Introduction
Systemic lupus erythematosus (SLE) is a kind of
diffuse connective tissue disease (1), usually involving the whole body. The
course and number of affected organs of SLE are negatively
correlated with its prognosis (2).
The morbidity and mortality rates of lupus nephritis (LN) account
for approximately 60% in SLE (3,4). The
pathogenesis of LN remains unclear currently, which, according to
the literature, may be caused by interaction of factors such as
environment, heredity, autoimmunity and estrogen (5,6). LN is
characterized by a high prevalence rate and long treatment cycle,
and it leads to death in severe cases (7). Therefore, the diagnosis of LN is of
great significance in providing a basis for clinical treatment and
prognosis.
Interleukin-34 (IL-34) is an inflammatory factor,
another major ligand of colony-stimulating factor-1 receptor
(CSF-1R) following CSF-1, which can directly bind to CSF-1R to
exert similar and independent biological effects of CSF-1 (8). IL-34, mainly through binding to CSF-R,
regulates the activation, survival, proliferation, chemotaxis and
secretion of corresponding cytokines in monocytes or macrophages
(9). Inflammatory injury mediated by
macrophages plays an important role in the pathogenesis of LN
(10). IL-17 is an inflammatory
factor with important effects in autoimmune diseases,
pro-inflammatory and organ transplant rejection reactions (11). IL-17 can bind to the corresponding
receptors to result in the infiltration of inflammatory cells and
tissue damage (12). According to
the literature, IL-17 can promote the progression of SLE, which is
highly expressed in serum of SLE patients and animal model of lupus
(13).
This study investigated the expression levels of
serum IL-17 and IL-34 and analyze the influencing factors for
prognosis in LN patients. Results showed IL-17 and IL-34 are
independent risk factors for poor prognosis of LN. The findings
provide a theoretical basis for the diagnosis, treatment and
prognosis of LN in the future.
Materials and methods
General data
A total of 45 patients treated and diagnosed with LN
via renal biopsy in Yanan University Affiliated Hospital (Yanan,
China) from October 2010 to October 2012 were selected as LN group,
including 8 males and 37 females with an average age of 42.08±16.52
years. Another 50 healthy subjects, including 10 males and 40
females with an average age of 41.28±15.85 years, undergoing
physical examination during the same period were selected as the
control group. There were no significant differences in age and sex
between the two groups (P>0.05), while leukocyte, hemoglobin,
blood albumin, blood platelet, blood uric acid, serum creatinine,
systolic pressure, diastolic pressure, urinary protein and
triglyceride had statistically significant differences (P<0.05).
None of the patients had undergone treatment with hormones and
immunosuppressors in the prior 3 months. Pregnant or breastfeeding
patients, or patients with autoimmune diseases, severe infection,
other kidney-related diseases or rheumatoid arthritis were
excluded.
The study was approved by the Ethics Committee of
Yanan University Affiliated Hospital (Yanan, China). All the
patients, or their families, signed the informed consent, and the
patients had complete clinical data. General patient information is
shown in Table I.
 | Table I.General data. |
Table I.
General data.
| Factor | LN group (n=45) | Control group
(n=50) | t/χ2
value | P-value |
|---|
| Age (years) | 42.08±16.52 | 41.28±15.85 | 0.241 | 0.810 |
| Sex [n (%)] |
|
| 0.800 | 0.076 |
| Male | 8
(17.78) | 10 (20.00) |
|
|
|
Female | 37 (82.22) | 40 (80.00) |
|
|
| Leukocyte
(×109) |
6.34±0.45 |
5.98±0.84 | 2.562 | 0.012 |
| Hemoglobin (g/l) |
110.86±15.25 |
137.94±14.28 | 8.937 | <0.001 |
| Blood albumin
(g/l) |
30.85±7.46 |
46.52±2.48 | 14.020 | <0.001 |
| Blood platelet
(×109/l) |
232.94±52.05 |
257.76±53.49 | 0.287 | 0.025 |
| Blood uric acid
(mmol/l) |
374.26±82.45 |
300.15±52.34 | 5.284 | <0.001 |
| Serum creatinine
(µmol/l) |
64.15±20.54 |
53.14±7.53 | 3.537 | <0.001 |
| Systolic pressure
(mmHg) | 128.82±9.46 | 123.92±8.45 | 2.667 | 0.009 |
| Diastolic pressure
(mmHg) |
81.46±8.24 |
77.46±6.82 | 2.587 | 0.011 |
| Urinary protein
(g) |
2.79±2.14 |
0.12±0.02 | 8.827 | <0.001 |
| Triglyceride
(mmol/l) |
2.43±1.25 |
1.43±0.72 | 4.837 | <0.001 |
Reagents and equipment
Human serum IL-17 and IL-34 enzyme-linked
immunosorbent assay (ELISA) kits were purchased from Shanghai
Lengton Biotechnology Co., Ltd., and Anthos PHOMO full-automatic
microplate reader was purchased from Shanghai Zhongsheng Life
Science Development Co., Ltd. (Shanghai, China).
