Introduction
Pneumonia is a common respiratory disease in the
clinic. It is an inflammation of the alveoli, the distal airways,
and interstitium of the lungs caused by infection of pathogenic
microorganisms, immune regulation, physical and chemical factors.
The main clinical manifestations include fever, cough, shortness of
breath and continuous dry and wet rales in the lung (1). Mycoplasma pneumoniae pneumonia
(MPP) is the most common form of pneumonia in childhood caused by
Mycoplasma pneumoniae (MP) infection. In China, MPP is a
leading cause of death in children (2). In recent years, the number of pediatric
patients infected with MP has increased year by year worldwide, and
patient age has shown a younger trend (3). However, the diagnosis or differential
diagnosis of MPP is difficult based on clinical symptoms. In this
regard, the lab test is especially helpful in the diagnosis of MPP.
Although D-dimer and interferon-γ (INF-γ) were reported to be
associated with pneumonia in the literature, the diagnostic value
and clinical implication of assessing both indicators in diagnosis
of MPP in children were not reported (4–7). In this
study, the serum levels of D-dimer and INF-γ in 185 pediatric
patients with MPP and 92 healthy children were measured, to explore
their associations with MPP and the clinical value of assessing
both in diagnosis of MPP. The aim of this study was to find a more
accurate, convenient and rapid diagnostic method for the clinical
prediction and diagnosis of MPP in children.
Patients and methods
Subjects
Enrolled in this study were 185 pediatric patients
with MPP confirmed through assessment of clinical presentation,
medical history, chest X-ray radiography findings and laboratory
data who were admitted to the Second Affiliated Hospital of Qiqihar
Medical University's Pediatric Department and the First Hospital of
Qiqihar City (both in Qiqihar, China) from January 2017 to October
2017. Patients were divided into two groups according to the
severity of their sickness: The mild and severe pneumonia group
with an average age of 3.316±1.088 and 3.350±1.078 years,
respectively. All patients met the criteria for the diagnosis of
MPP outlined in Zhu Fu Tang Practical Pediatrics, including fever
duration of >10 days, severe clinical presentation in the lungs,
pulmonary consolidation and pleural effusion. Patients who
developed extra-pulmonary complications or experienced poor
outcomes after 10 days of solo treatment with macrolide antibiotics
were regarded as being with severe MPP (8). A total of 92 healthy children with an
average age of 3.296±1.127 years who underwent physical examination
during the same time period were assigned to the control group. The
general data such as sex and age of the three groups of subjects
were comparable, and the differences between groups were not
statistically significant. Patients with the following conditions
were excluded from this study: Diarrhea, anemia, liver and kidney
diseases, systemic diseases, congenital heart disease, congenital
immunodeficiency disorders, long-term use of immunosuppressive
agents, tuberculosis and asthma. The duration of fever or cough was
2–7 days for all patients with MPP. This study was approved by the
Ethics Committee of the Second Affiliated Hospital of Qiqihar
Medical University. All participating children and their families
were briefed on the specific protocols and procedures of this
study. Guardians of all the children participating in this study
signed informed consent and children voluntarily participated in
this study.
Sample collection and plasma D-dimer
detection
Pre- and post-treatment blood samples were collected
from pediatric patients with mild and severe pneumonia. Each time 5
ml of venous blood was taken from all the patients in the morning
under fasting. The blood sample was centrifuged at 500 × g for 10
min using a centrifuge manufactured by Anhui Zhongke Zhongjia
Scientific Instrument Co., Ltd. (Hefei, China). The plasma was
stored in a dry tube protected from light. The D-dimer level was
determined using the erythrocyte sedimentation rate (ESR) test kit
(Siemens AG, Munich, Germany) with the immune turbidimetric assay.
The assay was performed on a fully automated hematology analyzer
(Sysmex Corp., Kobe, Japan). The kit was used strictly in
accordance with the manufacturer's protocol. The measured plasma
D-dimer levels were recorded for all subjects in the three groups.
A D-dimer level >0.115 µg/ml was regarded as positive.
