Introduction
Endometriosis (EM), caused by the presence of the
active endometrium at the outer side of the uterine cavity, is a
common gynecological disease (1,2). Most of
EM lesions are located in the pelvic genital organs and the organs
adjacent to the peritoneal surface; this is referred to as pelvic
EM, of which ovarian EM is the most common type. The pathological
process of EM comprises periodic bleeding, migration of uterine
cells and their attachment to other organs. In general, EM is only
seen in women of childbearing age, mostly at the age of 25–45 years
(3,4). The major symptoms of the disease are
dysmenorrhea, chronic pelvic pain and infertility that seriously
affect the quality of life of young women (5). The incidence of EM is 10–15%, and a
significant increase has been observed in recent years (2,6).
Although EM is a benign lesion, it has a similar biological
behavior to that of malignant tumors, including invasion, distant
metastasis and spread (7,8). To date, the pathogenesis of EM has
remained to be fully elucidated. In recent years, research has
focused on the association between EM and apoptosis. An increasing
number of studies have demonstrated that spontaneous apoptosis of
endometrial cells is a key factor in maintaining the normal
structure and function of endometrial tissue, while ectopic
endometrial cells may settle in the uterine cavity and continue to
survive, which is due to a low rate of spontaneous apoptosis and
sensitivity to apoptotic signals as well as other changes in
apoptotic characteristics (9). Thus,
excessive proliferation and apoptosis-evading properties of EM
cells are considered to participate in the development of EM
(10,11).
Propofol is a commonly used intravenous anesthetic
agent, which is widely used in various types of surgery due to its
short-term effects and rapid recovery. However, increasing evidence
has demonstrated that propofol has numerous non-anesthetic effects
(12). In recent years, studies have
confirmed the anti-cancer properties of propofol, including the
repression of cell metastasis, adhesion and proliferation as well
as induction of cell apoptosis (13–15).
Thus, propofol has an important role in maintaining the balance of
cell proliferation and apoptosis, the dysregulation of which is
implicated in EM-associated processes.
To the best of our knowledge, the role of propofol
in the development of EM has not been previously reported.
Therefore, the present study aimed to investigate the role of
propofol in EM by exploring the effects of propofol on the
biological behavior of EM cells, as well as to elucidate the
underlying molecular mechanisms.
Materials and methods
Cell culture
The EM cell line CRL-7566 was obtained from the
American Type Culture Collection (Manassas, VA, USA). The cells
were grown in Dulbecco's modified Eagle's medium (Invitrogen;
Thermo Fisher Scientific, Inc., Waltham, MA, USA) containing 10%
fetal bovine serum (Gibco; Thermo Fisher Scientific, Inc.) and 1%
penicillin-streptomycin solution at 37°C in a humidified atmosphere
containing 5% CO2.
Cell treatment
Propofol was obtained from Corden Pharma Caponago
S.P.A. (Milan, Italy) and dissolved in dimethyl sulfoxide (DMSO;
Sigma-Aldrich; Merck KGaA, Darmstadt, Germany). The day before the
cell treatments, the CRL-7566 cells were seeded on 96-well plates
and then incubated under standard conditions for 12–18 h. The cells
were then treated with various concentrations of propofol (0, 1, 5
or 10 µg/ml) for specific durations. The cells in the control group
were treated with DMSO only and the final DMSO concentration was
0.2%. The cell suspension was then harvested for subsequent
analyses.
MTT assay
To detect the cell viability, an MTT assay was
applied in the present study. In brief, CRL-7566 cells were
collected, re-suspended and then re-seeded in 96-well plates
(1×104 cells/well). The cells were then treated with
different concentrations of propofol (0, 1, 5, 10 µg/ml) for 24, 48
or 72 h. Subsequently, 10 µl MTT (Sigma-Aldrich; Merck KGaA) was
added to each well, followed by incubation for 4 h at 37°C. The
medium in each well was then replaced with 150 µl DMSO. At the end
of this experiment, the optical density was read at 490 nm by using
a microplate reader. All tests were performed in triplicate.
