Introduction
Periodontal diseases are bacteria-induced chronic
inflammatory diseases which affect the teeth-supporting tissues and
are highly prevalent worldwide (1).
Periodontitis is one of the most common forms of periodontal
disease and is characterized by periodontal pocket formation,
attachment loss and alveolar bone resorption. Periodontal therapy
aims to achieve periodontal regeneration by reforming gingival
connective tissue, cementum and alveolar bone (2). Unfortunately, due to the complex and
particular etiology of periodontitis and the periodontal
microenvironment, traditional treatment strategies fail to repair
damage through periodontal disease completely (3). With the increasing knowledge of stem
cells and tissue engineering, stem cell-based therapy is a
promising candidate for periodontal regeneration and identifying
the ideal seed cells which is an important part (4).
Mesenchymal stem cells (MSCs) emerged as an
alternative cell source for tissue engineering due to their
self-renewal ability and multi-differentiation potential (5). Bone marrow stromal cells (BMSCs) and
several kinds of dental mesenchymal stem cells have been proved to
promote periodontal regeneration (6). Dental mesenchymal stem cells are MSCs
that are harvested from a dental body and subsidiary tissue,
including the periodontal ligament (7), dental pulp (8) and dental follicle (9). However, certain drawbacks and
limitations hinder the common application of these MSCs. For
instance, the process of bone marrow isolation is an invasive
procedure for donors and the yield of BMSCs is small. The
proliferative and differentiation potential of BMSCs decrease
during long-term culture and certain specific growth factors are
usually needed to prolong the lifespan and differentiation ability
of BMSCs (10). Dental MSCs are
generally obtained from extracted teeth, but these cells are also
not commonly isolated or cultured. The gingival MSCs (GMSCs) are
stem cells derived from gingival tissue in recent years, which
possess MSC characteristics including self-renewal, clonogenicity,
multi-differentiation and expression of MSCs associated surface
markers (11). GMSCs are easy to
isolate and exhibit a stable phenotype, maintain a normal karyotype
and telomerase activity in long-term cultures. GMSCs have been
confirmed to participate in periodontal defect regeneration in
animal models (12,13). In the previous study, green
fluorescent protein (GFP)-labeled GMSCs transplanted via the tail
vein into mice with mandibular bone defects were demonstrated to
home to the defect sites and promoted bone regeneration (14). However, the effect of systemically
transplanted GMSCs on periodontitis in mice is still unknown.
In the present study, GMSCs labeled with GFP were
transplanted into C57BL/6J mice with periodontitis in the second
maxillary molar induced by silk thread ligation. GFP detection,
morphometric and histopathological analysis were performed to
evaluate the contribution of GMSCs to periodontitis.
Materials and methods
Animals
A total of 36 C57BL/6J mice (weight, 21.08±2.14 g)
were obtained from the Peking University Health Science Center
(Beijing, China) and kept under specific-pathogen-free conditions
with controlled temperature (22±2°C), humidity (60%) and lighting
(12-h light/dark cycle), and access to sterile food and water. Mice
were used for experiments at the age of 8 weeks. All
animal-experiment procedures described in this study were reviewed
and approved by the Institutional Animal Care and Use Committee of
Qingdao University, (Qingdao, China).
Isolation of GMSCs
Human gingival samples were harvested from four
healthy volunteers (2 males and 2 females; age, 18–25 years) who
underwent routine dental procedures at the Department of
Stomatology, Affiliated Hospital of Medical College, Qingdao
University were obtained. All procedures are approved by the
clinical research ethics committee of Qingdao University and
informed consent was provided. The gingival tissues were washed
several times by PBS containing 400 µg/ml streptomycin and 400 U/ml
penicillin and the tissues were incubated overnight with α-minimum
essential medium (MEM; Hyclone, Logan, Utah, USA) containing 2
mg/ml dispase (Sigma-Aldrich; Merck KGaA, Darmstadt, Germany) at
4°C. Following the epithelial layer separation, the connective
tissues were minced into fragments and digested with 2 mg/ml
collagenase (Sigma-Aldrich; Merck KGaA) at 37°C for 40 min. The
tissue explants were placed into a 25 mm2 culture flask
containing α-MEM medium with 15% fetal bovine serum (FBS; Hyclone)
at 37°C in 5% CO2. The cell medium was changed every 3
days and cells were subcultured at 80% confluence using 0.25%
trypsin/EDTA solution (Beijing Solarbio Science & Technology
Co., Ltd., Beijing, China).
Colony-forming unit-fibroblast (CFU-F)
assay
Assessing the colony forming efficiency of GMSCs, a
CFU-F assay was performed. A total of 500 cells of passage 1 were
seeded in a 60 mm petri dish. The culture medium (α-MEM with 10%
FBS) was replaced every 3 days. After 14 days, cells were fixed
with 4% paraformaldehyde at room temperature for 30 min, and
stained with 0.1% crystal violet (Beijing Solarbio Science &
Technology Co., Ltd.) at room temperature for 10 min, then cells
were washed with distilled water and dried. The cells counted by an
inverted light microscope. A cluster of 50 or more cells was scored
as a CFU-F.
