Introduction
Temporomandibular joint (TMJ) cartilage degeneration
and defects caused by rheumatoid arthritis and osteoarthritis are
common clinical problems, which can restrict opening of the mouth
and cause TMJ locking and pain. Articular cartilage defects can be
fully self-regenerated when the cartilage defect is <3 mm in
diameter (1); however,
self-regeneration is limited in defects >4 mm in diameter due to
a lack of a proper chondrogenic niche (2). Current clinical treatments, including
condylar surface shaving and periosteal grafts, are not adequately
effective (3,4). The repair of TMJ cartilage defects
continues to perplex oral and maxillofacial surgeons.
Chondrocytes are one of the major cell types
suitable for the repair of cartilage defects and may also have an
essential role in the development and maintenance of the articular
niche (5). Previous studies have
demonstrated that mature articular chondrocytes can regenerate
cartilage and steadily maintain the cartilage phenotype in
subcutaneous environments (6,7);
however, the limited chondrocyte resources restrict the further
utilization and generalization of these results.
Bone marrow stromal cells (BMSCs) have
self-duplication capacity and possess the potential to
differentiate into several tissues, including bone, cartilage,
tendon, muscle, and fat (8,9). BMSCs exist in bone marrow and can be
harvested by a minimally invasive procedure. BMSCs can also be
cultured in sufficient numbers in vitro while preserving
their multipotential differentiation capacity (10). Therefore, BMSCs have become a popular
focus of tissue engineering research.
It has been shown that BMSCs can maintain a high
proliferative status in vitro (11). Therefore, previous investigations
have focused on the cartilage formation induced from the BMSCs
in vivo and in vitro (12). Yang et al (13) reported that the co-transplantation of
BMSCs, chondrocytes, and chondrogenic factors into a hydrogel may
enhance the chondrogenesis of BMSCs in subcutaneous environments,
suggesting that chondrocytes may possess the potential to promote
BMSC chondrogenesis. However, these studies adopted a large number
of cellular factors to stimulate the differentiation of BMSCs into
chondrocytes. The economic cost of the procedures used in these
studies was great, and adverse effects may result. Liu et al
(14) demonstrated that paracrine
signalling by chondrocytes created a chondro-inductive niche
similar to the articular subcutaneous environment used to direct
the chondrogenesis of BMSCs in vitro. However, the
co-culture of BMSCs and chondrocytes in the regeneration of
condylar articular cartilage defects in vivo has not been
reported until recently.
Pluronic F-127 (Poloxamer 407, PF-127) is a
polyoxyethylene-polyoxypropylene surface active block copolymer.
These gels exhibit reverse thermal behaviour and are therefore
fluid at refrigerator temperature (0–4°C) but are soft gels at body
temperature (15). This
characteristic has allowed PF-127 to be used as a carrier for
various routes of administration, including oral (16), intranasal (17), rectal (18), and ocular (19).
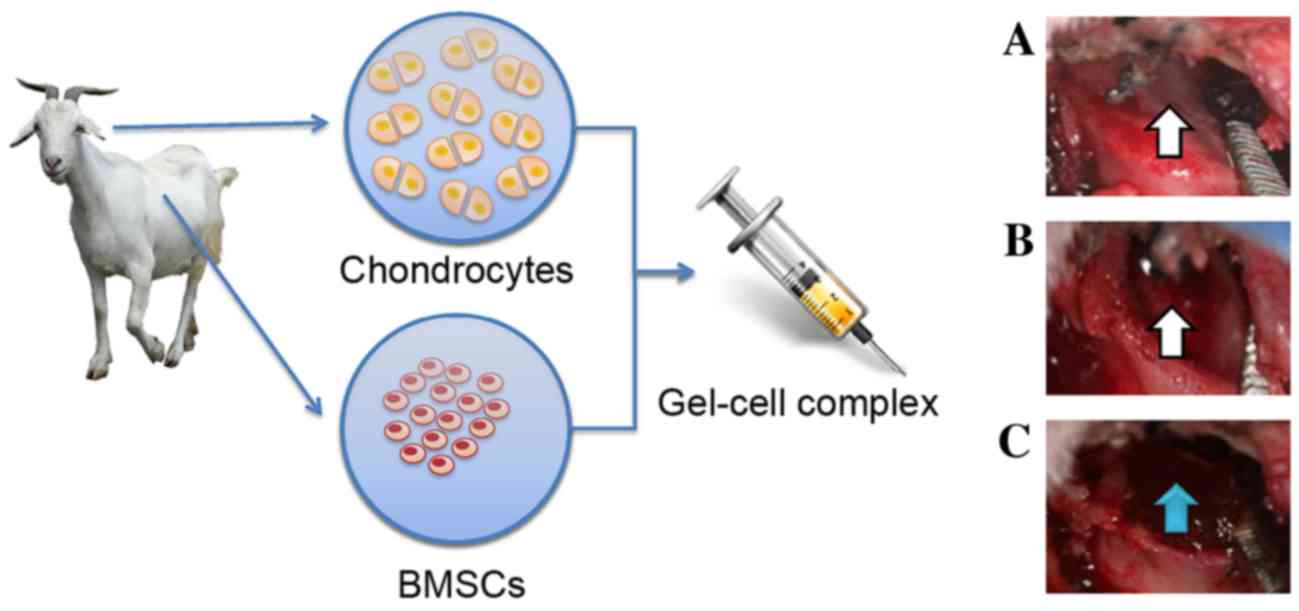
In the present study, a combination of BMSCs and
chondrocytes in hydrogel constructs (Pluronic F-127 gel) was used
to repair goat TMJ articular cartilage defects. A green
fluorescence protein (GFP) retrovirus vector was used to track the
presence of BMSCs in vivo and to evaluate the possibility of
using BMSCs and chondrocytes for cartilage defect repairs in
vivo to develop a novel tissue engineering approach for the
clinical reconstruction of TMJ cartilage.
Materials and methods
Animal model
All procedures followed the ethical guidelines of
the Animal Experimental Ethical Inspection of Shanghai Ninth
People's Hospital affiliated to Shanghai Jiao Tong University
(Shanghai, China). A total of 12 mature male healthy goats, aged
6–8 months and weighing 10–22 kg were purchased from Shanghai
Agricultural Institute (Shanghai, China) and subsequently randomly
divided into a gel-cell group (group 1) and a gel alone group
(control; group 2; Table I).
 | Table I.Animal grouping. |
Table I.
