Introduction
Hip arthroplasty patients suffering from intense
pain is thought to prolong mobilization and hospitalization. It
would be of value to identify good postoperative analgesia, which
may help reduce pain-related multiple problems including anxiety,
emergency agitation, and lack of confidence in medical team.
Different modes of preoperative, intraoperative and postoperative
local analgesic administration have been described in a variety of
surgical procedures, such as tangential excision surgery (1), abdominal hysterectomy (2), orthopaedic surgery (3), and thoracotomy (4). However, few studies have described pre-
and intraoperative analgesia for hip arthroplasty. Pre-and
postoperative administration of valdecoxib reduces the amount of
morphine required for postoperative pain relief and provides
greater analgesic efficacy compared with morphine alone in
orthopedic surgery patients (5).
Intraoperative high-volume local infiltration analgesia with
ropivacaine 0.2% provided no additional reduction in acute pain
after total hip arthroplasty when combined with oral analgesic
regimen consisting of acetaminophen, celecoxib, and gabapentin
(6), but more documentation is
needed.
Postoperative cognitive decline (POCD) is a common
and impactful outcome of surgical procedures in elderly patients
(7). It was thought to be associated
with cardiac surgery although 40% of patients were affected after
non-cardiac surgical procedures. POCD can last for a long period of
time; from a few days to a few years. Patients over 60 reported an
incidence of 25.8% at one week post-surgery and 9.9% at three weeks
post-surgery (8). The
pathophysiology and causative mechanisms for POCD are poorly
understood. Risk factors include advanced age, preoperative
cognitive function, a second operation, length of the operation,
respiratory complications and postoperative infection (9). Thus, POCD is an important concern for
the patients with surgery.
Inflammatory state characterized by the release of
both pro- and anti-inflammatory cytokines is involved in the
occurrence of POCD (10). Increased
levels of pro-inflammatory cytokines are also associated with a
higher incidence of postoperative infections and respiratory
failure (11). Considerable evidence
suggests a correlation between POCD and factors, such as tumor
necrosis factor α (TNF-α), interleukelin-1β (IL-1β), and IL-6
(12,13). However, direct evidence showing a
relationship between POCD and pro-inflammatory cytokines is
lamentably absent from the literature.
Nonsteroidal anti-inflammatory drug (NSAID) with
high affinity to the site of surgical incision and inflammatory
tissues provides postoperative pain relief after different types of
surgery (14). The aims of this
study were to evaluate the postoperative pain, cognitive function
and serum levels of pro-inflammatory cytokines in patients
undergoing hip arthroplasty surgery with pre- or intraoperative
flurbiprofen.
Patients and methods
Selection of patients
One hundred and eighty patients undergoing hip
arthroplasty surgery from June, 2014 to March, 2016 were involved
in this study. The patients were obtained from The Second People's
Hospital of Nantong (Nantong, China). The inclusion criteria were:
i) American Society of Anesthesiologists (ASA) I–II and ii) age
>70 years. The exclusion criteria were: i) patients with a
history of gastric ulcer and duodenal ulcer, ii) patients with a
history of allergic reaction to flurbiprofen, iii) patients with
severe hepatic and renal functional disorders, iv) patients with
ischemic heart disease, and v) patients with general and local
infections.
This randomized and double-blind clinical study was
approved by the Ethics Committee of The Second People's Hospital of
Nantong, and informed consent was obtained from the patients prior
to study enrollment.
Study design
The patients undergoing hip arthroplasty surgery
were randomly divided into three groups (n=60 in each group). The
control group received no treatment before or at the end of
surgery. The PRE group received 50 mg flurbiprofen (Taide
Pharmaceutical Co., Beijing, China) intravenously 15 min before
surgery. The INTRA group received flurbiprofen 30 min before the
end of surgery.
