Introduction
Temporal lobe epilepsy (TLE) is the most common form
of partial epilepsy in humans (40–60%) and in ~30% of patients it
is refractory to treatment and drug resistance emerges (1). A randomized clinical trial has
demonstrated that surgery is superior to prolonged drug treatment
for patients with refractory TLE (2). However, surgical treatment remains
unsuccessful in providing a seizure-free outcome in 20–30% of
patients with TLE (3). The
coexistence of hippocampal sclerosis (HS) and temporal neocortical
lesions, including focal cortical dysplasia (FCD), vascular
malformations and benign primary brain tumors, is termed dual
pathology, which may be a major cause of surgical failure in
patients with TLE (4–7).
A majority of epileptic cases with dual pathology
are poor surgical candidates due to unclear diagnosis leading to
failure of complete resection of the epileptogenic zone (5). Clear and complete electroencephalogram
(EEG) and magnetic resonance imaging (MRI) evidence for each dual
pathological lesion is rare. Of note, EEG and MRI-based diagnosis
of one epileptogenic lesion typically guides the diagnosis of other
lesions (8). Several studies have
indicated that the surgical outcome for patients with neocortical
epilepsy were less satisfactory compared with patients with mesial
temporal lobe epilepsy (mTLE), a type of epilepsy originates from
mesial temporal lobe structure, including the hippocampus and
amygdala (9–12). HS is the most common underlying
pathological cause of mTLE (~60–80%), and in a majority of cases,
MRI findings of unilateral HS predict a favorable prognosis
(13,14). Additionally, several reports have
clarified that neocortical lesions, including FCD, are associated
with early seizure onset, high seizure frequency and poor
postsurgical outcomes (4,15,16).
Resection of the mesial temporal lobe instead of the neocortical
lesion in patients with dual pathology is therefore favored,
particularly when mTLE foci has complete EEG and MRI evidence
(8). In other cases, surgical
decisions are more difficult.
The present study investigated the surgical outcome
for patients with temporal lobe dual pathology in the absence of
matched EEG and MRI findings. While surgical indication of
resecting both lesions is not sufficient, prognostic implications
of the severity of pathology, clinical factors, surgical procedures
and the results of presurgical diagnostic modalities were examined,
aiming to provide a novel surgical strategy for similar cases.
Materials and methods
Patients
Data of 24 patients with TLE and dual pathology
presurgically verified by radiologic and EEG evidence was reviewed
retrospectively. A total of 14 females and 10 males participated in
the study (mean age, 26.0±8.5 years). Patients were surgically
treated at the Epilepsy Center of Liao Ning Province, The Second
Hospital of Dalian Medical University (Liaoning, China) between
January 2012 and December 2015. Selected patients exhibited a
coexistence of HS and a temporal neocortical lesion, with either
radiologic or EEG proof. Patients with other causes of seizure,
including brain trauma, encephalitis and meningitis, or diagnosed
with idiopathic epilepsy were excluded. Clinical features,
including age at onset, age at surgery, duration of epilepsy,
seizure frequency, preoperational EEG and radiologic data, surgical
strategy, postsurgical pathological diagnosis and outcome were
examined (Table I). All patients
were followed-up for ≥2 years. The present study was approved by
the Ethics Committee of The Second Hospital of Dalian Medical
University (Liaoning, China).
 | Table I.Clinical characteristics of 24
patients with dual pathology diagnosis. |
Table I.
Clinical characteristics of 24
patients with dual pathology diagnosis.