Serum INF-γ detection
Pre- and post-treatment blood samples were collected
from all pediatric patients with mild and severe pneumonia. Blood
samples were also collected from the healthy subjects. Each time 5
ml of venous blood was taken in the morning under fasting. The
blood sample was centrifuged at 500 × g for 10 min using a
centrifuge manufactured by Anhui Zhongke Zhongjia Scientific
Instrument Co., Ltd. The supernatant (serum) was taken and stored
in a freezer at −80°C. The serum level of INF-γ was determined with
the enzyme-linked immunosorbent assay (ELISA) using the ELISA kit
(Thermo Fisher Scientific, Inc., Waltham, MA, USA). The kit was
used strictly in accordance with the manufacturer's protocol. The
assay was performed on a Biotek EL 311 (BioTec U.S., Winooski, VT,
USA) microplate reader. The measured serum levels of INF-γ were
recorded for all subjects in the three groups.
Statistical analysis
All data were expressed as mean ± SEM. The t-test
was used for the comparison of two means. All data were subjected
to statistical analysis using the analysis of variance (ANOVA)
statistical software. Fisher's analysis was used after ANOVA. The
ANOVA software was used to test whether the differences in the
means between multiple data sets were statistically significant. A
difference was statistically significant at p<0.05.
Results
General data of subjects in the three
groups
Age and sex were comparable in the three groups
(Table I), and the differences
between groups were not statistically significant (p>0.05). The
numbers of patients who had symptoms of fever and cough, abnormal
findings in chest X-ray radiography, and positive responses in MP
antibody test were comparable in the mild and severe pneumonia
group, and the differences between the two groups were not
statistically significant (p>0.05).
 | Table I.General data of subjects in the three
groups. |
Table I.
General data of subjects in the three
groups.
|
| Groups |
|---|
| Items | Control | Mild pneumonia | Severe pneumonia |
|---|
| Case no. | 92 | 90 | 95 |
| Sex |
| Male | 46 | 46 | 48 |
|
Female | 46 | 44 | 47 |
| Average age
(years) | 3.296 | 3.316 | 3.350 |
| Fever (n) | 0 | 90 | 95 |
| Cough (n) | 0 | 90 | 95 |
| Abnormal findings in
chest X-ray radiography (n) | 0 | 90 | 95 |
| Positive responses in
MP antibody test (n) | 0 | 90 | 95 |
Levels of D-dimer and INF-γ in healthy
children and pediatric patients before treatment
As shown in Table
II, the plasma D-dimer levels in the control, the mild and the
severe pneumonia group were 0.08±0.19, 0.30±0.21 and 0.61±0.25
µg/ml, respectively. Apparently, the D-dimer levels in patients
with pneumonia were significantly higher than that in healthy
children (p<0.001), and it tended to be higher in patients with
severe pneumonia (p<0.001).
| Table II.Levels of D-dimer and INF-γ in healthy
children and pediatric patients before treatment. |
Table II.
Levels of D-dimer and INF-γ in healthy
children and pediatric patients before treatment.
|
| D-dimer (µg/ml) | INF-γ (pg/ml) |
|---|
|
|
|
|
|---|
| Groups | Value | P-value | t-value | Value | P-value | t-value |
|---|
| Control | 0.08±0.19 | – | – | 24.01±3.17 | – | – |
| Mild pneumonia | 0.30±0.21 | 0.0012 | 3.840 | 33.16±4.38 | 0.003 | 3.421 |
| Severe pneumonia | 0.61±0.25 | 0.0001 | 7.235 | 46.43±4.10 | 0.0001 | 6.595 |
Levels of D-dimer and INF-γ in
patients with mild MPP after 24 and 120 h of treatment
The plasma D-dimer levels were 0.44±0.17 and
0.19±0.09 µg/ml, respectively, after 24 and 120 h of treatment in
pediatric patients with mild MPP (Table III). Clearly, the D-dimer level
decreased over time in the treatment. The decrease between the two
recorded time-points was statistically significant. The INF-γ
levels were 26.15±2.09 and 18.62±1.98 pg/ml, respectively, after 24
and 120 h of treatment in pediatric patients with mild MPP. The
decreasing trend in the INF-γ level over time in the treatment was
similar to that in the D-dimer level. The decrease between the two
recorded time-points was statistically significant (p<0.05).
| Table III.Levels of D-dimer and INF-γ in
patients with mild MPP over time in the treatment. |
Table III.