Animal grouping.
| Group | 4 weeks | 8 weeks | 12 weeks | Total |
|---|
| Gel-cell
complex | 2 | 2 | 2 | 6 |
| Gel only | 2 | 2 | 2 | 6 |
Cell source and culture
conditions
Mature goats were given intramuscular injections of
ketamine-846 (Institute of Animal Science, Changchun University of
Agriculture and Animal Science, Changchun, China.) anaesthesia
mixture prior to bone marrow harvesting. Bone marrow cells were
harvested from the ilium by a sterile surgical technique and
suspended in 1X phosphate-buffered saline (PBS) containing 2%
bovine serum albumin (BSA). Following centrifugation (179 × g at
room temperature) for 5 min to remove serum ingredients, bone
marrow cells were treated with sterile water for 10 sec to disrupt
red blood cells, re-suspended in 2% BSA in PBS, and centrifuged
(179 × g at room temperature) again for 5 min. Precipitated bone
marrow cells from each goat were cultured in 100-mm diameter tissue
culture dishes with 10 ml α-minimum essential medium (Gibco; Thermo
Fisher Scientific, Inc., Waltham, MA, USA) supplemented with 10%
foetal bovine serum (FBS) (Gibco; Thermo Fisher Scientific, Inc.)
and ampicillin antibiotic at 37°C in a humidified atmosphere
containing 5% CO2 for 1 week. Once the attached cells
formed a large colony, the cells were transferred to a new plate
for expansion until 80% confluence was achieved.
BMSCs were labelled with green fluorescence protein
(GFP), as previously described (13). GFP lentiviruses were produced by
transient transfection into the 293FT cell line (Invitrogen; Thermo
Fisher Scientific, Inc.) with the pLenti6.2-GW/EmGFP vector and
three packaging plasmids, pLP1, pLP2, and pLP/VSVG (Invitrogen;
Thermo Fisher Scientific, Inc.).
For the isolation of auricular chondrocytes,
auricular cartilage (3×3 cm2) was harvested from the
goat ear by a sterile surgical technique and cut into 2×2
mm2 sections. The tissue was then digested by 0.25%
pancreatic enzyme for 30 min, followed by digestion with 0.1%
collagenase II for 4 h at 37°C. Following filtration, cells were
centrifuged (179 × g at room temperature) for 5 min and
re-suspended in 1X PBS containing 2% BSA. The auricular
chondrocytes from each goat were cultured in 100-mm diameter tissue
culture dishes with 10 ml 10% FBS Dulbecco's modified Eagle
medium.
Surgical procedures
Goats were administered general intramuscular
anaesthesia using ketamine-846 anaesthesia mixture prior to
harvesting condylar cartilage. An incision was made near the ear
side to expose the article area and the cartilage on the surface of
the condylar process (Fig. 1). The
full-thickness condylar cartilage was totally removed to create a
lesion in the condyle surface using a surgical drill (Fig. 1).
Chondrocytes and GFP-labelled BMSCs were also
collected from the culture and mixed using a ratio of 3:7
(chondrocytes:BMSCs), as previously described by our group
(14). Mixed cells were re-suspended
in 30% Pluronic F-127 at a density of 5×107 cells/ml to
form a gel-cell complex. Pluronic F-127 gel mixed with chondrocytes
and BMSCs was implanted into both sides of the condylar cartilage
defects (Fig. 1). Pluronic F-127 gel
alone was implanted into the condylar cartilage defects of group 2
as a control. Articular capsules were adequately closed. All goats
were allowed to move freely after these procedures and housed in
separated cages, fed soft food pellets ad libitum, and kept in a
temperature-controlled environment with a 12-h light/dark
cycle.
Gross morphology and X-ray
observations
At 4, 8, and 12 weeks after surgery, the maximal
passive mouth-opening range under general intramuscular anaesthesia
was measured. Four goats in both groups were X-rayed and
subsequently sacrificed for gross morphology observation. The TMJ
was exposed, and the whole joint and adjacent tissues were
harvested for gross morphology and histology analyses.
Histology
After evaluating the gross morphology, the TMJ
samples were fixed in 10% neutral formalin buffer for 1 week at
room temperature and decalcified in 30% formic acid for ~2 weeks.
The samples were then dehydrated and embedded into paraffin
blocks.
Samples were cut into 5-µm sections and stained with
hematoxylin and eosin, as previously described (8). Sections were viewed under a light
microscope and graded semi-quantitatively, using a scoring system
modified from that described by Wakitani et al (20). The scale is composed of five
categories and assigns a score ranging from 0 to 14 points
(Table II). The distribution of
GFP-labelled cells was observed and captured by laser scanning
spectral confocal microscopy (TCS SP5; Leica Microsystems Wetzlar,
Maneheim, Germany). The inflammatory response (inflammatory cells,
fibroblasts) and osteophyte formation were also evaluated using
histological slides.
| Table II.Histological grading scale for the
cartilage defects. |
Table II.
Histological grading scale for the
cartilage defects.
| Category | Points |
|---|
| Cell
morphology |
|
| Hyaline
cartilage | 0 |
| Mostly
hyaline cartilage | 1 |
| Mostly
fibrocartilage | 2 |
| Mostly
non-cartilage | 3 |
|
Non-cartilage only | 4 |
| Matrix-staining
(metachromasia) |
|
| Normal
(compared with host adjacent cartilage) | 0 |
|
Slightly reduced | 1 |
|
Markedly reduced | 2 |
| No
metachromatic stain | 3 |
| Surface
regularity |
|
| Smooth
(>3/4) | 0 |
|
Moderate (>1/2-3/4) | 1 |
|
Irregular (1/4-1/2) | 2 |
|
Severely irregular
(<1/4) | 3 |
| Thickness of
cartilage |
|
|
>2/3 | 0 |
|
1/3-2/3 | 1 |
|
<1/3 | 2 |
| Integration of
donor with host adjacent cartilage |
|
| Both
edges integrated | 0 |
| One
edge integrated | 1 |
| Neither
edge integrated | 2 |
| Total
maximum | 14 |
Detection of GFP-labelled cells in
mixed cell tissues
Chondrocytes and BMSCs (labelled with GFP) were
seeded together in 30% Pluronic F-127 at a ratio of 3:7 at a
density of 5×107 cells/ml to form a gel-cell complex.
The tissues containing GFP-labelled BMSCs were collected, frozen in
optimum cutting temperature gel, and sliced at a thickness of 5 µm.
The exact distribution of the labelled cells was observed and
captured by a Leica TCS SP5 laser scanning spectral confocal
microscope. The chondrogenic differentiation of the labelled cells
was further confirmed by histological analysis.
Immunohistochemical staining
Following de-paraffinisation and an endogenous
peroxidase block, the sections were heated in a water bath at 98°C
with 0.01 M citrate buffer (pH, 6.0) for 20 min, treated with 1%
H2O2 in water for 30 min, incubated with
mouse monoclonal antibody to type II collagen (Neomarkers, Fremont,
CA, USA) at a dilution of 1:5,000 overnight at 4°C, and visualized
using a 3,3′-diaminobenzidine (DAB) detection kit (Dako; Agilent
Technologies, Inc., Santa Clara, CA, USA). Negative controls were
prepared using PBS instead of antibody.
Statistical analysis
Statistical analysis was performed using Student's
t-test to assess the differences between the two groups. Estimates
were given as medians, and two-tailed values of P<0.05 were
considered to indicate a statistically significant difference.