Flow cytometric analysis
In the present study, fluorescence-assisted cell
sorting (FACS) following fluorescein isothiocyanate (FITC)-Annexin
V and propidium iodide (PI) double labeling was performed to
determine cell apoptosis in different groups by using an Annexin
V-FITC/PI Apoptosis Detection Kit (cat. no. 6592; Cell Signaling
Technology, Inc., Danvers, MA, USA). In brief, at 24 h after
treatment with propofol, the CRL-7566 cells were collected with
trypsin and then re-suspended in a binding buffer. The cells were
then labeled with Annexin V-FITC and PI according to the
manufacturer's instructions, and then incubated for 15 min without
light at room temperature. Subsequently, FACS (BD Biosciences,
Franklin Lakes, NJ, USA) was performed for flow cytometric analysis
and the percentage of apoptotic cells was calculated. All tests
were performed in triplicate.
Reverse-transcription quantitative
polymerase chain reaction (RT-qPCR)
Total RNA from the EM cells was extracted by using
TRIzol reagent (Invitrogen; Thermo Fisher Scientific, Inc.). Total
RNA (1 µg) was reversely transcribed into complementary (c)DNA by
using a Maxima First Strand cDNA Synthesis kit (cat. no. K1641;
Fermentas, Vilnius, Lithuania) according to the manufacturer's
recommended protocol. qPCR was performed using a 2X Maxima
SYBR-Green/ROX qPCR Master Mix kit (cat. no. K0221; Fermentas). The
amplification program was initial denaturation for 2 min at 95°C,
followed by 37 cycles of 30 sec at 95°C and 60 sec at 60°C. GAPDH
was used as an internal control. The primer sequences (Genscript,
Nanjing, China) were as following: FOXO1 forward,
5′-TCGTCATAATCTGTCCCTACACA-3′ and reverse,
5′-CGGCTTCGGCTCTTAGCAAA-3′; FOXO3 forward,
5′-CGGACAAACGGCTCACTCT-3′ and reverse, 5′-GGACCCGCATGAATCGACTAT-3′;
Bim forward, 5′-CATATAACCCCGTCAACGCAG-3′ and reverse,
5′-GCAGCCGCCACAAACATAC-3′; p21 forward, 5′-TAGCAGCGGAACAAGGAG-3′
and reverse, 5′-AAACGGGAACCAGGACAC-3′; p53 forward,
5′-CCACCATCCACTACAACTAC-3′ and reverse, 5′-AAACACGCACCTCAAAGC-3′;
and GAPDH forward, 5′-GAAGGTGAAGGTCGGAGTC-3 and reverse,
5′-GAAGATGGTGATGGGATTTC-3′. Relative gene expression was calculated
by using the 2−ΔΔCq method (16).
Western blot analysis
After incubation for 24 h, CRL-7566 cells were
harvested using trypsin, centrifuged and then lysed in
radioimmunoprecipitation assay buffer. The extracted total protein
was measured by using a bicinchoninic acid assay kit (Pierce;
Thermo Fisher Scientific, Inc.). Protein samples (30 µg/lane) were
resolved by 12% SDS-PAGE and then transferred to a polyvinylidene
difluoride membrane (EMD Millipore, Billerica, MA, USA). Membranes
were then washed with PBS and blocked with 5% non-fat milk for 1.5
h. Subsequently, the membranes were incubated overnight at 4°C with
the following primary antibodies: Forkhead box (FOX)O1 (cat no.
2880), FOXO3 (cat no. 2497), Bim (cat no. 2933), pro-caspase-3 (cat
no. 9665), active caspase-3 (cat no. 9664), p53 (cat no. 2527) and
p21 (cat no. 2947; all dilution, 1:1,000; Cell Signaling
Technology, Inc.), followed by incubation with anti-rabbit
immunoglobulin G horseradish peroxidase-coupled secondary
antibodies (cat no. 7074; 1:1,000; Cell Signaling Technology, Inc.)
at room temperature for 2 h. The protein bands were finally
visualized by using enhanced chemiluminescent reagent (EMD
Millipore, Billerica, MA, USA) and imaged by the ChemiDoc XRS+
System (Bio-Rad Laboratories, Inc., Hercules, CA, USA).
Statistical analysis
Statistical analysis was performed using SPSS 17.0
software (SPSS, Inc., Chicago, IL, USA). One-way analysis of
variance followed by Tukey's test or Student's t-test was used to
assess the statistical significance of differences between groups.
All values are expressed as the mean ± standard deviation.
P<0.05 was considered to indicate a statistically significant
difference.
