anat. 19:371–375. 1997. View Article : Google Scholar
|
|
33
|
Dalens B, Vanneuville G and Tanguy A:
Comparison of the fascia iliaca compartment block with the 3-in-1
block in children. Anesth Analg. 69:705–713. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Szucs S, Iohom G, O'Donnell B, Sajgalik P,
Ahmad I, Salah N and Shorten G: Analgesic efficacy of continuous
femoral nerve block commenced prior to operative fixation of
fractured neck of femur. Perioper Med (Lond). 1:42012.PubMed/NCBI
|
|
35
|
Yu B, He M, Cai GY, Zou TX and Zhang N:
Ultrasound-guided continuous femoral nerve block vs continuous
fascia iliaca compartment block for hip replacement in the elderly:
A randomized controlled clinical trial (CONSORT). Medicine
(Baltimore). 95:e50562016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Fletcher AK, Rigby AS and Heyes FL:
Three-in-one femoral nerve block as analgesia for fractured neck of
femur in the emergency department: A randomized, controlled trial.
Ann Emerg Med. 41:227–233. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Paul JE, Arya A, Hurlburt L, Cheng J,
Thabane L, Tidy A and Murthy Y: Femoral nerve block improves
analgesia outcomes after total knee arthroplasty: A meta-analysis
of randomized controlled trials. Anesthesiology. 113:1144–1162.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Monzon Godoy D, Iserson KV and Vazquez JA:
Single fascia iliaca compartment block for post-hip fracture pain
relief. J Emerg Med. 32:257–262. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Inan N, Takmaz Akin S, Iltar S, Yazici I
and Basar H: The effects of two different multimodal analgesic
regimens in total hip replacement surgery. Agri. 21:69–74.
2009.PubMed/NCBI
|
|
40
|
Capdevila X, Biboulet P, Bouregba M,
Barthelet Y, Rubenovitch J and d'Athis F: Comparison of the
three-in-one and fascia iliaca compartment blocks in adults:
Clinical and radiographic analysis. Anesth Analg. 86:1039–1044.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Newman B, McCarthy L, Thomas PW, May P,
Layzell M and Horn K: A comparison of pre-operative nerve
stimulator-guided femoral nerve block and fascia iliaca compartment
block in patients with a femoral neck fracture. Anaesthesia.
68:899–903. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Deniz S, Atım A, Kürklü M, Çaycı T and
Kurt E: Comparison of the postoperative analgesic efficacy of an
ultrasound-guided fascia iliaca compartment block versus 3 in 1
block in hip prosthesis surgery. Agri. 26:151–157. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Dolan J, Williams A, Murney E, Smith M and
Kenny GN: Ultrasound guided fascia iliaca block: A comparison with
the loss of resistance technique. Reg Anesth Pain Med. 33:526–531.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ganapathy S, Wasserman RA, Watson JT,
Bennett J, Armstrong KP, Stockall CA, Chess DG and MacDonald C:
Modified continuous femoral three-in-one block for postoperative
pain after total knee arthroplasty. Anesth Analg. 89:1197–1202.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Lopez S, Gros T, Bernard N, Plasse C and
Capdevila X: Fascia iliaca compartment block for femoral bone
fractures in prehospital care. Reg Anesth Pain Med. 28:203–207.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Hebbard P, Ivanusic J and Sha S:
Ultrasound-guided supra-inguinal fascia iliaca block: A cadaveric
evaluation of a novel approach. Anaesthesia. 66:300–305. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Sanzone AG: Current challenges in pain
management in hip fracture patients. J Orthop Trauma. 30 Suppl
1:S1–S5. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Lau TW, Fang C and Leung F: The
effectiveness of a geriatric hip fracture clinical pathway in
reducing hospital and rehabilitation length of stay and improving
short-term mortality rates. Geriatr Orthop Surg Rehabil. 4:3–9.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
French DD, Bass E, Bradham DD, Campbell RR
and Rubenstein LZ: Rehospitalization after hip fracture: Predictors
and prognosis from a national veterans study. J Am Geriatr Soc.
56:705–710. 2008. View Article : Google Scholar : PubMed/NCBI
|