Results
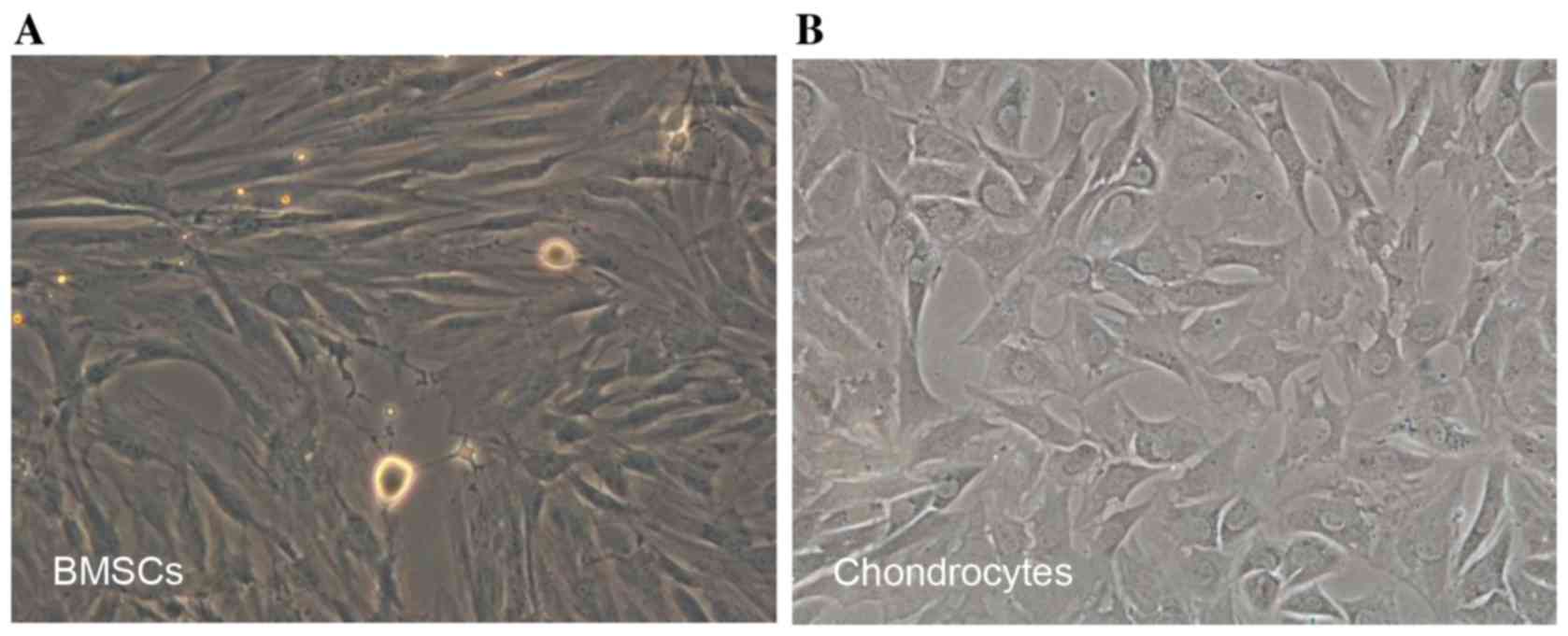
Preparation of BMSCs and
chondrocytes
Newly isolated BMSCs began to adhere within 24 h
after incubation on a 10-cm culture dish. Several cell colonies
were formed after 5 days of culture. BMSCs exhibited spindle-like
or elongated shapes (Fig. 2A). Newly
isolated chondrocytes were polygonal in shape with more regular
dimensions. Cells were shown to attach to the dish within 3 days
(Fig. 2B).
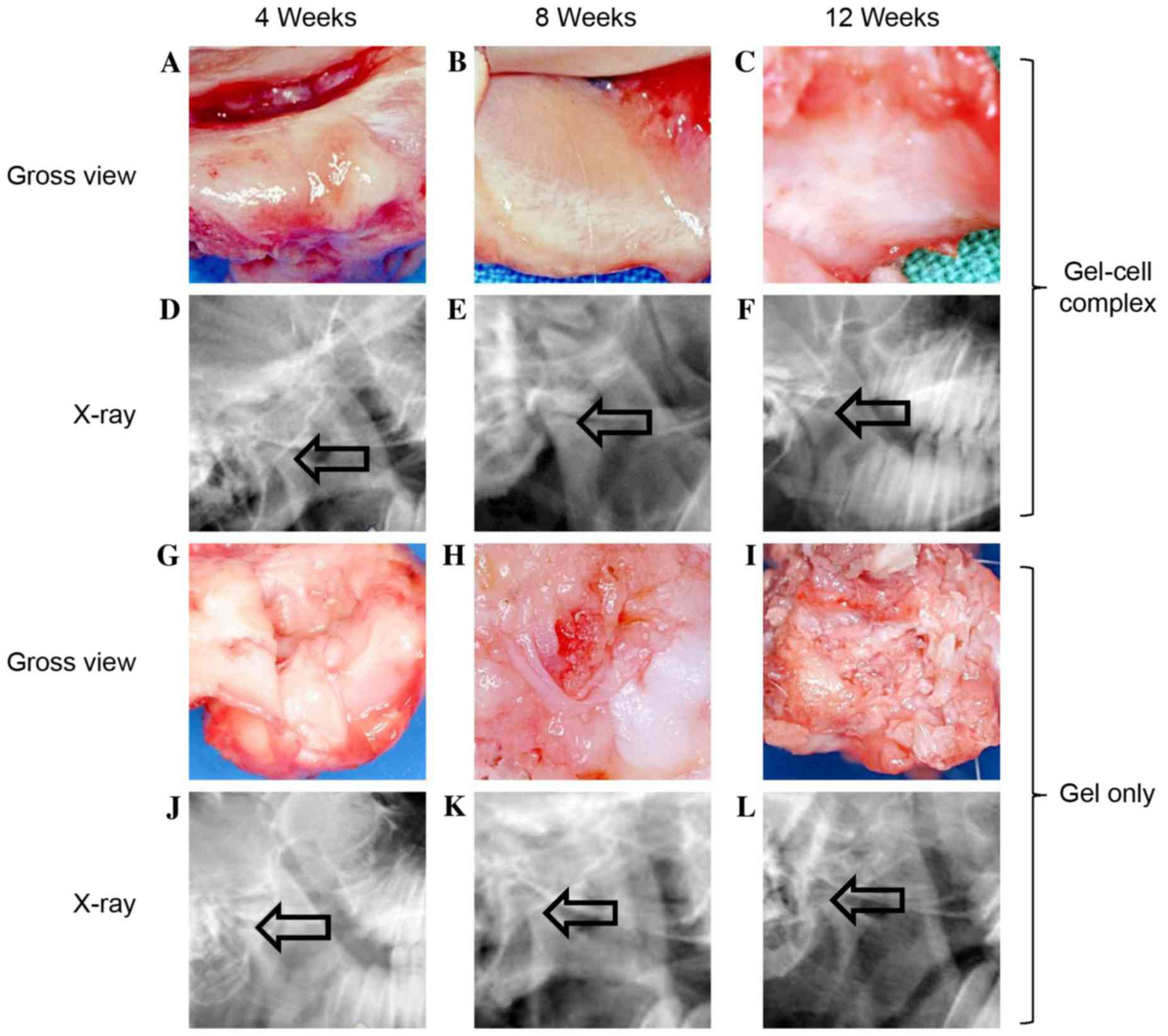
Gross assessment and X-ray
observation
As outlined in Fig.