Results
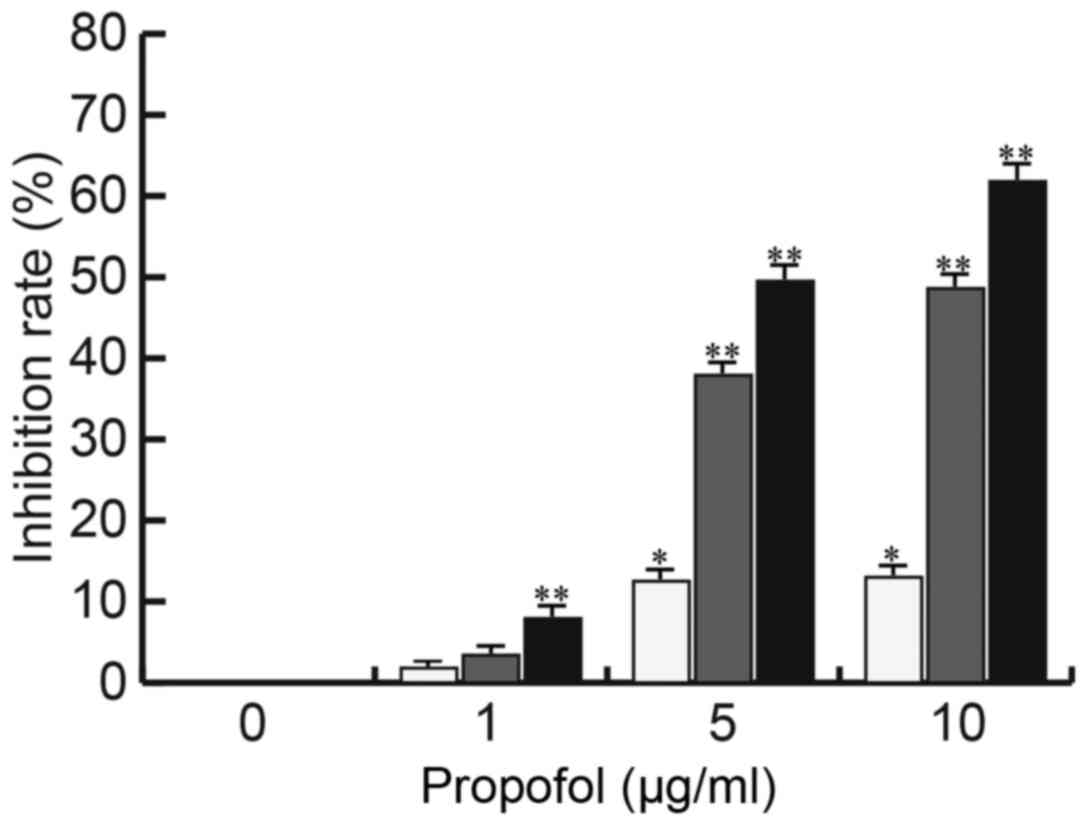
Propofol inhibits CRL-7566 cell
proliferation
The EM cell line CRL-7566 was treated with various
concentrations of propofol (0, 1, 5 or 10 µg/ml) for 24, 48 or 72 h
and the cell viability was analyzed by an MTT assay for
determination of the inhibition rate. As presented in Fig. 1, the proliferation of CRL-7566 cells
was significantly inhibited by propofol in a dose- and
time-dependent manner.