Anesthesia and analgesia
procedures
General anesthesia was induced by intravenous
administration of 0.05 mg/kg midazolam, 0.3 µg/kg sufentanil, 0.3
mg/kg etomidate, and 0.1 mg/kg vecuronium bromide. Anesthesia was
maintained with continuous infusion of 1–3% sevoflurane, 0.5–1
mg/kg/h propofol, 1–2 µg/kg/h sufentanil and additional 10 µg/kg
atropine and 40 µg/kg neostigmine as required after the surgery.
The drug doses were adjusted according to the change of
hemodynamics.
Assessment of pain score and cognitive
function
A physician who was blinded to the group assignment
assessed spontaneous postsurgical pain intensity at rest using a
10-cm visual analog scale (VAS), anchored at ‘no pain’ and ‘worst
pain I can imagine’, at 24 h before surgery (T0), and 3 h (T1), 12
h (T2) and 24 h (T3) after surgery. Another physician who was
blinded to the group assignment assessed cognitive function at T0,
T1, T2 and T3 using mini-mental state examination (MMSE). A score
of 24 out of a possible 30 was considered the cut-off score for
POCD (15).
Determination of the levels of
systemic pro-inflammatory cytokines
Blood samples were collected at the time of T0, T1,
T2 and T3 to measure serum TNF-α, IL-1β, IL-6, and cyclooxygenase-2
(Cox-2) levels. Peripheral venous blood samples were collected and
then centrifuged at 1,000 × g at 4°C for 10 min, and serum samples
were obtained. Serum pro-inflammatory cytokines TNF-α, IL-1β, IL-6,
and Cox-2 levels were measured, using the commercially available
human ELISA kit (Jiancheng Technology Co., Ltd., Nanjing, China) as
described. All steps involved were according to the manufacturers'
protocol.
Statistical analysis
Parametric results were expressed as mean ± standard
deviation for each group. Statistical analysis was performed with
SPSS software, version 17.0 (SPSS, Inc., Chicago, IL, USA).
Student's t-test and one-way ANOVA followed by Turkey's post hoc
test were used for the assessment among the groups. P<0.05 was
considered to indicate a statistically significant difference.
Results
Patient characteristics
In total, 180 patients were involved in the present
study. As shown in Table I, there
were no significant differences in the three groups in terms of
sex, age, weight, height, and operation time.
 | Table I.General data of the three groups (mean
± standard deviation). |
Table I.
General data of the three groups (mean
± standard deviation).
| Items | Control (n=60) | PRE (n=60) | INTRA (n=60) |
|---|
| Sex (F/M) | 28/32 | 22/38 | 24/36 |
| Age (years) | 75.2±5.3 | 78.3±6.1 | 76.1±5.9 |
| Weight (kg) | 59.6±8.7 | 61.5±5.4 | 62.8±7.6 |
| Height (cm) | 164.3±7.5 | 162.8±5.8 | 161.9±6.4 |
| Operation time
(min) | 118.3±20.5 | 123.7±22.9 | 112.1±24.7 |
VAS scores
VAS data are presented in Table II. The results showed there were no
significant differences among the control, PRE and INTRA groups at
24 h before surgery (T0). VAS scores in groups PRE and INTRA were
significantly decreased compared to that in control group at 3
(T1), 12 (T2) and 24 h (T3) after surgery, and the VAS score in the
PRE group was significantly lower than that in the INTRA group at
the time of T1, T2 and T3.
| Table II.VAS score among the three groups (mean
± standard deviation). |
Table II.
VAS score among the three groups (mean
± standard deviation).
| Items | Control (n=60) | PRE (n=60) | INTRA (n=60) |
|---|
| T0 | 1.0±0.5 | 1.3±0.2 | 1.5±0.3 |
| T1 | 5.9±0.8 | 3.2±0.4b,c | 4.3±0.5a |
| T2 | 4.8±0.5 | 2.7±0.4b,c | 3.5±0.2a |
| T3 | 3.5±0.5 | 1.8±0.3b,c | 2.5±0.3a |
MMSE scores
To further investigate the efficacy of flurbiprofen,
we assessed the cognitive function by MMSE. As shown in Table III, there was no significant
difference among the three groups at T0. The MMSE scores at T1, T2
and T3 in PRE and INTRA group were significantly higher than that
in the control group, and the MMSE score in the PRE group was
significantly higher than that in the INTRA group at the time of
T1, T2 and T3.
| Table III.MMSE score in the three groups (mean ±
standard deviation). |
Table III.
