Introduction
Spontaneous bacterial peritonitis (SBP) is one of
the common complications in liver cirrhosis (LC) patients with
ascites (1). Several mechanisms
contribute to the occurrence of SBP, including translocation of gut
bacteria and their products, reduction of intestinal motility
provoking bacterial overgrowth, alteration of the gut's barrier
function and local immune responses (2). The occurrence of SBP in hospitalized
ascites patients range from 10–30% (3). Furthermore, SBP secondary to LC
frequently aggravates liver damage and induces serious
complications, including hepatorenal syndrome and hepatic
encephalopathy (4). Therefore, early
diagnosis and effective treatment are vital to improve the clinical
outcome.
The clinical manifestations of SBP range from
asymptomatic to typical peritoneal infection and even to severe
hepatic encephalopathy or hepatorenal syndrome, easily leading to a
missed diagnosis and misdiagnosis. Diagnostic puncture frequently
has an important role in the diagnosis of SBP (5). In a previous study, the diagnosis was
based on bacterial positive cultures in ascitic fluid and/or the
testing of an elevated absolute fluid polymorphonuclear neutrophil
(PMN) count in the ascites (>250/mm3) without any
obvious abdominal intra-operatively detected source of infection
(6).
In recent years, with the prevalence of
multidrug-resistant bacteria and the re-distribution of the
bacterial spectrum, SBP has become a serious clinical problem in
several countries. In addition, a variation in the epidemiology of
bacteria, which may be the reason for the increased prevalence of
SBP, was reported in patients with long-term norfloxacin
prophylaxis, appearing in the quinolone-resistant bacterial
culture, as well as Gram-positive bacteria (GPB) (7). Numerous studies have focused on the
therapeutic effects of various antibiotics and suggested that their
efficacy is associated with SBP infection strains. A recent
analysis determined that the rate of third-generation cephalosporin
resistance ranged from 15.6–44.0% in SBP cases (8). In conclusion, the selection of
effective antibiotics according to the type of pathogen it is
crucial for SBP patients.
The present study aimed to retrospectively examine
changes in the bacterial spectrum, laboratory characteristics and
drug resistance in LC patients with SBP. The results may contribute
to the understanding of the etiologic features of SBP and may
provide guidance for the selection of medication for empirical
treatment.
Materials and methods
Subjects
A total of 3, 189 patients with ascites, including
912 LC patients, of which 247 had SBP, who had been admitted to
Beijing Di Tan Hospital, Capital Medical University (Beijing,
China) between January 2011 and December 2016 were retrospectively
enrolled in the present study. Patients with ascites were assigned
to Group A (admission, 2011–2013) and Group B (admission,
2014–2016). Patients with LC were assigned to Group A1 (admission,
2011–2013) and Group B1 (admission, 2014–2016). Of these, the
patients with SBP identified by positive culture were assigned to
Group 1 (admission, 2011–2013) and Group 2 (admission,
2014–2016).
All of the patient data were retrospectively
retrieved from their electronic health records. The present study
was approved by the Ethics Committee of the Beijing Di Tan Hospital
(Beijing, China) and was in accordance with the 1975 Declaration of
Helsinki.
According to the guidelines published by the
American Association for the Study of Liver Diseases (9) and the European Association for the
Study of the Liver (10), the
diagnostic standard for SBP was a positive ascitic fluid culture
and/or a polymorphonuclear leukocyte count of the ascitic fluid of
≥250 cells/mm3.
Laboratory techniques
The ascitic fluid (10 ml) was collected and
inoculated into aerobic and anaerobic blood bottles (BD
Biosciences) and cultured at an automated culture system (BACTEC
9240 and FX200; BD Biosciences) at 35°C for up to 5 days prior to
being reported as negative. After a positive signal was obtained on
the instrument, the cells were smeared and inoculated on a blood
agar, and cultivated at 35°C. These cultivated bacteria were
identified with the BD Phoenix™ automated identification and
susceptibility testing system (BD Biosciences).
Statistical analysis
All data were analyzed using SPSS 19.0 software (IBM
Corp.). The patients' features were assessed using the median
(interquartile range) for continuous variables and n (%) for
categorical variables. The Mann-Whitney U-test and chi-square test
were used for continuous and categorical variables, respectively. A
two-sided P<0.05 was considered to indicate statistical
significance.
Results
Patient characteristics at
baseline
Among the 912 patients, SBP was detected in 247
(27.1%), while the remaining 665 (72.9%) were without SBP. The mean
age of the 912 patients (681 males and 231 females) was 56.3±11.9
years. The most general chronic underlying diseases included
diabetes in 207 cases (22.7%), high blood pressure in 190 cases
(20.8%), coronary heart disease in 15 cases (1.6%) and alcoholic
hepatitis, which was not viral hepatitis, in 260 cases (28.5%). The
most general cause of LC was viral hepatitis, which was identified
in 717 patients (78.6%), including hepatitis B in 139 patients
(73.3%), hepatitis C in 17 (9.4%) and hepatitis B + C in 3 patients
(1.7%). In addition, among the SBP patients, primary biliary
hepatitis was identified in 6 patients (3.3%), autoimmune hepatitis
in 6 patients (3.3%) and other types of hepatitis in 9 patients
(5.0%). On the other hand, among the patients without SBP,
hepatitis B was present in 410 patients (68.9%), hepatitis C in 49
patients (9.10%) and Hepatitis B + C in 9 patients (1.7%).
