Introduction
Calcifying fibrous tumor (CFT) was first described
as a ‘childhood fibrous tumor with psammoma bodies’ by Rosenthal
and Abdul-Karim (1) in 1988, but
later studies demonstrated it may also occur among the adult
population (2,3). CFT is a rare but distinctive entity; it
is a benign lesion that consists of abundant hyalinized collagen
with psammomatous or dystrophic calcifications (4). CFTs primarily originate from the soft
tissue, e.g. pleura and abdominal viscera; the stomach only rarely
participates (5). CFT confined to
the gastric wall is a rare and benign lesion, which usually
presents without any gastrointestinal symptoms and is often
detected incidentally (5). Gastric
CFT is less likely to cause serious complications such as
perforation or obstruction. In spite of its benign course and good
prognosis, with known histological and immunohistochemical
features, the exact pathogenic mechanism of this lesion remains
elusive. Gastric CFT should be carefully differentiated from other
spindle cell mesenchymal lesions involved in the stomach, such as
inflammatory myofibroblastic tumor, sclerosing calcified
gastrointestinal stromal tumor, schwannoma and IgG4-related
sclerosing disease. Furthermore, given the rarity of gastric CFT
(less than 50 cases reported to date), it is important to enhance
the understanding of this lesion among clinicians. Therefore, the
present study focused on exploring its clinical and pathological
features by presenting 9 cases of gastric CFT, and reviewing
previous English language articles regarding gastric CFT to
determine whether this kind of tumor has a sex predilection.
Furthermore, the current study aimed to analyze the possible
association between female predominance and expression of G
protein-coupled estrogen receptor (GPER).
Subjects and methods
The clinical information, relevant biochemical
indicators [blood routine, tumor markers, C reactive protein,
hepatitis B virus and Helicobacter pylori (HP)] and
pathological features (gross examination and microscopic findings)
of 9 patients with gastric CFT who had been admitted to the
Department of Gastroenterology and Gastrointestinal Surgery at the
Renmin Hospital of Wuhan University (Wuhan, China) between January
2015 and July 2018 were retrospectively reviewed. The present
protocol was approved by the Institutional Review Board of the
Renmin Hospital of Wuhan University, and all patient data was
handled confidentially. All patients included in the present study
provided written informed consent. The tumor slides from the 9
cases were collected from the Department of Pathology of the Renmin
Hospital of Wuhan University. In addition, literature databases up
to July 2018 were searched, including PubMed (www.ncbi.nlm.nih.gov/pubmed), Embase (www.embase.com), Scopus (www.scopus.com) and Google Scholar (scholar.google.com), for previously published English
language articles regarding gastric CFT case reports or case
series. The search terms were ‘calcifying fibrous tumor AND
gastric’, and ‘calcifying fibrous pseudotumor AND gastric’. Two
authors reviewed potential studies, and any discrepancies were
resolved by a third author.
Tumor specimens resected by endoscopic submucosal
dissection (ESD) or gastric wedge excision (GWE) were fixed in 10%
formalin solution for 4 h at room temperature and embedded in
paraffin using routine methods. Deparaffinized sections with 4 µm
thickness were used for staining with hematoxylin and eosin (5 min
for hematoxylin and 1 min for eosin). Immunohistochemical
techniques were conducted according to the SP method as described
previously (6). Deparaffinized
sections with 4 µm thickness were quenched in 3%
H2O2, then subjected to antigen retrieval in
boiling citric acid (pH 6.0) for 15 min and washed with PBS.
Following incubation overnight with primary antibodies against GPER
(ab39742; 1:200), estrogen receptor (ER; ab17230; 1:200) or
vimentin (ab24525; 1:5,000; all from Abcam, Cambridge, UK) at 4°C,
the sections were incubated for 15 min at room temperature with
horseradish peroxidase-labeled polymer-conjugated secondary
antibodies (MaxVision™ kits; Maxim Bio, Fujian, China). The
specimens were then incubated for 1 min at room temperature with
diaminobenzidine (Maxim Bio). Finally, the sections were
counterstained at room temperature with hematoxylin for 30 sec.
Results
Clinical characteristics of the 9
cases
Six patients (cases 4–9) originally attended the
hospital for a check-up for non-specific symptoms, such as belching
or a bloated abdomen. Among the 9 cases, there were 6 female
patients and 3 male patients (2:1). The age of the patients ranged
from 40–71 years, with a mean age of 52.22 years. A total of 6
tumor cases (cases 1, 2, 5, 6, 7 and 8) originated from the gastric
body, whereas the remaining 3 originated from the fundus of the
stomach (cases 3, 4 and 9; Table I).
Cases 1 and 9 were concomitant with reflux esophagitis, case 2 was
accompanied with duodenal ulcer, and erosive hemorrhagic gastritis
and hypertension were reported in case 3. Furthermore, type 2
diabetes and superficial gastritis were diagnosed in cases 6 and 8,
respectively. No patients were reported to suffer from autoimmune
disorders. The details of smoking, alcohol consumption and body
mass index are listed in Table
I.
 | Table I.Clinicopathologic features of 9 cases
of gastric calcifying fibrous tumor. |
Table I.