Levels of D-dimer and INF-γ in
patients with mild MPP over time in the treatment.
| Treatment time
(h) | D-dimer (µg/ml) | INF-γ (pg/ml) |
|---|
| 24 | 0.44±0.17 | 26.15±2.09 |
| 120 | 0.19±0.09 | 18.62±1.98 |
Levels of D-dimer and INF-γ in
patients with severe MPP after 24 and 120 h of treatment
The plasma D-dimer levels were 0.69±0.21 and
0.33±0.17 µg/ml, respectively, after 24 and 120 h of treatment in
pediatric patients with severe MPP (Table IV). The decrease between the two
time-points in the treatment was statistically significant
(p<0.001). The INF-γ levels were 51.22±2.31 and 36.71±2.08
pg/ml, respectively, after 24 and 120 h of treatment in pediatric
patients with severe MPP. The decrease between the two time-points
in the treatment was statistically significant (p<0.01).
Although the decreasing trends in both the D-dimer and the INF-γ
level were expected to be the same between patients with mild and
severe pneumonia, the final levels of both indicators after 120 h
of treatment were higher in the severe pneumonia group than those
in the mild pneumonia group.
| Table IV.Levels of D-dimer and INF-γ in
patients with severe MPP over time in the treatment. |
Table IV.
Levels of D-dimer and INF-γ in
patients with severe MPP over time in the treatment.
| Treatment time
(h) | D-dimer (µg/ml) | INF-γ (pg/ml) |
|---|
| 24 | 0.69±0.21 | 51.22±2.31 |