Furthermore, among the patients without SBP, primary biliary
hepatitis was present in 19 patients (3.5%), autoimmune hepatitis
in 16 patients (3.0%) and other types of hepatitis in 34 patients
(6.3%). The ratios were similar between the groups with SBP and
without SBP (Table I).
 | Table I.Baseline characteristics of the
enrolled patients. |
Table I.
Baseline characteristics of the
enrolled patients.
| Item | Total (n=912) | SBP+ (n=247) | SBP- (n=665) |
|---|
| Age (years) | 56.3±11.9 | 55.5±11.4 | 56.6±12.1 |
| Male gender | 681 (74.7) | 193 (78.1) | 488 (73.4) |
| Diabetes | 207 (22.7) | 52 (21.1) | 155 (23.3) |
| High blood
pressure | 190 (20.8) | 51 (20.6) | 139 (20.9) |
| Coronary heart
disease | 15 (1.6) | 5 (2.0) | 10 (1.5) |
| Cause |
|
|
|
| Alcoholic
hepatitis | 260 (28.5) | 66 (26.7) | 194 (29.2) |
| Hepatitis B
virus | 549 (60.20) | 139 (56.3) | 410 (61.7) |
| Hepatitis C
virus | 66 (7.24) | 17 (6.9) | 49 (7.4) |
| Hepatitis B+C
virus | 12 (1.32) | 3 (1.2) | 9 (1.4) |
| Primary biliary
hepatitis | 25 (2.74) | 6 (2.4) | 19 (2.9) |
| Autoimmune
hepatitis | 22 (2.41) | 6 (2.4) | 16 (2.4) |
| Other hepatitis | 43 (4.71) | 9 (3.6) | 34 (5.1) |
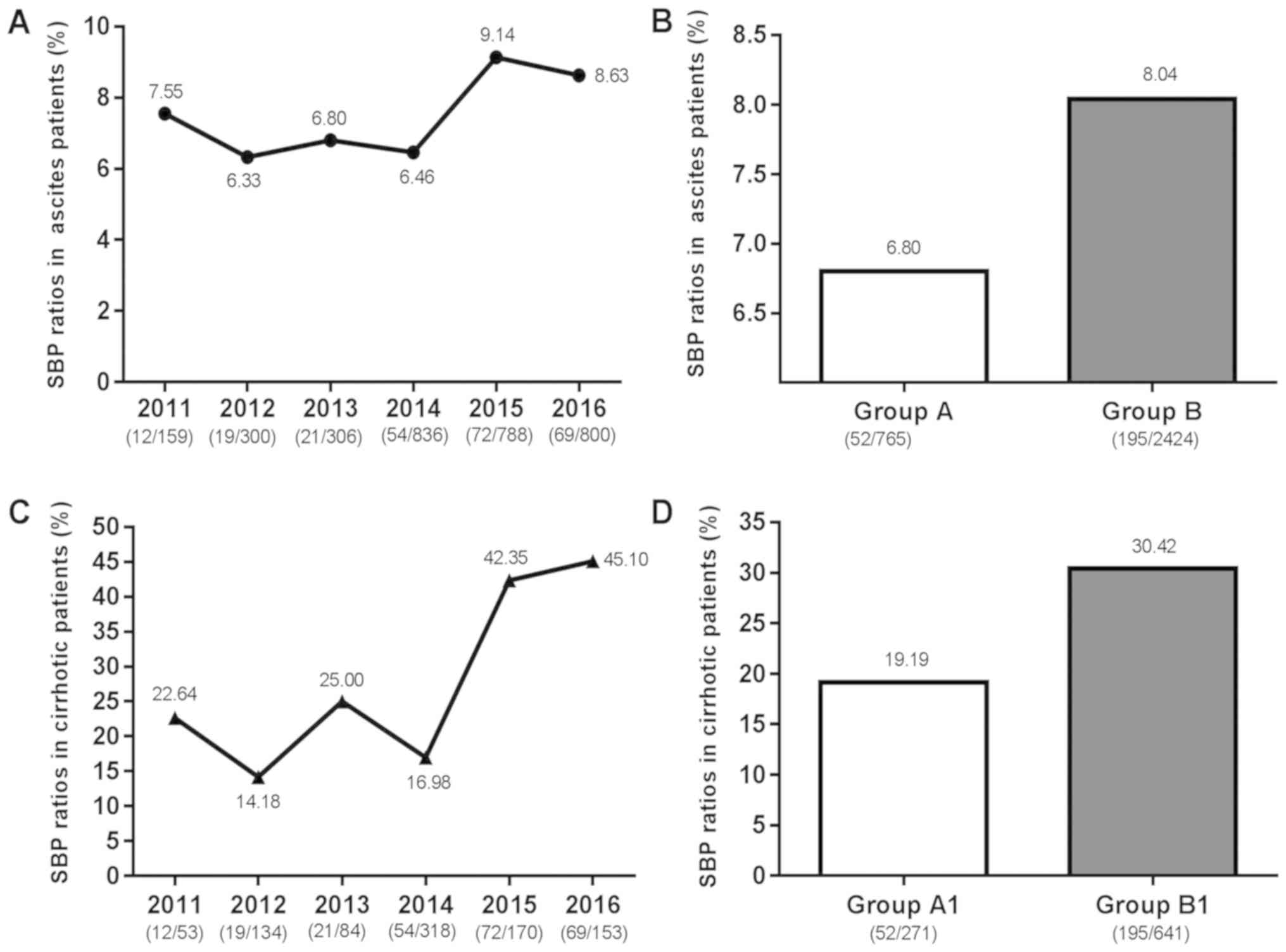
SBP ratios in ascites patients and
cirrhotic patients
As presented in Fig.