MMSE score in the three groups (mean ±
standard deviation).
| Items | Control (n=60) | PRE (n=60) | INTRA (n=60) |
|---|
| T0 | 28.9±1.2 | 29.5±0.8 | 28.1±1.4 |
| T1 | 20.4±0.8 | 24.8±0.9b,c |
23.1±0.5a |
| T2 | 21.1±0.9 |
26.8±1.3b,c |
24.1±0.8a |
| T3 | 22.8±1.3 |
28.8±1.4b,c |
25.7±1.2a |
Serum levels of pro-inflammatory
cytokines
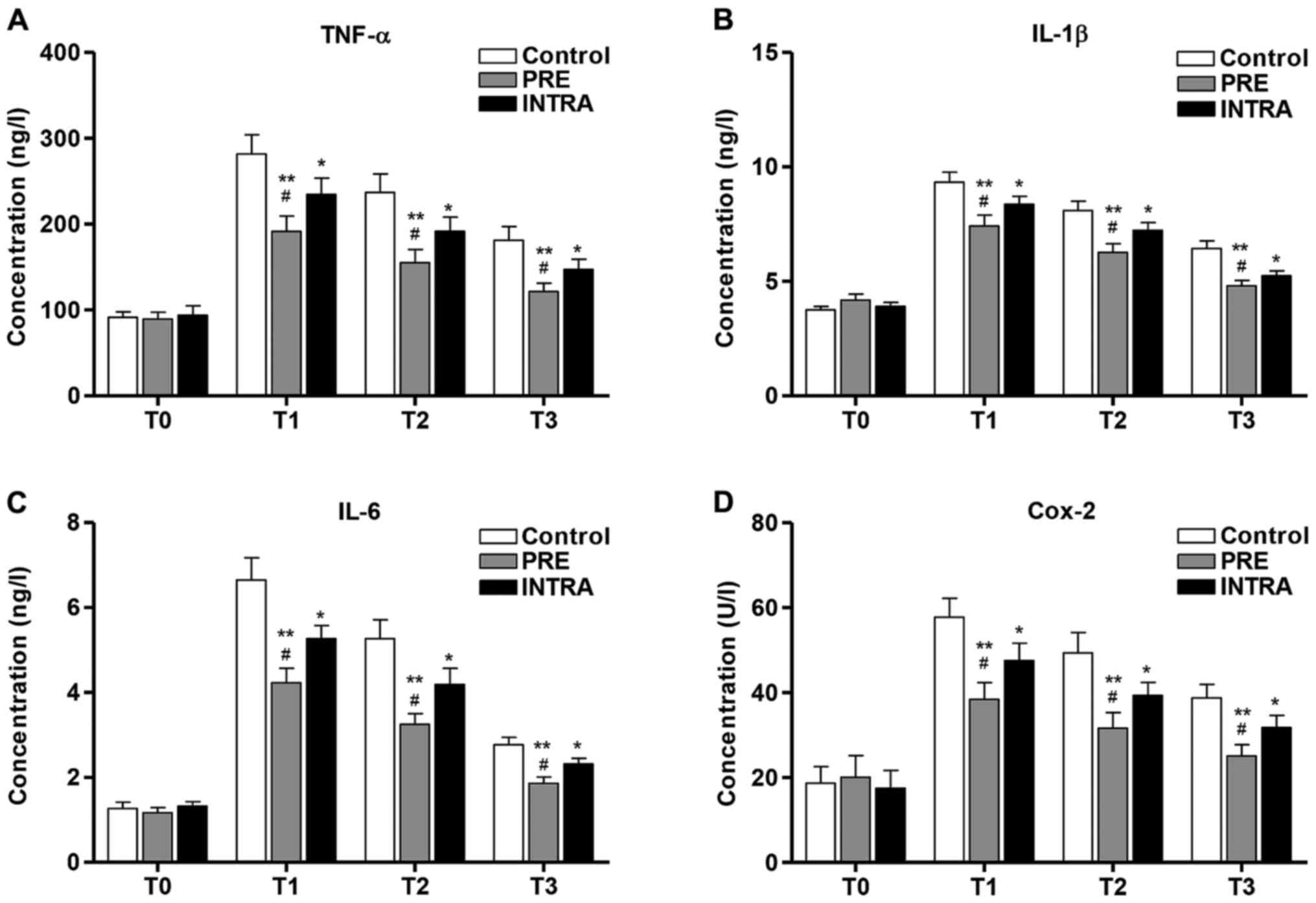
We investigated the anti-inflammatory effects of
flurbiprofen in patients undergoing hip arthroplasty surgery. As
shown in Fig. 1A-D, postoperative
increases in serum TNF-α, IL-1β, IL-6 and Cox-2 concentrations were
observed among the three groups. Serum TNF-α, IL-1β, IL-6 and Cox-2
levels did not differ significantly in T0 among the three groups.
However, TNF-α, IL-1β, IL-6 and Cox-2 levels were significantly
decreased in the PRE and INTRA groups compared to that in the
control group, and the pro-inflammatory cytokines were
significantly lower in the PRE group than that in the INTRA group
at the time of T1, T2 and T3.
Discussion
Previous studies reported attentional dysfunction as
sensitive and prominent characteristics of POCD (16). The clinical significance of POCD is
evidenced by the impact that daily activities confers particularly
on the elderly patients (17). The
cohort study confirms that there is a significantly increased
incident of cognitive dysfunction in patients over 70 undergoing
non-cardiac surgery, and emphasized by the evidence that
preoperative or intraoperative intravenous administration of
flurbiprofen reduces the level of cognitive dysfunction at 3, 12
and 24 h after hip arthroplasty surgery. In line with our findings
that a greater level of cognitive dysfunction is still observed