Detection of IL-17 and IL-34
After 3 ml fasting venous blood was drawn from the
patients in the morning and centrifuged at 2,600 × g at 4°C for 10
min, 1 ml serum was taken using a pipette for standby application.
Levels of serum IL-17 and IL-34 were detected via ELISA. The kit
and sample to be detected were taken from the refrigerator 30 min
in advance to be balanced to the room temperature, and sample,
standard and blank wells were set up. Enzyme-labeled reagents and
samples were not added into blank well, 100 µl samples to be
detected or standard substances were added into the remaining wells
and mixed evenly. Then the ELISA plate was covered with a membrane,
followed by incubation at 37°C for 2 h. After the liquid in each
well was discarded and spun dry, each well was added with 100 µl
working solution A and covered with the membrane, followed by
incubation at 37°C for 1 h. After the liquid in each well was
discarded and spun dry, the plate was washed 3 times, and each well
was added with 100 µl working solution B and covered with the
membrane, followed by incubation at 37°C for 1 h. After the liquid
in each well was discarded and spun dry, the plate was washed again
3 times, each well was added with 90 µl substrate solution and
covered with the membrane, followed by color development in the
dark at room temperature for 20 min. Stop solution (50 µl) was
added to each well, and the optical density (OD) of each well was
detected at a wavelength of 450 nm using the microplate reader.
Finally, the IL-34 and IL-17 concentrations were calculated.
Statistical analysis
Statistical Product and Service Solutions (SPSS)
17.0 software (Shanghai Cabit Information Technology Co., Ltd.) was
used for analysis. Chi-square test was used for enumeration data,
and t-test was used for measurement data. Univariate survival
analysis was performed using the Kaplan-Meier method and log-rank
test, and univariate and multivariate analyses were performed using
the Cox proportional hazards model. P<0.05 was considered to
indicate a statistically significant difference.
Results
Comparison of serum IL-17 and IL-34