Adipogenic differentiation
The forth-passage GMSCs were seeded in 24-well
plates (5×103 cells/well) in the α-MEM growth medium.
Following 24 h, the medium was replaced by adipogenic medium (α-MEM
containing 10% FBS, 0.5 mM IBMX, 200 µM indomethacin, 10 µM insulin
and 10 µM dexamethasone; Sigma-Aldrich; Merck KGaA). Cells which
cultured in α-MEM containing 10% FBS were as the control group.
Cells were stained with Oil Red O (Beijing Solarbio Science &
Technology Co., Ltd.) at room temperature for 10 min to identify
the oil globules under light microscopy after two weeks.
Osteogenic differentiation
The forth-passage GMSCs were seeded in 24-well
plates (5×103 cells/well) in α-MEM growth medium. After
24 h the culture medium was replaced with osteogenic medium (α-MEM
containing 5% FBS, 50 µM ascorbate-2-phosphate, 10 mM
β-glycerophosphate and 0.1 µM dexamethasone; Sigma-Aldrich; Merck
KGaA). The cells which cultured in α-MEM containing 5% FBS were as
the control group. Cells were characterized by Alizarin Red S
(Beijing Solarbio Science & Technology Co., Ltd.) to identify
the mineral nodules after 4 weeks.
Flow cytometry
GMSCs (1×106) at passage 4 were collected
and washed twice by PBS, and then the cells were incubated with
monoclonal fluorescein isothiocyanate-conjugated anti-human
antibodies for CD45 (cat. no. 368507), CD73 (cat. no. 344015), CD90
(cat. no. 328107) and phycoerythrin-conjugated anti-human
antibodies for CD105 (cat. no. 323205) (BioLegend, Inc., San Diego,
CA, USA) at 4°C for 40 min in the dark. After the incubation, cells
were washed three times and fixed in 1% paraformaldehyde at room
temperature for 30 min. The suspension was analyzed by flow
cytometer (Beckman Coulter, Inc., Brea, CA, USA).
GFP transfection of GMSCs
Tracing the fate of GMSCs in mice, the lentiviral
vectors with GFP (Shanghai Genechem, Co., Ltd., Shanghai, China)
were used to label GMSCs. The first-passage GMSCs (2×103
cells/well) were seeded in 6-well plates for 24 h. Then the culture
medium was replaced with virus solution diluted by serum-free
α-MEM. The viral solution was replaced with complete culture medium
following transfection for 8 h. The GFP+ GMSCs were
expanded and cells from the third to fifth passage (following ~2
weeks of culture) were transplanted into animals.
Animal surgery and GMSCs
transplantation
After mice were anesthetized by intraperitoneal
injection of 10% chloral hydrate, a 5-0 silk ligature was placed on
the two maxillary second molars. The ligature was tied firmly with
a triple-knot on the buccal side of the maxillary second molar and
left for 4 weeks. The mice were randomly divided into group A and
B. Silk ligatures were removed after the maxillary second molars
had been tied for 4 weeks and 500 µl α-MEM containing
1×106 GMSCs were injected into Group A mice via the tail
vein. Group B mice were injected with 500 µl α-MEM as the control
group. At 1, 2 and 4 weeks post-injection in this study, mice were
sacrificed with carbon dioxide and this was confirmed by mice
exhibiting a lack of pulse, breathing, corneal reflex and response
to firm toe pinch. In addition, peritonitis was not observed in the
mice during the experiment.
Tissue preparation and
histopathological analysis
The left maxillaries were isolated following
perfusion-fixation with 4% paraformaldehyde at room temperature for
~20 min. The tissues were embedded in paraffin following
demineralization in 10% EDTA (Beijing Solarbio Science &
Technology Co., Ltd.) for 4 weeks. Tissue sections, 3-µm thick,
were cut in the mesial-distal direction. The nearest segments to
the central area were selected. Two sections were stained with
hematoxylin and eosin (HE; for 5 min and 30 sec, respectively) and
Masson trichrome (MT; Weigert's hematoxylin, 10 min; acid ponceau,
5 min; 1% acetic acid, 1 min), respectively, at room temperature.
Images were taken under a light microscope at ×100
magnification.
Fluorescent microscope
observation
To trace the fate of GMSCs in periodontitis mice,
fluorescent microscope observation and immunohistochemical staining
were performed. The rehydrated sections were washed with PBS for 5
min and then stained with DAPI (Beijing Solarbio Science &
Technology Co., Ltd.) at room temperature for 5 min. The slices
were observed under a fluorescent microscope after washing with
PBS.
Immunohistochemical staining for
GFP
Immunohistochemical study was performed using a
rabbit monoclonal antibody (1:100; cat. no. AB183734; Abcam,
Cambridge, USA) against GFP. Sections were treated with 3%
H2O2 for 10 min to block peroxidase activity
following dewaxing and hydrating. Then the sections were incubated
with the primary antibody at 37°C for 90 min, washed by PBS and
incubated with the horseradish peroxidase-conjugated anti-rabbit
secondary antibody (PV-6001; 1:10; Origene Technologies, Inc.,
Beijing, China) at 37°C for 30 min. Nuclear staining was performed
with hematoxylin at room temperature for 5 min.