after 52 weeks in people over 60 undergoing abdominal or
orthopaedic surgery in comparison to age-matched controls (3). Despite the persistent impact of POCD on
mortality and welfare of patients was not included in the present
study the cognitive impairment was indeed observed during the
period of 24 h after surgery, highlighting the clinical importance
of POCD and its long time impact on cognition in the patients with
non-cardiac surgery.
VAS scoring is a simple and commonly used method for
evaluating variations in pain intensity in the early postoperative
period. VAS scoring was used for evaluating postoperative pain in
different studies, including total hip arthroplasty (14), spinal fusion (18), abdominal (19), and minor gynecological surgery
(20). In the present study,
postoperative VAS scores were significantly increased compared with
preoperative controls, while preoperative or intraoperative
flurbiprofen administration reduced postoperative pain induced by
surgery after 3, 12 and 24 h, which is in line with a previous
study (21). MMSE is a brief test of
cognitive impairment used widely to screen for dementia. The
original test, developed by Folstein et al, includes
questions about orientation, attention, recall, and language
(22). In the present study, the
MMSE measure was used to analyze the level of cognitive decline and
similar to the previous study that postoperative MMSE scores were
significantly decreased compared with preoperative controls, while
preoperative or intraoperative flurbiprofen administration improved
POCD evidenced by increased MMSE scores induced by surgery after 3,
12 and 24 h (23).