levels between the two groups
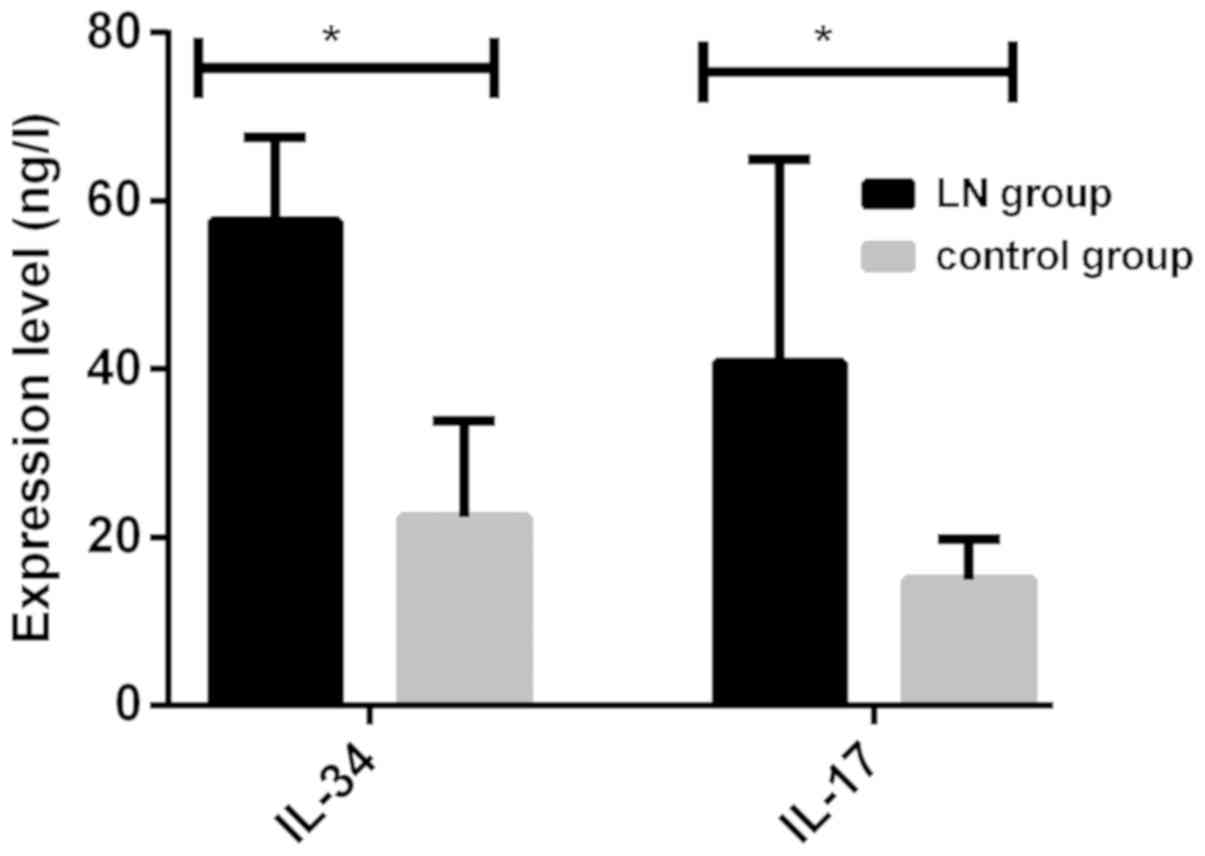
Levels of serum IL-17 and IL-34 in patients in LN
group were significantly higher than those in control group, and
there were statistically significant differences (P<0.001)
(Fig. 1 and Table II).
| Table II.Comparison of serum IL-34 and IL-17
levels between the two groups. |
Table II.
Comparison of serum IL-34 and IL-17
levels between the two groups.
| Index | LN group | Control group | t value | P-value |
|---|
| No. | 45 | 50 |
|
|
| IL-34 (ng/l) | 57.61±16.24 |
22.34±11.53 | 12.300 | <0.001 |
| IL-17 (ng/l) | 40.82±24.15 | 14.94±4.86 |
7.417 | <0.001 |
Correlation analysis of IL-17 and
IL-34 with urinary protein in LN
Serum IL-17 and IL-34 in LN patients were positively
correlated with urinary protein (r=0.436 and 0.714, P<0.05)
(Table III).
| Table III.Correlation analysis of IL-34 and
IL-17 with urinary protein in LN. |
Table III.
Correlation analysis of IL-34 and
IL-17 with urinary protein in LN.
| Item | IL-34 | IL-17 | P-value |
|---|
| Urinary protein | 0.714 | 0.436 | P<0.05 |
Analysis of influencing factors for
survival time of LN patients
The 3- and 5-year overall survival rates of LN
patients were 86.42 and 74.67%, respectively. Influencing factors
for survival time of 45 LN patients were analyzed via univariate
analysis, and results manifested that adverse factors affecting the
prognosis of LN patients included age, hemoglobin, platelet, blood
uric acid, urinary protein, IL-17 and IL-34, displaying
statistically significant differences (P<0.05). According to
results of multivariate Cox regression analysis, age, hemoglobin,
blood uric acid, urinary protein, IL-17 and IL-34 were independent
risk factors for the poor prognosis of LN, and differences were
statistically significant (P<0.05) (Tables IV and V).
| Table IV.Univariate analysis results of
prognosis of LN patients. |
Table IV.
Univariate analysis results of
prognosis of LN patients.
| Factors | P-value | Hazard ratio
(HR) | 95% confidence
interval (95% CI) |
|---|
| Sex (male vs.
female) | 0.306 | 1.052 | 0.357–1.138 |
| Age (<40 years vs.