1, the SBP ratios in patients with ascites and cirrhotic
increased between 2011 and 2016, with a rising trend observed
between 2014 and 2015. Since 2014, as the popularity of the
hospital increased, the number of patients substantially increased.
Hence, the 3, 189 patients with ascites were divided into two
observation groups: Group A, containing 52 SBP patients from the
765 patients with ascites admitted between 2011 and 2013, and Group
B, containing 195 SBP patients from the 2, 424 patients with
ascites admitted between 2014 and 2016. The patients in Group A and
Group B did not distinctly differ regarding their epidemiological
and clinical features. However, the laboratory results of the
bacterial culture between the two groups were significantly
different, i.e., they were distinctly lower in Group A than in
Group B (P=0.009; Table II). The
912 LC patients were divided into two observation groups: Group A1,
containing 52 SBP patients from the 271 patients with cirrhosis
admitted between 2011 and 2013, and Group B1, containing 195 SBP
patients from the 641 patients with cirrhosis admitted between 2014
and 2016. The results demonstrated that the ratio of SBP in Group B
and Group B1 were higher than those in Group A and Group A1,
respectively.
| Table II.Laboratory results of patients with
spontaneous bacterial peritonitis in plasma and ascitic fluid in
Group 1 (n=52, 21.1%) and Group 2 (n=195, 78.9%). |
Table II.
Laboratory results of patients with
spontaneous bacterial peritonitis in plasma and ascitic fluid in
Group 1 (n=52, 21.1%) and Group 2 (n=195, 78.9%).
| Parameter | Group 1 | Group 2 | Reference range | P-value |
|---|
| Male gender | 42 | 152 | – | 0.939 |
| Age (years) | 55.00 (49.00,
62.75) | 56.00 (47.00,
63.00) | – | 0.681 |
| WBC
(109/l) | 7.31 (4.51,
10.97) | 8.50 (4.98,
13.29) | 4.00–10.00 | 0.144 |
| Plasma |
|
|
|
|
| Albumin
(g/l) | 28.95 (25.88,
31.85) | 29.20 (26.20,
32.70) | 40.00–55.00 | 0.542 |
| Total
bilirubin (µmol/l) | 50.60 (15.43,
101.78) | 50.60 (23.80,
117.70) | 0.00–18.80 | 0.308 |
|
Creatinine (µmol/l) | 85.85 (67.10,
124.35) | 79.00 (62.70,
128.00) | 57.00–111.00 | 0.814 |
| Sodium
(mmol/l) | 134.40 (130.63,
138.35) | 134.20 (130.10,
138.10) | 137.00–147.00 | 0.925 |
| Glucose
(mmol/l) | 6.93 (5.54,
8.63) | 7.16 (5.47,
9.44) | 4.16–6.44 | 0.578 |
| Urea
(mmol/l) | 8.55 (5.50,
13.26) | 9.19 (5.80,
15.00) | 1.70–8.30 | 0.512 |
|
Chloride (mmol/l) | 102.00 (94.48,
104.35) | 99.00 (94.70,
104.60) | 99.00–110.00 | 0.658 |
| ALT
(U/l) | 41.65 (19.98,
60.05) | 29.60 (16.00,
60.30) | 9.00–50.00 | 0.145 |
| AST
(U/l) | 60.30 (28.65,
130.95) | 42.80 (25.00,
92.20) | 15.00–40.00 | 0.092 |
| Direct
bilirubin (µmol/l) | 21.75 (6.43,
63.90) | 28.80 (13.30,
77.50) | 0.00–6.80 | 0.034 |
| Total
protein (g/l) | 58.95 (52.28,
67.48) | 58.90 (51.80,
65.20) | 65.00–85.00 | 0.781 |
| Total
bile acid (µmol/l) | 28.05 (16.28,
61.78) | 36.10 (8.20,
102.60) | 0.00–10.00 | 0.784 |
|
Prothrombin time (sec) | 16.30 (14.20,
19.15) | 16.00 (14.00,
19.90) | 9.40–12.50 | 0.847 |
|
Prothrombin time (INR) | 1.38 (1.21,
1.55) | 1.44 (1.26,
1.81) | 0.80–1.20 | 0.136 |
| CRP
(mg/l) | 28.63 (10.78,
61.88) | 44.50 (18.36,
87.88) | 0.00–5.00 | 0.018 |
| Ascites |
|
| – |
|
| WBC
(cells/µl) | 1,771.00 (450.00,
3,195.00) | 1,515.00 (600.00,
6,127.00) | – | 0.741 |
| PMN
(cells/µl) | 1,077.10 (279.70,
2,494.00) | 800.00 (120.12,
4,262.65) | – | 0.931 |
| Kalium
(mmol/l) | 3.79 (3.44,
4.29) | 3.93 (3.36,
4.47) | – | 0.977 |
| Sodium
(mmol/l) | 134.60 (131.30,
139.00) | 134.30 (129.80,
139.40) | – | 0.485 |
|
Chloride (mmol/l) | 106.90 (99.20,
110.30) | 104.80 (98.10,
110.00) | – | 0.315 |
| Glucose
(mmol/l) | 7.78 (6.51,
8.79) | 7.70 (6.28,
9.75) | – | 0.538 |
| Albumin
(g/l) | 9.20 (4.20,
17.00) | 7.10 (4.40,
11.80) | – | 0.260 |
|
Positive ascitic fluid
culture | 21 (8.50) | 118 (47.5) | – | 0.009 |
|
In-hospital mortality | 12 (4.86) | 37 (14.98) | – | 0.511 |
Laboratory results of plasma and
ascitic fluid analysis in Groups 1 and 2
The results of the laboratory analyses of plasma and
ascitic fluid were compared between Group 1 (SBP; 2011–2013) and
Group 2 (SBP, 2014–2016). The laboratory results for Group 1 and
Group 2 were not distinctly different, except for direct bilirubin
[21.75 (6.43, 63.90) vs. 28.80 (13.30, 77.50), P=0.034], C-reactive
protein (CRP) in the plasma [28.63 (10.78, 61.88) vs. 44.50 (18.36,
87.88), P=0.018] and positive bacterial culture of ascitic fluid
[21 (8.50%) vs. 118 (47.5%), P=0.009]; these values were distinctly
lower in Group 1 compared with those in Group 2 (Table II).