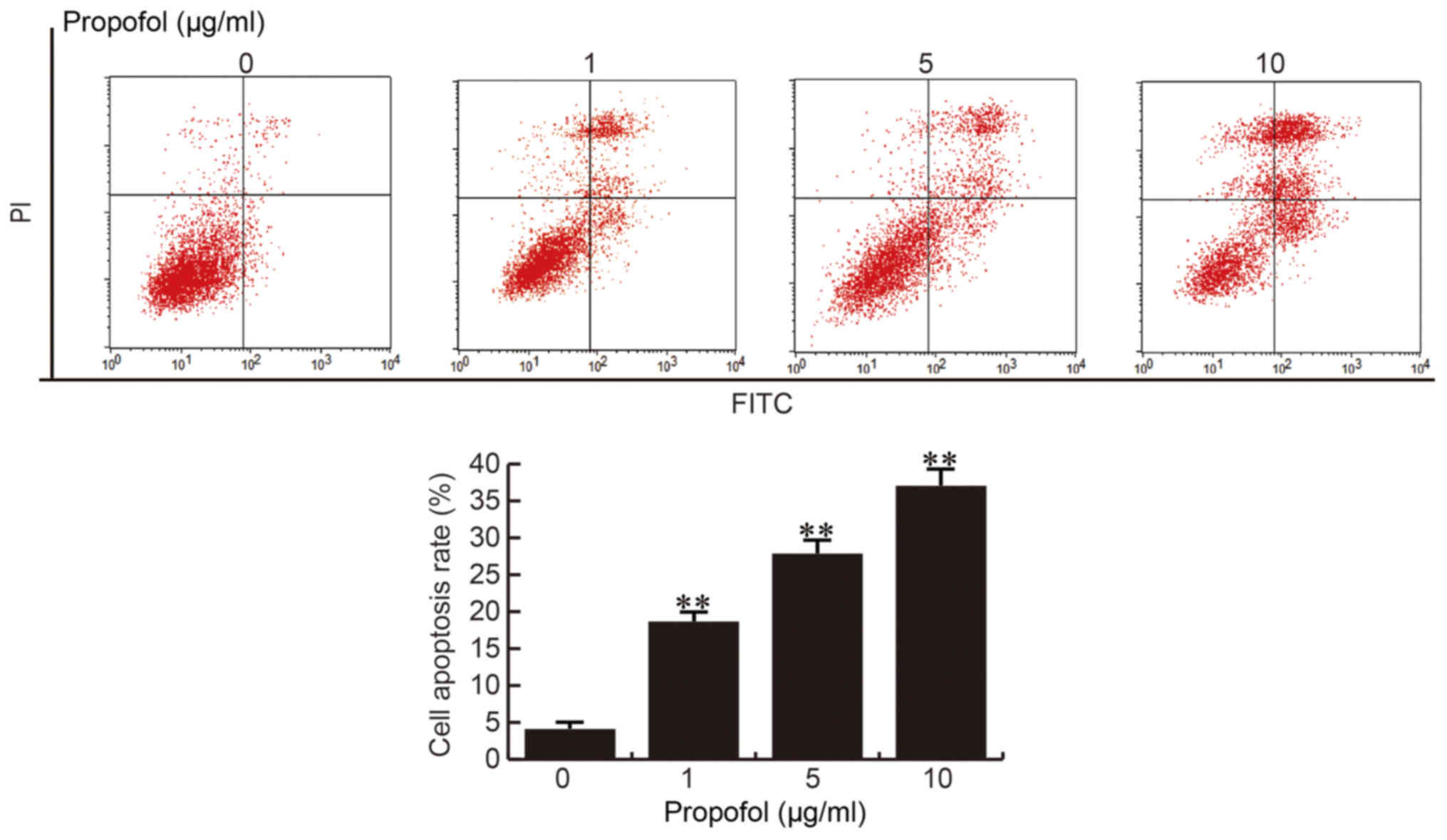
Propofol induces CRL-7566 cell
apoptosis
Following 24 h of treatment with different
concentrations of propofol (0, 1, 5 or 10 µg/ml), CRL-7566 cells
were collected and subjected to cell apoptosis analysis. The
results of the cell apoptosis assay demonstrated that compared with
the control group, the apoptotic rate of CRL-7566 cells was
significantly increased in the propofol treatment groups, and the
apoptotic rate was enhanced with the increase of the propofol
concentration (Fig. 2). These
results indicted that propofol promotes CRL-7566 cell apoptosis in
a dose-dependent manner.
Propofol enhances FOXO1, FOXO3, Bim,
pro-caspase-3 and active caspase-3 levels in CRL-7566 cells
After 24 h of treatment with different
concentrations of propofol (0, 1, 5 or 10 µg/ml), the levels of
cell proliferation- and apoptosis-associated proteins/genes were
detected by western blot and RT-qPCR analysis, respectively. It was
observed that treatment with propofol increased the protein levels
of FOXO1, FOXO3, Bim, pro-caspase-3 and active caspase-3 in
CRL-7566 cells in a dose-dependent manner (Fig. 3A). The mRNA levels of FOXO1, FOXO3
and Bim were also dose-dependently increased by propofol treatment
(Fig. 3B-D).