Morphometric analysis of alveolar bone
loss
The right maxillaries were boiled for 10 min under 1
bar pressure to remove the soft tissue and then maxillaries were
soaked in hydrogen peroxide solution for 12 h. Maxillaries were
washed by PBS after staining with methylene blue at room
temperature for 10 min. Images of maxillary molar and alveolar were
captured under a stereo microscope and assessed by Image-Pro-Plus
6.0 software (Media Cybernetics, Inc., Rockville, MD, USA).
Alveolar bone losses were measured as the sum of distances from
cementoenamel junction (CEJ) to the alveolar bone crest (ABC) at 6
sites (mesio-palatal cusp, palatal groove, disto-palatal cusp,
mesio-buccal cusp, buccal groove and disto-buccal cusp).
Statistical analysis
All data were expressed as the mean ± standard
deviation. Statistical analysis was performed using a statistical
package SPSS 19.0, (IBM, Corps., Armonk, NY, USA). Alveolar bone
loss levels of the two groups were assessed with an
independent-samples t-test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Characterization and transfection of
GMSCs
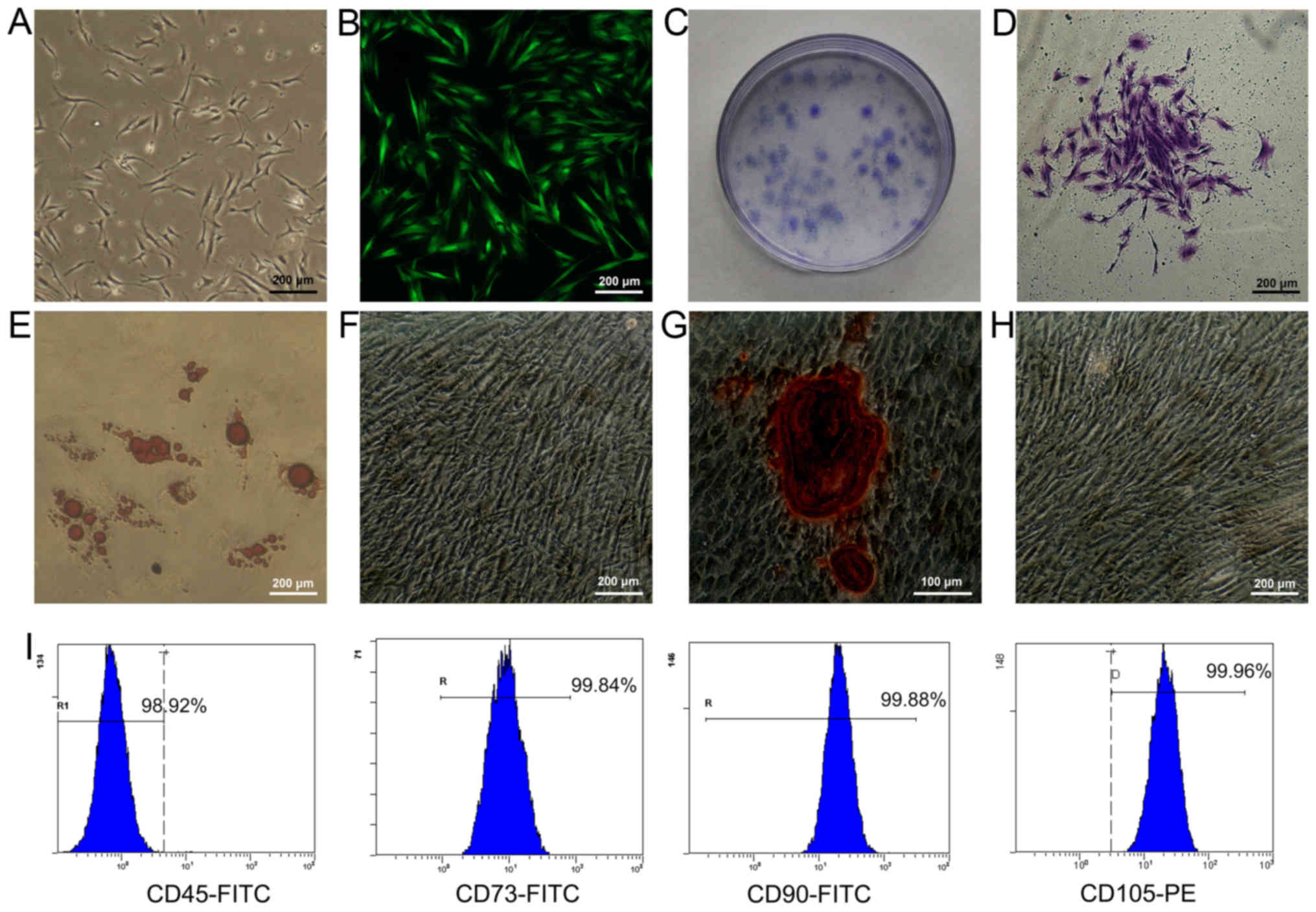
The adherent GMSCs were observed 5–7 d following
initiation of the primary culture and reaching 80% confluence by
14–21 d. Under an optical microscope, the primary GMSCs
demonstrated a fibroblast-like spindle shape (Fig. 1A). At 72 h post-transfection, stable
expression of GFP could be observed under the fluorescence
microscope and GMSCs with stable GFP expression were subcultured
(Fig. 1B). A large number of
colonies (19±6%) were identified following crystal violet staining
(Fig. 1C and D). As GMSCs had been
cultured in the adipogenic medium for 2 weeks, lipid-rich globules
were confirmed by Oil Red O staining in the cytoplasm of
differentiated cells (Fig. 1E).