| Sex | Age of onset
(years) | Duration of epilepsy
(years) | MRI findings | EEG findings | Pathological
findings | Engel
classification |
|---|
| Male | <1 | 50 | HS+FCD | mTLE+FO | HS+FCD | I |
| Female | 6 | 18 | HS+VM | mTLE+FO | HS+VM | II |
| Male | 18 | 22 | HS+FCD | mTLE | HS+FCD | I |
| Male | 13 | 7 | HS+FCD | mTLE | HS+FCD | II |
| Female | 15 | 2 | HS+tumor | mTLE | HS+tumor | II |
| Female | 12 | 22 | HS+FCD | mTLE | HS+FCD | I |
| Female | 8 | 17 | HS+FCD | mTLE+FO | HS+FCD | I |
| Male | 17 | 15 | HS+FCD | mTLE+FO | HS+FCD | I |
| Male | 14 | 24 | HS+tumor | mTLE | HS+tumor | I |
| Female | 7 | 11 | HS+FCD | mTLE | HS+FCD | II |
| Male | 11 | 6 | HS+FCD | NC | HS+FCD | II |
| Female | 13 | 10 | HS+FCD | FO | HS+FCD | I |
| Female | 23 | 21 | HS+VM | NC | HS+VM | I |
| Male | 15 | 20 | HS+FCD | FO | HS+FCD | II |
| Male | 19 | 16 | HS+FCD | NC | HS+FCD | I |
| Male | 22 | 22 | HS+VM | N | VM | II |
| Female | 18 | 9 | HS+FCD | N | FCD | II |
| Male | 11 | 14 | HS+FCD | Wide-spread
discharges | FCD | III |
| Female | 17 | 21 | HS+tumor | N | Tumor | I |
| Female | 11 | 17 | HS+FCD | Wide-spread
discharges | FCD | II |
| Female | 6 | 19 | HS+FCD | Wide-spread
discharges | FCD | III |
| Female | 8 | 20 | VM | mTLE | VM | II |
| Female | 10 | 21 | FCD | mTLE | FCD | III |
| Female | 9 | 25 | Tumor | mTLE+FO | Tumor | II |
MRI
All patients underwent a 3.0-T cerebral MRI scan
(MAGNETOM Skyra, Siemens Healthineers, Erlangen, Germany). MRI
sequences included T1-weighted and T2-weighted axial, sagittal and
coronal images at a section thickness of 1.5 mm. T2-weighted
fluid-attenuated inversion recovery sequences were further obtained
at an angle perpendicular to the long axis of the hippocampus.
EEG monitoring
Long-term scalp V-EEG was performed with additional
anterior temporal electrodes placed on the scalp of patients. A
total of 13 patients did not receive a conclusive diagnosis from
V-EEG. Therefore, electrocorticography was performed in these
patients with a combination of subdural grids and strips on the
cortex of the patient. Intracranial electrodes were installed in
various combinations, always directed from the lateral neocortex to
the para-hippocampal gyrus, to monitor mesial temporal epileptiform
discharges, enabling to locate the epileptogenic onset. For
patients with FCD or a temporal tumor identified by MRI scans, and
an unclear on-scalp EEG, subdural electrodes were placed over the
area of the lesion. A localizing pattern of ictal onset/interictal
spike was defined by monitoring the electrodes of an epileptogenic
lobe or two adjacent electrodes.
Groups and surgical strategies
Based on presurgical evaluations, including clinical
symptoms, MRI scans and EEG results, groups were divided and
surgical strategies and resection margins were defined accordingly
(Table II). In group 1, HS was
confirmed by MRI and EEG and a temporal lesion was detected by MRI
but not by EEG. An anterior temporal lobectomy and the resection of
the temporal neocortical lesion were performed. Anterior temporal
lobectomy was defined as the removal of medial structures,
including the amygdala, hippocampus and parahippocampal gyrus. In
group 2, HS was detected by MRI. EEG revealed epileptic discharges
in the anterior temporal lobe (ATL) and was unable to locate the
onset zone to the hippocampus without depth electrodes. A temporal
lesion around the hippocampus was detected by MRI. The surgical
strategy was to resect the neocortical lesion and the hippocampus
to completely remove the potential epileptogenic focus. In group 3,
HS was detected by MRI, with multiple epileptic onset or widespread
epileptic discharges detected on the EEG. A temporal lesion was
detected by MRI. A resection of the temporal lesion was performed
and ATL, including the hippocampus, was spared. In group 4, HS was
unclear on the MRI, but the epileptic onset was captured by the
EEG. A distinct temporal lesion was detected by MRI. The surgical
strategy was to resect the temporal lesion, following a discussion
with and consensus from the patients.
| Table II.Pathology of resection-based
grouping. |
Table II.