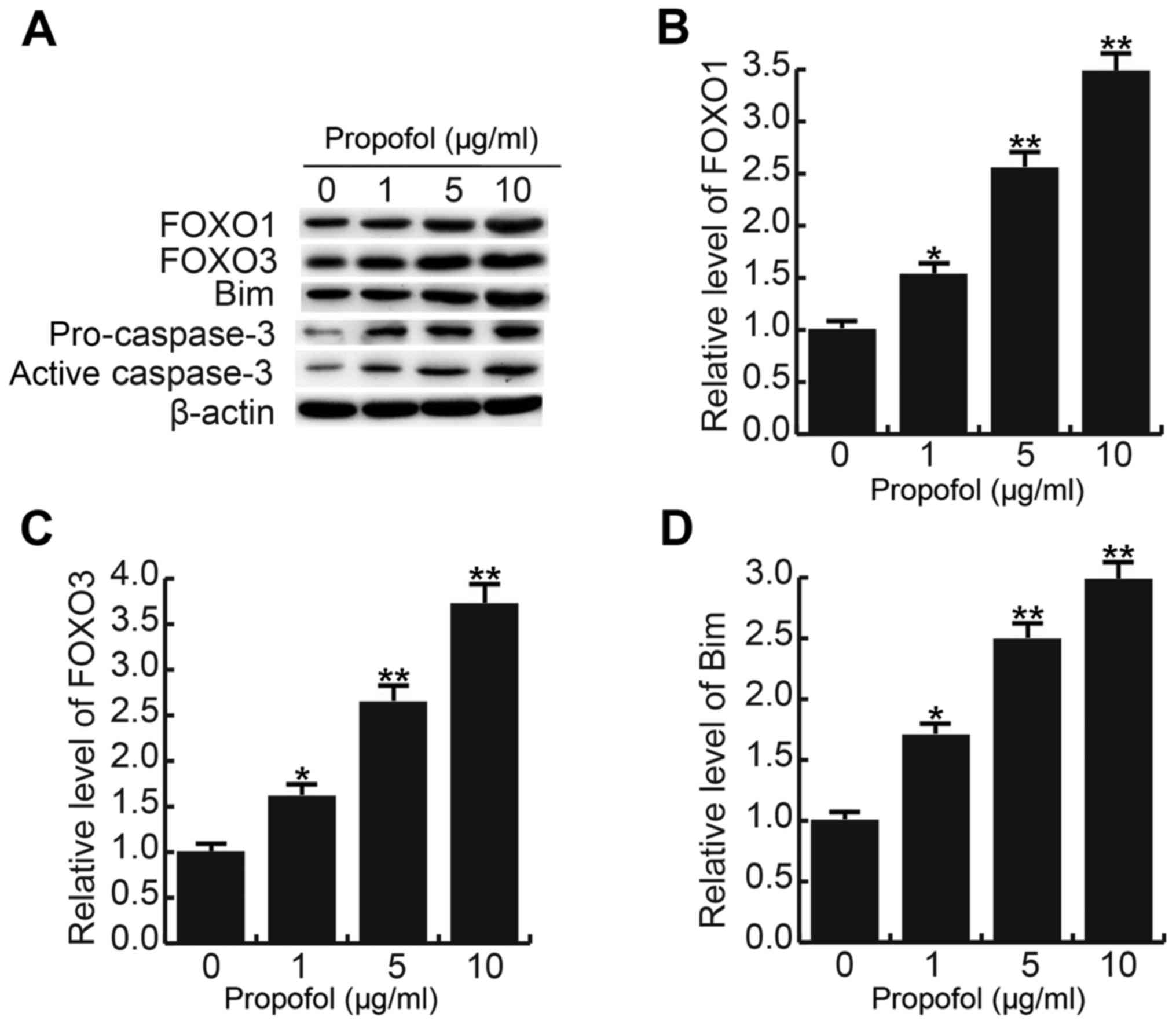 | Figure 3.Effect of propofol on FOXO1, FOXO3,
Bim, pro-caspase-3 and active caspase-3 levels in CRL-7566 cells.
After 24 h of treatment with various concentrations of propofol (0,
1, 5 or 10 µg/ml), (A) the protein levels of FOXO1, FOXO3, Bim,
pro-caspase-3 and active caspase-3 in CRL-7566 cells were
determined by western blot analysis, and (B-D) the mRNA levels of
(B) FOXO1, (C) FOXO3 and (D) Bim were determined by
reverse-transcription quantitative polymerase chain reaction.