Furthermore, no positive cells were detected in the control group,
which was cultured with standard medium (Fig. 1F). When GMSCs had been cultured in
the osteogenic medium for 4 weeks, mineralized nodules were
observed following Alizarin Red S staining (Fig. 1G). So, no positive cells were
detected in the control group, which was cultured with standard
medium (Fig. 1H). Flow cytometry
analysis revealed that GMSCs were positive for MSCs markers CD73,
CD90 and CD105 and expression percentages were >95% for all. In
addition, GMSCs were negative for hematopoietic cell marker CD45
with an expression percentage <2% (Fig. 1I).
Alveolar bone loss determination
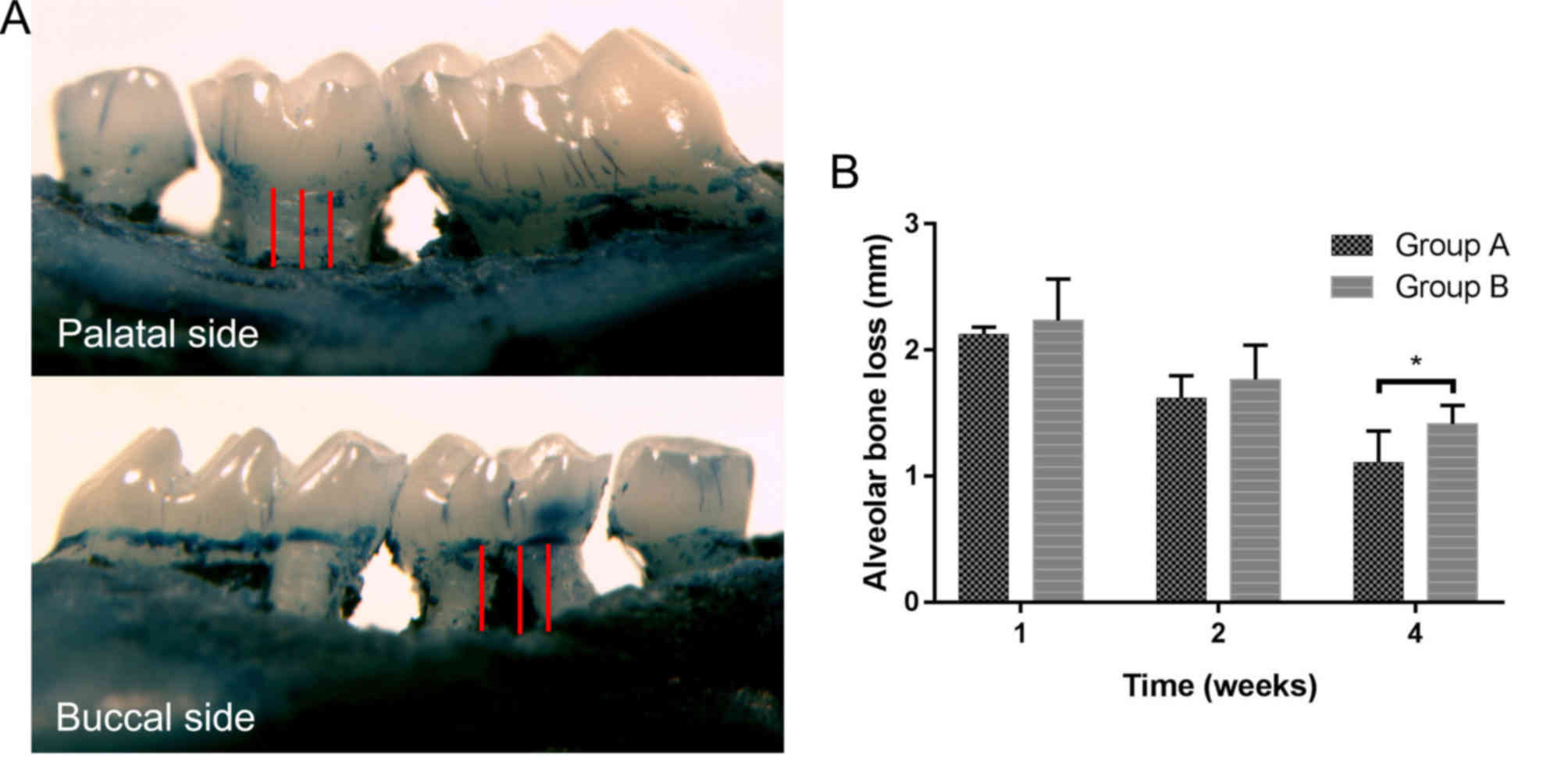
The alveolar bone loss was measured as the distance
from the CEJ to ABC. At week 1 and 2 following cell
transplantation, there were non-significant differences between
group A and B. However, alveolar bone loss in group A was
significantly decreased compared with group B by the 4th week
(Table I; P<0.05; Fig. 2), which indicated promotion of
systemically transplanted GMSCs on alveolar bone regeneration.