Clinicopathologic features of 9 cases
of gastric calcifying fibrous tumor.
| Case no. | Age (years) | Sex | Smoking | Drinking | BMI
(Kg/m2) | Concomitant
disease | Site | Layer | Size (cm) | Treatment | Complications | Follow-up
(months) |
|---|
| 1 | 44 | Female | No | No | 22.89 | Reflux
esophagitis | Body | Submucosa | 1.5×1.0×0.8 | ESD | None | 25 |
| 2 | 50 | Female | No | No | 27.06 | Duodenal ulcer | Body | Lamina propria | 1.5×1.5×1.0 | ESD | Celialgia | 14 |
| 3 | 42 | Female | No | Yes | 23.81 | Erosive hemorrhagic
gastritis hypertension | Fundus | Lamina propria | 1.3×0.8×0.6 | ESD | None | 23 |
| 4 | 61 | Male | Yes | Yes | 17.90 | None | Fundus | Lamina propria | 2.5×2.0×1.5 | ESD | None | 17 |
| 5 | 46 | Female | No | No | 21.33 | None | Body | Submucosa | 1.7×1.5×0.2 | ESD | None | 11 |
| 6 | 71 | Male | No | No | 20.24 | Diabetes | Body | Submucosa | 2.0×1.5×0.5 | GWE | Celialgia | 9 |
| 7 | 54 | Female | No | No | 23.44 | None | Body | Submucosa | 2.0×1.5×1.5 | ESD | None | 9 |
| 8 | 62 | Male | Yes | Yes | 27.34
(alcoholism) | Superficial
gastritis | Body | Lamina propria | 2.0×1.2×0.4 | ESD | None | 6 |
| 9 | 40 | Female | No | No | 19.52 | Superficial
gastritis | Fundus | Submucosa | 1.8×1.3×0.8 | ESD | None | 4 |
Laboratory tests
No abnormalities were evident in routine and tumor
marker blood tests [including carcinoembryonic antigen,
α-fetoprotein, carbohydrate antigen (CA)19-9 and CA-125]. Cases 1
and 2 presented with chronic hepatitis B virus (HBV) infection, and
cases 1, 3 and 8 were positive in the 13C breath test
and diagnosed with HP infection (Table
II). Furthermore, C-reactive protein (CRP) levels were slightly
elevated in 5 cases (cases 1, 2, 3, 7 and 8).
| Table II.Laboratory tests of 9 cases of
gastric calcifying fibrous tumor. |
Table II.
Laboratory tests of 9 cases of
gastric calcifying fibrous tumor.
| Case no. | Blood routine | Tumor
markersa | CRP | HBV | HP |
|---|
| 1 | – | – | ↑ | + | + |
| 2 | – | – | ↑ | + | N |
| 3 | – | – | ↑ | N | + |
| 4 | – | – | – | N | N |
| 5 | – | – | – | N | N |
| 6 | – | – | – | N | N |
| 7 | – | – | ↑ | N | N |
| 8 | – | – | ↑ | N | + |
| 9 | – | – | – | N | N |
Gross examination and microscopic
findings
Sections from all 9 cases revealed well-defined
lumps; each section contained an isolated nodular lesion covered by
intact mucosa. The maximum diameter ranged from 1.3–2.5 cm, with a
mean of 1.81 cm. A total of 4 tumors (cases 2, 3, 4 and 8) were
located in the lamina propria, with extension to the submucosa,
whereas the remaining 5 cases (1, 5, 6, 7 and 9) occurred in the
submucosa (Table I).