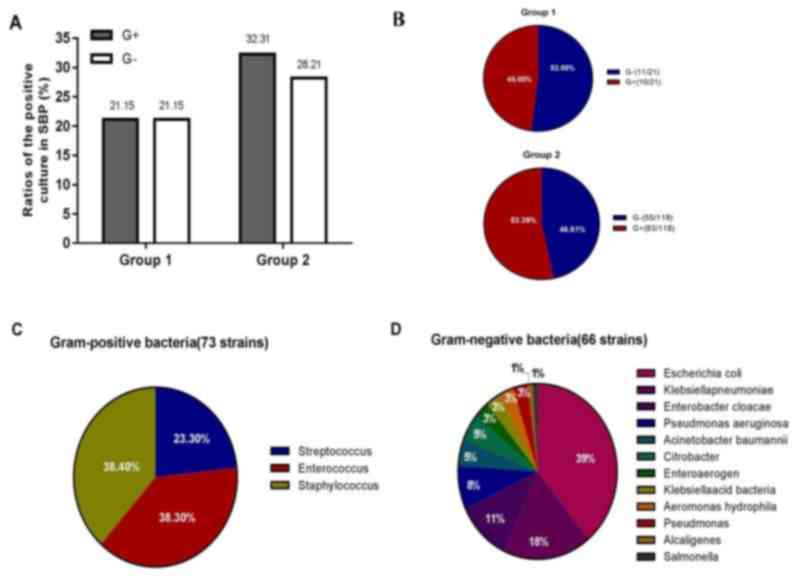
Classification of total bacteria
As presented in Fig.
2, during the retrospective enrolment period, a total of 247
patients were diagnosed with SBP, and the total number of bacterial
strains obtained from the positive culture of ascitic fluid was
139. In addition, the number of bacteria detected in Group 1 (21
strains) was markedly lower than that in Group 2 (118 strains).
Furthermore, the rate of infection with GPB was markedly higher in
Group 2 than that in Group 1 [10/21 (48%) vs. 63/118 (53.4%);
Fig. 2B]. Over time, GPB and
gram-negative bacteria (GNB) were increased, while the increase of
GPB was greater than that of GNB (Fig.
2A and B).
The strains obtained from the ascitic fluid of
patients during the whole term of the study (2011–2016) are
presented in Fig. 2C and D. Among
the bacteria in ascitic fluid, 139 species were identified, of
which 66 (47.5%) were GPB and 73 (52.5%) were GNB. Among the GNB,
Escherichia coli was the most common isolated stain (26 out
of 66 cases, 39.4%), followed by Klebsiella pneumonia (12
cases, 18.2%), Enterobacter cloacae (7 cases, 10.6%),
Pseudomonas aeruginosa (5 cases, 7.6%), Acinetobacter
baumannii and Citrobacter (3 cases, 4.6%, respectively),
as well as Enteroaerogen, Klebsiella acid bacteria,
Aeromonas hydrophila and Pseudomonas (2 cases, 3.0%,
respectively), Alcaligenes and Salmonella (1 case,
1.5%, respectively). The GPB comprised Streptococcus (17
cases, 23.3%), as well as Enterococcus and
Staphylococcus species (28 cases, 38.3%, respectively).
Laboratory results of cirrhotic
patients with culture-positive SBP compared between GNB and
GPB
The 73 SBP patients with GPB, compared with the 66
SBP patients with GNB, were discovered to have decreased mean
plasma ALT [23.5 (15.0, 56.2) vs. 41.1 (21.2, 73.1), P=0.001] and
AST [38.5 (24.3, 75.9) vs. 62.0 (29.3, 139.9), P=0.004] levels, and
a greater prothrombin time [international normalized ratio, 4.49
(1.30, 1.87) vs. 1.38 (1.21, 1.60), P=0.011]. Furthermore, SBP
patients with GPB, compared with those with GNB, had an obviously
lower median ascitic white blood cell count [884.0 (173.0, 6891.8)
vs. 1, 973.0 (937.8, 3, 913.0), P=0.002], PMN [362.6 (43.2, 5,
040.0) vs. 1232.2 (498.8, 2, 557.5), P=0.001] and albumin [6.20
(4.15, 10.20) vs. 8.60 (4.58, 16.63), P=0.008; Table III].
| Table III.Laboratory parameters of cirrhotic
patients with culture-positive spontaneous bacterial peritonitis
compared between Gram-negative bacteria and Gram-positive
bacteria. |
Table III.