Pathology of resection-based
grouping.
| A, Group 1 |
|---|
|
|---|
| Variable | Hippocampal
sclerosis | Temporal
lesion |
|---|
| Analytical
method |
|
|
|
MRI | + | + |
|
EEG | + | N |
| Surgical
strategy | Resection of ATL
and temporal lesion |
|
|
| B, Group
2 |
|
|
Variable | Hippocampal
sclerosis | Temporal
lesion |
|
| Analytical
method |
|
|
|
MRI | + | + |
|
EEG | NC (limited to
ATL) | N |
| Surgical
strategy | Resection of ATL
and temporal lesion |
|
|
| C, Group
3 |
|
|
Variable | Hippocampal
sclerosis | Temporal
lesion |
|
| Analytical
method |
|
|
|
MRI | + | + |
|
EEG | NC (multiple onsets
or wide-spread discharges) | N |
| Surgical
strategy | Resection of the
temporal lesion |
|
|
| D, Group
4 |
|
|
Variable | Hippocampal
sclerosis | Temporal
lesion |
|
| Analytical
method |
|
|
|
MRI | N | + |
|
EEG | + | N |
| Surgical
strategy | Resection of the
temporal lesion |
|
Notably, there was a concern that the resection of
the bilateral hippocampus may be associated with unexpected memory
and emotional dysfunction following surgery, which may be
considered as postoperative complication. Therefore, only with
complete MRI and EEG evidence confirming that the hippocampus was
responsible for the epileptic onset was the hippocampus
resected.
Neuropathological examination
Postsurgical pathological diagnoses of temporal
lesions, including vascular malformations and benign primary brain
tumors, were performed according to the WHO classification of
tumors of the central nervous system (17). Diagnosis of the severity and
classification of FCD was based on standards described by Palmini
et al (18) (Table III).
| Table III.Diagnosis criteria of FCD according
to Palmini's classification. |
Table III.
Diagnosis criteria of FCD according
to Palmini's classification.
| Classification | Pathologic
findings |
|---|
| mMCD I | Ectopically placed
neurons in cortex molecular layer only |
| mMCD II | Ectopically placed
neurons outside of cortex molecular layer only |
| FCD 1A | Isolated
architectural abnormalities (dyslamination) |
| FCD 1B | Additional immature
or giant neurons |
| FCD 2A | Presence of
dysmorphic neurons |
| FCD 2B | Additional balloon
cells |
Postoperative follow-up
Seizure-free was defined as patients receiving
antiepileptic treatments with no seizures and EEG abnormalities for
≥2 years (4). All patients were
followed-up for 24–36 months. Follow-up data were collected
annually in the subsequent years and included information regarding
epilepsy attacks, antiepileptic drugs taken, neuroimaging and EEG
monitoring. The mean follow-up duration was 30.7±1.8 months and
median follow-up time was 33 months (range, 24–36 months). Surgical
outcome was classified according to the Engel classification
(4): (Ia) Completely seizure-free;
(I) seizure-free, or auras or convulsions with drug withdrawal
only; (II) rare seizures (<2 seizures/year or >90% seizure
reduction); (III) reduction of seizure frequency >75%; and (IV)
reduction of seizure frequency <75%.
Statistical tests
All statistical analyses, including the clinical
characteristics of the seizure-free group with the non-seizure-free
group, were performed using the χ2 test. All analyses
were conducted using SPSS version 12.0 (SPSS, Inc., Chicago, IL,
USA) and STATA version 9.2 (Stata Corp LP, College Station, TX,
USA). P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics and surgical
outcomes
Between January 2012 and December 2015, a total of
24 patients were diagnosed and underwent surgery for dual pathology
due to HS and temporal lesions, including FCD or benign tumors, at
the Epilepsy Center of Liao Ning Province, The Second Hospital of
Dalian Medical University (Liaoning, China). Patients were
followed-up for 24–36 months postoperatively and all data were
analyzed retrospectively. Among the patients were 14/24 (58.3%)
females and 10/24 (41.7%) were males, with a mean age of 26.0±8.5
years (range, 17–51 years) at time of surgery. Mean age at seizure
onset was 12.7±1.1 years (range, <1-23 years) and the mean
interval between seizure onset and surgery was 17.8±1.9 years
(range, 2–50 years).
According to the postsurgical follow-up data, 10/24
(41.7%) patients were seizure-free, while 14/24 (58.3%) patients
did not achieve this outcome.