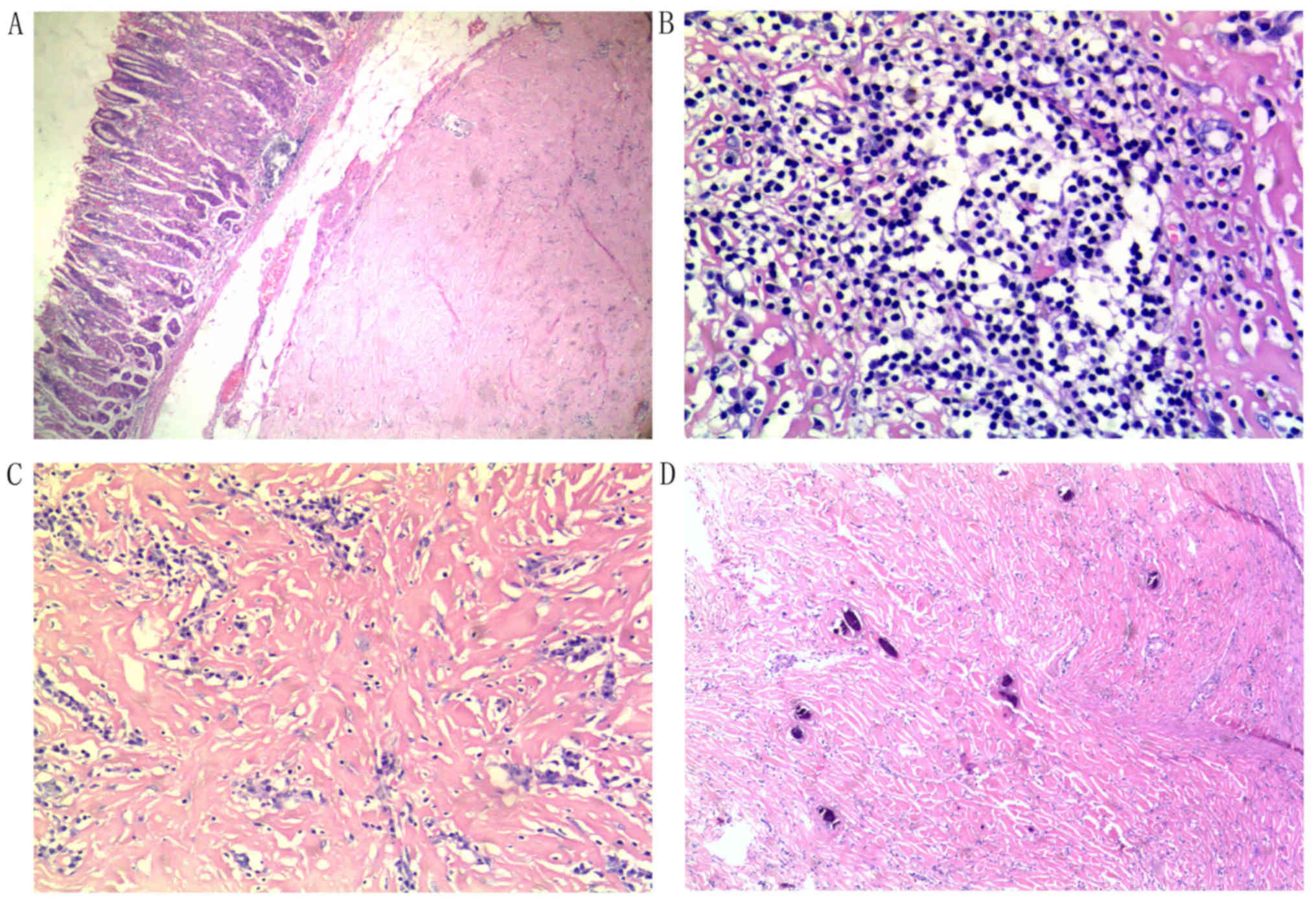
Microscopically, the common characteristics of the 9
cases included considerable hypocellular sclerosis and wavy
storiform coarse collagen infiltrated with scattered or patchy
mononuclear inflammatory cells. Six cases (cases 1, 2, 4, 5, 6 and
9) exhibited a predominance of dense hyaline fibrous tissue
infiltrated with many inflammatory cells and multifocal dystrophic
calcifications. Psammomatous and dystrophic calcifications are
indicated in Fig. 1.
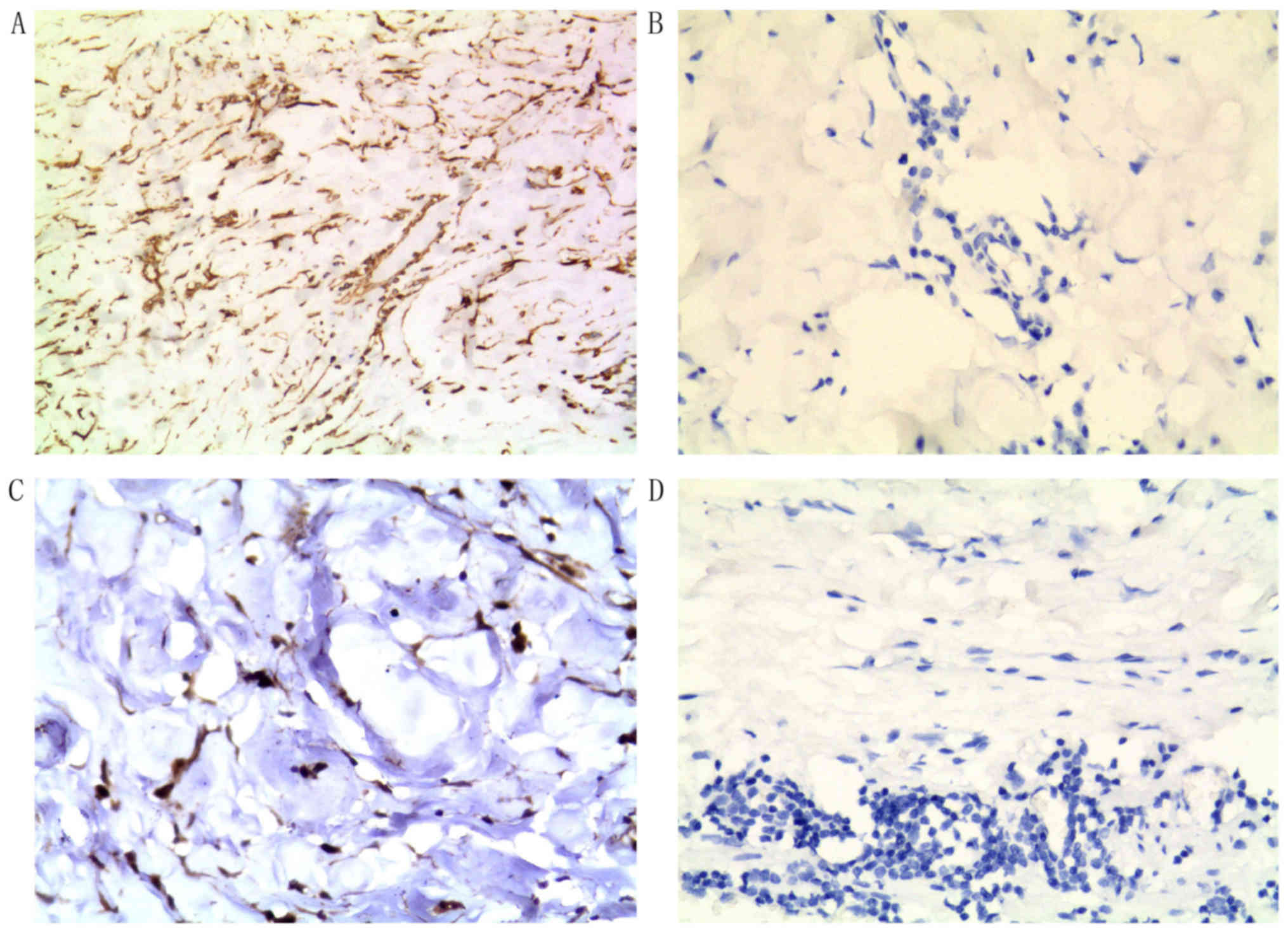
Immunohistochemical staining
From the immunohistochemical examination of gastric
CFT specimens, lesional cells were determined to be positive for