3, no infection was observed in any of the TMJ joints from
either group. In the gel-cell transplanted group, the passive
mouth-opening range of the experimental animals 4 weeks after
surgery was similar to their pre-operative states. No adhesions
were found between the cartilage defects of the condylar processes
and the articular discs. However, the condylar process surfaces
were slightly rough and depressed (Fig.
3A). At 8 weeks post-surgery, the passive mouth-opening range
remained similar to the pre-operative levels. No further adhesions
were found in the gap between cartilage defect areas and the
articular discs. The condylar process surfaces became smooth, and a
cartilage-like layer was observed on the condylar process surfaces
(Fig. 3B). At 12 weeks post-surgery,
the mouth-opening range showed no notable change compared to
pre-operative levels. The condylar process surface of each goat was
smooth, and more cartilage-like layers were observed on the
condylar process surfaces (Fig. 3C).
The X-ray film analysis showed that there was no obvious bone
destruction and no osteophyte was formed (Fig. 3D-F).
In the gel alone group, the passive mouth-opening
range of the goat was slightly shorter than the pre-operative
levels at 4 weeks post-surgery. Adhesive tissue was observed
between the cartilage defect areas of the condylar process and the
articular disc. The condylar process surface was rough and
depressed. No Pluronic F-127 gel was found on the defect areas
(Fig. 3G). At 8 weeks post-surgery,
mouth opening was much shorter compared to both the pre-operative
levels and the levels 4 weeks post-surgery. More adhesive tissue
was found between the cartilage defect areas and articular discs
compared to 4 weeks post-surgery. The rough condylar process
surface remained the same (Fig. 3H).
At 12 weeks post-surgery, the animal mouth-opening range was even
shorter than that observed at 8 weeks post-surgery. Severe
adhesions were observed between the cartilage defect areas and
articular discs. However, some fibrous-like tissues were observed
on the rough condylar process surfaces (Fig. 3I). X-ray film analysis showed that
the joint space seem broadened compared with the gel-cell group
(Fig. 3J-L). These results suggested
that the cartilage defect healing process was delayed in the goats
exposed to gel alone.
Histological evaluation
As outlined in Fig.
4, in the gel-cell group after hematoxylin and eosin staining,
the condylar process surfaces were slightly rough and filled with
cartilaginous and fibrous tissue at 4 weeks post-surgery (Fig. 4A). At 8 weeks, 70% of the defect
areas were filled with cartilaginous and fibrous tissue (Fig. 4B). At 12 weeks, the surfaces became
smooth and the superficial layers were repaired with cartilage-like
tissue, while the deeper layers were replaced with bone or
osseous-like tissue (Fig. 4C).
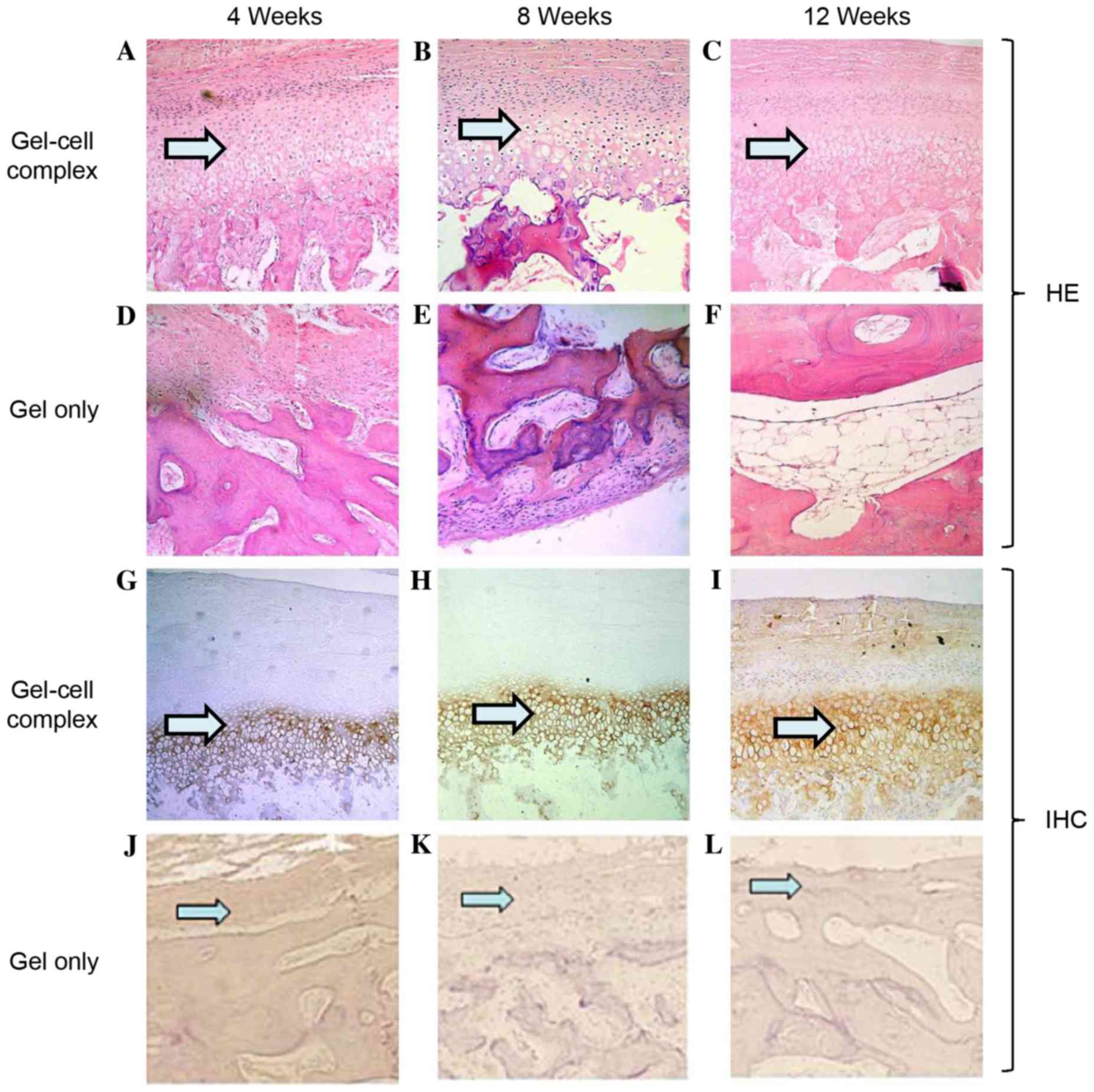 | Figure 4.Histological evaluation of defects
via HE staining and IHC staining with collagen II. For HE staining
in the gel-cell complex group: (A) At week 4, the surfaces were
slightly irregular and filled with cartilaginous and fibrous
tissue; (B) at week 8, the surfaces were much smoother, and most
parts of the defects were filled with cartilaginous and fibrous
tissue; (C) and at week 12, the surface became very smooth, and the
superficial layer was repaired with cartilage and the deeper layer
was remodelled with bone or osseous-like tissue. For HE staining in
the gel only group: (D) At week 4, the surfaces were irregular and
filled with fibrous tissue but not cartilaginous and/or osseous
tissue; (E) at week 8, the surfaces were still irregular, and most
parts of the defects were filled with fibrous or osseous-like
tissue; (F) at week 12, the surfaces were smooth and repaired with
mostly osseous-like tissue and some fibrous tissue without any
cartilage tissue (phase contrast, ×100). For IHC staining in the
gel-cell complex group: (G) At week 4, the cartilage layer was
stained with type II collagen at a low intensity; (H) at week 8,
the cartilage layer was stained with type II collagen at a much
higher intensity; (I) at week 12, the cartilage layer was stained
with type II collagen at a high intensity. For IHC staining in the
gel only group: (J) At week 4, type II collagen staining was
negative, and no Pluronic F-127 gel was found on the surface. The
same was observed at (K) 8 weeks and (L) 12 weeks post-surgery. HE,
hematoxylin and eosin; IHC, immunohistochemical. |
In the gel only control group, the surface tissue of
the defect areas in the condylar processes were disorganised and
filled with a small amount of fibrous tissue at 4 weeks
post-surgery (Fig. 4D). However, no
Pluronic F-127 gel was left on the defect areas, indicating that
the gel had degraded by that time. At 8 weeks, the surfaces of the
defects were still rough; ~60% of the defects were filled with
fibrous or osseous-like tissue (Fig.