| 120 | 0.33±0.17 | 36.71±2.08 |
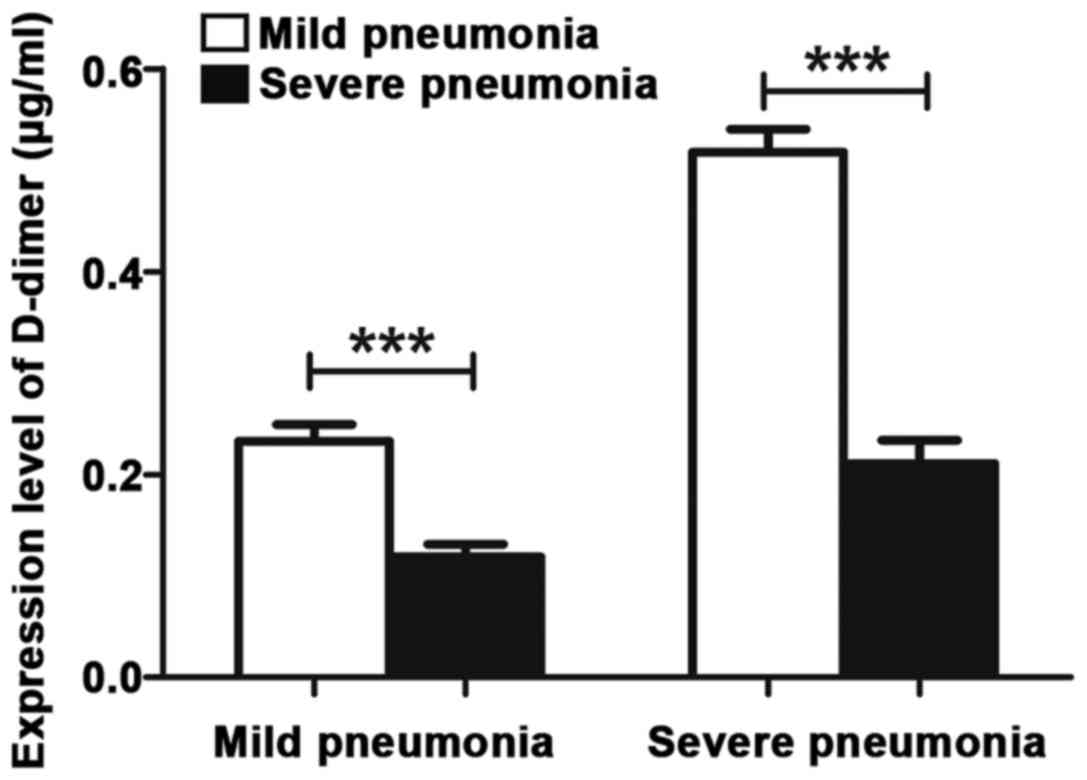
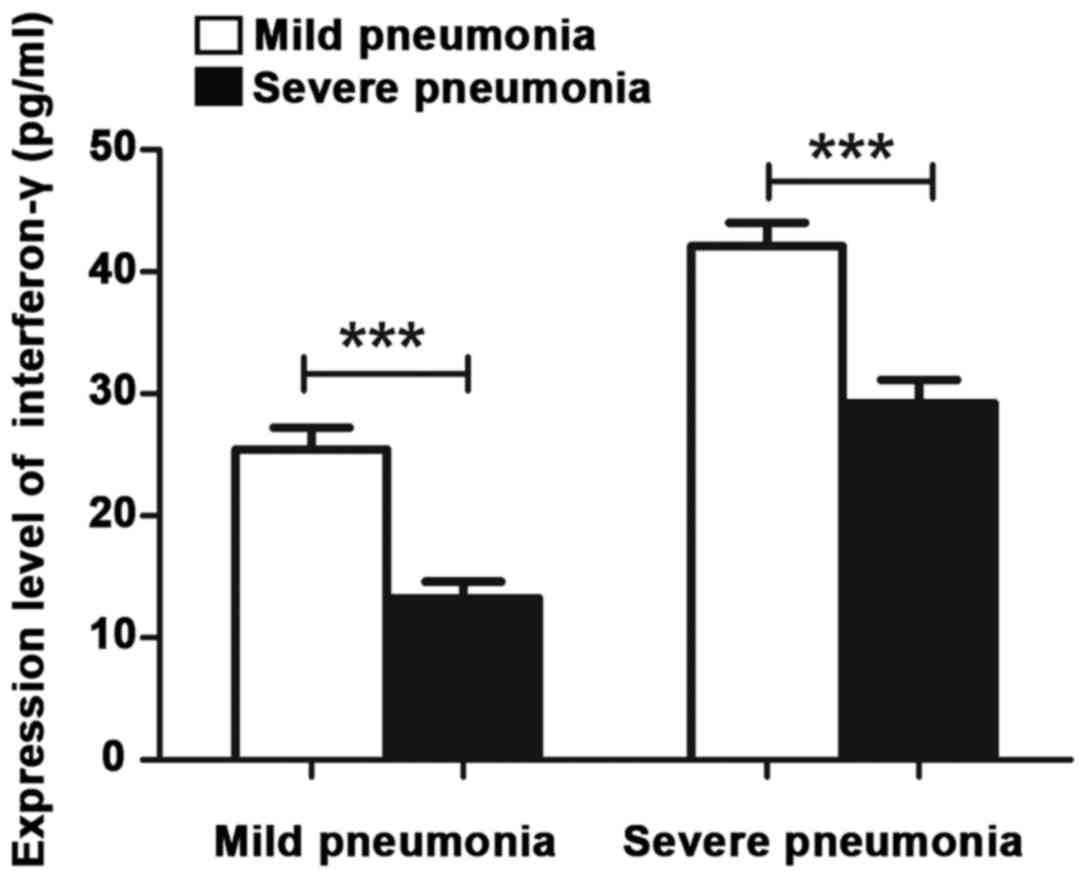
Levels of D-dimer and INF-γ in
patients who developed extra-pulmonary complications in the mild
and severe pneumonia group
Patients in the mild and severe pneumonia group were
further divided into four subgroups: Τhe mild pneumonia with
extra-pulmonary complications subgroup, the mild pneumonia without
extra-pulmonary complications subgroup, the severe pneumonia with
extra-pulmonary complications subgroup, and the severe pneumonia
without extra-pulmonary complications subgroup. The levels of
D-dimer and INF-γ in these four subgroups were compared after 120 h
of treatment. Among patients in the mild pneumonia group, the
D-dimer levels in patients who developed extra-pulmonary
complications and those who did not were 0.27±0.18 and 0.11±0.12
µg/ml, respectively. The former was more than double the latter,
and the difference was statistically significant (p<0.001). The
INF-γ levels in patients who developed extra-pulmonary
complications and those who did not were 23.62±2.36 and 14.15±2.20
pg/ml, respectively. The former was much more than the latter, and
the difference was statistically significant (p<0.001) (Table V).
| Table V.Levels of D-dimer and INF-γ in
patients who developed extrapulmonary complications in the mild and
severe pneumonia group. |
Table V.