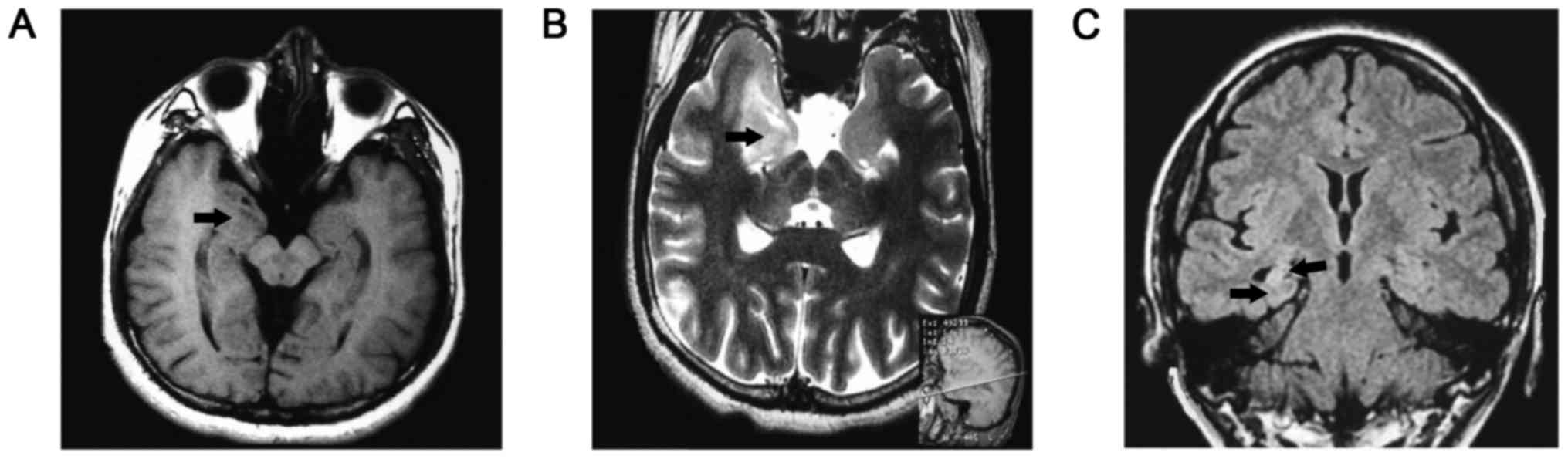
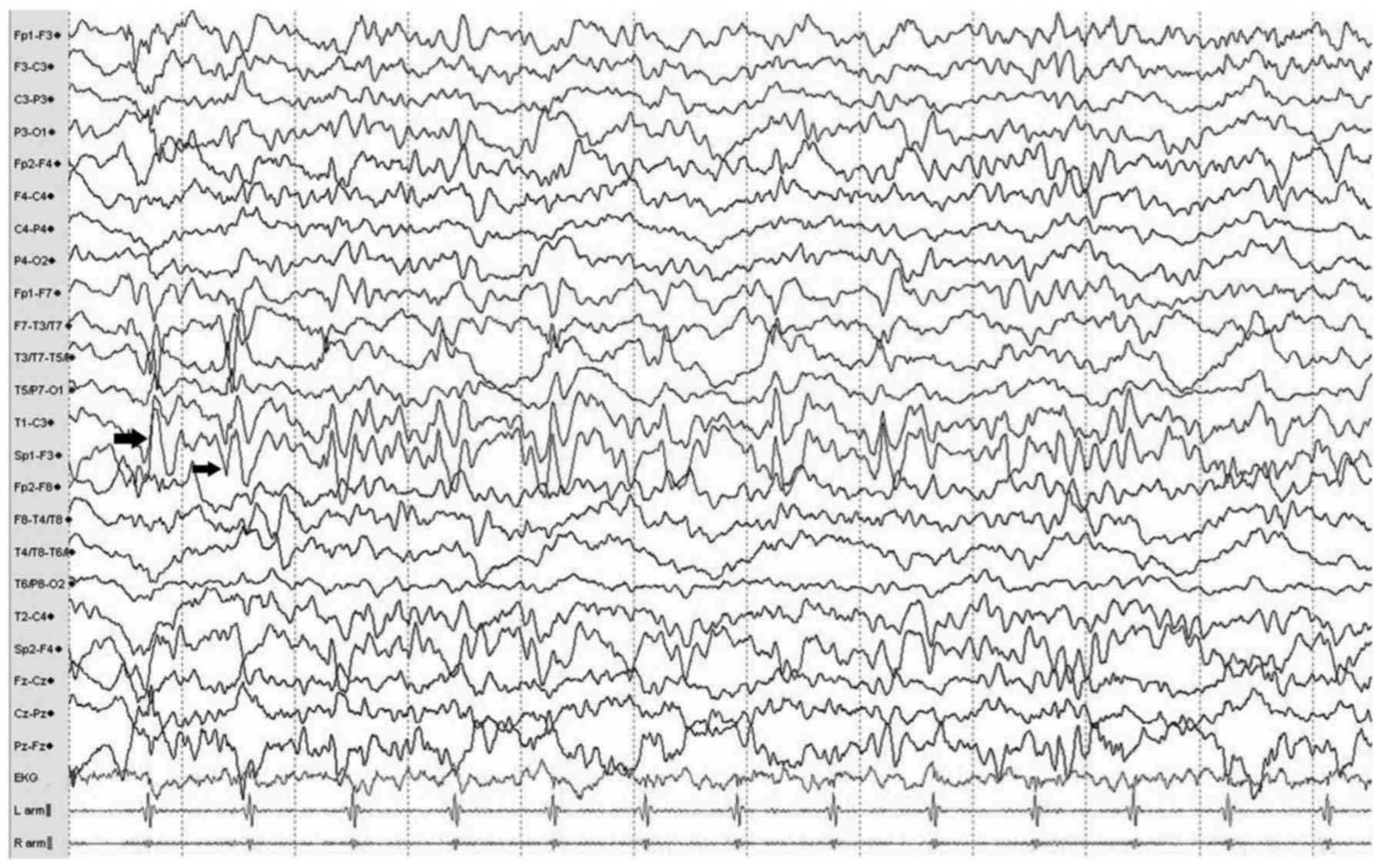
Typical MRI findings of dual pathology lesions,
including hippocampal sclerosis and neocortical malformation, were
located in the right temporal lobe (in Fig. 1) and multiple continuous slowing
epileptic discharges from the left anterior temporal electrodes,
indicating a potential onset zone located in hippocampus, are
presented in the EEG (Fig. 2).
Analysis of surgical outcomes based on
patient characteristics
Data representing the surgical outcomes and patient
characteristics were analyzed and suggested that the male/female
ratio, age of onset, duration of epilepsy and seizure frequency
were not associated with postsurgical outcome (Table IV).
| Table IV.Analysis of surgical outcomes based