vimentin and GPER expression. However, all 9 cases were negative
for ER expression (Fig. 2).
Treatment and follow-up
A total of 8 patients were treated with ESD; only 1
patient (case 6) underwent partial gastrectomy. Following ESD or
surgical treatment, all patients recovered fully. None of the 9
patients available to follow-up (mean follow-up time, 13.11 months;
range, 4–25 months) have experienced local recurrence (Table I).
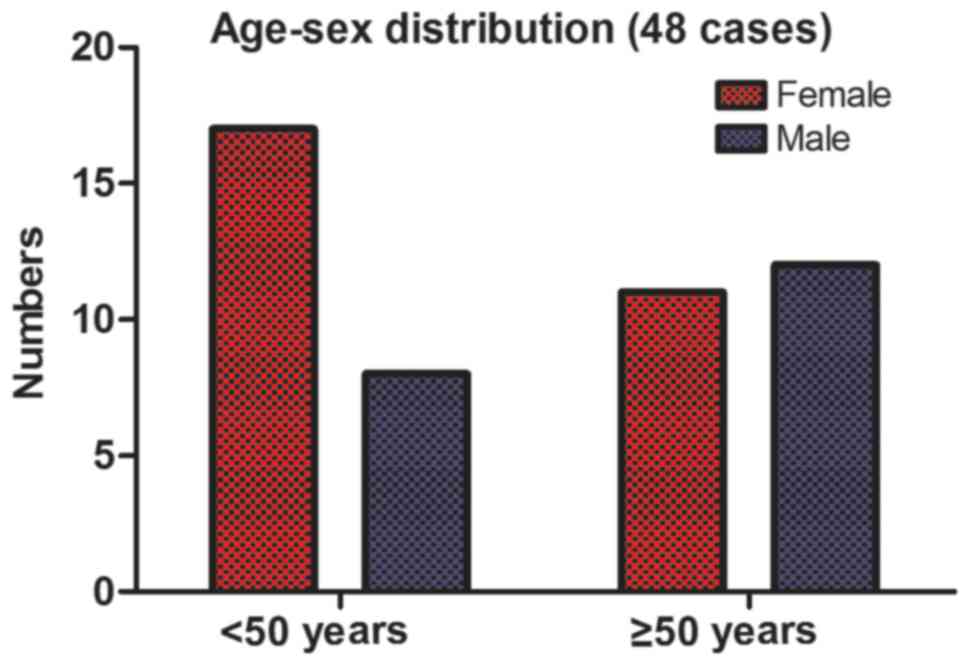
Literature search
In total, 25 previous studies regarding gastric CFT
were identified, including 39 individual cases (Table III) (7–31). At
present, there are 48 cases of gastric CFT reported in the English
language literature, including the 9 cases from the present study.