4E). At 12 weeks, the surfaces were filled with fibro-like
tissue without any cartilaginous tissue (Fig. 4F).
Histological grading of the repair
tissue
Scores of group 1 were improved at 8 and 12 weeks
compared with those at 4 weeks (Table
III). These results were in accordance with those of
macroscopic and histological observations. The scores of the
experimental groups were similar, with the exception of surface
regularity. In group 2, the histological scores indicated markedly
inferior repair, when compared with group 1.
| Table III.Results of the histological grading
scale. |
Table III.
Results of the histological grading
scale.
|
|
| Grade |
|---|
|
|
|
|
|---|
| Group | Time (weeks) | Cell
morphology | Matrix
staining | Surface
regularity | Thickness of
cartilage | Integration | Total |
|---|
| Gel-cell
complex | 4 | 2.0 | 1.0 | 0.7 | 1 | 0.0 | 4.7 |
|
| 8 | 2.0 | 1.0 | 0.0 | 1 | 0.0 | 4.0 |
|
| 12 | 2.0 | 1.0 | 0.0 | 1 | 0.0 | 4.0 |
| Gel only | 4 | 3.5 | 2.5 | 1.5 | 2 | 1.5 | 11.0 |
|
| 8 | 3.0 | 3.0 | 2.0 | 2 | 2.0 | 12.0 |
|
| 12 | 4.0 | 3.0 | 2.5 | 2 | 2.0 | 13.5 |
Immunohistochemical staining
To determine if the newly formed tissue was
cartilage, immunohistochemical staining was performed using
sections harvested at 4, 8 and 12 weeks post-surgery. In the
gel-cell complex group, newly formed surface layers exhibited weak
staining of type II collagen at 4 weeks, indicating that the cells
in this layer had become chondrocytes and started to secrete type
II collagen (Fig. 4G). At 8 and 12
weeks, the cartilage layer demonstrated strong staining of type II
collagen (Fig. 4H and I,
respectively), suggesting that more cartilage had formed. No type
II collagen staining was observed in the gel alone group at any of
the three time points, indicating that no cartilage formed in the
gel alone group (Fig. 4J-L).
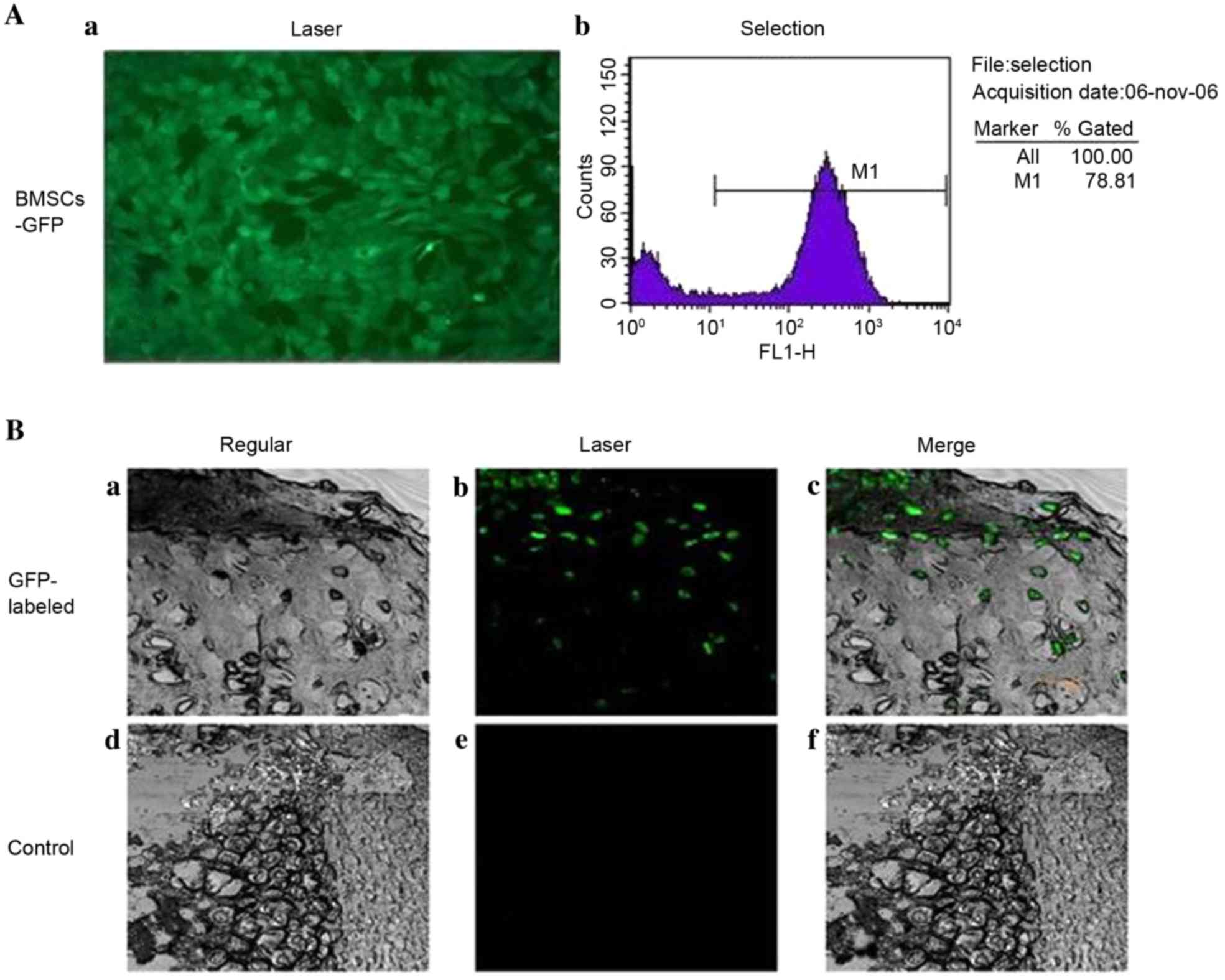
GFP-labelled cells in mixed cell
engineered tissues
BMSCs were successfully infected and labelled with
GFP (Fig. 5A). GFP-labelled cells
were detected in the newly formed cartilage lacuna of the newly
formed tissue at 12 weeks post-surgery in gel-cell
complex-transplanted goats, using laser confocal microscopy
(Fig. 5B), which provided direct
evidence that the BMSCs had been transformed into chondrocyte-like
cells. No GFP-positive cells were observed in the control group.