 | Table I.Alveolar bone loss levels of the two
groups at 1, 2 and 4 weeks post-transplantation (mean ± standard
deviation; mm, n=6). |
Table I.
Alveolar bone loss levels of the two
groups at 1, 2 and 4 weeks post-transplantation (mean ± standard
deviation; mm, n=6).
| Group | 1 W | 2 W | 4 W |
|---|
| A | 2.12±0.59 | 1.61±0.18 |
1.11±0.25a |
| B | 2.23±0.33 | 1.77±0.27 | 1.41±0.15 |
Histopathological analysis
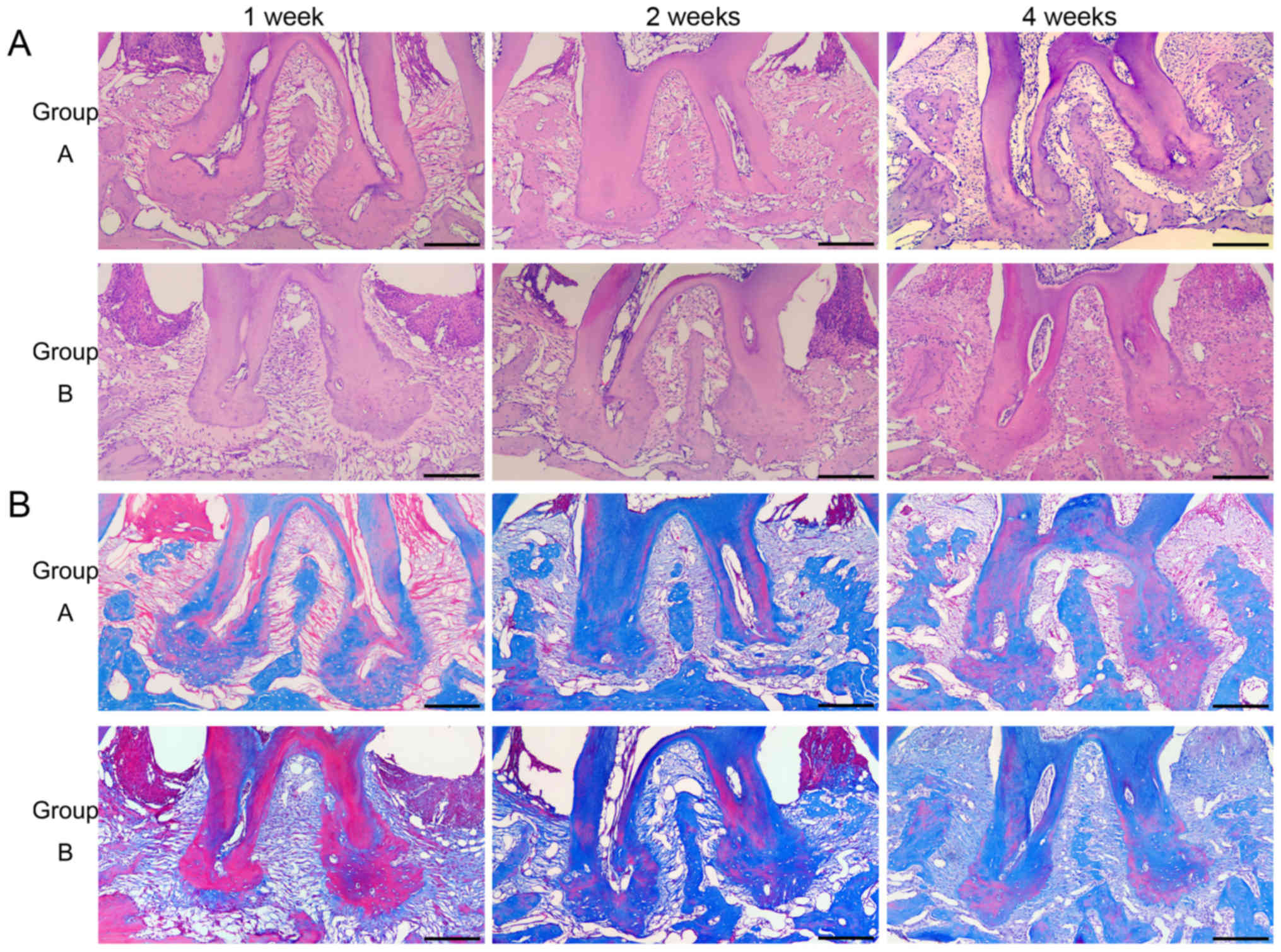
Histopathological changes of root furcation were
observed by HE and MT staining. At the 1st week and 2nd-week
post-transplantation, inflammatory cell infiltration, deep
periodontal pockets, attachment loss and severe alveolar bone
destruction was detected in the two groups by HE staining (Fig. 3A). MT staining demonstrated almost
all of alveolar bone was blue stained. At the 4th week
post-transplantation, alveolar bone loss of group A was
significantly decreased compared with group B (Table I). There was more reddish mature
stained bone in group A than group B (Fig. 3B).