Among the 48 cases of gastric CFT, there were 28 female and 20 male
patients, a sex ratio of 1.4:1. The number of female patients was
more than twice that of the male patients in the patients <50
years of age (17 vs. 8), whereas the number was almost equal
between women and men ≥50 years of age (11 vs. 12; Fig. 3). Regarding geographical distribution
of the gastric CFT patients, Asia ranked the highest (including 17
patients in China, 4 in Korea, 3 in Japan, 1 in Kuwait, 1 in Turkey
and 1 in Pakistan), followed by Europe (7 patients in Germany, and
1 in each of Greece, Slovakia, Switzerland, France and Italy),
whereas only 9 cases occurred in North America (8 patients in the
USA and 1 in Canada). According to the distribution of these 48
cases, it appears that people from Asia, especially from East Asia,
are more likely to suffer from this disease than people from Europe
or North America, potentially due to ethnic or regional
differences.
| Table III.Clinicopathologic features of 39
cases of gastric calcifying fibrous tumor from previous
studies. |
Table III.
Clinicopathologic features of 39
cases of gastric calcifying fibrous tumor from previous
studies.
| Author | Case no. | Country | Age (years) | Sex | Site | Layer | Size (cm) | Treatment | (Refs.) |
|---|
| Tanaka et
al | 10 | Japan | 43 | Female | NA | Submucosa | NA | Local excision | (7) |
| Liu and Song | 11 | China | 32 | Male | Body | Submucosa | 3.0×2.0×2.0 | Local excision | (8) |
| Nascimento et
al | 12 | USA | 64 | Male | NA | NA | 1.1 | Local excision | (9) |
| Nascimento et
al | 13 | USA | 65 | Female | NA | NA | 0.8 | Local excision | (9) |
| Kitamura et
al | 14 | Japan | 44 | Female | Body | Submucosa | 3×2.6×2.4 | LWGR | (10) |
| Yun et
al | 15 | Korea | 59 | Male | Fundus | Lamina propria | 3.9×2.7 | LWGR | (11) |
| Agaimy et
al | 16 | Germany | 51 | Male | Body | Lamina propria | 2.0 | Local excision | (12) |
| Agaimy et
al | 17 | Germany | 77 | Female | Body | Lamina propria | 1.0 | Local excision | (12) |
| Agaimy et
al | 18 | Germany | 59 | Female | Body | Lamina propria | 3.0 | Local excision | (12) |
| Agaimy et
al | 19 | Germany | 53 | Male | Antrum | Muscularis
mucosae | 2.0 | Local excision | (12) |
| Agaimy et
al | 20 | Germany | 40 | Male | Body | Lamina propria | 2.0 | Local excision | (12) |
| Agaimy et
al | 21 | Germany | 42 | Female | Body | Lamina propria | 3.0 | Local excision | (12) |
| Agaimy et
al | 22 | Germany | 51 | Male | Body | Lamina propria | 2.2 | Local excision | (12) |
| Pezhouh et
al | 23 | USA | 70 | Female | NA | Submucosa | 1.3 | NA | (13) |
| Pezhouh et
al | 24 | USA | 39 | Male | NA | Submucosa | 1.5 | NA | (13) |
| Pezhouh et
al | 25 | USA | 51 | Female | NA | Serosa | 0.5 | NA | (13) |
| Pezhouh et
al | 26 | USA | 40 | Female | NA | Submucosa | 2.5 | NA | (13) |
| Pezhouh et
al | 27 | USA | 65 | Female | NA | Submucosa | 1.5 | NA | (13) |
| Shi et
al | 28 | China | 58 | Female | Body | Lamina propria | 2.3 | ESD | (14) |
| Shi et
al | 29 | China | 46 | Female | Body | Lamina propria | 1.0 | ESD | (14) |
| Shi et
al | 30 | China | 61 | Male | Body | Lamina propria | 2.0 | EFR | (14) |
| Shi et
al | 31 | China | 53 | Male | Antrum | Lamina propria | 2.5 | EFR | (14) |
| Fan et
al | 32 | China | 49 | Male | Body | NA | 2.0×2.5 | Local excision | (15) |
| Ogasawara et
al | 33 | Japan | 37 | Female | Body | Lamina propria | 1.0 | ESD | (16) |
| George and
Abdeen | 34 | Kuwait | 27 | Female | Fundus | Submucosa | 1.5×1×0.5 | Surgery | (17) |
| Zhang et
al | 35 | China | 55 | Female | Body | Submucosa | 2.0 | ESD | (18) |
| Vasilakaki et
al | 36 | Greece | 60 | Male | Body | Lamina propria | 1.0×0.8 | Local excision | (19) |
| Attila et
al | 37 | Canada | 47 | Female | Body | Mucosa | 2.0×2.0 | LWGR | (20) |
| Elpek et
al | 38 | Turkey | 25 | Man | Body | Submucosa | 1×0.9×0.5 | Urgent surgery | (21) |
| Puccio et
al | 39 | Italy | 49 | Female | Body | NA | NA | LWGR | (22) |
| Štofíková et
al | 40 | Slovakia | 68 | Female | Body | Submucosa | 3.2 | Local excision | (23) |
| Abbadessa et
al | 41 | USA | 17 | Male | NA | NA | NA | LWGR | (24) |
| Lee et
al | 42 | Korea | 49 | Man | Body | Submucosa | 3.0 | Laparoscopic and
endoscopic excision | (25) |
| Liu et
al | 43 | China | 37 | Female | NA | NA | NA | Endoscopic
resection | (26) |
| Lee et
al | 44 | Korea | 5 | Female | Fundus/body | NA | 4.0×3.0 | Total excision | (27) |
| Delbecque et
al | 45 | Switzerland | 63 | Male | Body | Submucosa | 2×1.5×1.5 | Local excision | (28) |
| Azam et
al | 46 | Pakistan | 13 | Male | Fundus | NA | 8.0×6.0×6.0 | Surgery | (29) |