These results further indicate that the chondrogenic niche
accelerates the transition of BMSCs to chondrocytes in the TMJ
environment.
Discussion
Despite its remarkable ability to resist mechanical
loading, articular cartilage is not capable of mounting a useful
reparative reaction in response to damage (21). Among the most common causes of damage
to cartilage are trauma, osteoarthritis and osteochondritis
dissecans (22). Each of these three
conditions can present in similar ways, with pain, swelling and
impaired movement of the joint. Avascularity is a major factor in
the poor cartilage repair response; this means that there is no
supply of clotting materials or cells to produce repair material
following damage or insult (23).
Avascularity may also indicate that there is no supply of
mesenchymal stem cells.
For a long time, it has been the goal of surgeons to
develop a reliable method to repair damaged articular cartilage.
Techniques have ranged from debris removal techniques, such as
debridement and lavage developed in the 1940s, to osteochondral
transplant techniques, marrow stimulation techniques and the latest
generation of cell-based tissue engineering techniques, such as
autologous chondrocyte implantation (24). Bone marrow stimulation techniques are
based on the principle that when natural full-depth defects cross
the subchondral bone, bleeding from the bone marrow leads to the
production of repair tissue within the lesion (25). The problem with these techniques is
that, although the clot produced fills the defect and produces
repair tissue, this tissue is mostly fibro-cartilaginous and is a
poor mechanical substitute for the natural hyaline cartilage
(26).
Difficulties associated with producing hyaline
cartilage-like repair tissue in defects using these surgical
techniques, combined with the problems associated with revision
surgery of total joint replacements in young active individuals,
has led to the expansion of tissue engineering approaches to treat
damaged cartilage. Currently, the only cell-based tissue
engineering approach that is licenced for use in patients is
autologous chondrocyte implantation (ACI). This procedure, which
was pioneered by Brittberg and first used in 1987, involves the use
of autologous chondrocytes to produce repair tissue within a defect
(27). ACI has been a successful
technique, and even the first generation used in the late 1980 s
produced improvements in joint function, reduced pain scores, and
in some cases, produced hyaline-like repair tissue (28). Despite this success, ACI has had and
continues to have problems. The first is the risk of donor site
morbidity, this has been partially dealt with by moving away from
the use of periosteal flaps but still remains a problem at the
cartilage harvest site. Damage to the cartilage can lead to further
degeneration and osteoarthritis over the long term (29). Another major drawback with ACI is the
in vitro cell culture stage. When chondrocytes are cultured
in a 2D environment for an extended period of time, they
dedifferentiate. Dedifferentiation involves a decrease in the
expression of collagen markers, such as type II collagen, and an
increase in type I collagen production; the cells also develop a
fibroblastic morphology (30). This
process prevents chondrocytes cultured for too long in vitro
from being able to produce repair cartilage. The very low cell
density in cartilage and the small areas available for harvesting,
combined with their limited ability for useful expansion in
vitro, means that ACI can only utilise a particularly small
number of cells, whereas a larger number may have more success in
producing hyaline-like cartilage repair tissue as cell-to-cell
contact is believed to be important for chondrogenesis (31). There is a wide range of different
approaches that are used to surgically treat damaged or diseased
cartilage, ranging from marrow stimulation and debridement to
cell-based tissue engineering in the form of ACI. However, each of
the aforementioned techniques has faults, as well as benefits, so
other avenues are being explored to treat damaged cartilage. One of
these avenues is the use of mesenchymal stem cells (MSCs), rather
than chondrocytes, in tissue engineering applications (32).
The broad definition of an MSC is often given as a
culture-adherent multipotent progenitor cell that can differentiate
down the adipogenic, chondrogenic and osteogenic lineages (33). As well as being found in various
different tissue types, under the correct conditions, MSCs are
capable of producing a wide range of tissues in vivo and
in vitro. By definition, MSCs can be differentiated into
cartilage, bone and fat-producing cells in vivo and in
vitro and it is this feature that makes them such a potentially
powerful tool within tissue engineering. To induce chondrogenesis
in MSCs, the cells need to be in close contact, as well as exposed
to the correct soluble factors (31). To achieve this, MSCs are suspended in
culture medium and spun in a centrifuge to produce a pellet
culture. The pellet is then cultured in a growth medium containing
tumor growth factor (TGF)-β, leading to the development of
cartilaginous tissue that stains for toluidine blue and contains
type II collagen (34). A problem
with this cartilage model, however, is that TGF-β-induced
chondrogenesis over time leads to the hypertrophy of chondrogenic
MSCs and an increased expression of osteogenic markers, such as
type X collagen and Runx2, in a similar progression of
differentiation to that observed during bone formation via
endochondral ossification, in which chondrocytes undergo
hypertrophy leading to apoptosis calcification (35). MSCs maintain their chondrogenic
ability, even throughout long-term monolayer culture, although
their replicative capacity is not infinite. Banfi et al
(36) estimated that the useful
clinical limit for expansion would be 17 population doublings, more
than twice as many as chondrocytes can be usefully expanded by.
In the present study, BMSCs and chondrocytes were
co-cultured in vitro at ratios of 6:4 or 7:3 and the
findings showed that chondrocytes provided a chondrogenic
micro-environment to induce chondrogenic differentiation of BMSCs
and thus promote the in vitro chondrogenesis of BMSCs. It
was also demonstrated that, at a ratio of 1:4, chondrocytes with
BMSCs provided a chondrogenic microenvironment (37). In this experiment to repair condylar
defects, BMSCs and chondrocytes were mixed using a ratio of 7:3 in
Pluronic F-127 without any growth factors. The condylar surface
became very smooth, the superficial layer was repaired with
cartilaginous tissue, and the deeper layer was remodelled with bone
or osseous-like tissue at 12 weeks after surgery. Cartilaginous
tissue was formed at 4, 8 and 12 weeks after surgery, as shown by
the staining of type II collagen. The mouth-opening range of the
experimental group was similar to pre-operative levels, and no
adhesions were found between the cartilage defect areas and the
articular discs at 4, 8 and 12 weeks after surgery. These data
suggest that mixed BMSCs and chondrocytes enhance the healing of
articular cartilage defects.