Values are expressed as the mean ± standard deviation. *P<0.05,
**P<0.01 vs. control group. FOXO, forkhead box O. |
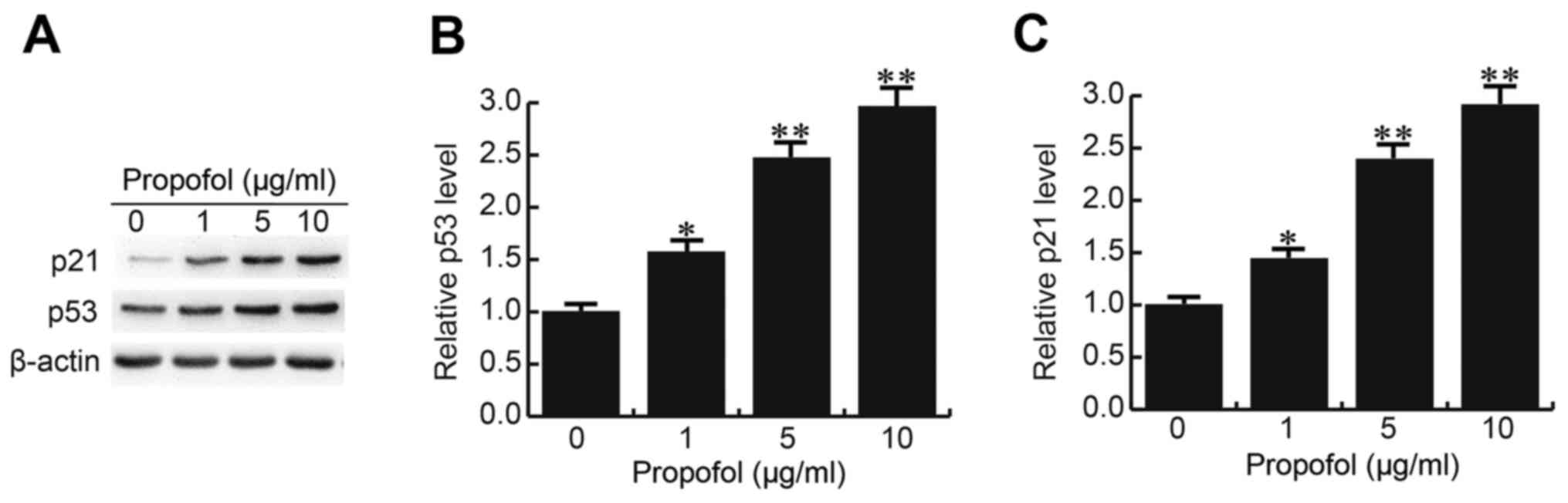
Propofol enhances p53 and p21
expression in CRL-7566 cells
p53 and p21, which were previously reported to be
downregulated in EM cells and to have critical roles in cell growth
regulation (17,18), were also assessed in the present
study. As expected, propofol increased the mRNA and protein
expression levels of p53 and p21 in CRL-7566 cells in a
dose-dependent manner (Fig. 4).
Discussion
EM, a prevalent and complex gynecological disease,
affects the health and life quality of ~10% of women of
reproductive age (19). Multiple
factors may contribute to the development and progression of EM,
including environmental factors, the immune response and hormones
(20–22). EM is benign; however, it has the
characteristics of malignant tumors, including metastasis,
infiltration and recurrence (7,8). To
date, the treatment outcomes of EM have remained unsatisfactory,
and the pathogenesis of EM has not been fully elucidated (23). The association between apoptosis and
EM has attracted the attention of numerous researchers (9–11). Cell
apoptosis, also known as programmed cell death, is required for the
maintenance of tissue homeostasis, and is a type of cell death of
independent order that is controlled by specific genes (24). Cell apoptosis has an important role
in the upstate and steady-state maintenance of normal tissue as
well as the prevention and treatment of diseases (25). Following its initiation, the
occurrence of cell apoptosis is achieved by transduction of a
variety of cell apoptosis signals and is controlled by
apoptosis-associated genes (26). In
recent years, the association between EM and apoptosis has received
increasing attention from researchers (27).
Propofol is an intravenous sedative-hypnotic agent,
which is employed in the clinic to induce and sustain anesthesia.
Various studies have suggested that propofol prevents cancer
procession through directly and indirectly inhibiting cancer cell
viability and proliferation by facilitating cell apoptosis
(28–30). Therefore, propofol has critical roles
in regulating the balance of cell proliferation and apoptosis. To
date, the effect of propofol on EM has remained elusive. Thus, the
present study investigated the potential role of propofol in the
pathogenesis of EM. It was revealed that propofol inhibited the
proliferation of the EM cell line CRL-7566 in a dose- and
time-dependent manner, and cell apoptosis was dose-dependently
induced by propofol treatment. These results indicated that
propofol may have a protective role in EM.