on patient characteristics. |
Table IV.
Analysis of surgical outcomes based
on patient characteristics.
| Variable | Seizure-free | Not
seizure-free | P-value |
|---|
| Male/female | 5/5 | 5/9 | 0.21 |
| Age of onset
(years) | 13.5±1.7 | 11.6±1.3 | 0.25 |
| Duration of
epilepsy (years) | 21.9±3.4 | 15.0±1.8 | 0.18 |
| Resection of
FCD | 7/16 (43.7%) | 9/16 (56.0%) | 0.12 |
| Resection of
HS | 9/15 (60.0%) | 6/15 (40.0%) | 0.04 |
| Complete resection
of dual pathology | 9/15 (60.0%) | 6/15 (40.0%) | 0.04 |
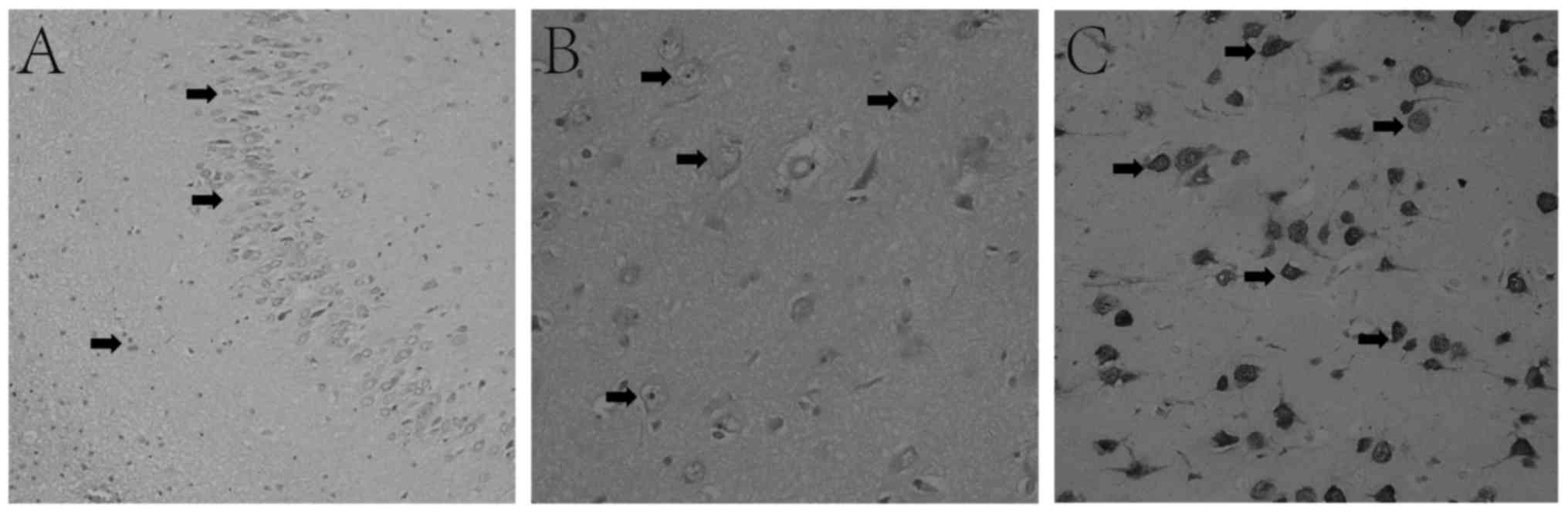
Pathological diagnosis revealed 16/24 (66.7%) cases
of FCD. Hippocampal resection was performed in 15/24 (62.5%)
patients, which was considered to be associated with a higher
chance of becoming seizure-free (44% vs. 60% for FCD vs.