Laboratory parameters of cirrhotic
patients with culture-positive spontaneous bacterial peritonitis
compared between Gram-negative bacteria and Gram-positive
bacteria.
| Parameter | Gram-positive
bacteria (n=73) | Gram-negative
bacteria (n=66) | P-value |
|---|
| WBC
(109/l) | 8.07 (4.80,
13.1) | 8.49 (4.85,
13.15) | 0.633 |
| Plasma |
|
|
|
| Albumin
(g/l) | 29.3 (26.2,
32.2) | 29.0 (26.2,
32.5) | 0.600 |
| Total
bilirubin (µmol/l) | 51.8 (23.9,
114.2) | 50.7 (20.3,
106.8) | 0.351 |
|
Creatinine (µmol/l) | 87.0 (62.7,
131.2) | 77.4 (64.1,
119.5) | 0.362 |
| Sodium
(mmol/l) | 134.8 (130.6,
138.9) | 134.0 (139.8,
137.2) | 0.213 |
| Glucose
(mmol/l) | 7.25 (5.34,
9.45) | 6.94 (5.54,
9.19) | 0.606 |
| Urea
(mmol/l) | 9.83 (6.21,
15.42) | 8.01 (5.74,
13.92) | 0.157 |
|
Chloride (mmol/l) | 99.3 (95.2,
104.9) | 100.4 (93.9,
103.8) | 0.780 |
| ALT
(U/l) | 23.5 (15.0,
56.2) | 41.1 (21.2,
73.1) | 0.001 |
| AST
(U/l) | 38.5 (24.3,
75.9) | 62.0 (29.3,
139.9) | 0.004 |
| Direct
bilirubin (µmol/l) | 28.9 (13.2,
76.1) | 25.0 (9.5,
70.6) | 0.450 |
| Total
protein (g/l) | 58.5 (51.2,
64.9) | 60.0 (53.2,
66.8) | 0.396 |
| Total
bile acid (µmol/l) | 38.4 (10.0,
99.7) | 31.5 (11.8,
100.1) | 0.873 |
|
Prothrombin time (sec) | 16.4 (14.3,
20.4) | 16.0 (13.9,
18.9) | 0.339 |
|
Prothrombin time (INR) | 4.49 (1.30,
1.87) | 1.38 (1.21,
1.60) | 0.011 |
| CRP
(mg/l) | 47.7 (21.7,
85.5) | 43.3 (20.5,
80.5) | 0.962 |
| Ascites |
|
|
|
| WBC
(cells/µl) | 884.0 (173.0,
6,891.8) | 1973.0 (937.8,
3,913.0) | 0.002 |
| PMN
(cells/µl) | 362.6 (43.2,
5,040.0) | 1232.2 (498.8,
2,557.5) | 0.001 |
| Kalium
(mmol/l) | 3.94 (3.34,
4.44) | 3.90 (3.43,
4.43) | 0.793 |
| Sodium
(mmol/l) | 134.8 (129.9,
139.7) | 134.2 (130.0,
138.8) | 0.712 |
|
Chloride (mmol/l) | 105.6 (98.9,
109.8) | 105.7 (98.3,
111.0) | 0.903 |
| Glucose
(mmol/l) | 7.81 (6.60,
9.65) | 7.62 (6.27,
9.43) | 0.314 |
| Albumin
(g/l) | 6.20 (4.15,
10.20) | 8.60 (4.58,
16.63) | 0.008 |
In-hospital complications and
different pathogenies compared between GNB and GPB
Comparison of the in-hospital complications and
different pathogenies revealed significantly higher alcoholic
hepatitis (18.18 vs. 35.62, P=0.042) and Splenauxe (10.61 vs.
27.40, P=0.008), as well as lower constipation (0.001 vs. 9.09,
P=0.020) in subjects with GPB vs. GNB (Table IV).
| Table IV.Comparison of in-hospital
complications and different pathogenies between Gram-negative
bacteria and Gram-positive bacteria. |
Table IV.
Comparison of in-hospital
complications and different pathogenies between Gram-negative
bacteria and Gram-positive bacteria.
| Item | Gram-positive
bacteria (n=73) | Gram-negative
bacteria (n=66) | P-value |
|---|
| Pathogenies, n
(%) |
|
|
|
|
Alcoholic hepatitis | 27 (36.99) | 13 (19.70) | 0.042 |
|
Hepatitis B | 35 (47.95) | 32 (48.48) | 1.000 |
|
Hepatitis C | 3 (4.11) | 5 (7.58) | 1.000 |
|
Hepatitis B + C | 1 (1.37) | 1 (1.52) | 1.000 |
| Primary
biliary hepatitis | 0 (0.00) | 3 (4.55) | 1.000 |
|
Autoimmune hepatitis | 2 (2.74) | 2 (3.03) | 1.000 |
| Complications, n
(%) |
|
|
|
| Reflux
esophagitis | 11 (15.07) | 12 (18.18) | 0.348 |
|
Hepatorenal syndrome | 14 (19.18) | 19 (28.79) | 0.259 |
|
Hypoproteinemia | 58 (79.45) | 47 (71.21) | 0.354 |
| Upper
gastrointestinal hemorrhage | 16 (21.92) | 7 (10.61) | 0.074 |
| Hepatic
encephalopathy | 30 (41.10) | 18 (27.27) | 0.088 |
|
Esophagus varix | 25 (34.25) | 18 (27.27) | 0.278 |
|
Esophagus bleeding | 17 (23.29) | 9 (13.64) | 0.228 |
|
Splenauxe | 21 (28.77) | 8 (12.12) | 0.008 |
| Spleen
hyperfunction | 32 (43.84) | 25 (37.88) | 0.477 |
|
Gallstone | 11 (15.07) | 9 (13.64) | 0.989 |
|
Cholecystitis | 6 (8.22) | 5 (7.58) | 0.889 |
|
Pulmonary infection | 16 (21.92) | 17 (25.76) | 0.597 |
| Pleural
effusion | 13 (17.81) | 15 (22.73) | 0.472 |
|
Constipation | 1 (1.37) | 7 (10.61) | 0.020 |
|
Gastrohelcosis | 11 (15.07) | 9 (13.64) | 0.588 |
| Hepatic
failure | 17 (23.29) | 17 (25.76) | 0.590 |