Pro-inflammatory cytokine response induced by
surgical damage has been reported and is thought to provide a
source of postoperative sensory signals and induce central
sensitization (24). Moreover, a
meta-analysis strengthens the clinical evidence that POCD is
accompanied by a peripheral inflammatory reaction (13). IL-6 and TNF-α are major mediators of
the acute-phase protein response to tissue damage caused by
surgical intervention. Furthermore, it has been reported that
postoperative IL-6 levels correlate with postoperative
complications and mortality, and might have contribution to the
occurrence of POCD (13). IL-1β is a
pro-inflammatory cytokine that contributes to neuro-inflammation in
many central nervous system (CNS) disorders (25). Studies have shown that Cox-2
inhibitor impeded neuro-inflammation and induced amelioration of
cognitive function in patients with Alzheimer disease, suggesting a
critical role of Cox-2 in driving the pathogenesis of cognitive
decline after surgery (26). In the
present study, the concentrations of TNF-α, IL-1β, IL-6 and Cox-2
increased significantly in the patients after hip arthroplasty
surgery compared to before. There was a significant increase in
TNF-α, IL-1β, IL-6 and Cox-2 concentration at 3 h after surgery,
although IL-1β protein was significantly increased at 24 h after
surgery and no increase in protein expression of TNF-α (27). Importantly, preoperative or
intraoperative flurbiprofen administration reduced the increase in
the concentrations of TNF-α, IL-1β, IL-6 and Cox-2 induced by
surgery after 3, 12 and 24 h.
Although some clinical studies have conflicting
results regarding the efficacy of preemptive analgesia, it is to
give a first dose of analgesics before pain stimulation and has
been regarded as a new concept to enhance the postoperative
analgesia. Flurbiprofen, an injectable NSAID, is an effective and
safe analgesic providing postoperative pain relief after different
surgery. However, the efficacy of pre-emptive analgesia with NSAID
remains disputed. Preoperative administration of piroxicam
sublingually would reduce postoperative pain and opioid
requirements more than would postoperative piroxicam (28). Nimesulide is a well-tolerated oral
anti-inflammatory drug with a superior analgesic activity compared
with naproxen and placebo after out-patient orthopedic surgery
(29). Moreover, a combination of
paracetamol and an NSAID may offer superior analgesia compared with
either drug alone (30). Intravenous
flurbiprofen reduces postoperative rescue analgesic requirement
after abdominal hysterectomy, and is more effective when given
before than after surgery (2). In
the present study, we consider that flurbiprofen reduced the
postoperative pain and the occurrence of POCD evidenced by
increased MMSE scores after surgery through preoperative or
intraoperative administration. Importantly flurbiprofen is more
effective when given preoperatively than intraoperatively. This is
the first report that intraoperatively administrated flurbiprofen
confers a postoperative pain relief for hip arthroplasty surgery,
although the efficacy is less than preoperatively.
Other anti-postoperative pain effect of
flurbiprofen, anti-inflammatory response was also found in variety
of studies and correlated with the occurrence of POCD. Zhang et
al found that preoperative flurbiprofen can effectively inhibit
pro-inflammatory cytokines, maintain the balance of cytokines and
reduce myocardiac injury, and be beneficial to patients with early
rehabilitation after operation (31). Thus, we speculated that flurbiprofen
is a suitable NSAID to induce a preemptive effect. Geng et
al found that preoperative administration of flurbiprofen
reduced the plasma levels of TNF-α and IL-6, and was further
reduced by postoperative administration of flurbiprofen at 24 and
48 h after the operation (1).
Consistent with the above findings, we found that preoperative or
intraoperative administration of flurbiprofen, especially
intraoperative flurbiprofen significantly decreased the
concentrations of TNF-α, IL-1β, IL-6 and Cox-2 at 3, 12, and 24 h
after surgery, indicating that analgesia with anti-inflammatory
drug may contribute to the attenuation of the postoperative
inflammatory response and prevent postoperative pain in patients
undergoing hip arthroplasty.
We conclude that the preoperative or intraoperative
intravenous administration of flurbiprofen is effective in reducing
postoperative pain and the occurrence of POCD, as well as the
concentrations of pro-inflammatory cytokines. Moreover,
flurbiprofen is more effective when given preoperatively than
intraoperatively.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
JT and WHL performed experiments and data analysis;
and ZJZ and WDT designed the project and wrote the study. All
authors read and approved the study.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
the Second People's Hospital of Nantong (Nantong, China). Signed
informed consents were obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Geng W, Hong W, Wang J, Dai Q, Mo Y, Shi
K, Sun J, Qin J, Li M and Tang H: Flurbiprofen axetil enhances
analgesic effects of sufentanil and attenuates postoperative
emergence agitation and systemic proinflammation in patients
undergoing tangential excision surgery. Mediators Inflamm.