hippocampal resection). Pathological findings of temporal lobe
lesions are presented as hippocampal sclerosis (Fig. 3A), FCD (Fig. 3B) and ganglioma (Fig. 3C).
A complete resection of the potential epileptogenic
area was performed in 15/24 (62.5%) patients. A total of 9/24
(37.5%) patients did not receive complete resection and the
hippocampus was spared due to a lack of either MRI abnormality or
corresponding ictal discharges in the EEG.
Statistics of surgical strategy and
outcomes
According to the presurgical evaluation, patients
were divided into four groups (Table
II). Patients of group 1, with explicit evidence on MRI and EEG
for HS and another temporal lesion on MRI scan, received complete
resection of the abnormalities and exhibited a significantly better
outcome compared with groups 3 (60.0% vs. 11.1%; P=0.03) and 4
(60.0% vs. 0%; P=0.01; Table V).
Patients of group 2 further had a significantly better chance to
become seizure-free compared with group 3 (60.0% vs. 11.1%; P=0.03)
and 4 (60.0% vs. 0%; P=0.01), which may be associated with the
resection of an increased amount of the potential epileptogenic
area. The association of the surgical strategy and patients classed
as groups 3 and 4 was not determined due to the small sample
numbers. However, it was suggested that group 3 had a significantly
increased chance of becoming seizure-free compared with group 4
(16.7% vs. 0%; P=0.02). Furthermore, EEG findings of epileptic
discharges may be important for the decision of resecting,
considering that patients of group 3 exhibited EEG abnormalities
while patients of group 4 did not.
| Table V.Statistics of surgical strategy and
outcomes. |
Table V.
Statistics of surgical strategy and
outcomes.
| Surgical
strategy | Cases (n) | Seizure-free
(n) | Seizure-free
(%) |
|---|
| Dual pathology
resection | 15 | 9 | 60.0 |
| Group
1 | 10 | 6 | 60.0 |
| Group
2 | 5 | 3 | 60.0 |
| Temporal lesion
resection | 9 | 1 | 11.1 |
| Group
3 | 6 | 1 | 16.7 |
| Group
4 | 3 | 0 | 0 |
Discussion
HS is frequently associated with neocortical
lesions, including FCD (5).
Coexistence of HS with another lesion is a well-known phenomenon
that is defined as dual pathology (8). There are various explanations for the
pathogenesis of dual pathology, including the secondary development
of HS from seizures induced by FCD or seizures resulting from the
combined effect of HS and FCD (19–22).
Another study suggested that according to EEG findings, there was
no epileptic discharge spreading between the hippocampus and the
extra-temporal lobe, which may indicate an association between the
pathogenic mechanisms during embryogenesis and early development
instead of epileptic pathways between them (23). Regarding therapy, it has been widely
accepted that surgery is a beneficial solution for patients with
epilepsy and dual pathology (8).
However, the demarcation of resection and the association with or
independence from epilepsy is still debated (11). Salanova et al (6) claimed that the complete resection of
the dual pathology lesions was associated with an improved outcome.
A total of 70.2% of the patients with complete resection were
seizure-free and 21.6% had rare seizure attacks; 30–60% of patients
with TLE achieved Engel class I (1).