Homing properties of GMSCs
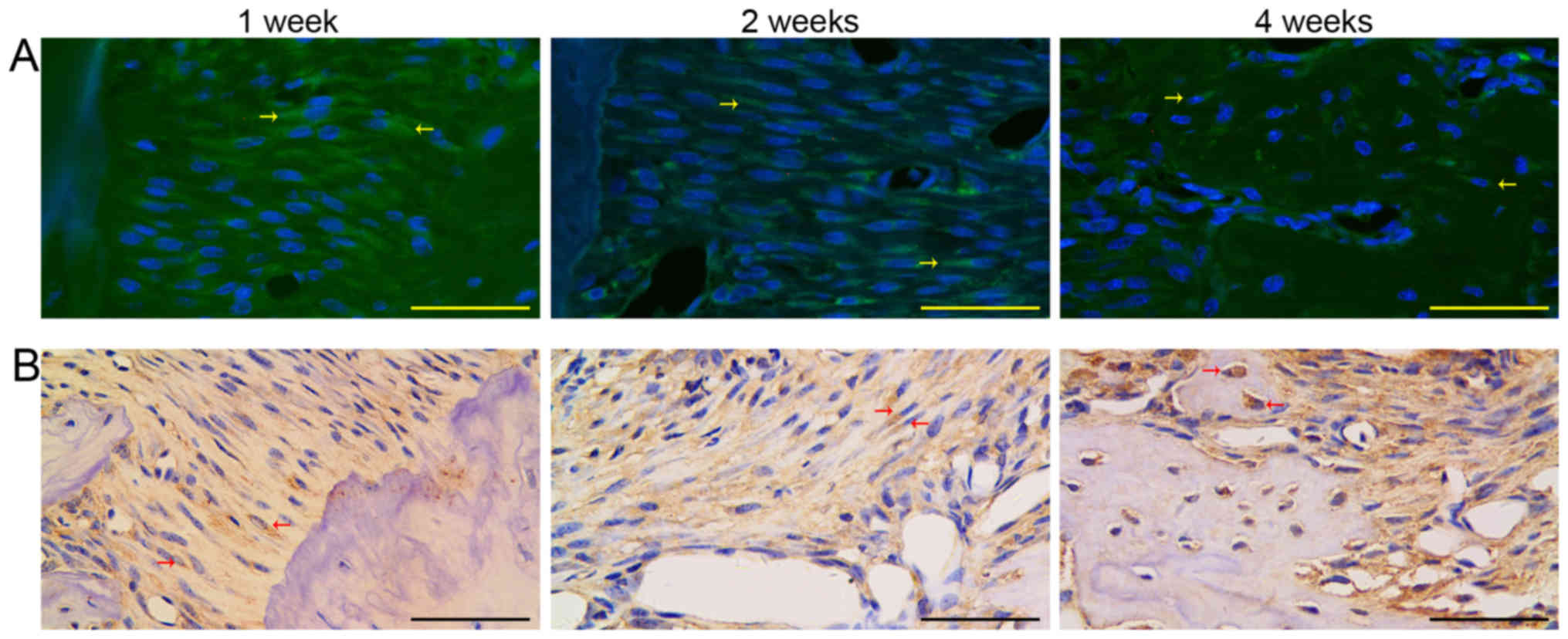
GFP-positive cells were detected by fluorescence
microscopy and immunohistochemical staining which demonstrated that
GMSCs can home to periodontal injury sites and promote tissue
regeneration. At 1-week and 2-weeks post-transplantation,
GFP+ fibroblast-like cells could be identified in the
gingival tissue and periodontal ligament. Furthermore,
GFP+ osteoblasts were identified in the area of newly
formed alveolar bone at 4 weeks post-transplantation (Fig. 4).
Discussion
Gingival tissue is an inherent oral barrier against
different insults, including chemicals and bacteria. The most
notable characteristics of gingival tissue are its fast
reconstitution of tissue and scarless wound healing (15), suggesting that MSCs exist in gingival
tissue. Zhang et al (11)
first isolated cells possessing MSCs properties within the gingival
tissue, these cells displayed a stable phenotype, normal karyotype
and telomerase activity and non-tumorigenic in long-term cultures.