| Chatelain et
al | 47 | France | 50 | Female | Body | NA | 2.0 | Local excision | (30) |
| Jang et
al | 48 | Korea | 43 | Female | Body | Submucosa | 3.0×2.0 | LGWR | (31) |
Discussion
To the best of our knowledge, the present study
reported the largest case series on gastric CFTs to date. Among the
9 gastric CFT patients included in this study, 3 were infected with
HP, and 2 with HBV. Due to the extremely low incidence of this type
of tumor, there is no previous research considering the association
between the occurrence of gastric CFT and HP or HBV. In addition,
the distribution of the 48 reported cases indicated that people
from East Asia may be more likely to suffer from this disease
compared with people from Europe or North America. Whether this is
a coincidence requires further exploration.
At present, the etiology and pathogenesis of CFT
confined to the gastric wall remain elusive (5,11–14). In
a previous study, cases of CFT following trauma were reported, and
it has been speculated that gastric CFT may represent a localized
inflammatory fibrosclerosis in response to tissue injury affecting
the stomach (32). However, no prior
history of any trauma or tissue injuries to the stomach, such as
ulcers or perforation, were identified in the present 9 cases.
Furthermore, previous studies have indicated that these tumors are
true neoplasms, with the potential for non-destructive local
recurrence (33), rather than a
reactive process resulting from abnormal tissue healing (5,7). It has
also been suggested that this lesion results from an immunoglobulin
(Ig)G4-associated disorder (34,35);
gastric CFTs may represent a stage of an IgG4-associated disorder,
and steroid therapy should be included in clinical management prior
to GWE or ESD (18). However, among
the present 9 cases, none of the patients presented with autoimmune
disorders such as primary biliary cirrhosis, chronic atrophic
gastritis, inflammatory bowel disease or IgG4-associated
pancreatitis.
The present study demonstrated that gastric CFT may
have a female predominance (female:male, 2:1), which is consistent
with the previous literature (1.27:1) (5,13).
Including the 9 cases in the current study and the 39 from previous
studies, the sex ratio is 1.4:1. Following age stratification, a
marked difference was identified in the sex ratio of patients above
or below age 50. This suggests that this rare tumor is more common
in female patients, particularly premenopausal women. Based on the
marked difference in sex ratio before and after age 50, it is
speculated that estrogen may serve a role in the occurrence and
progression of gastric CFT.
As estrogen exerts its effects via binding GPER or
ER, the ER and GPER expression status of the patient samples was
detected with immunohistochemistry. Immunostaining was performed on
samples from 9 cases; cells from the lesions exhibited positive
immunoreactivity for GPER, but no immunoreactivity for ER. ER, also
known as classical steroid receptor, is a ligand-activated nuclear
transcription factor that recognizes cis-acting hormone response
elements in the promoters of hormonally regulated genes (36). The present results revealed that the
ER mediation of the classical genomic signal pathway was not
associated with the potential effects of estrogen on the
pathogenesis of gastric CFTs. Thus, any effects of estrogen on this
tumor are likely to be mediated by an alternative pathway. GPER is
a membrane-associated estrogen receptor that can mediate both the
rapid estrogen and traditional genomic estrogen response signal
pathways (36). A previous study
demonstrated that estrogen exerts its physiological effects through
GPER in normal stromal cells (37).
Furthermore, the activation of GPER signaling by estrogen has been
reported to stimulate the formation of fibers in fibroblasts
(38). Therefore, it can be
hypothesized that the activation of GPER by estrogen may promote
the formation of fibers, and even fibrosis, in the stomach.
However, more basic research regarding the effects of estrogen in
gastric CFTs will be required in the future to confirm this
hypothesis.
Gastric CFT is a benign lesion with a good prognosis
that demonstrates a predilection for female patients, especially
premenopausal women. Estrogen mediated by GPER rather than ER may
serve a role in this female predominance. The association between
gastric CFTs and HP or HBV infection remains to be elucidated in
high-calibrated studies.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from the
National Natural Science Foundation of China (grant nos. 81372551
and 81602535).