Levels of D-dimer and INF-γ in
patients who developed extrapulmonary complications in the mild and
severe pneumonia group.
| Groups | D-dimer (pg/ml) | INF-γ (µg/ml) |
|---|
| Mild pneumonia |
|
|
| With extra pulmonary
complications | 0.27±0.18 | 23.62±2.36 |
| Without extra
pulmonary complications | 0.11±0.12 | 14.15±2.20 |
| Severe pneumonia |
|
|
| With extra pulmonary
complications | 0.50±0.16 | 41.62±2.19 |
| Without extra
pulmonary complications | 0.18±0.10 | 33.15±2.31 |
Among patients in the severe pneumonia group, the
D-dimer levels in patients who developed extra-pulmonary
complications and those who did not were 0.50±0.16 and 0.18±0.10
µg/ml, respectively. The former was more than double the latter,
and the difference was statistically significant (p<0.001). The
INF-γ levels in patients who developed extra-pulmonary
complications and those who did not were 41.62±2.19 and 33.15±2.31
pg/ml, respectively. The former was higher than the latter, and the
difference was statistically significant (p<0.001) (Table V; Figs.
1 and 2).
Discussion
Pneumonia is an inflammation of the alveoli, the
airways, and interstitium of the lungs caused by infection of a
variety of pathogenic microorganisms or by inhaling toxic
substances (9). The symptoms often
include fever, cough and expectoration. For severe pneumonia,
dyspnea and chest pain can also occur (10). Childhood pneumonia is a common
pediatric disease with a high incidence. In most cases, the
pathogens are bacteria, viruses, and MP, which inflict substantial
harm to pediatric patients' lungs and systemic health. In recent
years, childhood pneumonia associated with MP infection has drawn
much attention from medical practitioners due to a significantly
rising incidence being observed in children (11). In the clinic, it is still difficult
to accurately identify childhood pneumonia associated with MP
infection as the clinical symptoms are not consistent. Delayed
diagnosis not only increases the risk of irreversible damage to
patients' respiratory system, but also potentially leads to harm in
multiple organs and systems (12).
Therefore, accurate, rapid and timely identification of MPP in
children is critical and should be the focus of clinical work.
It was reported that immune response to MP infection
played an important role in the onset and progression of MPP. Thus,
immunoassays relevant to hematology following infection with MP
have become a hot topic in recent years (13). In this study, the levels of D-dimer
and INF-γ were measured in blood samples collected from 185
pediatric patients with MPP and 92 healthy children. To the best of
our knowledge, there is no report in literature on assessment of
these two indicators at the same time in the diagnosis and
identification of MPP in children (5,14–16).
D-dimer is a specific fibrin degradation product
after activation by cross-linking of the fibrin monomer with
activating factors. It is also a specific marker of the
fibrinolytic system. D-dimer can be used as one of the indicators
for monitoring inflammation and severe infection (17). Patients with MPP appear hypoxic.
Hypoxia and endotoxin stimulates inflammatory cells to release a
variety of inflammatory mediators, resulting in injuries of
vascular endothelial cells leading to a significant increase in
plasma D-dimer levels (18).
INF-γ is a small polypeptide that regulates cell
function. It plays an important role in cell-mediated immune
regulation (19). On the one hand,
INF-γ stimulates the production of macrophages. On the other hand,
INF-γ promotes the differentiation of T cells into cytotoxic
CD4+ TH1 and CD8+ Tc1 T-cell subsets. In
addition, INF-γ activates neutrophils and vascular endothelial
cells, thereby promoting endothelial cellular secretion and
adhesion (20).