≥40 years) | 0.008 | 0.035 | 0.018–0.052 |
| Leukocyte
(<6×109 vs. ≥6×109) | 0.526 | 1.012 | 0.004–1.756 |
| Hemoglobin (<123
g/l vs. ≥123 g/l) | 0.004 | 0.047 | 0.032–0.069 |
| Blood albumin
(<38 g/l vs. ≥38 g/l) | 0.852 | 2.121 | 0.104–4.265 |
| Blood platelet
(<244×109/l vs. ≥244×109/l) | 0.035 | 0.462 | 0.254–0.672 |
| Blood uric acid
(<337 mmol/l vs. ≥337 mmol/l) | <0.001 | 3.026 | 1.389–4.258 |
| Serum creatinine
(<58 μmol/l vs. ≥58 µmol/l) | 0.418 | 0.627 | 0.237–2.467 |
| Systolic pressure
(<126 mmHg vs. ≥126 mmHg) | 0.691 | 0.508 | 0.118–0.964 |
| Diastolic pressure
(<79 mmHg vs. ≥79 mmHg) | 0.483 | 0.620 | 0.004–2.586 |
| Urinary protein
(<1 g vs. ≥1 g) | <0.001 | 2.895 | 0.623–4.953 |
| Triglyceride (<2
mmol/l vs. ≥2 mmol/l) | 1.462 | 0.743 | 0.372–2.561 |
| IL-34 (<55.37
ng/l vs. ≥55.37 ng/l) | <0.001 | 2.865 | 1.423–4.824 |
| IL-17 (<42.62
ng/l vs. ≥42.62 ng/l) | <0.001 | 2.541 | 1.147–3.749 |
| Table V.Multivariate analysis results of
prognosis of LN patients. |
Table V.
Multivariate analysis results of
prognosis of LN patients.
| Factors | P-value | HR | 95% CI |
|---|
| Age (<40 years
vs. ≥40 years) | 0.036 | 1.624 | 1.306–3.251 |
| Hemoglobin (<123
g/l vs. ≥123 g/l) | 0.021 | 0.429 | 0.284–0.672 |
| Blood platelet
(<244×109/l vs. ≥244×109/l) | 0.082 | 1.327 | 0.876–2.728 |
| Blood uric acid
(<337 mmol/l vs. ≥337 mmol/l) | 0.007 | 2.681 | 1.512–4.903 |
| Urinary protein
(<1 g vs. ≥1 g) | 0.010 | 2.546 | 2.014–4.865 |
| IL-34 (<55.37
ng/l vs. ≥55.37 ng/l) | 0.032 | 1.625 | 1.004–3.126 |
| IL-17 (<42.62
ng/l vs. ≥42.62 ng/l) | 0.028 | 1.451 | 0.438–3.647 |
Discussion
Lupus nephritis is a chronic disease that often
relapses and remits alternately. Renal injury is aggravated
continuously in the acute phase, thus accelerating the progression
of end-stage renal disease of LN (14). The prevalence rate of end-stage renal
disease is as low as 26%, but the proportion of active lesions and
relapse in LN is up to 27–66%, leading to the increased mortality
rate of LN (15). Currently,
commonly used diagnostic methods for LN include decreased
glomerular filtration rate, proteinuria and renal biopsy. However,
renal biopsy has not been universally employed because it affects
treatment and prognosis (16).
Therefore, the early diagnosis, treatment and monitoring of
progression of LN have become research hotspots, providing clues
for the prognosis (17).
Results of this study revealed that the levels of
serum IL-17 and IL-34 in patients in LN group were obviously higher
than those in control group, showing statistically significant
differences (P<0.001). Research results of Bethunaickan et
al (18) and Susianti et
al (19) are consistent with
those in this study. Bethunaickan et al (18) showed that IL-34 messenger ribonucleic
acid (mRNA) is highly expressed in the kidney of lupus mice and it
is significant in the pathogenesis of LN. A possible reason is that
the glomerular and renal interstitial damage is aggravated through
damage to inflammatory factors. Susianti et al (19) found that the IL-17 level is
significantly increased in LN. A possible reason is that IL-17 can
promote other immune inflammatory mediators and epithelial cells,
and make inflammatory cells accumulate and damage renal tissues,
thereby leading to proteinuria. According to results of Pearson's
correlation analysis, the levels of serum IL-34 and IL-17 in LN
patients had positive correlations with urinary protein (r=0.714
and 0.436, P<0.05). There are few studies on the correlation
between IL-17 and urinary protein, so the results in this study are
not confirmed. Moreover, Menke et al (20) found that the IL-34 content in urine
of LN mice is positively correlated with secretion of urinary
albumin (r=0.915, P<0.01), which is basically consistent with
the results in this study. Therefore, IL-34 can display the
activity degree of LN.