Availability of data and materials
The data generated during the present study are
available from the corresponding author on reasonable request.
Authors' contributions
ST and WD conceived and designed the present study;
XP performed the literature review; ZZ assessed the
immunohistochemical results; ST wrote the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of the Renmin Hospital of Wuhan University (Wuhan,
China). All patients included in this study provided written
informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rosenthal NS and Abdul-Karim FW: Childhood
fibrous tumor with psammoma bodies. Clinicopathologic features in
two cases. Arch Pathol Lab Med. 112:798–800. 1988.PubMed/NCBI
|
|
2
|
Pinkard NB, Wilson RW, Lawless N, Dodd LG,
McAdams HP, Koss MN and Travis WD: Calcifying fibrous pseudotumor
of pleura: A report of three cases of a newly described entity
involving the pleura. Am J Clin Pathol. 105:189–194. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Van Dorpe J, Ectors N, Geboes K, D'Hoore A
and Sciot R: Is calcifying fibrous pseudotumor a late sclerosing
stage of inflammatory myofibroblastic tumor? Am J Surg Pathol.
23:329–335. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Im S, Jung JH, Yoo C, Choi HJ, Yoo J and
Kang CS: Calcifying fibrous tumor presenting as rectal submucosal
tumor: First case reported in rectum. World J Surg Oncol.
12:282014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chorti A, Papavramidis TS and
Michalopoulos A: Calcifying fibrous tumor. Medicine (Baltimore).
95:e36902016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ma J, Guo X, Zhang J, Wu D, Hu X, Li J,
Lan Q, Liu Y and Dong W: PTEN gene induces cell invasion and
migration via regulating AKT/GSK-3β/β-catenin signaling pathway in
human gastric cancer. Dig Dis Sci. 62:3415–3425. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tanaka H, Baba Y, Matsusaki S, Isono Y,
Saito T, Sase T, Okano H, Mukai K, Taoka H and Murata T: A case of
calcifying fibrous tumor in the abdominal wall, morphologically
resembling a gastric submucosal tumor. Nihon Shokakibyo Gakkai
Zasshi. 111:529–534. 2014.(In Japanese). PubMed/NCBI
|
|
8
|
Liu DD and Song LH: Calcifying fibrous
tumor in gastric wall: Report of a case. Zhonghua Bing Li Xue Za
Zhi. 38:346–347. 2009.(In Chinese). PubMed/NCBI
|
|
9
|
Nascimento AF, Ruiz R, Hornick JL and
Fletcher CD: Calcifying fibrous ‘pseudotumor’: Clinicopathologic
study of 15 cases and analysis of its relationship to inflammatory
myofibroblastic tumor. Int J Surg Pathol. 10:189–196. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kitamura H, Takehara A, Shimada M,
Moriyama H, Saito K, Hada M, Shibahara K, Sasaki M, Konishi K and
Maeda Y: Calcifying fibrous tumor of the gastric wall. Nippon
Shokaki Geka Gakkai Zasshi. 42:1773–1778. 2009. View Article : Google Scholar
|
|
11
|
Yun JK, Park HS, Moon WS, Lee H and Chan
YK: Calcifying fibrous tumor of the stomach: A case report. J
Korean Surg Soc. 83:56–59. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Agaimy A, Bihl MP, Tornillo L, Wünsch PH,
Hartmann A and Michal M: Calcifying fibrous tumor of the stomach:
Clinicopathologic and molecular study of seven cases with
literature review and reappraisal of histogenesis. Am J Surg
Pathol. 34:271–278. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pezhouh MK, Rezaei MK, Shabihkhani M,
Ghosh A, Belchis D, Montgomery EA and Voltaggio L:
Clinicopathologic study of calcifying fibrous tumor of the
gastrointestinal tract: A case series. Hum Pathol. 62:199–205.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Shi Q, Xu MD, Chen T, Zhong YS, Zhou PH,
Wu HF and Yao LQ: Endoscopic diagnosis and treatment of calcifying
fibrous tumors. Turk J Gastroenterol. 25 Suppl 1:S153–S156. 2014.
View Article : Google Scholar
|
|
15
|
Fan SF, Yang H, Li Z and Teng GJ: Gastric
calcifying fibrous pseudotumour associated with an ulcer: Report of
one case with a literature review. Br J Radiol. 83:e188–e191. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ogasawara N, Izawa S, Mizuno M, Tanabe A,
Ozeki T, Noda H, Takahashi E, Sasaki M, Yokoi T and Kasugai K:
Gastric calcifying fibrous tumor removed by endoscopic submucosal
dissection. World J Gastrointest Endosc. 5:457–460. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
George SA and Abdeen S: Gastric calcifying
fibrous tumor resembling gastrointestinal stromal tumor: A case
report. Iran J Pathol. 10:306–309. 2015.PubMed/NCBI
|
|
18
|
Zhang H, Zhu J and Ding S: Gastric
calcifying fibrous tumor: A case of suspected immunoglobulin
G4-related gastric disease. Saudi J Gastroenterol. 21:423–426.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vasilakaki T, Skafida E, Tsavari A,
Arkoumani E, Koulia K, Myoteri D, Grammatoglou X, Moustou E,
Firfiris N and Zisis D: Gastric calcifying fibrous tumor: A very
rare case report. Case Rep Oncol. 5:455–458. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Attila T, Chen D, Gardiner GW, Ptak TW and
Marcon NE: Gastric calcifying fibrous tumour. Can J Gastroenterol.