In this study, 92 healthy children were recruited as
a control, 90 pediatric patients with mild pneumonia and 95
pediatric patients with severe pneumonia were recruited as study
subjects. The general data such as age and sex of subjects in the
three groups were comparable, and the differences were not
statistically significant. Blood samples were collected from all
pediatric patients before and after treatment, and from healthy
subjects in the control group as well. The levels of D-dimer and
INF-γ were determined for all subjects in the three groups. The
results showed that the levels of D-dimer and INF-γ in the mild and
severe pneumonia group were all significantly higher than those in
the control group, and the levels of both indicators increased
progressively with the disease severity. Elevation of the D-dimer
level implied that the pediatric patient was at the stage of MP
infection, and elevation of the INF-γ level indicated that the
patient was infected and was seriously ill. After a period of
treatment, the levels of D-dimer and INF-γ were measured again in
all subjects. It was found that the levels of these two indicators
decreased significantly after treatment, and the final levels of
both indicators after 120 h of treatment were higher in the severe
pneumonia group than those in the mild pneumonia group. The
immunoassay showed that the levels of D-dimer and INF-γ increased
significantly in pediatric patients with MPP, and the increase was
much more evident in patients with severe pneumonia. The levels of
D-dimer and INF-γ were found to be positively correlated with
extra-pulmonary complications in pediatric patients with pneumonia.
The sensitivity, specificity and negative predictive value were
90.18, 91.75 and 76.2%, respectively. The sensitivity and
specificity were all in the good range. In the case of severe MPP,
excessive and persistent stimulation of inflammatory cytokines
inflicted damage on the vascular endothelial cells, disturbing the
balance between coagulation, anticoagulation and fibrinolysis.
Elevation of the D-dimer level in pediatric patients with MPP
indicated the presence of a hypercoagulable state and vascular
endothelial dysfunction in patients, resulted from damage of
vascular endothelial cells inflicted by inflammatory cytokines.
When an infection occurs, early induced responses play an important
role. The body secretes IFN-γ to inhibit the growth of pathogens
directly and participate in the immune response in vivo.
Results of this study suggested that the serum IFN-γ level in
pediatric patients with pneumonia may be positively correlated with
disease severity. The severity of the patient's condition can be
evaluated by detecting the serum IFN-γ level in pediatric patients
with pneumonia. As a benefit, the patients get timely and
appropriate treatment. This study demonstrated that the
inflammatory response of diseases can be evaluated by assessing the
levels of D-dimer and INF-γ in plasma, which was helpful in early
diagnosis of severe diseases and prediction of patient
prognosis.
In summary, the levels of D-dimer and INF-γ in
pediatric patients with MPP were measured, and the results provided
evidence that the assessment of both indicators at the same time
may prove useful in the diagnosis of MPP in children, the
evaluation of the disease severity and the prediction of prognosis.
The findings in this study can serve as a reference for rapid
diagnosis of MPP, evaluation of treatment efficacy and prediction
of prognosis.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
XJ drafted the manuscript. XJ, YZhu and YZha were
mainly devoted to the sample collection and plasma D-dimer
detection. JC, LR and XZ were responsible for the serum INF-γ
detection. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the Second Affiliated Hospital of Qiqihar Medical University
(Qiqihar, China). Guardians of all the children participating in
this study signed informed consent and children voluntarily
participated in this study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Leong CL, Norazah A, Azureen A and Lingam
R: Community-acquired necrotising pneumonia caused by
Panton-Valentine leucocidin-producing methicillin-resistant
Staphylococcus aureus. Med J Malaysia. 72:378–379.
2017.PubMed/NCBI
|
|
2
|
Tashiro M, Fushimi K, Kawano K, Takazono
T, Saijo T, Yamamoto K, Kurihara S, Imamura Y, Miyazaki T,
Yanagihara K, et al: Adjunctive corticosteroid therapy for
inpatients with Mycoplasma pneumoniae pneumonia. BMC Pulm
Med. 17:2192017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Qiu L, Wang L, Tan L, Li M, Wu C, Li L,
Zhang Z, Jiang H, Sun Q and Zhang T: Molecular characterization of
genomic DNA in Mycoplasma pneumoniae strains isolated from
serious mycoplasma pneumonia cases in 2016, Yunnan, China. Infect
Genet Evol. 58:125–134. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Millot G, Voisin B, Loiez C, Wallet F and
Nseir S: The next generation of rapid point-of-care testing
identification tools for ventilator-associated pneumonia. Ann
Transl Med. 5:4512017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li YX, Zheng ZG, Liu N, Wang XN, Wu LL and
Chen RC: Risk factors for pulmonary embolism in acute exacerbation
of chronic obstructive pulmonary disease. Zhonghua Jie He He Hu Xi
Za Zhi. 39:298–303. 2016.(In Chinese). PubMed/NCBI
|
|
6
|
Imdad A, Mayo-Wilson E, Herzer K and
Bhutta ZA: Vitamin A supplementation for preventing morbidity and
mortality in children from six months to five years of age.