The 3- and 5-year overall survival rates of LN
patients were 86.42 and 74.67%, respectively. Influencing factors
for survival time of 45 LN patients were analyzed via univariate
analysis, and results manifested that adverse factors affecting the
prognosis of LN patients included age, hemoglobin, platelet, blood
uric acid, urinary protein, IL-17 and IL-34, displaying
statistically significant differences (P<0.05). According to
results of multivariate Cox regression analysis, age, hemoglobin,
blood uric acid, urinary protein, IL-17 and IL-34 were independent
risk factors for poor prognosis of LN, and differences were
statistically significant (P<0.05). Research results of Shen
et al (21) revealed that
there is a certain correlation between pathological types and
clinical manifestations and prognosis of LN patients. Daniel et
al (22) thought that
influencing factors for prognosis of LN patients include age,
decline in complement 3, increase in urinary protein, decrease in
hemoglobin and blood platelet, and increase in uric acid level,
which are basically consistent with the results in this study.
There will be changes in structure and function of both kidneys
with age. Urinary protein can reflect glomerular lesion and damage,
and increase the expression of inflammatory factors, thus leading
to renal damage. At the same time, the increase in urinary protein
results in a lower level of hemoglobin (23). In LN, the renal tubule and
interstitium can be damaged, leading to decline in erythropoietin,
and IL-1 can be increased, leading to inhibited production of
erythropoietin (24). High-level
uric acid can aggravate renal hypertension, lead to glomerular
autoregulation dysfunction and promote production of nitric oxide,
thereby causing excretion disorder (25). In addition, Wu et al (26) and Zhao et al (12) studied and found that the levels of
IL-17 and IL-34 are positively correlated with urinary protein, and
these levels can reflect the severity of LN, indicating that the
disease condition and clinical manifestations of LN patients is
gradually aggravated with the increase in levels of serum IL-17 and
IL-34.
In conclusion, IL-17 and IL-34 are highly expressed
in serum of LN patients. Results of univariate and multivariate Cox
regression analyses reveal that age, hemoglobin, blood uric acid,
urinary protein, IL-17 and IL-34 are independent risk factors for
poor prognosis of LN. Studies on IL-17 and IL-34 provide broader
ideas for clinical diagnosis, treatment and prognosis prediction of
LN, displaying a bright prospect.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YC and XY drafted the manuscript. YC, XY and XZ were
mainly devoted to collecting and interpreting the data. XZ and ZA
detected IL-17 and IL-34. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Yanan University Affiliated Hospital (Yanan, China). Signed
informed consents were obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rönnblom L and Pascual V: The innate
immune system in SLE: Type I interferons and dendritic cells.
Lupus. 17:394–399. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mackay M, Stanevsky A, Wang T, Aranow C,
Li M, Koenig S, Ravetch JV and Diamond B: Selective dysregulation
of the FcgammaIIB receptor on memory B cells in SLE. J Exp Med.
203:2157–2164. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Faurschou M, Starklint H, Halberg P and
Jacobsen S: Prognostic factors in lupus nephritis: Diagnostic and
therapeutic delay increases the risk of terminal renal failure. J
Rheumatol. 33:1563–1569. 2006.PubMed/NCBI
|
|
4
|
Bajaj S, Albert L, Gladman DD, Urowitz MB,
Hallett DC and Ritchie S: Serial renal biopsy in systemic lupus
erythematosus. J Rheumatol. 27:2822–2826. 2000.PubMed/NCBI
|
|
5
|
Ramos-Casals M, Nardi N, Lagrutta M,
Brito-Zerón P, Bové A, Delgado G, Cervera R, Ingelmo M and Font J:
Vasculitis in systemic lupus erythematosus: Prevalence and clinical
characteristics in 670 patients. Medicine (Baltimore). 85:95–104.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Heimovski FE, Simioni JA and Skare TL:
Systemic lupus erythematosus and Raynaud's phenomenon. An Bras
Dermatol. 90:837–840. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
D'Cruz DP, Mellor-Pita S, Joven B, Sanna
G, Allanson J, Taylor J, Khamashta MA and Hughes GR: Transverse
myelitis as the first manifestation of systemic lupus erythematosus
or lupus-like disease: Good functional outcome and relevance of
antiphospholipid antibodies. J Rheumatol. 31:280–285.
2004.PubMed/NCBI
|
|
8
|
Lin H, Lee E, Hestir K, Leo C, Huang M,
Bosch E, Halenbeck R, Wu G, Zhou A, Behrens D, et al: Discovery of
a cytokine and its receptor by functional screening of the
extracellular proteome. Science. 320:807–811. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Foucher ED, Blanchard S, Preisser L, Garo
E, Ifrah N, Guardiola P, Delneste Y and Jeannin P: IL-34 induces
the differentiation of human monocytes into immunosuppressive
macrophages. antagonistic effects of GM-CSF and IFNγ. PLoS One.