To further explore the underlying mechanism of the
inhibition of cell proliferation and promotion of cell apoptosis
caused by propofol, the levels of FOXO1, FOXO3, Bim, pro-caspase-3,
active caspase-3, p53 and p21 in CRL-7566 cells were determined.
FOXO participates in the growth and apoptosis of cells through
directly promoting the expression of FOXO3a-dependent apoptotic
protein Bim (31,32) and the activation of caspase family
proteins (33). In addition, p53 and
p21, which have important roles in the regulation of cell apoptosis
and have been reported to be downregulated in EM (17,18),
were analyzed in the present study. The results demonstrated that
propofol treatment significantly increased the levels of FOXO1,
FOXO3, Bim, pro-caspase-3, active caspase-3, p53 and p21,
indicating that propofol exerts its roles in EM via affecting the
expression levels and activation of cell growth- and
apoptosis-associated genes/proteins.
In conclusion, to the best of our knowledge, the
present study was the first to reveal that propofol had a
protective role in EM though inhibiting cell proliferation and
inducing cell apoptosis via regulating the expression/activation of
multiple cell proliferation- and apoptosis-associated
genes/proteins in EM cells. The results provide a scientific basis
for the development of novel clinical treatments for EM.
Acknowledgements
The authors would like to thank Professor Xiuping Lv
and Professor Zhaori Chen (Department of Gynecology, Affiliated
Hospital of Weifang Medical University, Weifang, China), and
Professor Kechang Huang (Department of Anesthesiology, Affiliated
Hospital of Weifang Medical University, Weifang, China) for their
guidance and assistance.
Funding
No funding was received.
Availability of data and materials
The analyzed data sets generated during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SF and YS collaborated to design the study, access
and analysis the data, interpret the results, and write the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nyholt DR, Low SK, Anderson CA, Painter
JN, Uno S, Morris AP, MacGregor S, Gordon SD, Henders AK, Martin
NG, et al: Genome-wide association meta-analysis identifies new
endometriosis risk loci. Nat Genet. 44:1355–1359. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cramer DW and Missmer SA: The epidemiology
of endometriosis. Ann NY Acad Sci. 955:11–22; discussion 34–36,
396–406. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Benagiano G, Habiba M and Brosens I: The
pathophysiology of uterine adenomyosis: An update. Fertil Steril.
98:572–579. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Maheshwari A, Gurunath S, Fatima F and
Bhattacharya S: Adenomyosis and subfertility: A systematic review
of prevalence, diagnosis, treatment and fertility outcomes. Hum
Reprod Update. 18:374–392. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Giudice LC and Kao LC: Endometriosis.
Lancet. 364:1789–1799. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tandrasasmita OM, Sutanto AM, Arifn PF and
Tjandrawinata RR: Anti-inflammatory, antiangiogenic, and
apoptosis-inducing activity of DLBS1442, a bioactive fraction of
Phaleria macrocarpa, in a RL95-2 cell line as a molecular model of
endometriosis. Int J Womens Health. 7:161–169. 2015.PubMed/NCBI
|
|
7
|
Kodaman PH: Current strategies for
endometriosis management. Obstet Gynecol Clin North Am. 42:87–101.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Grimstad FW and Carey E: Periclitoral
endometriosis: The dilemma of a chronic disease invading a rare
location. J Minim Invasive Gynecol. 22:684–686. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Agic A, Djalali S, Diedrich K and Hornung
D: Apoptosis in endometriosis. Gynecol Obstet Invest. 68:217–223.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nasu K, Yuge A, Tsuno A, Nishida M and
Narahara H: Involvement of resistance to apoptosis in the
pathogenesis of endometriosis. Histol Histopathol. 24:1181–1192.
2009.PubMed/NCBI
|
|
11
|
Nishida M, Nasu K, Ueda T, Fukuda J, Takai
N and Miyakawa I: Endometriotic cells are resistant to
interferon-gamma-induced cell growth inhibition and apoptosis: A
possible mechanism involved in the pathogenesis of endometriosis.
Mol Hum Reprod. 11:29–34. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Vasileiou I, Xanthos T, Koudouna E, Perrea
D, Klonaris C, Katsargyris A and Papadimitriou L: Propofol: A
review of its non-anaesthetic effects. Eur J Pharmacol. 605:1–8.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang L, Wang N, Zhou S, Ye W, Jing G and
Zhang M: Propofol induces proliferation and invasion of gallbladder
cancer cells through activation of Nrf2. J Exp Clin Cancer Res.