There are several possible explanations for the
manner whereby BMSCs and chondrocytes interact with each other in
osteochondral repair. Several types of soluble factors secreted by
chondrocytes, such as TGF-βs, IGF-1 and BMPs, have a direct effect
on BMSCs by inducing the differentiation of BMSCs into chondrocytes
(37). In addition, chondrocytes
synthesize and secrete cartilage-specific extracellular matrix to
induce BMSC differentiation into chondrocytes (38). BMSCs differentiate into chondrocytes
by cell-to-cell contact signalling between BMSCs and chondrocytes.
Finally, chondrocytes can secrete anti-angiogenic factors to
prevent vascular invasion and retain their own phenotypes, thus
preventing neo-vascularization and ossification (39). The findings of this study also showed
no vascular invasion at the superficial and the deeper layers of
the condylar surface at 12 weeks after surgery.
In the present study, goats were implanted with
BMSCs labelled with GFP, and thus, it was possible to trace the
implanted BMSCs and to further illustrate the differentiation and
distribution of BMSCs post-surgery. As shown in our results, the
GFP-labelled cells were detected in newly formed cartilage lacunae
of repaired tissue at 12 weeks post-surgery, which provides
convincing evidence that the implanted BMSCs were able to
differentiate into mature chondrocytes in the chondrocyte-mediated
chondro-inductive niche in the TMJ environment. These results also
indicate that the implanted BMSCs were a vital cell source of newly
formed articular tissue.
Another precondition for a cartilage regeneration
system is suitable matrices that can be used as scaffold frameworks
for cell viability and proliferation while maintaining the original
cellular phenotype. Investigating biomaterials used as
three-dimensional scaffolds for cell delivery and therapy has
recently become a major focus in the field of tissue engineering
(40,41).
The culture of autologous chondrocytes has
previously been used to induce proliferation and differentiation in
a hydrogel system (42). Fully
thermo-reversible gelling polymers have attracted considerable
attention for use as scaffolds to hold cells in situ during
cartilage formation (43,44). These thermo-reversible polymers can
revert from a solid to a liquid state and from a liquid to a solid
state without losing their intrinsic properties. Additionally,
these polymers are fully soluble in aqueous solutions at
temperatures below their lower critical solution temperature (LCST)
but solidify to form a hydrated gel at temperatures above their
LCST (45). Although many studies
have been conducted to evaluate thermo-reversible hydrogels for use
as injectable scaffolds, few in vivo cartilage tissue
engineering tests involving differentiated materials have been
conducted.
In this study, Pluronic F-127 gel provided suitable
three-dimensional scaffolds for the BMSC and chondrocyte co-culture
system. GFP-labelled BMSCs were detected in the newly formed
cartilage lacuna of the newly formed tissue in gel-cell
transplanted goats, which provided direct evidence that the BMSCs
had been transformed into chondrocyte-like cells.
In conclusion, the present findings have
demonstrated the possibility of using BMSCs and chondrocytes for
the osteochondral repair of TMJ in vivo, which offer a novel
treatment for the clinical reconstruction of TMJ. However, the
exact mechanism whereby chondrocytes promote chondrogenic
differentiation of BMSCs remains to be addressed.
Acknowledgements
This project was financially supported in part by
the National Science Foundation of China (grant no. 81271122), the
Interdisciplinary Program of Shanghai Jiao Tong University (grant
nos. YG2017ZD03 and YG2014QN02), the Research Fund of Science and
Technology Commission of Shanghai City (grant no. 18410712000), and
the Shanghai Municipal Education Commission-Gaofeng Clinical
Medicine Grant Support (grant no. 20152225).
References
|
1
|
Kim HK, Moran ME and Salter RB: The
potential for regeneration of articular cartilage in defects
created by chondral shaving and subchondral abrasion. An
experimental investigation in rabbits. J Bone Joint Surg Am.
73:1301–1315. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Convery FR, Akeson WH and Keown GH: The
repair of large osteochondral defects. An experimental study in
horses. Clin Orthop Relat Res. 82:253–262. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Valentini V, Vetrano S, Agrillo A, Torroni
A, Fabiani F and Iannetti G: Surgical treatment of TMJ ankylosis:
Our experience (60 cases). J Craniofac Surg. 13:59–67. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hikiji H, Takato T, Matsumoto S and Mori
Y: Experimental study of reconstruction of the temporomandibular
joint using a bone transport technique. J Oral Maxillofac Surg.
58:1270–1277. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Görtz S and Bugbee WD: Allografts in
articular cartilage repair. J Bone Joint Surg Am. 88:1374–1384.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hangody L, Feczkò P, Bartha L, Bodò G and
Kish G: Mosaicplasty for the treatment of articular defects of the
knee and ankle. Clin Orthop Relat Res. 391 Suppl:S328–S36. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jamali AA, Emmerson BC, Chung C, Convery
FR and Bugbee WD: Fresh osteochondral allografts: Results in the
patellofemoral joint. Clin Orthop Relat Res. 176–185. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liechty KW, MacKenzie TC, Shaaban AF, Radu
A, Moseley AM, Deans R, Marshak DR and Flake AW: Human mesenchymal
stem cells engraft and demonstrate site-specific differentiation
after in utero transplantation in sheep. Nat Med. 6:1282–1286.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Minguell JJ, Erices A and Conget P:
Mesenchymal stem cells. Exp Biol Med (Maywood). 226:507–520. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Pittenger MF, Mackay AM, Beck SC, Jaiswal
RK, Douglas R, Mosca JD, Moorman MA, Simonetti DW, Craig S and
Marshak DR: Multilineage potential of adult human mesenchymal stem
cells. Science. 284:143–147. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Baksh D, Yao R and Tuan RS: Comparison of
proliferative and multilineage differentiation potential of human
mesenchymal stem cells derived from umbilical cord and bone marrow.
Stem Cells. 25:1384–1392. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li WJ, Tuli R, Huang X, Laquerriere P and
Tuan RS: Multilineage differentiation of human mesenchymal stem
cells in a three-dimensional nanofibrous scaffold. Biomaterials.
26:5158–5166. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yang HN, Park JS, Na K, Woo DG, Kwon YD
and Park KH: The use of green fluorescence gene (GFP)-modified
rabbit mesenchymal stem cells (rMSCs) co-cultured with chondrocytes
in hydrogel constructs to reveal the chondrogenesis of MSCs.
Biomaterials. 30:6374–6385. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Liu X, Sun H, Yan D, Zhang L, Lv X, Liu T,
Zhang W, Liu W, Cao Y and Zhou G: In vivo ectopic chondrogenesis of
BMSCs directed by mature chondrocytes. Biomaterials. 31:9406–9414.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bohorquez M, Koch C, Trygstad T and Pandit
N: A study of the temperature-dependent micellization of pluronic
F127. J Colloid Interface Sci. 216:34–40. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Padilla M, Clark GT and Merrill RL:
Topical medications for orofacial neuropathic pain: A review. J Am
Dent Assoc. 131:184–195. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ved PM and Kim K: Poly(ethylene
oxide/propylene oxide) copolymer thermo-reversible gelling system
for the enhancement of intranasal zidovudine delivery to the brain.