| Chronic
renal failure | 15 (20.55) | 10 (15.15) | 0.410 |
|
Hyperkalemia | 9 (12.33) | 9 (13.64) | 0.819 |
|
Hypokalemia | 23 (31.51) | 22 (33.33) | 0.819 |
|
Hyponatremia | 7 (9.59) | 8 (12.12) | 0.843 |
|
Anemia | 30 (41.10) | 23 (34.85) | 0.451 |
|
Hemorrhagic shock | 4 (5.48) | 2 (3.03) | 0.802 |
| Primary
hepatic carcinoma | 19 (26.03) | 17 (25.76) | 0.971 |
| Portal
hypertension | 7 (9.59) | 7 (10.61) | 0.843 |
|
Metabolic acidosis | 5 (6.85) | 4 (6.06) | 0.851 |
Antibiotic resistance of GNB and GPB
strains
In the present study, Escherichia coli (GNB)
and coagulase-negative Staphylococcus (GPB) were the major
pathogens in SBP. Furthermore, 16 Escherichia coli strains
and 12 Klebsiella pneumonia strains were extended-spectrum
β-lactamase-positive (Table V). The
resistance rate of Staphylococcus aureus (n=8) and
coagulase-negative Staphylococcus (n=20) to penicillin
(ampicillin) was 100% (8,20), while the corresponding rate for
vancomycin, teicoplanin, amikacin and linezolid was 0%, which was
consistent with recommendations provided by the Clinical Laboratory
Standards Institute (11).
| Table V.Antibiotic resistance of
Gram-negative and -positive bacterial strains. |
Table V.
Antibiotic resistance of
Gram-negative and -positive bacterial strains.
| A, Antibiotic
resistance of Gram-negative bacterial strains |
|---|
|
|---|
|
| Escherichia
coli (n=26) | Klebsiella
pneumoniae (n=12) |
|---|
|
|
|
|
|---|
| Antibiotic, n
(%) | ESBL-positive
(n=16) | ESBL-negative
(n=10) | ESBL-positive
(n=16) |
|---|
| Ampicillin | 16 (100.00) | 10 (100.00) | 12 (75.00) |
|
Ticarcillin/clavulanic acid | 3 (18.75) | 0 (0.00) | 1 (6.25) |
| Amikacin | 0 (0.00) | 0 (0.00) | 1 (6.25) |
| Aztreonam | 7 (43.75) | 0 (0.00) | 2 (12.50) |
| Chloromycetin | 8 (50.00) | 0 (0.00) | 1 (6.25) |
| Cefazidime | 3 (18.75) | 0 (0.00) | 2 (12.50) |
| Ciprofloxacin | 13 (81.25) | 2 (20.00) | 2 (12.50) |
| Cefotaxime | 11 (68.75) | 0 (0.00) | 2 (12.50) |
| Cephazolin | 15 (93.75) | 1 (10.00) | 2 (12.50) |
| Cefepime | 6 (37.50) | 0 (0.00) | 2 (12.50) |
| Gentamicin | 7 (43.75) | 0 (0.00) | 1 (6.25) |
| Imipenem | 0 (0.00) | 0 (0.00) | 1 (6.25) |
| Levofloxacin | 13 (81.25) | 2 (20.00) | 2 (12.50) |
| Meropenem | 0 (0.00) | 0 (0.00) | 1 (6.25) |
| Piperacillin | 16 (100.00) | 0 (0.00) | 3 (18.75) |
|
Ampicillin/sulbactam | 5 (31.25) | 0 (0.00) | 2 (12.50) |
| SMZ | 12 (75.00) | 0 (0.00) | 3 (18.75) |
| Acheomycin | 14 (87.50) | 1 (10.00) | 3 (18.75) |
|
Piperacillin/tazobactam | 2 (12.50) | 0 (0.00) | 1 (6.25) |
|
| B, Antibiotic
resistance of Gram-positive bacterial strains |
|
| Antibiotic, n
(%) |
Staphylococcus aureus
(n=8) |
Coagulase-negative
Staphylococcus (n=20) |
|
| Ampicillin | 8 (100.00) | 20 (100.00) |
|
Ticarcillin/clavulanic acid | 1 (12.50) | 18 (90.00) |
| Amikacin | 0 (0.00) | 0 (0.00) |
| Clindamycin | 1 (12.50) | 6 (30.00) |
| Ciprofloxacin | 0 (0.00) | 10 (50.00) |
| Erythromycin | 3 (37.50) | 18 (90.00) |
| Macrodantin | 0 (0.00) | 19 (95.00) |
| Cefoxitin | 1 (12.50) | 20 (100.00) |
| Gentamicin | 0 (0.00) | 9 (45.00) |
| Linezolid | 0 (0.00) | 1 (5.00) |
| Tobramycin | 1 (12.50) | 9 (45.00) |
| Oxacillin | 1 (12.50) | 18 (90.00) |
| Penicillin | 6 (75.00) | 20 (100.00) |
| Rifampicin | 0 (0.00) | 16 (80.00) |
| SMZ | 1 (12.50) | 14 (70.00) |
|
Quinupristin/dalfopristin | 0 (0.00) | 0 (0.00) |
| Tetracycline | 0 (0.00) | 6 (30.00) |
| Teicoplanin | 0 (0.00) | 0 (0.00) |
| Vancomycin | 0 (0.00) | 0 (0.00) |
Discussion
SBP is a general and severe complication of LC
patients with ascites. It remains to be associated with a
significant amount of mortality, in spite of recent improvements in
curative approaches (12). It is
generally accepted that an intestinal GNB flora, particularly
Enterobacteriaceae, is the major cause of SBP (13). However, a number of studies have
indicated that the proportion of GPB in SBP was increased even more
than that of GNB (2,14,15).