Cochrane Database Syst Rev. 3:CD0085242017.PubMed/NCBI
|
|
7
|
Zhang Y, Zhou X, Zhang H, Huan C and Ye Z:
Establishment of Acinetobacter baumannii-induced pneumonia
model in mice. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi. 33:1392–1397.
2017.(In Chinese). PubMed/NCBI
|
|
8
|
Miyashita N, Obase Y, Ouchi K, Kawasaki K,
Kawai Y, Kobashi Y and Oka M: Clinical features of severe
Mycoplasma pneumoniae pneumonia in adults admitted to an
intensive care unit. J Med Microbiol. 56:1625–1629. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Li MS, Hung GC, Yang SY, Pan CH, Liao YT,
Tsai SY, Chen CC and Kuo CJ: Excess incidence and risk factors for
recurrent pneumonia in bipolar disorder. Psychiatry Clin Neurosci.
72:337–348. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Li W, Ding C and Yin S: Aging increases
the expression of lung CINCs and MCP-1 in senile patients with
pneumonia. Oncotarget. 8:108604–108609. 2017.PubMed/NCBI
|
|
11
|
Minz A, Agarwal M, Singh JV and Singh VK:
Care seeking for childhood pneumonia by rural and poor urban
communities in Lucknow: A community-based cross-sectional study. J
Family Med Prim Care. 6:211–217. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yin YD, Wang R, Zhuo C, Wang H, Wang MG,
Xie CM, She DY, Yuan X, Wang RT, Cao B, et al: Macrolide-resistant
Mycoplasma pneumoniae prevalence and clinical aspects in
adult patients with community-acquired pneumonia in China: A
prospective multicenter surveillance study. J Thorac Dis.
9:3774–3781. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Joob B and Wiwanitkit V:
Leukoagglutination, Mycoplasma pneumoniae pneumonia and EDTA
acid blood. Turk J Haematol. 35:75–76. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Parois SP, Faoüen A, Le Floc'h N and
Prunier A: Influence of the inflammatory status of entire male pigs
on their pubertal development and fat androstenone. Animal.
11:1071–1077. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ye Q, Xu XJ, Shao WX, Pan YX and Chen XJ:
Mycoplasma pneumoniae infection in children is a risk factor
for developing allergic diseases. ScientificWorldJournal.
2014:9865272014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jiang YL and Peng DH: Serum level of
vitamin A in children with pneumonia aged less than 3 years.
Zhongguo Dang Dai Er Ke Za Zhi. 18:980–983. 2016.(In Chinese).
PubMed/NCBI
|
|
17
|
Wu HB, Ma WG, Zhao HL, Zheng J, Li JR, Liu
O and Sun LZ: Risk factors for continuous renal replacement therapy
after surgical repair of type A aortic dissection. J Thorac Dis.
9:1126–1132. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yuan SJ, Xie HT and Li ZL: Clinical
significance of hypersensitive C-reactive protein, fribrinogen and
D-dimmer in connective tissue disease-related interstitial lung
disease. Nan Fang Yi Ke Da Xue Xue Bao. 37:415–419. 2017.(In
Chinese). PubMed/NCBI
|
|
19
|
Duarte T, Barbisan F, do Prado-Lima PAS,
Azzolin VF, da Cruz Jung IE, Duarte MMMF, Teixeira CF, Mastella MH
and da Cruz IBM: Ziprasidone, a second-generation antipsychotic
drug, triggers a macrophage inflammatory response in vitro.
Cytokine. 106:101–107. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xu J, Gu Y, Sun J, Zhu H, Lewis DF and
Wang Y: Reduced CD200 expression is associated with altered Th1/Th2
cytokine production in placental trophoblasts from preeclampsia. Am
J Reprod Immunol. 79:e127632018. View Article : Google Scholar
|