20:487–489. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Elpek GO, Küpesiz GY and Ogüs M:
Incidental calcifying fibrous tumor of the stomach presenting as a
polyp. Pathol Int. 56:227–232. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Puccio F, Solazzo M, Marciano P and Benzi
F: Laparoscopic resection of calcifying fibrous pseudotumor of the
gastric wall. Surg Endosc. 15:12272001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Štofíková M, Rychlý B, Bocko J and Daniš
D: Submucosal calcifying fibrous tumor of the stomach: A case
report. Cesk Patol. 52:164–167. 2016.PubMed/NCBI
|
|
24
|
Abbadessa B, Narang R, Mehta R, Martinez
J, Leitman IM Jr and Karpeh M: Laparoscopic resection of a gastric
calcifying fibrous pseudotumor presenting with ulceration and
hematemesis in a teenage patient. J Surg Radiol. 4:48–51. 2012.
|
|
25
|
Lee S, Jahng J and Han W: Gastric
calcifying fibrous tumor manifesting as a subepithelial tumor. J
Gastrointest Surg. 22:1127–1129. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Liu Z, Guo J, Ren W, Sun S, Tang S and Xie
L: A gastric calcifying fibrous pseudotumor detected by
transabdominal ultrasound after oral administration of an echoic
cellulose-based gastrointestinal ultrasound contrast agent.
Ultraschall Med. 35:181–183. 2014.PubMed/NCBI
|
|
27
|
Lee D, Suh YL and Lee SK: Calcifying
fibrous pseudotumour arising in a gastric inflammatory
myofibroblastic tumour. Pathology. 38:588–591. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Delbecque K, Legrand M, Boniver J, Lauwers
GY and de Leval L: Calcifying fibrous tumour of the gastric wall.
Histopathology. 44:399–400. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Azam M, Husen YA and Pervez S: Calcifying
fibrous pseudotumor in association with hyaline vascular type
Castleman's disease. Indian J Pathol Microbiol. 52:527–529. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chatelain D, Lauzanne P, Yzet T, Guernou
M, Delcenserie R, Regimbeau JM and Sevestre H: Gastric calcifying
fibrous pseudotumor, a rare mesenchymal tumor of the stomach.
Gastroenterol Clin Biol. 32:441–444. 2008.(In French). View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Jang EY, Kim HJ, Kim JH, Lee SO, Choi K
and Lee HJ: A case of gastric calcifying fibrous tumor presenting
as a subepithelial tumor. Korean J Helicob Upper Gastrointest Res.
13:248–251. 2013. View Article : Google Scholar
|
|
32
|
Zámecník M, Dorociak F and Veselý L:
Calcifying fibrous pseudotumor after trauma. Pathol Int.
47:8121997. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tseng IT, Chen ST, Huang ZZ, Tung HI and
Ker CK: Multiple calcifying fibrous tumors in the small intestine
and the mesentery. Formosan J Surg. 45:33–36. 2012. View Article : Google Scholar
|
|
34
|
Nagai Y, Hayama N, Kishimoto NH, Furuya M,
Takahashi Y, Otsuka M, Miyazaki M and Nakatani Y: Predominance of
lgG4+ plasma cells and CD68 positivity in sclerosing
angiomatoid nodular transformation (SANT). Histopathology.
53:495–498. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yamamoto H, Yamaguchi H, Aishima S, Oda Y,
Kohashi K, Oshiro Y and Tsuneyoshi M: Inflammatory myofibroblastic
tumor versus IgG4-related sclerosing disease and inflammatory
pseudotumor: A comparative clinicopathologic study. Am J Surg
Pathol. 33:1330–1340. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Prossnitz ER, Arterburn JB, Smith HO,
Oprea TI, Sklar LA and Hathaway HJ: Estrogen signaling through the
transmembrane G protein-coupled receptor GPR30. Annu Rev Physiol.
70:165–190. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Prossnitz ER and Hathaway HJ: What have we
learned about G protein-coupled estrogen receptor function in
physiology and disease from knockout mice? J Steroid Biochem Mol
Biol. 153:114–126. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mao S, Wang Y, Zhang M and Hinek A:
Phytoestrogen, tanshinone IIA diminishes collagen deposition and
stimulates new elastogenesis in cultures of human cardiac
fibroblasts. Exp Cell Res. 323:189–197. 2014. View Article : Google Scholar : PubMed/NCBI
|