Furthermore, the emergence of multidrug-resistant bacteria and the
variation in the epidemiology of bacteria may lead to failure of
the first-line empirical treatment program, thereby posing great
challenges (16). In view of the
complexity of SBP strains and the dependence on empirical
treatment, the present study aimed to clarify the changes of the
bacterial spectrum in SBP and drug resistance, so as to provide a
reliable reference for clinical practice.
In the present study, during the observational
period, the number of patients with SBP increased, and the number
of bacteria also increased over time. The proportion of GPB
increased between 2014–2016 compared with 2011–2013, and was even
higher than the proportion of GNB. Since the detection methods and
instruments used were the same between 2011 and 2016, there should
be no significant difference in detection sensitivity. These
results were in coherence with several studies, which reported a
high frequency of GPB infection associated with SBP (17). Through the analysis of serological
and ascites indexes, it was revealed that direct bilirubin, CRP in
the plasma and the positive rate of ascites culture in Group 2 were
all higher than those in Group 1. This may be attributed to the
clinicians paying more attention to patients with cirrhosis
compared to patients with SBP, leading to an improved rate of
detection.
Next, the laboratory parameters of cirrhotic
patients with culture-positive SBP and their in-hospital
complications, as well as the pathogeny and complications were
compared between GNB and GPB. The results indicated that GPB
infection was more likely to occur in alcoholic hepatitis patients,
and to be associated with complications of splenauxe and
constipation, while GNB infection caused more serious liver damage
and severe abdominal infection. Therefore, the results of the
present study suggested that clinicians should pay attention to the
possibility of GPB infection in alcoholic hepatitis patients with
SBP, and to consider taking measures to prevent splenauxe and
constipation in SBP patients with GPB infection. In addition, for
SBP patients with GNB infection, it is essential to keep a watchful
eye on the occurrence of liver damage.
Furthermore, the antibiotic resistance of GPB and
GNB was assessed. The results on drug sensitivity revealed that the
resistance rate of GPB and GNB to penicillin (ampicillin) was 100%,
while the resistance rates to amikacin, imipenem, meropenem,
piperacillin/tazobactam were 0% for GNB, and the resistance rates
to vancomycin, teicoplanin, amikacin and linezolid were 0% for GPB.
These results indicate that the antibiotics to be appliedmay in
part be determined based on the bacterial strains involved in SBP
in individual patients. The reported percentage of drug resistance
of major pathogenic bacteria to antibiotics recommended as
first-line medications by guidelines is relatively high (10,18,19).
This may be attributed to the imperfection of the antibiotic
management system in China. The results of the present study
suggest that the use of acombination of ampicillin/sulbactam or
piperacillin/tazobactam as an experiential therapy for SBP
patients. In nosocomial cases, the abovementioned drugs should be
combined with vancomycin, linezolid or teicoplanin, when
required.
The present study has a number of limitations.
First, the patients included were from a single unit (Beijing Di
Tan Hospital, Capital Medical University, Beijing, China) where the
occurrence of HBV associated with chronic kidney disease, LC and
hepatocellular carcinoma is high. Furthermore, due to the
retrospective nature of the study, a possibility for bias and
imprecise data collection may exist. More comprehensive prospective
studies using a larger number of cases and involving multiple units
may be essential. Furthermore, more samples will be collected to
validate this trend in the future. It is imperative that physicians
consider all relevant factors when diagnosing and treating patients
with cirrhosis and SBP (20,21).
Furthermore, SBP is a severe complication of LC, and
all patients should be considered for inchoate diagnosis and
curative treatment in order to lower the amount of fatalities
(22). High vigilance in patients
with ascites presenting with acute clinical deterioration is
imperative. The present study indicated differences of the
laboratory results of Groups 1 and 2, as well as in-hospital
complications between patients with GPB and GNB infection. Combined
use of ampicillin/sulbactam or piperacillin/tazobactamin
experiential therapy is recommended. In nosocomial cases, these
drugs should be combined with vancomycin, linezolid or teicoplanin
when required. Therefore, it is essential to watch out for changes
in respective indicatorsin plasma and ascites, as well as detect
pathogens as early as possible to ensure for timely diagnosis and
treatment of SBP.
Acknowledgements
Not applicable.
Funding
The present study was supported by a grant from the
Beijing Key Laboratory of Emerging Infectious Diseases Project
(grant no. DTKF201702).
Availability of data and materials
The dataset supporting the results of the present
study are included in the article.