Patients that only received a hippocampal resection suffered from
frequent seizure attacks and are described as Engel class III and
IV (6). Li et al (24) published a study that included 38
patients with dual pathology and 3 patients that underwent two
surgical procedures. Based on the location of resection, the
outcome of three groups, defined as simple lesion resection,
hippocampus resection and dual pathology complete resection, were
compared. Following a 37-month follow-up, outcome analysis reported
12.5, 20.0 and 73.0% of patients, respectively, as
seizure-free.
In the present study, 15 patients underwent complete
resection of dual pathology and 9 of these patients were
seizure-free (60%) post surgery, which was similar to previous
reports (6,22). It was further demonstrated that
improved outcomes may be achieved when patients receive a complete
resection of the neocortical lesion and HS compared with the
resection of the neocortical lesion alone (60.0 vs. 11.1%).
The sensitivity of MRI scans and EEG examinations
remained problematic as these features hold the key for the
diagnosis of dual pathology and establishing a surgical strategy is
usually difficult as a result of incomplete evidence for both
lesions. The hippocampus may likely be associated with epilepsy and
is the preferred target of resection for surgeons. The present
study suggested that, compared with patients who had EEG and
MRI-based proof for dual pathology, a satisfactory surgical
outcome, classification as Engel class I, was still achieved in
patients whose EEG diagnosis was not convincing, yet their
dysplastic tissue and hippocampus were still removed together
(Group 1 vs. 2; 60% vs. 60%). This outcome was based on the
condition that the resected areas had to be near each other on the
MRI scan, even if the ictal epileptic attack revealed by EEG was
unable to differentiate the mesial hippocampus and lateral
neocortex due to the insufficient depth of the electrodes. When
comparing patients with dual pathology lesion resection with
patients who had the temporal lesion removed but the hippocampus
was spared, an improved prognosis was suggested (60.0 vs. 11.1%).
However, the decision of resection of dual pathology remains
problematic without sufficient proof that can confine epileptic
onset to the ATL (mesial or lateral) or if there were only wide
spread epileptic discharges observed in the EEG. The concern for
potential postsurgical emotional or memory dysfunctions due to
hippocampus resection remains a priority.
In conclusion, in patients with TLE the resection of
all lesions had an improved outcome. However, without complete
evidence for dual pathology, establishing a surgical strategy may
still be possible. Locating the lesions using MRI scans and EEG
monitoring may be the key factors in the decision of lesion
removal.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KY made substantial contributions to conception and
design of study. LL collected, analyzed and interpreted patients'
data. YQS analyzed patient data and was a major contributor in
writing the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This research was approved by the Ethical Committee
of The Second Hospital of Dalian Medical School (Liaoning, China).
The patients or parents provided written informed consent for the
publication of any associated data and accompanying images. No
identifying information of patients was included in this
manuscript.
Patient consent to publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Stafstrom CE and Carmant L: Seizures and
epilepsy: An overview for neuroscientists. Cold Spring Harb
Perspect Med. 5:a0224262015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wiebe S, Blume WT, Girvin JP and Eliasziw
M: Effectiveness and Efficiency of Surgery for Temporal Lobe
Epilepsy Study Group: A randomized, controlled trial of surgery for
temporal-lobe epilepsy. N Engl J Med. 345:311–318. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Harroud A, Bouthillier A, Weil AG and
Nguyen DK: Temporal lobe epilepsy surgery failures: A review.
Epilepsy Res Treat. 2012:2016512012.PubMed/NCBI
|
|
4
|
Engel J Jr, Wiebe S, French J, Sperling M,
Williamson P, Spencer D, Gumnit R, Zahn C, Westbrook E and Enos B;
Quality Standards Subcommittee of the American Academy of
Neurology; American EpilepsySociety; American Association of
Neurological Surgeons, . Practice parameter: Temporal lobe and
localized neocortical resections for epilepsy: Report of the
quality standards subcommittee of the american academy of
neurology, in association with the american epilepsy society and
the american association of neurological surgeons. Neurology.
60:538–547. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cendes F, Cook MJ, Watson C, Andermann F,
Fish DR, Shorvon SD, Bergin P, Free S, Dubeau F and Arnold DL:
Frequency and characteristics of dual pathology in patients with
lesional epilepsy. Neurology. 45:2058–2064. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Salanova V, Markand O and Worth R:
Temporal lobe epilepsy: Analysis of patients with dual pathology.