Int J Pharm. 411:1–9. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Barichello JM, Morishita M, Takayama K,
Chiba Y, Tokiwa S and Nagai T: Enhanced rectal absorption of
insulin-loaded Pluronic F-127 gels containing unsaturated fatty
acids. Int J Pharm. 183:125–132. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Desai SD and Blanchard J: Evaluation of
pluronic F127-based sustained-release ocular delivery systems for
pilocarpine using the albino rabbit eye model. J Pharm Sci.
87:1190–1195. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wakitani S, Okabe T, Horibe S, Mitsuoka T,
Saito M, Koyama T, Nawata M, Tensho K, Kato H, Uematsu K, et al:
Safety of autologous bone marrow-derived mesenchymal stem cell
transplantation for cartilage repair in 41 patients with 45 joints
followed for up to 11 years and 5 months. J Tissue Eng Regen Med.
5:146–150. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hodge WA, Fijan RS, Carlson KL, Burgess
RG, Harris WH and Mann RW: Contact pressures in the human hip joint
measured in vivo. Proc Natl Acad Sci USA. 83:2879–2883. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Madry H, Grün UW and Knutsen G: Cartilage
repair and joint preservation: Medical and surgical treatment
options. Dtsch Arztebl Int. 108:669–677. 2011.PubMed/NCBI
|
|
23
|
Becerra J, Andrades JA, Guerado E,
Zamora-Navas P, Lòpez-Puertas JM and Reddi AH: Articular cartilage:
Structure and regeneration. Tissue Eng Part B Rev. 16:617–627.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Redman SN, Oldfield SF and Archer CW:
Current strategies for articular cartilage repair. Eur Cell Mater.
9:23–32. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kim HK, Moran ME and Salter RB: The
potential for regeneration of articular cartilage in defects
created by chondral shaving and subchondral abrasion. An
experimental investigation in rabbits. J Bone Joint Surg Am.
73:1301–1315. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kelly DJ and Prendergast PJ:
Mechano-regulation of stem cell differentiation and tissue
regeneration in osteochondral defects. J Biomech. 38:1413–1422.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Brittberg M, Lindahl A, Nilsson A, Ohlsson
C, Isaksson O and Peterson L: Treatment of deep cartilage defects
in the knee with autologous chondrocyte transplantation. N Engl J
Med. 331:889–895. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Brittberg M: Cell carriers as the next
generation of cell therapy for cartilage repair: A review of the
matrix-induced autologous chondrocyte implantation procedure. Am J
Sports Med. 38:1259–1271. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fischer J, Dickhut A, Rickert M and
Richter W: Human articular chondrocytes secrete parathyroid
hormone-related protein and inhibit hypertrophy of mesenchymal stem
cells in coculture during chondrogenesis. Arthritis Rheum.
62:2696–2706. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Weiss S, Hennig T, Bock R, Steck E and
Richter W: Impact of growth factors and PTHrP on early and late
chondrogenic differentiation of human mesenchymal stem cells. J
Cell Physiol. 223:84–93. 2010.PubMed/NCBI
|
|
31
|
Mueller MB and Tuan RS: Functional
characterization of hypertrophy in chondrogenesis of human
mesenchymal stem cells. Arthritis Rheum. 58:1377–1388. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Williams R, Khan IM, Richardson K, Nelson
L, McCarthy HE, Analbelsi T, Singhrao SK, Dowthwaite GP, Jones RE,
Baird DM, et al: Identification and clonal characterisation of a
progenitor cell sub-population in normal human articular cartilage.
PLoS One. 5:e132462010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Caplan AI: Why are MSCs therapeutic? New
data: New insight. J Pathol. 217:318–324. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Johnstone B, Hering TM, Caplan AI,
Goldberg VM and Yoo JU: In vitro chondrogenesis of bone
marrow-derived mesenchymal progenitor cells. Exp Cell Res.
238:265–272. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Pelttari K, Steck E and Richter W: The use
of mesenchymal stem cells for chondrogenesis. Injury. 39 Suppl
1:S58–S65. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Banfi A, Muraglia A, Dozin B,
Mastrogiacomo M, Cancedda R and Quarto R: Proliferation kinetics
and differentiation potential of ex vivo expanded human bone marrow
stromal cells: Implications for their use in cell therapy. Exp
Hematol. 28:707–715. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zhou GD, Miao CL, Wang XY, Liu TY, Cui L,
Liu W and Cao YL: Experimental study of in vitro chondrogenesis by
co-culture of bone marrow stromal cells and chondrocytes. Zhonghua
Yi Xue Za Zhi. 84:1716–1720. 2004.(In Chinese). PubMed/NCBI
|
|
38
|
Gardner OF, Archer CW, Alini M and
Stoddart MJ: Chondrogenesis of mesenchymal stem cells for cartilage
tissue engineering. Histol Histopathol. 28:23–42. 2013.PubMed/NCBI
|
|
39
|
Park SS, Jin HR, Chi DH and Taylor RS:
Characteristics of tissue-engineered cartilage from human auricular
chondrocytes. Biomaterials. 25:2363–2369. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Smeriglio P, Lai JH, Yang F and Bhutani N:
3D Hydrogel Scaffolds for articular chondrocyte culture and
cartilage generation. J Vis Exp. Oct 7–2015.doi: 10.3791/53085.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Raghunath J, Rollo J, Sales KM, Butler PE
and Seifalian AM: Biomaterials and scaffold design: Key to
tissue-engineering cartilage. Biotechnol Appl Biochem. 46:73–84.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kisiday J, Jin M, Kurz B, Hung H, Semino
C, Zhang S and Grodzinsky AJ: Self-assembling peptide hydrogel
fosters chondrocyte extracellular matrix production and cell
division: Implications for cartilage tissue repair. Proc Natl Acad
Sci USA. 99:9996–10001. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Fisher JP, Jo S, Mikos AG and Reddi AH:
Thermoreversible hydrogel scaffolds for articular cartilage
engineering. J Biomed Mater Res A. 71:268–274. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Yasuda A, Kojima K, Tinsley KW, Yoshioka
H, Mori Y and Vacanti CA: In vitro culture of chondrocytes in a
novel thermoreversible gelation polymer scaffold containing growth
factors. Tissue Eng. 12:1237–1245. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Kaneko Y, Nakamura S, Sakai K, Kikuchi A,
Aoyagi T, Sakurai Y and Okano T: Synthesis and swelling-deswelling
kinetics of poly(N-isopropylacrylamide) hydrogels grafted with LCST
modulated polymers. J Biomater Sci Polym Ed. 10:1079–1091. 1999.
View Article : Google Scholar : PubMed/NCBI
|