Compared with other sources of MSCs, GMSCs have a clear advantage,
as they are easily obtainable from the discarded tissue in routine
dental procedures. Also, there was no significant difference in the
characteristics of GMSCs derived from healthy gingival tissue and
hyperplastic or inflamed gingival tissue (16,17). In
the authors' previous study, it was demonstrated that systemically
transplanted GMSCs could home to mandibular defects as other MSCs
and promoted bone regeneration involved in novel bone formation.
Therefore, it was assumed that systemically transplanted GMSCs
could home to periodontal damage sites induced by periodontitis and
encourage periodontal tissue regeneration.
To verify the present study's hypothesis, GMSCs were
isolated from gingival tissue and the harvested cells displayed
self-renewal capability and multilineage differentiation potential
in vitro. Furthermore, the results of flow cytometric
analysis demonstrated that GMSCs express MSCs markers CD73, CD90
and CD105, but lack CD45. All characteristics above were consistent
with the criteria of mesenchymal stromal cells suggested by the
International Society for Cellular Therapy (18).
To trace the fate of GMSCs in vivo, the GFP
gene was transduced into GMSCs using lentiviral vectors. The
lentiviral vectors can integrate exogenous GFP genes into GMSCs
chromosomes, therefore achieving persistent expression (19). Most importantly, the integration and
expression of GFP genes in mesenchymal stem cells have no
significant effect on the characteristics of stem cells. At 72 h
following transfection, >90% transfected cells emitted bright
green fluorescence under a fluorescent microscope and expressed GFP
stably with each passage.
A periodontitis model was established in mice by
tying a ligature at the second maxillary molar, then overt bone
loss and gingival inflammation were detected at 4 weeks following
ligation. A total of 12 sites on alveolar bone were susceptible to
bone loss following ligature-induced periodontitis in mice
(20). In this study, the alveolar
bone loss was measured as the sum of distances from the CEJ to the
ABC at 6 sensitive sites of the second maxillary molars. As a
result, alveolar bone heights in group A were increased compared
with group B at 4 weeks post-transplantation. Results of HE and MT
staining demonstrated more newly formed bone and higher alveolar
bone heights in group A at 4 weeks post-transplantation. These
results proved that GMSCs are effective in promoting bone
regeneration. In addition, compared with group B, reduced
inflammatory cell infiltration and more periodontal attachment were
demonstrated in group A at 2 and 4 weeks post-transplantation. This
suggests that GMSCs have an anti-inflammatory effect on
periodontitis, but the specific anti-inflammatory mechanism should
be a key task in future research.
Fluorescent microscopy and anti-GFP
immunohistochemical staining were performed to trace the fate of
GFP-labeled GMSCs in vivo. GFP+ gingival
fibroblasts and periodontal ligament cells were detected at 1 and 2
weeks post-transplantation. In addition, GFP+
osteoblasts can be detected in the newly formed bone area by the
4th-week post-transplantation. The results proved that GMSCs could
home to periodontal defect sites and differentiate into periodontal
tissue cells. Previous studies have demonstrated that the
microenvironment of MSCs can induce the transplanted cells to
differentiate into specific tissues (21–23). At
the same time, transplanted stem cells also produce bioactive
molecules which stimulate the precursor cells to differentiate
(24). The question of whether the
same mechanism occurs in GMSCs and periodontitis remains to be
answered. Periodontal disease is a chronic disease developing with
an active stage and resting stage appearing alternately. The model
established in this study simulates an acute episode of
periodontitis. Future studies should put more effort into
clarifying the therapeutic effect and mechanism of GMSCs on chronic
inflammation.
In conclusion, GMSCs have been identified that
possess characteristics of MSCs and GMSCs could home to the
inflammatory periodontium sites and be employed in novel tissue
formation. GMSCs serve an essential anti-inflammation role,
although the exact mechanism is unclear so far.
Acknowledgements
The authors would like to thank The Key Lab of Oral
Clinical Medicine and The Central Lab of Affiliated Hospital of
Qingdao University for the use of laboratories.
Funding
The present study was supported by grants from the
National Natural Science Foundation of China (grant no. 81500849)
to Dr Quanchen Xu and Shandong Province Key Research Plan (grant
no. 2018GSF118150) to Dr Quanchen Xu.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZW, QX and HS designed the study. WS, RH, XL and JY
performed the experiments. QX analyzed the data and WS wrote the
manuscript. All authors discussed the results and reviewed the
manuscript.
Ethics approval and consent to
participate
Ethical approval for the study was granted from the
Affiliated Hospital of Qingdao University (Qingdao, China) and
informed consent was provided.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kassebaum NJ, Bernabé E, Dahiya M,
Bhandari B, Murray CJ and Marcenes W: Global burden of severe
periodontitis in 1990–2010: A systematic review and
meta-regression. J Dent Res. 93:1045–1053. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hynes K, Menicanin D, Gronthos S and
Bartold PM: Clinical utility of stem cells for periodontal
regeneration. Periodontology. 59:203–227. 2012. View Article : Google Scholar
|
|
3
|
Salvi GE, Mischler DC, Schmidlin K,
Matuliene G, Pjetursson BE, Brägger U and Lang NP: Risk factors
associated with the longevity of multi-rooted teeth. Long-term
outcomes after active and supportive periodontal therapy. J Clin
Periodontol. 41:701–707. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Silvério KG, Benatti BB, Casati MZ, Sallum
EA and Nociti FH Jr: Stem cells: Potential therapeutics for
periodontal regeneration. Stem Cell Rev. 4:13–19. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Luria EA, Panasyuk AF and Friedenstein AY:
Fibroblast colony formation from monolayer cultures of blood cells.