8:e560452013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chalmers SA, Chitu V, Ramanujam M and
Putterman C: Therapeutic targeting of macrophages in lupus
nephritis. Discov Med. 20:43–49. 2015.PubMed/NCBI
|
|
11
|
Roussel L, Houle F, Chan C, Yao Y, Bérubé
J, Olivenstein R, Martin JG, Huot J, Hamid Q, Ferri L, et al: IL-17
promotes p38 MAPK-dependent endothelial activation enhancing
neutrophil recruitment to sites of inflammation. J Immunol.
184:4531–4537. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhao XF, Pan HF, Yuan H, Zhang WH, Li XP,
Wang GH, Wu GC, Su H, Pan FM, Li WX, et al: Increased serum
interleukin 17 in patients with systemic lupus erythematosus. Mol
Biol Rep. 37:81–85. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hsu HC, Yang P, Wang J, Wu Q, Myers R,
Chen J, Yi J, Guentert T, Tousson A, Stanus AL, et al: Interleukin
17-producing T helper cells and interleukin 17 orchestrate
autoreactive germinal center development in autoimmune BXD2 mice.
Nat Immunol. 9:166–175. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sprangers B, Monahan M and Appel GB:
Diagnosis and treatment of lupus nephritis flares - an update. Nat
Rev Nephrol. 8:709–717. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mok CC, Ying KY, Tang S, Leung CY, Lee KW,
Ng WL, Wong RW and Lau CS: Predictors and outcome of renal flares
after successful cyclophosphamide treatment for diffuse
proliferative lupus glomerulonephritis. Arthritis Rheum.
50:2559–2568. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Saxena R, Mahajan T and Mohan C: Lupus
nephritis: Current update. Arthritis Res Ther. 13:2402011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Balow JE, Waldman M and Austin HA: Lupus
nephritis. Therapy in Nephrology & Hypertension. Saunders;
Philadelphia, PA: pp. 157–171. 2008, View Article : Google Scholar
|
|
18
|
Bethunaickan R, Berthier CC, Zhang W,
Kretzler M and Davidson A: Comparative transcriptional profiling of
3 murine models of SLE nephritis reveals both unique and shared
regulatory networks. PLoS One. 8:e774892013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Susianti H, Iriane VM, Dharmanata S,
Handono K, Widijanti A, Gunawan A and Kalim H: Analysis of urinary
TGF-β1, MCP-1, NGAL, and IL-17 as biomarkers for lupus nephritis.
Pathophysiology. 22:65–71. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Menke J, Rabacal WA, Byrne KT, Iwata Y,
Schwartz MM, Stanley ER, Schwarting A and Kelley VR: Circulating
CSF-1 promotes monocyte and macrophage phenotypes that enhance
lupus nephritis. J Am Soc Nephrol. 20:2581–2592. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shen K, Yu Y, Tang Z, Liu Z and Li L: The
prognosis of biopsy-proven lupus nephritis in Chinese patients:
Long term follow-up of 86 cases. Chin Med J (Engl). 110:502–507.
1997.PubMed/NCBI
|
|
22
|
Daniel L, Sichez H, Giorgi R, Dussol B,
Figarella-Branger D, Pellissier JF and Berland Y: Tubular lesions
and tubular cell adhesion molecules for the prognosis of lupus
nephritis. Kidney Int. 60:2215–2221. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Nee R, Jindal RM, Little D, Ramsey-Goldman
R, Agodoa L, Hurst FP and Abbott KC: Racial differences and income
disparities are associated with poor outcomes in kidney transplant
recipients with lupus nephritis. Transplantation. 95:1471–1478.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Yap DY, Tang CS, Ma MK, Lam MF and Chan
TM: Survival analysis and causes of mortality in patients with
lupus nephritis. Nephrol Dial Transplant. 27:3248–3254. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sánchez-Lozada LG, Tapia E, López-Molina
R, Nepomuceno T, Soto V, Avila-Casado C, Nakagawa T, Johnson RJ,
Herrera-Acosta J and Franco M: Effects of acute and chronic
L-arginine treatment in experimental hyperuricemia. Am J Physiol
Renal Physiol. 292:F1238–F1244. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wu T, Fu Y, Brekken D, Yan M, Zhou XJ,
Vanarsa K, Deljavan N, Ahn C, Putterman C and Mohan C: Urine
proteome scans uncover total urinary protease, PGDS, SAP and SOD as
potential markers of lupus nephritis. J Immunol. 184:2183–2193.
2010. View Article : Google Scholar : PubMed/NCBI
|