Authors' contributions
JG and YW contributed to the conception of the study
and prepared the manuscript, as well as overall supervision. JS
revised the manuscript. JG and HW collected he data. SL, HC and JL
analyzed the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
All of the patients' data were collected
retrospectively from their electronic health records. The present
study was approved by the Ethics Committee of the Beijing Di Tan
Hospital (Beijing, China) and was in accordance with the 1975
Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
SBP
|
spontaneous bacterial peritonitis
|
|
LC
|
liver cirrhosis
|
|
CRP
|
C-reactive protein
|
|
PMN
|
polymorphonuclear neutrophil
|
|
GNB
|
Gram-negative bacteria
|
|
GPB
|
Gram-positive bacteria
|
References
|
1
|
Tsochatzis EA, Bosch J and Burroughs AK:
Liver cirrhosis. Lancet. 383:1749–1761. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fiore M, Maraolo AE, Gentile I, Borgia G,
Leone S, Sansone P, Passavanti MB, Aurilio C and Pace MC: Current
concepts and future strategies in the antimicrobial therapy of
emerging Gram-positive spontaneous bacterial peritonitis. World J
Hepatol. 9:1166–1175. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Cui Y and Jia J: Update on epidemiology of
hepatitis B and C in China. J Gastroenterol Hepatol. 28 (Suppl
1):S7–S10. 2013. View Article : Google Scholar
|
|
4
|
Enomoto H, Inoue S, Matsuhisa A and
Nishiguchi S: Diagnosis of spontaneous bacterial peritonitis and an
in situ hybridization approach to detect an ‘unidentified’
pathogen. Int J Hepatol. 2014:6346172014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kim JH, Jeon YD, Jung IY, Ahn MY, Ahn HW,
Ahn JY, Ku NS, Han SH, Choi JY, Ahn SH, et al: Predictive factors
of spontaneous bacterial peritonitis caused by gram-positive
bacteria in patients with cirrhosis. Medicine (Baltimore).
95:e34892016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Paul K, Kaur J and Kazal HL: To study the
incidence, predictive factors and clinical outcome of spontaneous
bacterial peritonitis in patients of cirrhosis with ascites. J Clin
Diagn Res. 9:OC09–OC12. 2015.PubMed/NCBI
|
|
7
|
Yan K and Garcia-Tsao G: Novel prevention
strategies for bacterial infections in cirrhosis. Expert Opin
Pharmacother. 17:689–701. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fukui H: Gut Microbiome-based therapeutics
in liver cirrhosis: Basic consideration for the next step. J Clin
Transl Hepatol. 5:249–260. 2017.PubMed/NCBI
|
|
9
|
Runyon BA: Management of adult patients
with ascites due to cirrhosis: Update 2012. American Association
for the Study of Liver Diseases. 2012, https://www.aasld.org/sites/default/files/guideline_documents/adultascitesenhanced.pdfMay
6–2012
|
|
10
|
European Association for the Study of the
Liver, . EASL clinical practice guidelines on the management of
ascites, spontaneous bacterial peritonitis, and hepatorenal
syndrome in cirrhosis. J Hepatol. 53:397–417. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Clinical and Laboratory Standards
Institute (CLSI), . Reference Method for Broth Dilution Antifungal
Susceptibility Testing of Yeasts. 4th. CLSI standard M27. CLSI;
Wayne, PA: 2017
|
|
12
|
Bal CK, Daman R and Bhatia V: Predictors
of fifty days in-hospital mortality in decompensated cirrhosis
patients with spontaneous bacterial peritonitis. World J Hepatol.
8:566–572. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wong F: Acute kidney injury in liver
cirrhosis: New definition and application. Clin Mol Hepatol.
22:415–422. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cholongitas E, Papatheodoridis GV, Lahanas
A, Xanthaki A, Kontou-Kastellanou C and Archimandritis AJ:
Increasing frequency of Gram-positive bacteria in spontaneous
bacterial peritonitis. Liver Int. 25:57–61. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yang Y, Li L, Qu C, Zeng B, Liang S, Luo
Z, Wang X and Zhong C: Diagnostic accuracy of serum procalcitonin
for spontaneous bacterial peritonitis due to end-stage liver
disease: A Meta-analysis. Medicine (Baltimore). 94:e20772015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
de Mattos AA, Costabeber AM, Lionco LC and
Tovo CV: Multi-resistant bacteria in spontaneous bacterial
peritonitis: A new step in management? World J Gastroenterol.
20:14079–14086. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hatami B, Ashtari S, Sharifian A, Rahmani
Seraji H, Khalili E, Hatami Y and Zali MR: Changing the cause of
liver cirrhosis from hepatitis B virus to fatty liver in Iranian
patients. Gastroenterol Hepatol Bed Bench. 10 (Suppl):S20–S26.
2017.PubMed/NCBI
|
|
18
|
Li YT, Yu CB, Huang JR, Qin ZJ and Li LJ:
Pathogen profile and drug resistance analysis of spontaneous
peritonitis in cirrhotic patients. World J Gastroenterol.
21:10409–10417. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Xie Y, Tu B, Zhang X, Bi J, Shi L, Zhao P,
Chen W, Liu S, Xu D and Qin E: Investigation on outcomes and
bacterial distributions of liver cirrhosis patients with
gram-negative bacterial bloodstream infection. Oncotarget.
9:3980–3995. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kim T, Hong SI, Park SY, Jung J, Chong YP,
Kim SH, Lee SO, Kim YS, Woo JH, Lim YS, et al: Clinical features
and outcomes of spontaneous bacterial peritonitis caused by
streptococcus pneumoniae: A matched Case-control study. Medicine
(Baltimore). 95:e37962016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Acevedo J: Multiresistant bacterial
infections in liver cirrhosis: Clinical impact and new empirical
antibiotic treatment policies. World J Hepatol. 7:916–921. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Karkmann K, Piecha F, Runzi AC, Schulz L,
von Wulffen M, Benten D, Kluwe J and Wege H: Management of
compensated liver cirrhosis 2018-Evidence based prophylactic
measures. Z Gastroenterol. 56:55–69. 2018.(In German). PubMed/NCBI
|