Transfusion. 11:345–349. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Du J, Shan Z, Ma P, Wang S and Fan Z:
Allogeneic bone marrow mesenchymal stem cell transplantation for
periodontal regeneration. J Dent Res. 93:183–188. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Seo BM, Miura M, Gronthos S, Bartold PM,
Batouli S, Brahim J, Young M, Robey PG, Wang CY and Shi S:
Investigation of multipotent postnatal stem cells from human
periodontal ligament. Lancet. 364:149–155. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Huang TJ, Sonoyama W, Chen J and Sang HP:
In vitro characterization of human dental pulp cells: Various
isolation methods and culturing environments. Cell Tissue Res.
324:225–236. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Morsczeck C, Götz W, Schierholz J,
Zeilhofer F, Kühn U, Möhl C, Sippel C and Hoffmann KH: Isolation of
precursor cells (PCs) from human dental follicle of wisdom teeth.
Matrix Biol. 24:155–165. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tomar GB, Srivastava RK, Gupta N,
Barhanpurkar AP, Pote ST, Jhaveri HM, Mishra GC and Wani MR: Human
gingiva-derived mesenchymal stem cells are superior to bone
marrow-derived mesenchymal stem cells for cell therapy in
regenerative medicine. Biochem Biophys Res Commun. 393:377–383.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang Q, Shi S, Liu Y, Uyanne J, Shi Y,
Shi S and Le AD: Mesenchymal stem cells derived from human gingiva
are capable of immunomodulatory functions and ameliorate
inflammation-related tissue destruction in experimental colitis. J
Immunol. 183:7787–7798. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Su WR, Zhang QZ, Shi SH, Nguyen AL and Le
AD: Human gingiva-derived mesenchymal stromal cells attenuate
contact hypersensitivity via prostaglandin E2-dependent mechanisms.
Stem Cells. 29:1849–1860. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wada N, Wang B, Lin NH, Laslett AL,
Gronthos S and Bartold PM: Induced pluripotent stem cell lines
derived from human gingival fibroblasts and periodontal ligament
fibroblasts. J Periodontal Res. 46:438–447. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Xu QC, Wang ZG, Ji QX, Yu XB, Xu XY, Yuan
CQ, Deng J and Yang PS: Systemically transplanted human
gingiva-derived mesenchymal stem cells contributing to bone tissue
regeneration. Int J Clin Exp Pathol. 7:4922–4929. 2014.PubMed/NCBI
|
|
15
|
Häkkinen L, Uitto VJ and Larjava H: Cell
biology of gingival wound healing. Periodontology. 24:127–152.
2000. View Article : Google Scholar
|
|
16
|
Ge S, Mrozik KM, Menicanin D, Gronthos S
and Bartold PM: Isolation and characterization of mesenchymal stem
cell-like cells from healthy and inflamed gingival tissue:
Potential use for clinical therapy. Regen Med. 7:819–832. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tang L, Li N, Xie H and Jin Y:
Characterization of mesenchymal stem cells from human normal and
hyperplastic gingiva. J Cell Physiol. 226:832–842. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Dominici M, Le Blanc K, Mueller I,
Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A,
Prockop Dj and Horwitz E: Minimal criteria for defining multipotent
mesenchymal stromal cells. The International Society for Cellular
Therapy position statement. Cytotherapy. 8:315–317. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ye Z, Yu X and Cheng L: Lentiviral gene
transduction of mouse and human stem cells. Methods Mol Biol.
430:243–253. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Abe T and Hajishengallis G: Optimization
of the ligature-induced periodontitis model in mice. J Immunol
Methods. 394:49–54. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Liechty KW, Mackenzie TC, Shaaban AF, Radu
A, Moseley AM, Deans R, Marshak DR and Flake AW: Human mesenchymal
stem cells engraft and demonstrate site-specific differentiation
after in utero transplantation in sheep. Nat Med. 6:1282–1286.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Guo X, Bai Y, Zhang L, Zhang B, Zagidullin
N, Carvalho K, Du Z and Cai B: Cardiomyocyte differentiation of
mesenchymal stem cells from bone marrow: New regulators and its
implications. Stem Cell Res Ther. 9:442018. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aggarwal S and Pittenger MF: Human
mesenchymal stem cells modulate allogeneic immune cell responses.
Blood. 105:1815–1822. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Seo BM, Miura M, Sonoyama W, Coppe C,
Stanyon R and Shi S: Recovery of stem cells from cryopreserved
periodontal ligament. J Dent Res. 84:907–912. 2005. View Article : Google Scholar : PubMed/NCBI
|