2015:6010832015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nakayama M, Ichinose H, Yamamoto S,
Nakabayashi K, Satoh O and Namiki A: Perioperative intravenous
flurbiprofen reduces postoperative pain after abdominal
hysterectomy. Can J Anaesth. 48:234–237. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ballard C, Jones E, Gauge N, Aarsland D,
Nilsen OB, Saxby BK, Lowery D, Corbett A, Wesnes K, Katsaiti E, et
al: Optimised anaesthesia to reduce post operative cognitive
decline (POCD) in older patients undergoing elective surgery, a
randomised controlled trial. PLoS One. 7:e374102012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Esme H, Kesli R, Apiliogullari B, Duran FM
and Yoldas B: Effects of flurbiprofen on CRP, TNF-α, IL-6, and
postoperative pain of thoracotomy. Int J Med Sci. 8:216–221. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Camu F, Beecher T, Recker DP and Verburg
KM: Valdecoxib, a COX-2-specific inhibitor, is an efficacious,
opioid-sparing analgesic in patients undergoing hip arthroplasty.
Am J Ther. 9:43–51. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lunn TH, Husted H, Solgaard S, Kristensen
BB, Otte KS, Kjersgaard AG, Gaarn-Larsen L and Kehlet H:
Intraoperative local infiltration analgesia for early analgesia
after total hip arthroplasty: A randomized, double-blind,
placebo-controlled trial. Reg Anesth Pain Med. 36:424–429. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Silbert B, Evered L and Scott DA:
Cognitive decline in the elderly: Is anaesthesia implicated? Best
Pract Res Clin Anaesthesiol. 25:379–393. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moller JT, Cluitmans P, Rasmussen LS, Houx
P, Rasmussen H, Canet J, Rabbitt P, Jolles J, Larsen K, Hanning CD,
et al; International Study of Post-Operative Cognitive Dysfunction,
. Long-term postoperative cognitive dysfunction in the elderly
ISPOCD1 study. ISPOCD investigators. Lancet. 351:857–861. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Newman S, Stygall J, Hirani S, Shaefi S
and Maze M: Postoperative cognitive dysfunction after noncardiac
surgery: A systematic review. Anesthesiology. 106:572–590. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Fidalgo AR, Cibelli M, White JP, Nagy I,
Maze M and Ma D: Systemic inflammation enhances surgery-induced
cognitive dysfunction in mice. Neurosci Lett. 498:63–66. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Takeda S, Takeda S, Kim C, Ikezaki H,
Nakanishi K, Sakamoto A, Okawa K, Miyashita M, Sasajima K, Tajiri
T, et al: Preoperative administration of methylprednisolone
attenuates cytokine-induced respiratory failure after esophageal
resection. J Nippon Med Sch. 70:16–20. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cibelli M, Fidalgo AR, Terrando N, Ma D,
Monaco C, Feldmann M, Takata M, Lever IJ, Nanchahal J, Fanselow MS,
et al: Role of interleukin-1β in postoperative cognitive
dysfunction. Ann Neurol. 68:360–368. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Peng L, Xu L and Ouyang W: Role of
peripheral inflammatory markers in postoperative cognitive
dysfunction (POCD): A meta-analysis. PLoS One. 8:e796242013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Andersen LJ, Poulsen T, Krogh B and
Nielsen T: Postoperative analgesia in total hip arthroplasty: A
randomized double-blinded, placebo-controlled study on peroperative
and postoperative ropivacaine, ketorolac, and adrenaline wound
infiltration. Acta Orthop. 78:187–192. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Galea M and Woodward M: Mini-mental state
examination (MMSE). Aust J Physiother. 51:1982005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
van Dijk D, Keizer AM, Diephuis JC, Durand
C, Vos LJ and Hijman R: Neurocognitive dysfunction after coronary