31:662012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang ZT, Gong HY, Zheng F, Liu DJ and Yue
XQ: Propofol suppresses proliferation and invasion of gastric
cancer cells via downregulation of microRNA-221 expression. Genet
Mol Res. 14:8117–8124. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang ZT, Gong HY, Zheng F, Liu DJ and Dong
TL: Propofol suppresses proliferation and invasion of pancreatic
cancer cells by upregulating microRNA-133a expression. Genet Mol
Res. 14:7529–7537. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Agui T, McConkey DJ and Tanigawa N:
Comparative study of various biological parameters, including
expression of survivin, between primary and metastatic human
colonic adenocarcinomas. Anticancer Res. 22:1769–1776.
2002.PubMed/NCBI
|
|
18
|
Palazzo JP, Mercer WE, Kovatich AJ and
McHugh M: Immunohistochemical localization of p21(WAF1/CIP1) in
normal, hyperplastic, and neoplastic uterine tissues. Hum Pathol.
28:60–66. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Giudice LC: Clinical practice.
Endometriosis. N Engl J Med. 362:2389–2398. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Painter JN, Anderson CA, Nyholt DR,
Macgregor S, Lin J, Lee SH, Lambert A, Zhao ZZ, Roseman F, Guo Q,
et al: Genome-wide association study identifies a locus at 7p15.2
associated with endometriosis. Nat Genet. 43:51–54. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Simpson JL, Elias S, Malinak LR and
Buttram VC Jr: Heritable aspects of endometriosis. I. Genetic
studies. Am J Obstet Gynecol. 137:327–331. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Anger DL and Foster WG: The link between
environmental toxicant exposure and endometriosis. Front Biosci.
13:1578–1593. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Vercellini P, Viganò P, Somigliana E and
Fedele L: Endometriosis: Pathogenesis and treatment. Nat Rev
Endocrinol. 10:261–275. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tower J: Programmed cell death in aging.
Ageing Res Rev. 23:90–100. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Favaloro B, Allocati N, Graziano V, Di
Ilio C and De Laurenzi V: Role of apoptosis in disease. Aging
(Albany NY). 4:330–349. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Fuchs Y and Steller H: Live to die another
way: Modes of programmed cell death and the signals emanating from
dying cells. Nat Rev Mol Cell Biol. 16:329–344. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gogacz M, Gałczyński K, Wojtaś M, Winkler
I, Adamiak A, Romanek-Piva K, Rechberger T and Kotarski J:
Fas-related apoptosis of peritoneal fluid macrophages in
endometriosis patients: Understanding the disease. J Immunol Res.
2017:31753942017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sun C, Li N, Yang Z, Zhou B, He Y, Weng D,
Fang Y, Wu P, Chen P, Yang X, et al: miR-9 regulation of BRCA1 and
ovarian cancer sensitivity to cisplatin and PARP inhibition. J Natl
Cancer Inst. 105:1750–1758. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Huang H, Benzonana LL, Zhao H, Watts HR,
Perry NJ, Bevan C, Brown R and Ma D: Prostate cancer cell
malignancy via modulation of HIF-1α pathway with isoflurane and
propofol alone and in combination. Br J Cancer. 111:1338–1349.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Mammoto T, Mukai M, Mammoto A, Yamanaka Y,
Hayashi Y, Mashimo T, Kishi Y and Nakamura H: Intravenous
anesthetic, propofol inhibits invasion of cancer cells. Cancer
Lett. 184:165–170. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gilley J, Coffer PJ and Ham J: FOXO
transcription factors directly activate bim gene expression and
promote apoptosis in sympathetic neurons. J Cell Biol. 162:613–622.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Stahl M, Dijkers PF, Kops GJ, Lens SM,
Coffer PJ, Burgering BM and Medema RH: The forkhead transcription
factor FoxO regulates transcription of p27Kip1 and Bim in response
to IL-2. J Immunol. 168:5024–5031. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Brunet A, Bonni A, Zigmond MJ, Lin MZ, Juo
P, Hu LS, Anderson MJ, Arden KC, Blenis J and Greenberg ME: Akt
promotes cell survival by phosphorylating and inhibiting a Forkhead
transcription factor. Cell. 96:857–868. 1999. View Article : Google Scholar : PubMed/NCBI
|