Acta Neurol Scand. 109:126–131. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jung R, Aull-Watschinger S, Moser D, Czech
T, Baumgartner C, Bonelli-Nauer S and Pataraia E: Is reoperation an
option for patients with temporal lobe epilepsy after failure of
surgery? Seizure. 22:502–506. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mathon B, Bielle F, Samson S, Plaisant O,
Dupont S, Bertrand A, Miles R, Nguyen-Michel VH, Lambrecq V,
Calderon-Garcidueñas AL, et al: Predictive factors of long-term
outcomes of surgery for mesial temporal lobe epilepsy associated
with hippocampal sclerosis. Epelepsia. 58:1473–1485. 2017.
View Article : Google Scholar
|
|
9
|
Engel J Jr: Update on surgical treatment
of the epilepsies. Clin Exp Neurol. 29:32–48. 1992.PubMed/NCBI
|
|
10
|
Tellez-Zenteno JF, Dhar R and Wiebe S:
Long-term seizure outcomes following epilepsy surgery: A systematic
review and meta-analysis. Brain. 128:1188–1198. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tonini C, Beghi E, Berg AT, Bogliun G,
Giordano L, Newton RW, Tetto A, Vitelli E, Vitezic D and Wiebe S:
Predictors of epilepsy surgery outcome: A meta-analysis. Epilepsy
Res. 62:75–87. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Spencer S and Huh L: Outcomes of epilepsy
surgery in adults and children. Lancet Neurol. 7:525–537. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Radhakrishnan K, So EL, Silbert PL, Jack
CR Jr, Cascino GD, Sharbrough FW and O'Brien PC: Predictors of
outcome of anterior temporal lobectomy for intractable epilepsy: A
multivariate study. Neurology. 51:465–471. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jeong SW, Lee SK, Hong KS, Kim KK, Chung
CK and Kim H: Prognostic factors for the surgery for mesial
temporal lobe epilepsy: Longitudinal analysis. Epilepsia.
46:1273–1279. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Bocti C, Robitaille Y, Diadori P, Lortie
A, Mercier C, Bouthillier A and Carmant L: The pathological basis
of temporal lobe epilepsy in childhood. Neurology. 60:191–195.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kelemen A, Barsi P, Eross L, Vajda J,
Czirjak S, Borbely C, Rasonyi G and Halasz P: Long-term outcome
after temporal lobe surgery-prediction of late worsening of seizure
control. Seizure. 15:49–55. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Louis DN, Perry A, Reifenberger G, von
Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD,
Kleihues P and Ellison DW: The 2016 world health organization
classification of tumors of the central nervous system: A summary.
Acta Neuropathol. 131:803–820. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Palmini A, Najm I, Avanzini G, Babb T,
Guerrini R, Foldvary-Schaefer N, Jackson G, Luders HO, Prayson R,
Spreafico R and Vinters HV: Terminology and classification of the
cortical dysplasias. Neurology. 62 Suppl 3:S2–S8. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eriksson SH, Nordborg C, Rydenhag B and
Malmgren K: Parenchymal lesions in pharmacoresistant temporal lobe
epilepsy: Dual and multiple pathology. Acta Neurol Scand.
112:151–156. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mueller SG, Laxer KD, Cashdollar N, Lopez
RC and Weiner MW: Spectroscopic evidence of hippocampal
abnormalities in neocortical epilepsy. Eur J Neurol. 13:256–260.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Parmar H, Lim SH, Tan NC and Lim CC: Acute
symptomatic seizures and hippocampus damage: DWI and MRS findings.
Neurology. 66:1732–1735. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Briellmann RS, Wellard RM and Jackson GD:
Seizure-associated abnormalities in epilepsy: Evidence from MR
imaging. Epilepsia. 46:760–766. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Lawn N, Londono A, Sawrie S, Morawetz R,
Martin R, Gilliam F, Faught E and Kuzniecky R: Occipitoparietal
epilepsy, hippocampal atrophy, and congenital developmental
abnormalities. Epilepsia. 41:1546–1553. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li LM, Cendes F, Andermann F, Watson C,
Fish DR, Cook MJ, Dubeau F, Duncan JS, Shorvon SD, Berkovic SF, et
al: Surgical outcome in patients with epilepsy and dual pathology.
Brain. 122:799–805. 1999. View Article : Google Scholar : PubMed/NCBI
|