artery bypass surgery: A systematic review. J Thorac Cardiovasc
Surg. 120:632–639. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kojima Y and Narita M: Postoperative
outcome among elderly patients after general anesthesia. Acta
Anaesthesiol Scand. 50:19–25. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yamashita K, Fukusaki M, Ando Y, Fujinaga
A, Tanabe T, Terao Y and Sumikawa K: Preoperative administration of
intravenous flurbiprofen axetil reduces postoperative pain for
spinal fusion surgery. J Anesth. 20:92–95. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
McDonnell JG, O'Donnell B, Curley G,
Heffernan A, Power C and Laffey JG: The analgesic efficacy of
transversus abdominis plane block after abdominal surgery: A
prospective randomized controlled trial. Anesth Analg. 104:193–197.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Paech MJ, Goy R, Chua S, Scott K,
Christmas T and Doherty DA: A randomized, placebo-controlled trial
of preoperative oral pregabalin for postoperative pain relief after
minor gynecological surgery. Anesth Analg. 105:1449–1453. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Takada M, Fukusaki M, Terao Y, Yamashita
K, Inadomi C, Takada M and Sumikawa K: Preadministration of
flurbiprofen suppresses prostaglandin production and postoperative
pain in orthopedic patients undergoing tourniquet inflation. J Clin
Anesth. 19:97–100. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Folstein MF, Folstein SE and McHugh PR:
‘Mini-mental state’. A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res. 12:189–198.
1975. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kan ZY, Hu J and Wang F: Effect of
Flurbiprofen on postoperative cognition and inflammatory cytokines
in elderly male patients. Practical J Clin Med. 2:81–83. 2012.(In
Chinese).
|
|
24
|
Rosczyk HA, Sparkman NL and Johnson RW:
Neuroinflammation and cognitive function in aged mice following
minor surgery. Exp Gerontol. 43:840–846. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu MD, Montgomery SL, Rivera-Escalera F,
Olschowka JA and O'Banion MK: Sustained IL-1β expression impairs
adult hippocampal neurogenesis independent of IL-1 signaling in
nestin+ neural precursor cells. Brain Behav Immun.
32:9–18. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Peng M, Wang YL, Wang FF, Chen C and Wang
CY: The cyclooxygenase-2 inhibitor parecoxib inhibits
surgery-induced proinflammatory cytokine expression in the
hippocampus in aged rats. J Surg Res. 178:e1–e8. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wan Y, Xu J, Ma D, Zeng Y, Cibelli M and
Maze M: Postoperative impairment of cognitive function in rats: A
possible role for cytokine-mediated inflammation in the
hippocampus. Anesthesiology. 106:436–443. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Gramke HF, Petry JJ, Durieux ME, Mustaki
JP, Vercauteren M, Verheecke G and Marcus MA: Sublingual piroxicam
for postoperative analgesia: preoperative versus postoperative
administration: a randomized, double-blind study. Anesth Analg.
102:755–758. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Binning A: Nimesulide in the treatment of
postoperative pain: A double-blind, comparative study in patients
undergoing arthroscopic knee surgery. Clin J Pain. 23:565–570.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ong CK, Seymour RA, Lirk P and Merry AF:
Combining paracetamol (acetaminophen) with nonsteroidal
antiinflammatory drugs: A qualitative systematic review of
analgesic efficacy for acute postoperative pain. Anesth Analg.
110:1170–1179. 2010.PubMed/NCBI
|
|
31
|
Zhang Y, Gu E and Liu X: Effects of
flurbiprofen axetil on inflammatory cytokines and myocardiac injury
in patients undergoing cardiac valve replacement surgery with
cardiopulmonary bypass. Acta Univ Med Anhui. 1:92–95. 2009.(In
Chinese).
|